
Abstract
Background:
The links between cerebral small vessel disease (CSVD) burden and neuropsychiatric symptoms (NPS) have not been fully studied.
Objective:
We aimed to explore the associations of the CSVD burden with Neuropsychiatric Inventory (NPI) total scores and its subsyndromes in the elderly without dementia.
Methods:
We investigated 630 non-demented participants from the Alzheimer’s Disease Neuroimaging Initiative. All of them had NPI assessments and 3 Tesla MRI scans at baseline and 616 had longitudinal NPI assessments during the follow-up. Linear mixed-effects models were used to investigate the cross-sectional and longitudinal associations of CSVD burden with NPI total scores and its subsyndromes.
Results:
Higher CSVD burden longitudinally predicted more serious neuropsychiatric symptoms, including NPS (p < 0.0001), hyperactivity (p = 0.0006), affective symptoms (p = 0.0091), and apathy (p < 0.0001) in the total participants. Lacunar infarcts (LIs), white matter hyperactivities (WMHs), and cerebral microbleeds (CMBs) might play important roles in the occurrence of NPS, since they were longitudinally associated with specific neuropsychiatric subsyndromes. LIs contributed to hyperactivity (p = 0.0092), psychosis (p = 0.0402), affective symptoms (p = 0.0156), and apathy (p < 0.0001). WMHs were associated with hyperactivity (p = 0.0377) and apathy (p = 0.0343). However, CMBs were only related to apathy (p = 0.0141).
Conclusion:
CSVD burden was associated with multiple neuropsychiatric symptoms, suggesting the importance of monitoring and controlling vascular risk factors. Different markers of CSVD were associated with specific subsyndromes of NPS, suggesting that different markers tended to occur in different encephalic regions.
Keywords
INTRODUCTION
Cerebral small vessel disease (CSVD) is a common accompaniment of aging which refers to a group of pathological processes with various aetiologias that affect the small arteries, arterioles, venules, and capillaries of the brain [1]. Previous studies showed that CSVD might aggravate some cognitive and psychiatric symptoms [2–4]. Various types of cerebral small vessel disease have been demonstrated to impair the brain network. Therefore, the CSVD burden was usually used to assess the global brain function [5]. Neuroimaging is considered an effective marker in defining small vessel disease [6, 7]. The neuroimaging characteristics of cerebral small vessel disease include white matter hyperintensities (WMHs), cerebral microbleeds (CMBs), lacunar infarcts (LIs), perivascular spaces, and brain atrophy [1, 2]. In our study, we focused on CMBs, WMHs, and lacunar infarcts.
Neuropsychiatric symptoms, such as aggression, apathy, and depression, are major manifestations of dementia and other neurodegenerative diseases [8]. Neuropsychiatric symptoms were associated with adverse effects on activities of daily living, imposing a heavy burden on caregivers [8, 9]. Accumulating evidence has demonstrated that neuropsychiatric symptoms may precede the occurrence of dementia [10, 11]. Furthermore, the patients with neuropsychiatric symptoms have more severe impairments in global, executive, and memory functions [12].
Many previous studies have evaluated the associations of NPS with WMHs, Lis, or CMBs [3, 13], while only a few investigated the relationship between NPS and CSVD burden. NPI scores are used to evaluate NPS. A study reported that cardiovascular and cerebrovascular risk factors were associated with some sub-scores of NPI rather than NPI total score [14]. Therefore, using a longitudinal cohort, we investigated the associations of NPI total score and NPI sub-scores with CSVD burden, WMHs, Lis, and CMBs.
METHODS
The Alzheimer’s Disease Neuroimaging Initiative
Data were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (https://adni.loni.usc.edu). The ADNI was initiated in 2003 as a public-private partnership with its primary objective of obtaining accessible data about the changes in serial MRI, PET, biological markers, as well as clinical and neuropsychological assessments among Alzheimer’s disease patients, mild cognitive impairment (MCI) patients, and cognitive normals [15]. Ethics approval was gained from local institutions and all participants had written informed consent.
