
Abstract
Background:
Recently it has been proposed that microglial response has a stage-dependent effect on the progression of Alzheimer’s disease (AD). Cerebrospinal fluid (CSF) sTREM2 has emerged as a promising microglial activation marker.
Objective:
To test the stage-dependent role of microglia by studying the association between baseline sTREM2 and dynamic brain structural changes in AD and mild cognitive impairment (MCI) patients.
Methods:
22 amyloid-β-positive (A+) and tau-positive (T+) AD and 24 A+T+MCI patients were identified from the Alzheimer’s Disease Neuroimaging Initiative. The patients had baseline CSF amyloid-β, phosphorylated-tau, and sTREM2, and were followed up for at least one year by T1-weighted and diffusion tensor imaging scans. Gray matter volumes and white matter microstructural integrity were evaluated. Linear mixed models were applied to analyze how baseline sTREM2 may influence the rate of brain structural changes while adjusting for the effects of age, APOE4 status, and the CSF core markers.
Results:
In A+T+AD patients, baseline CSF sTREM2 was associated with faster mean diffusivity increase in the bilateral posterior corona radiata and right superior longitudinal fasciculus. In A+T+MCI patients, baseline CSF sTREM2 was associated slower gray matter volumetric loss in parahippocampal gyrus, left fusiform cortex, left middle temporal gyrus, and left lateral occipital cortex. Baseline CSF sTREM2 also had a protective effect against mean diffusivity increase in right inferior fronto-occipital fasciculus, left superior longitudinal fasciculus, left forceps minor, and left uncinate fasciculus.
Conclusion:
Microglial activation at early stage might have a protective effect against neurodegeneration, while at late stage it might facilitate AD. Future efforts on modulating microglial activation could be promising, given a carefully selected time window for intervention.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common senile dementia with limited interventions to prevent disease progression. Previous efforts have been made mainly focusing on amyloid-β (Aβ) clearance and only lead to controversial and partial success [1]. Now it is well established that AD pathogenesis is a multifaceted process involving amyloid deposition, neurofibrillary tangle formation, and neuronal damage [2]. Apart from the A/T/N components, activated microglia and astrocytes have been readily observed in the vicinity of amyloid plaques and neurofibrillary tangles in pathological examinations; however, they were largely considered as a secondary response to the core pathologies [3, 4]. In the past decades, neuroinflammation has been increasingly recognized as an important process in the pathogenesis of AD [5]. Laboratory studies have established that activated microglia in an inflammatory state could disturb neuronal functions and cause neuronal damage by secretion of inflammatory cytokines and direct cellular interactions [6, 7]. Further clinical investigations using TSPO PET tracers have observed increased microglial activation in patients with clinically diagnosed AD dementia, which is in turn associated with cognitive impairment [8, 9]. Intriguingly, when the study scope expands to earlier stages of AD, contradicting results have been reported with regard to the association between microglial activation and cognitive impairment [10–12]. Originating from the clinical observations, a 2-peak model of microglial activation has been proposed, which posits that at early stage of the disease, an initial microglial mobilization serves to protect the brain, while as glial response fails to resolve under the neuroinflammatory milieu, a second peak of inflammatory microglial activation occurs at late stage of AD, this time causing neuronal damage and facilitates disease progression [13].
Apart from TSPO PET tracers, cerebrospinal fluid (CSF) soluble triggering receptor expressed on myeloid cells 2 (sTREM2) has emerged as a promising marker of microglial activation in patients. TREM2 is a immunoglobulin superfamily receptor glycoprotein and within the central nervous system, expressed mainly by microglia [14]. Genome-wide association studies have found that mutations of TREM2 gene are associated with increased risk of AD [15], strongly suggesting that microglia have an active role in the pathogenesis of AD. sTREM2 is originated from the ectodomain of TREM2 receptor and is released to extracellular space in the process of proteolytic cleavage of TREM2 [16, 17]. Elevated CSF sTREM2 concentration has been found in patients with AD [18], and the associations between sTREM2 and AD pathology markers have been then established [19–21]. However, similar to observations from TSPO imaging studies, multifaceted relationships between sTREM2 expression and neuronal damage or cognitive decline markers have been reported in recent years [22–24]. In the current study, we hypothesized that 1) Microglial activation plays an active role in brain damage in AD; 2) The role of microglial activation in AD is stage-dependent. We visited the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database and tested the following predictions: 1) CSF sTREM2 is associated with the rate of gray and white matter change in AD and mild cognitive impairment (MCI) patients, and 2) the effects of sTREM2 on slope of gray matter/white matter change are different at AD and MCI stages.