Participants
The participants of this study consist of cognitively normal individuals and MCI patients in ADNI-GO and ADNI-2 enrolled from March 2011 to December 2013. All subjects in this study were aged 55 to 91 years and had undergone MRI to identify whether they had cerebral small vessel diseases (CMBs, WMHs, and lacunar infarcts). The exclusion criteria are as follows: 1) subjects having a Hachinski ischemic score of more than 4; 2) subjects diagnosed with dementia or stroke; 3) participants without baseline or follow-up NPI scores. The inclusion criteria of CN participants as follows: 1) Mini-Mental State Examination (MMSE) score was equal or greater than 24, 2) Clinical Dementia Rating (CDR) score was 0, 3) Logical Memory II subscale of the Wechsler Memory Scale-Revised (maximum score of 25) ≥9 for 16 years of education, ≥5 for 8–15 years of education, and ≥3 for 0–7 years of education. The inclusion criteria of MCI participants as follows: 1) MMSE score was less than 24, 2) CDR score was at least 0.5, 3) Logical Memory II subscale of the Wechsler Memory Scale-Revised ≤8 for 16 years of education, ≤4 for 8–15 years of education, ≤2 for 0–7 years of education, and persevered activities of daily living, and absence of dementia.
Finally, 630 subjects (including 344 CSVD participants and 286 non-CSVD participants) were enrolled in this study at baseline. Among them, 616 subjects (including 334 CSVD participants and 282 non-CSVD participants) provided available follow-up data. Among them, 124 individuals were reported to develop dementia during an average follow-up of 56.9 months (range, 0–108 months). Participants with a simple CSVD score ≥1 were categorized into the CSVD group, and those with a simple CSVD score of 0 were categorized into the non-CSVD group.
Assessment of cerebral small vessel disease
Measurement of CMBs
CMBs are small (2 to 10 mm in diameter) areas of the signal void with associated blooming seen on T2-weighted MRI or other sequences that are sensitive to susceptibility effects [2, 16]. The number of CMBs was identified by two independent experienced neurologists blinded to clinical information after reading MRI images, and the third one would confirm the image if there was a disagreement between the first two. If the count of CMBs was more than one, it was recorded as present.
Assessment of WMHs
WMHs are hypertense on T2-weighted sequences and can appear as isointense or hypointense on T1-weighted sequences [2]. The Fazekas rating scale (range, 0–6) was used to assess WMHs by two experienced neurologists. The severity of WMHs was classified as 0 to 1 (Fazekas scale score, 0–1) and 2 to 3 (Fazekas scale score, 3–6).
LIs measurement
LIs are subcortical lesions in the territory of penetrating arteries, with a rounded, ovoid, or tubular cavity and a maximum diameter less than 20 mm on the axial plane, which are presented as hyperintense signals relative to white or gray matter on DWI [2]. We classified the severity of LIs as none-mild (0–2 counts) and moderate-severe (≥3 counts) [6].
Assessment of CSVD burden
In our study, we combined some MRI markers consisting of LIs, WMHs, and CMBs to rate the CSVD burden [6]. Simple CSVD score is the summary score of LIs (0 score = 0 to 2 counts, 1 score ≥3 counts), WMHs (0 score = 0 to 1 count, 1 score ≥2 counts), and CMBs (0 score = 0, 1 score ≥1 count), ranging from 0 to 3. Amended CSVD score is the summary score of LIs (0 score = 0, 1 score = 1 to 2 counts, 2 scores = 3 to 5 counts, 3 scores > 5 counts), WMHs (0 score = 0, 1 score = 1 count, 2 scores = 2 counts, 3 scores = 3 counts), and CMBs (0 score = 0, 1 score ≥1 count), ranging from 0 to 7. The severity of CSVD burden was classified as none (0 point), mild (1 point), and moderate-severe (2–3 points) according to simple CSVD scores.
Assessment of neuropsychiatric syndromes
The presence and severity of NPS in ADNI were evaluated by Neuropsychiatric Inventory (NPI) [17], which is the most generally accepted clinical tool to assess the neuropsychiatric symptoms [18]. The NPI was evaluated by the caregivers of the participants. NPI covers 12 domains of behavioral and neurovegetative symptoms, of which each contains four items–presence, severity, frequency, and caregiver distress. The score of each domain (0–12 points) was calculated by symptom frequency (0–4 points) multiplied by severity (0–3 points) [17]. Total scores range from 0 to 144. The 12 symptom domains have been frequently categorized into four subsyndromes: hyperactivity (including aggression, euphoria, disinhibition, irritability, and aberrant motor behaviors), psychosis (including delusion, hallucination, and night-time behavior disturbances), affective symptoms (including depression, and anxiety), and apathy (including apathy and appetite and eating abnormalities). We used the data from the first NPI evaluation of participants as the baseline NPI data.