MATERIALS AND METHODS
Patients
Thirty-one clinically diagnosed AD and 70 clinically diagnosed MCI patients who had baseline CSF sTREM2, phosphorylated tau (p-Tau), and total Aβ measures, and who had diffusion tensor and T1 weighted MRI scans at baseline and follow-up visits were included in the study from the ADNI database. ADNI was initiated and funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, the Food and Drug Administration, private pharmaceutical companies, and nonprofit organizations. The ADNI study is conducted in accordance with the Declaration of Helsinki, and procedures were approved by the institutional review boards of all participating sites.
The patients had been followed by MRI scans for at least 1 year. The follow-up scheme of ADNI is: visit at baseline (or screening visit), month 3, moth 6, month 12, and followed by annual visits. However, due to the data availability, not all participants had complete imaging data at all timepoints and at uniform intervals (Table 1). To ensure the patients included represents population within AD continuum, only patients with low CSF Aβ1–42 (< 980 Unit, A+) and high CSF p-Tau (> 23.8 Unit, T+) were included in the analysis. The cutoff values were chosen according to the ADNI3 batch analysis of the CSF amyloid and tau biomarkers, (https://adni.bitbucket.io/reference/docs/UPENNBIOK10/ADNI_Methods_Template_Shaw_2019_Roche_Elecsys_ADNI3_CSFs_Batch_1_v1.pdf), leaving 22 A+T+AD and 24 A+T+MCI patients for further analysis in the current study.
Demographic information
ADAS_cog13, Alzheimer’s dementia assessment scale, cognition part, 13 items. Data are shown as mean (standard deviation). *p < 0.05, #number of patients with 0, 1, and 2 alleles carrying APOE4.
T1 weighted structural and diffusion tensor image acquisition
The T1-weighted magnetization prepared rapid gradient echo (MPRAGE) images in ADNI study was acquired using the following parameters: TR =2300 ms, TE = 2.98 ms, 1 x 1 x 1 mm isotropic voxel size, FoV = 256 x 256 mm, 172 slices. The diffu-sion tensor imaging (DTI) scans were obtained with the following settings: TR = 12400 ms, TE =95 ms, 2 x 2 x 2 mm isotropic voxel size, FoV =232 x 232 mm, 80 axial slices, b-value = 1000 s/mm2, 30 diffusion directions. More detailed acquisition parameters can be found at ADNI website (http://adni.loni.usc.edu/methods/documents/mri-protocols/).
Pre-processing of T1 weighted and DTI images
The MPRAGE structural scans were processed using FSL-VBM tool [25]. The T1-weighted images were first skull-stripped, segmented, and transformed in to the MNI152 space using non-linear registration with limited degree of freedom. A study-specific gray matter template was created by averaging all images within the study and contralateral mirror images were averaged to ensure symmetry. All participants’ gray matter images were then registered to the template with non-linear transformation. Finally, local gray matter topology changes were modelled by a modulation process accounting for the non-linear warping estimated in the non-linear transformation process. The resulting modulated gray matter images were smoothed with 4 mm full-width half maximum (FWHM) Gaussian kernel and further used for statistical analysis.
The diffusion tensor MR images were processed using FMRIB’s diffusion toolbox [26]. The DTI scans were first brain extracted with FSL’s brain extraction tool. Motion correction and eddy-current induced and susceptibility correction were performed with FSL’s eddy tool. For the current study, the simple ellipsoid diffusion model was used, and a single diffusion tensor was fitted to each voxel using FSL’s DTIFIT function. Fractional anisotropy (FA) and mean diffusivity (MD) was calculated from the fitted diffusion tensor for each voxel. The FA and MD maps were then transformed to MNI 152 space with FA maps providing spatial reference and FMRIB68-FA as target image. The normalized MD and FA maps were smoothed using 4mm FWHM kernel within the white matter mask in MNI 152 space (> 50%probability) prior to voxel-wise statistical analysis.
Statistical analysis
Statistical analyses on demographic data and CSF biomarker measures were performed using RStudio v1.4. Between-group differences were examined using independent sample T-tests. To interrogate whether CSF sTREM2 is associated with longitudinal gray and white matter changes in patients at different stages of AD, the effects of sTREM2 on slopes of gray matter VBM intensity, white matter MD and FA values were tested using mixed linear models in MCI and AD groups respectively. The mixed effect model approach was chosen as it could better handle irregular follow-up intervals and variations in follow-up visit occurrences. All mixed effect analyses were performed at voxel-wise basis with the aid of VoxelStats package [27], and at region of interest (ROI) level with R. Each participant was allowed to have individual slopes and intercept, group intercept, group slope, sTREM2, and sTREM2:time interaction were included in the model. Age, APOE4 status, CSF total Aβ and p-Tau, and their interactions with time were adjusted in the models, as these factors may moderate the relationship between neuroinflammation and brain structural damage [28]. The effect size of sTREM2:time interaction was tested to answer whether baseline CSF sTREM2 concentration could influence longitudinal change of the dependent variable. FA and MD values in the splenium of corpus callosum, parahippocampal white matter, cingulum, inferior fronto-occipital fasciculus (IFOF) and the fornix were chosen a priori for ROI analysis, as previous studies have suggested these regions to be ‘at risk’ in AD [29]. All voxel-wise analyses were corrected for multiple comparisons using random field theory with an initial cluster forming threshold of 0.001. Clusters with corrected p < 0.05 were considered significant.
RESULTS
Demographics
A total of 22 A+T+AD and 24 A+T+MCI patients were included in the current study. Brief demographic information is described in Table 1. AD patients had significantly lower scores in AD dementia assessment scale (p < 0.001) and slightly lower concentration of CSF Aβ1 - 42 compared to MCI patients, while CSF sTREM2, total tau, and phosphorylated tau did not differ statistically between the two group of patients. AD patients were followed up over an average of 1.3 years, with the median number of follow-up visits being 2 times, while for MCI patients the average follow-up period was 2.6 years and the median follow-up visits was 4 times. The distribution of APOE4 non-carrier, heterozygote APOE4 carrier and homozygote APOE4 carrier were 4/14/6 in MCI patients and 7/10/5 in AD patients from the current study cohort.
Association between sTREM2 and gray matter change in AD and MCI patients
sTREM2 was not associated with the slope of gray matter change in AD patients. On the other hand, sTREM2 had positive interaction with time regarding gray matter change in MCI patients in the left parahippocampal gyrus, left fusiform cortex, left middle temporal gyrus, and left lateral occipital cortex (Fig. 1A and Table 2), suggesting that higher CSF sTREM2 was associated with slower gray matter loss in MCI patients.

Positive effect of sTREM2:Time interaction on gray matter volume and white matter fractional anisotropy in A+T+MCI patients. A) Baseline CSF sTREM2 was associated with slower loss of gray matter volume in the colored clusters. B) Baseline CSF sTREM2 was associated with slower FA decline in the anterior thalamic radiation.
Clusters where baseline sTREM2 influences longitudinal gray matter change in MCI patients
T-max, peak T-statistics within the cluster (positive T values indicate positive association and vice versa); p, cluster-level p value; X, Y, Z, the spatial coordinates of the peak T-statistics; L, left; R, right.