Statistical analysis
We normalized and standardized the NPS and its subsyndrome scores before analysis. However, the data were still non-normal distributed. Therefore, the difference in the baseline characteristics was assessed by the Wilcoxon test for continuous variables and the chi-square test for categorical variables. First, we evaluated the cross-sectional associations of CSVD burden and its markers with neuropsychiatric symptoms. Meanwhile, we assessed the longitudinal associations of baseline CSVD burden and its markers with the change rates of NPS. Considering the close relationships of cognition with CSVD and NPS, cognitive diagnosis was not included as a covariate. The linear mixed-effects (LME) models had random intercepts and slopes for time and an unstructured covariance matrix for the random effects, and they included the interaction between time (continuous) and the independent variables (CSVD burden, its severity, and markers) as predictors. In Model 1, covariates included age, gender, education, and APOE ɛ4 status. In Model 2, covariates included hypertension, hyperlipemia, diabetes, coronary heart disease, smoking status, alcohol drinking status, and the covariates in Model 1.
Next, we evaluated the severity of CSVD burden and its markers and tested the relationships of them with NPI total scores and neuropsychiatric subsyndromes in LME models. Bonferroni corrections were used for multiple comparisons (p < 0.0125).
The statistical analysis and figure preparation were conducted using R version 4.0.3 and SPSS software version 25. Statistical significance was defined as p < 0.05. The “arm”, “lme4”, and “ggplot2” packages in R 4.0.3 software were used to carry out the above analyses.
RESULTS
Characteristics of study participants
Table 1 showed the baseline demographic characteristics of the study participants in different subgroups stratified by the severity of CSVD. There were differences in age (p < 0.0001) and hypertension (p = 0.0040) between different groups. However, there was no significant difference in hyperlipemia, diabetes, coronary heart disease, smoking status, alcoholic drinking status, and educational level among the three groups. After Bonferroni corrections, we found no difference among the three groups in the scores of NPI and its subsyndromes (Fig. 1). The baseline demographic characteristics of the study subjects in subgroups stratified by the presence of CSVD were shown in Supplementary Table 1.
Demographic characteristics of study participants at baseline
p values of group comparisons were obtained using the Kruskal-Wallis test or chi-square test. CSVD, cerebral small vessel disease; NPI, Neuropsychiatric Inventory.

The variance of groups in NPI, hyperactivity, psychosis, affective symptoms, and apathy scores according to the severity of CSVD. NPI scores were higher in the moderate-severe CSVD group (A). No variance was performed on hyperactivity (B), psychosis (C), affective symptoms (D), and apathy (E) scores in different severities. NPI, Neuropsychiatric Inventory; CSVD, cerebral small vessel disease.
Associations of CSVD burden and neuropsychiatric symptoms at baseline
We found affective symptoms were associated with CSVD amended score (β= 0.1134, p = 0.0309) at baseline, as shown in Table 2. However, the associations were not significant after Bonferroni corrections.
Baseline and longitudinal change rates of neuropsychiatric symptoms with CSVD burden in linear mixed-effect model 2
Model 2, adjustment for age, gender, APOE ɛ4, education, hypertension, hyperlipemia, diabetes, coronary heart disease, smoking status, and alcohol drinking status. CSVD, cerebral small vessel disease; NPS, Neuropsychiatric symptoms; WMHs, white matter hyperintensities; CMBs, cerebral microbleeds; LIs, lacunar infarcts.