Association between sTREM2 and FA change in AD and MCI patients
In AD patients, sTREM2 did not have significant influence on the slope of FA changes after correcting for age, APOE4, and the CSF core markers. In MCI patients, sTREM2 had positive correlation over time with FA values in left anterior thalamic radiation (Fig. 1B), suggesting that CSF sTREM2 was associated with slower decline of white matter FA values MCI patients.
At ROI level, baseline sTREM2 and time interaction term was positively associated with FA values in the fornix in A+T+MCI patients (standardized β= 0.12, standard error = 0.043, p = 0.015, Fig. 3A).
Association between sTREM2 and MD change in AD and MCI patients
In AD patients, positive sTREM2-time interactions were found in bilateral posterior corona radiata and right superior longitudinal fasciculus with regard to MD values (Fig. 2A). While in MCI patients, sTREM2-time interaction had negative influence on MD increase in right inferior fronto-occipital fasciculus, left superior longitudinal fasciculus, left forceps minor, and left uncinate fasciculus (Fig. 2B and Table 3).
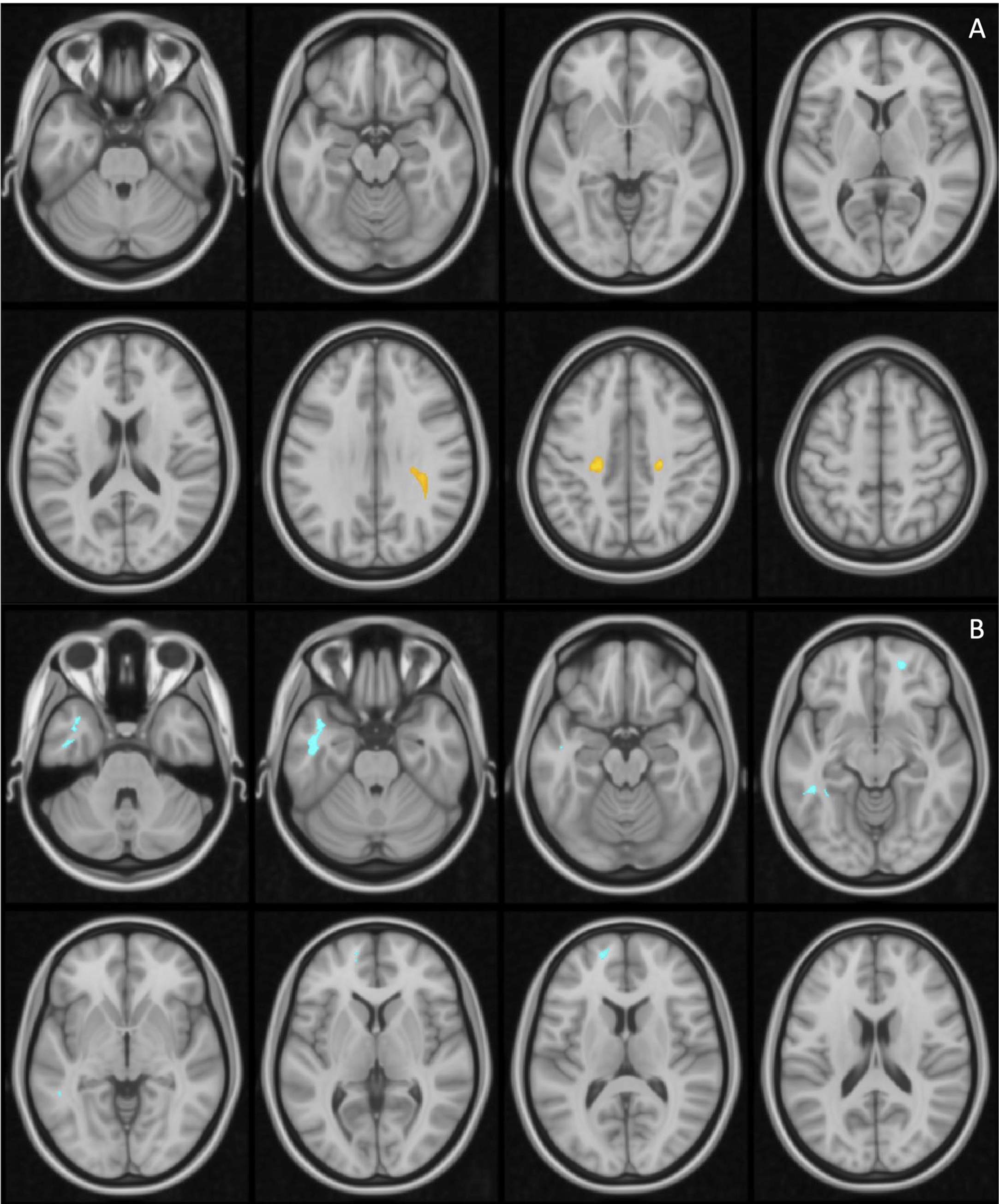
Effects of sTREM2:Time interaction on longitudinal MD value changes. A) Baseline sTREM2 was associated with faster MD increase in AD patients; B) Baseline sTREM2 was associated with slower MD increase in MCI patients. Clusters of positive interactions are shown in hot scheme and negative interactions are shown in blue.
Clusters where baseline sTREM2 influences longitudinal MD change in MCI patients
T-max, peak T-statistics within the cluster (negative T values indicate negative association and vice versa); p, cluster-level p value; X, Y, Z, the spatial coordinates of the peak T-statistics; L, left; R, right.
ROI level analyses also demonstrated the protective effect of sTREM2 on white matter integrity in MCI patients and its detrimental effect in AD patients. sTREM2 and time interaction term was negatively associated with MD values in the fornix (standardized β= –0.066, standard error = 0.028, p = 0.032) and IFOF (standardized β= –0.10, standard error = 0.042, p = 0.026, Fig. 3B, C), but not other regions. In A+T+AD patients, baseline sTREM2 and time interaction term had negative association with MD values in IFOF (standardized β= 0.10, standard error = 0.045, p = 0.027, Fig. 3D).
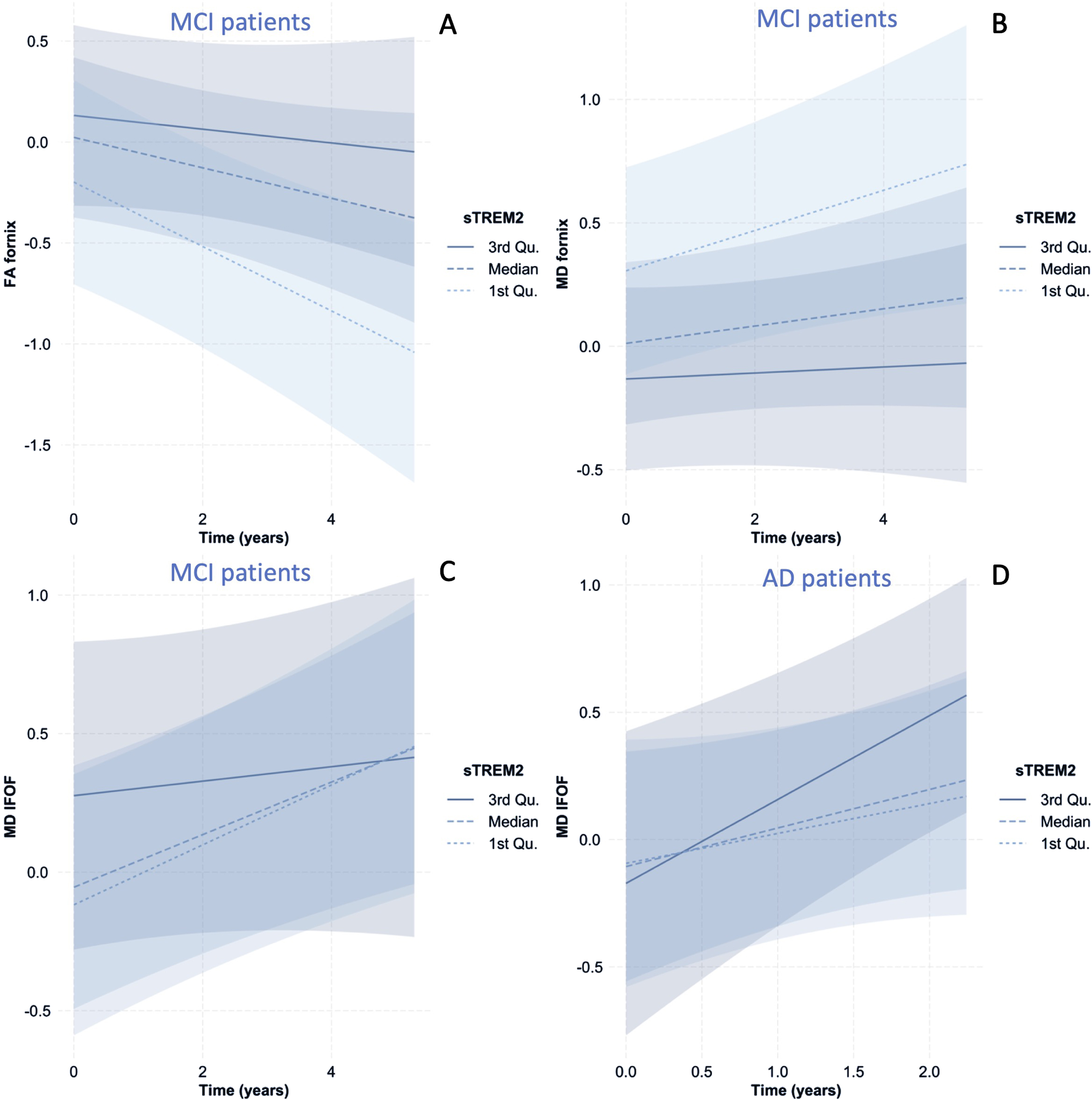
The Influence of baseline sTREM2 on the slope of FA and MD change in the white matter. A-C) MCI patients with higher baseline sTREM2 (3rd quartile) had slower FA decline and MD increase in the fornix compared to patients at median level, while those with lower baseline (1st quartile) sTREM2 underwent faster white matter degeneration. D) AD patients with higher baseline CSF sTREM2 had faster IFOF damage rate (faster MD increase). Qu., quartile.
DISCUSSION
In the current study, the association between CSF sTREM2 concentration and longitudinal brain structural damage (gray and white matter) was investigated in patients within the AD continuum. We were able to demonstrate that in amyloid-positive and tau-positive MCI patients, higher CSF sTREM2 was associated with slower gray matter volumetric loss and slower increase of white matter mean diffusivity in cortical association fibers, while in amyloid-positive and tau-positive AD patients, CSF sTREM2 concentration was associated with faster mean diffusivity increase in white matter. Taken together, the current observations suggest that microglial activation may have a protective effect at earlier stage but turn to be deleterious at late stage in AD continuum.