Associations of CSVD burden with longitudinal rates of change in neuropsychiatric symptoms
In this study, we found there were significant longitudinal associations of simple CSVD scores with change rates of NPS (β= 0.3813, p < 0.0001), hyper-activity (β= 0.1475, p = 0.0006), affective symptoms (β= 0.0610, p = 0.0091), and apathy (β= 0.1359, p < 0.0001) of the overall participants in LME model 1. Similarly, baseline amended CSVD scores showed significant associations with the change rates of NPS (β= 0.1966, p = 0.0002), hyperactivity (β=0.0839, p = 0.0006), affective symptoms (β= 0.0302, p = 0.0233), and apathy (β= 0.0655, p = 0.0002). Neither simple CSVD scores (β= 0.0296, p = 0.2579) nor amended CSVD scores (β= 0.0088, p = 0.5548) were related to psychosis. We also investigated whether there were longitudinal relationships of baseline LIs, WMHs, and CMBs with NPS and its subsyndromes. And we discovered that LIs had significant associations with the change rates of NPS (β= 0.9436, p = 0.0001), hyperactivity (β= 0.2961, p = 0.0092), psychosis (β= 0.1412, p = 0.0402), affectivity symptoms (β= 0.1505, p = 0.0156), and apathy (β= 0.3345, p < 0.0001). The presence of CMBs is positively related to apathy (β= 0.1366, p = 0.0141). WMHs (Fazekas score) were associated with hyperactivity (β= 0.0491, p = 0.0377) and apathy (β= 0.0359, p = 0.0346). Results showed that CSVD burden and its markers could predict the progression of neuropsychiatric symptoms, and different markers of CSVD were related to specific neuropsychiatric subsyndromes. After Bonferroni corrections, the associations of simple CSVD score with NPI total score, hyperactivity, affective symptoms, and apathy are still significant, and LIs still had associations with NPI total scores and hyperactivity.
The presence of CSVD at baseline tended to cause more serious NPS (β= 0.5907, p = 0.0002, Fig. 2A), hyperactivity (β= 0.2190, p = 0.0028, Fig. 2B), and apathy (β= 0.1688, p = 0.0012, Fig. 2C) compared to non-CSVD group.
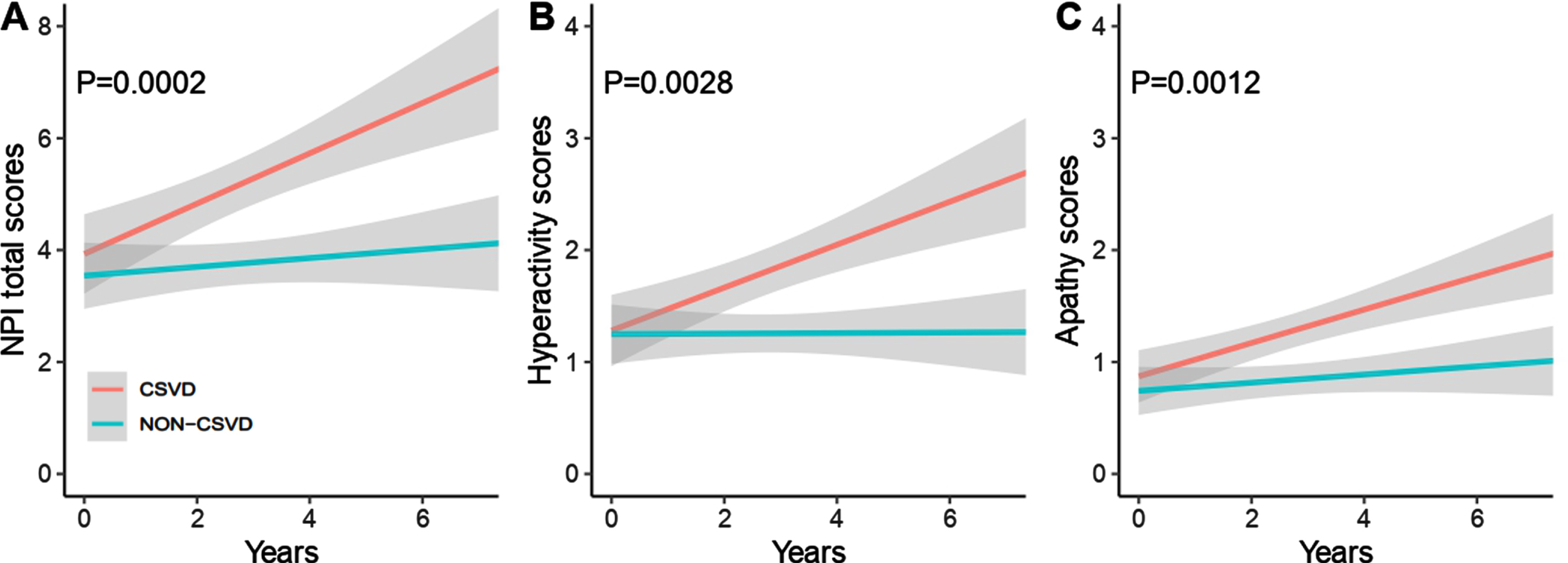
Presence of CSVD associated with neuropsychiatric subsyndromes progressions in multiple linear mixed-effects model 1. The presence of CSVD predicts more severe NPI (A), including hyperactivity (B), and apathy (C) scores. CSVD, cerebral small vessel disease; NPI, Neuropsychiatric Inventory.