Gray matter atrophy has been well established as a marker of neurodegeneration and regional atrophy in the medial temporal cortex, inferior temporal, temporal pole, angular gyrus, superior parietal, supramarginal, precuneus, and inferior frontal cortices has been considered a disease-specific atrophy pattern of AD [30]. In the current study, we found that baseline CSF sTREM2 expression had a positive relationship with slope of gray matter change in A+T+MCI patients, i.e., baseline sTREM2 had a protective effect against gray matter atrophy in cortical areas including AD signature regions. These findings fell in line with Femminella et al., who reported that cortical 11C-PBR28 bindings was associated with preserved hippocampal volume in a cross-sectional MCI cohort [31]. Microglial activation’s protective effect on gray matter at early MCI stage may be the basis of its reported association with cognitive preservation by imaging and fluid biomarker studies [12, 32]. The underlying biological mechanism of this protective function might be attributed to microglia’s amyloid clearance and trophic support capability, especially at early stage of the disease when they are likely be in phagocytic phenotypes [33, 34]. Further, sTREM2 itself has also been found to be protective against amyloid aggregation and Aβ related neurotoxicity in vitro. On the other hand, baseline CSF sTREM2 was not found to be associated with gray matter longitudinal change in A+T+AD patients in the current study group. While it might be simply due to the small sample size, the lack of linear relationship may also reflect a transition of microglial functions from being protective to detrimental at later stage of AD. However, it is also possible that the relationship is confounded by cerebral oedema induced by inflammation, which might have interfered the estimation of gray matter volume, and thus further studies are encouraged to further elucidate the issue.
While white matter degeneration used to be viewed as a secondary event due to gray matter atrophy or vascular comorbidity in AD, advances in the past decades has demonstrated that white matter microstructural damage could not be simply explained by the aforementioned factors [29, 37]. In fact, the retro-genesis hypothesis has been proposed, suggesting that late-myelinated tracts undergo degeneration first in AD, indicating a disease-specific pattern [38]. Further studies have established a link between white matter microstructural damage and tau pathology, as well as the value of white matter integrity as a promising biomarker in AD [39, 40]. In the current study, we observed that in A+T+MCI patients, sTREM2 expression was associated with slower longitudinal increase of mean diffusivity but not fractional anisotropy in association fibers. These findings might be related to the fact that FA and MD reflect different aspects of white matter microstructure. It could be speculated that FA could account for both demyelination and axonal loss, while MD is weighted more by diffusivity in the radial directions, therefore is better related to demyelination [41]. In light of the speculation, the current observation might suggest that microglial activation in AD has stronger influence on myeline structures and soma of the neurons but is less related to axonal impairment. In A+T+patients at dementia stage, we were able to demonstrate that sTREM2 concentration was associated with faster MD increase, suggesting that at late stage of AD, microglial activation is associated with accelerated white matter degeneration. This deleterious effect of microglial activation has also been reported by multiple neuroimaging studies evaluating neuroinflammation’s influence at AD stage [42, 43]. Interestingly, in cognitively normal adults with tau pathology, CSF sTREM2 has also been reported to be predictive of temporal lobe atrophy [44]. However, the latter observation might readily reflect the effect of chronic microglial activation, as the T+ older adults might have already borne a chronic inflammatory brain milieu for a period, as are the microglia observed in patients with Down syndrome [45].
The above discussion has led us to one of the limitations of the current study: it is still not fully elucidated whether CSF sTREM2 is preferentially related to certain phenotypes of activated microglia or it could represent activation of all microglia phenotypes in general, considering previous study has suggested sequential TREM2-independent and dependent activation process of microglia [46]. Therefore, the current study has considered CSF sTREM2 as a general marker of the quantity of activated microglia, regardless of specific phenotypes. Further, the CSF markers lacks spatial resolution and consequently whether the complex relationships found in MCI subjects are related to area-specific microglial-neuronal interactions, which might well be the case in AD [5]. Lastly, due to data availability from ADNI dataset, the study is limited by the modest sample size and further, some more recently validated CSF biomarkers such as Aβ42/40 and p-Tau181 were not used.
To summarize, the current study has observed that CSF sTREM2 expression has an overall protective effect on brain structure longitudinal change in A+T+MCI but is deleterious in A+T+AD patients. These findings supported the hypothesis that microglia activation have an active role in the pathogenesis in the AD continuum, and that its effect is dependent on disease stages. Overall, the current study has new evidence that novel strategies intervening microglial activation might be a viable option in efforts to find disease-modifying therapies for AD and has emphasized that caution should be taken in applying such strategies as the effect of microglial activation is likely to be stage-sensitive.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0102r1).