The results barely changed in the sensitive analyses (Table 2), which proved that our results were robust. The associations of baseline variables with longitudinal NPS and its subsyndromes were presented in Supplementary Table 3.
The severity of baseline CSVD burden and longitudinal change rates of neuropsychiatric symptoms
There were no correlations between the severity of CSVD and NPS as well as its subsyndromes at baseline (Supplementary Table 2). We analyzed the longitudinal associations between the baseline severity of CSVD burden and change rates of neuropsychiatric subsyndromes (Table 3). Significant associations were found of the severity of CSVD burden and markers with change rates of neuropsychiatric symptoms. In Model 1, compared to non-CSVD participants, mild CSVD participants showed progression in NPI total scores (β= 0.4588, p = 0.0082) and affective symptoms (β= 0.1055, p = 0.0146). Compared with non-CSVD individuals, moderate-severe CSVD was also significantly associated with the progression of NPS (β= 0.8340, p = 0.0001), hyperactivity (β= 0.3167, p = 0.0014), and apathy (β= 0.3212, p < 0.0001). In Model 2, the two associations were still significant, as shown in Table 3.
Baseline severity of CSVD associated with longitudinal change rates of neuropsychiatric subsyndromes in linear mixed-effect models
Model 1, adjustment for age, gender, APOE ɛ4, and education; Model 2, Model 1 + hypertension, hyperlipemia, diabetes, coronary heart disease, smoking status, and alcohol drinking status. CSVD, cerebral small vessel disease; NPS, Neuropsychiatric symptoms.
Then we found that change rates of NPS (β=0.9948, p = 0.0001; β= 0.9899, p < 0.0001), hyperactivity (β= 0.3374, p = 0.0036; β= 0.3366, p =0.0037), affective symptoms (β= 0.1622, p = 0.0104; β= 0.1619, p = 0.0104), and apathy (β= 0.3298, p = 0.0001; β= 0.3280, p < 0.0001) were dependent on moderate-severe LIs in Model 1 and 2 (Supplementary Table 4). We found mild WMHs were related to increases in NPS (β= 0.6294, p = 0.0003; β= 0.6266, p = 0.0004), hyperactivity (β= 0.3136, p = 0.0001; β= 0.3126, p = 0.0001), and apathy (β= 0.1486, p = 0.0100; β= 0.1480, p = 0.0103) in Model 1 and 2 (Supplementary Table 5). However, mild LIs and moderate-severe WMHs were irrelevant to neuropsychiatric subsyndromes.
DISCUSSION
In the present study, the consequences are consistent with our initial hypothesis that baseline CSVD burden may be associated with change rates of NPS and its subsyndromes, including progression in hyperactivity, affective symptoms, and apathy among the non-demented elderly. Our cross-sectional study showed that there was no difference among the three groups in the scores of NPI and its subsyndromes. Longitudinally, baseline CSVD burden could predict the development of neuropsychiatric symptoms in the non-demented elderly in the future.
When we assessed the associations of WMHs, CMBs, and LIs with NPS and its subsyndromes, we found that baseline LIs could predict deterioration of NPS and all its subsyndromes. However, baseline WMHs and CMBs were only related to specific neuropsychiatric subsyndromes. WMHs were related to hyperactivity and apathy. CMBs were only associated with apathy. After being graded by severity, the moderate-severe LIs and mild WMHs could be clinical indicators for specific neuropsychiatric symptoms. When we analyzed the differences between groups, we found there was a more obvious progression in the CSVD group in the following years. Our study found that there’s no relevance between CSVD burden and psychosis and this is consistent with a previous study that never found an association of cerebrovascular risk factors with delusion and hallucination [14]. The possible reason is that various neurotransmitters are involved in occurrence of psychosis [19].
A previous study of 170 participants illustrated that CSVD progression could predict worsened neuropsychiatric symptoms and cognitive decline [13]. At the same time, a large number of studies showed CSVD had a strong correlation with memory and executive dysfunction in patients with dementia [20–22]. Moreover, some studies also demonstrated that NPS were related to executive function impairment in patients with dementia [23, 24], suggesting that NPS were a precursor to dementia. Therefore, it is meaningful to explore the correlation whether CSVD could be a candidate predictor of NPS.
According to a previous study, simple CSVD scores can better predict dementia in CSVD compared to amended CSVD scores [6]. This finding suggests that CSVD burden is a powerful neuroimaging tool for tracking neuropsychiatric symptoms. The significance of this study is to find a noninvasive neuroimaging method to assess the development of NPS in older adults without dementia. CSVD burden can be achieved via neuroimaging, which is relatively noninvasive compared to plasma and cerebrospinal fluid.
Mild behavior impairment is also a construct to describe the neuropsychiatric symptoms tailored for pre-dementia populations [25]. A Singapore study showed that diabetes may be a risk factor for mild behavioral impairment [26]. However, there is also research concluded that mild behavior was unrelated to CSVD burden and its risk factors [27, 28].
Key factors of CSVD etiology are hypertensive angiopathy and cerebral amyloid angiopathy (CAA). Hypertension mainly affects the vessels in deep brain regions, and CAA primarily affects cortical vessels by the deposition of amyloid-β peptide in the wall of vessels introducing hemorrhagic or ischemic results [29]. Risk factors of CSVD include an unmodifiable factor (age) and acquired factors [30]. The acquired factors contain hypertension, hyperlipemia, diabetes, smoking, chronic kidney disease, and obstructive sleep apnea [30–33]. This research also showed the necessity to control or remove the risk factors of CSVD for preventing neuropsychiatricsymptoms.
The underlying pathological mechanisms about the associations of CSVD burden with NPS are still not clear. The vascular depression hypothesis postulates that CSVD burden gives rise to neuropsychiatric symptoms by disruption of deep and cortical brain structures or their connecting pathways involved in mood regulation [34]. Research has shown that microbleeds disrupt the structural and functional connectivity of the cerebral network and further influence the efficacy of transmitting and integrating information [35–37]. WMHs interrupt the neuronal network of frontal-subcortical circuits through cerebral hypoperfusion, which causes the abnormality of emotion and behavior [38]. The possible mechanism is that the CSVD burden leads to the degeneration of neurons, which subsequently induces focal injuries or aggravates the decrease in global brain connectivity [39, 40], finally influences the functional network associated with neuropsychiatric symptoms [41, 42]. Zhao et al. found that hyperactivity was associated with the abnormality of the right inferior temporal region [43]. Buren et al. got the conclusion that apathy was related to the change in the volume in the prefrontal cortex and basal ganglia [44]. Tang et al. showed that multiple CMBs, especially lobar CMBs, were associated with high NPS burden, particularly depression and disinhibition [45]. These results are consistent with a study that testified a modest significant inverse correlation between CSVD burden and global network efficiency. And it also reported among the markers of CSVD, global network efficiency was related to WMHs [46]. The pathological mechanism of small vessels and cerebral injury is still not clear. Maybe CSVD represents potential pathology, such as the change of capillary patency and blood viscosity [47]. Higher CSVD burden means more severe and extensive macrovascular injuries, which may affect neuropsychiatric symptoms. The influences of the varying severity of WMHs and LIs on neuropsychiatric subsyndromes were inconsistent.
There are some limitations in this study. First, it took a long time to track the progression of neuropsychiatric symptoms after the appearance of CSVD. Further studies should focus on more accurate associations among CSVD burden, neuropsychiatric symptoms, and cognition. Second, the data on perivascular spaces and brain atrophy were not concluded in ADNI. Thirdly, ADNI mainly includes MCI patients. Therefore, ADNI participants are more prone to Alzheimer’s disease. Finally, the NPI was finished by the caregivers and the assessment was subjective to some extent, especially when the caregivers suffered the pain from caring.
In conclusion, CSVD burden, especially LIs, was associated with change rates of neuropsychiatric subsyndromes in people without dementia. Therefore, simple CSVD scores could be a neuroimaging approach to tracing the neuropsychiatric symptoms. This study also suggests the importance of monitoring and controlling vascular risk factors.
Footnotes
ACKNOWLEDGMENTS
This study was supported by grants from the National Natural Science Foundation of China (91849126, 81971032, and 81801274), the National Key R&D Program of China (2018YFC1314700), ZJLab, Shanghai Center for Brain Science and Brain-Inspired Technology, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University.
Data collection and sharing for the ADNI data section was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.