
Abstract
Background:
The identification and understanding of the discrepancy between caregivers’ reports of people with dementia’s (PwD) performance of activities of daily living (ADLs) and observed performance, could clarify what kind of support a PwD effectively needs when completing tasks. Strategies used by caregivers have not been included in the investigation of this discrepancy.
Objective:
To (1) investigate if caregivers’ report of PwD’s ADL performance are consistent with PwD’s observed performance; (2) explore if caregiver management styles, depression, and anxiety, contribute to this discrepancy.
Methods:
PwD (n = 64) were assessed with standardized performance-based (Assessment of Motor and Process Skills, AMPS) and informant-based (Disability Assessment for Dementia, DAD) ADL assessments. Caregivers completed depression (PHQ-9), anxiety (GAD-7), and dementia management style (DMSS: criticism, active-management, and encouragement) questionnaires. Cohen’s kappa determined agreement/disagreement in ADL performance. To investigate the potential discrepancy between the DAD and AMPS, a continuous variable was generated: comparative ADL score. Multiple linear regression analysis explored whether caregivers’ management styles, depression or anxiety could explain the ADL discrepancy.
Results:
Poor level of agreement between observed and reported ADL performance [k = –0.025 (95% CI –0.123 –0.073)] was identified, with most caregivers underestimating ADL performance. The combined model explained 18% (R2 = 0.18, F (5,55) = 2.52, p≤0.05) of the variance of the comparative ADL score. Active-management (β= –0.037, t (60) = –3.363, p = 0.001) and encouragement (β= 0.025, t (60) = 2.018, p = 0.05) styles made the largest and statistically significant contribution to the model.
Conclusion:
Encouragement style could be advised for caregivers who underestimate ADL performance, while active management style for those who overestimate it. Findings have scope to increase caregivers’ abilities to support PwD activity engagement in daily life.
INTRODUCTION
The assessment of performance of activities of daily living (ADLs) for people living with dementia relies mostly on the caregiver’s report through widely used informant-based questionnaires [1]. As a result, decisions about the type and amount of support the caregiver provides to the person with dementia (PwD) are mainly based on the caregiver’s appraisal of the PwD’s ADL performance [2]. Although informant-based assessments are affordable and easy to administer [1], certain caregiver-related factors [3] have been shown to affect their appraisal of the PwD’s everyday functioning. Performance-based ADL assessments, on the other hand, require that the PwD performs day-to-day activities during the assessment, thus allowing clinicians and researchers to objectively observe and evaluate the individual’s task performance, but they are costly [4].
The World Health Organization (WHO) launched The International Classification of Functioning, Disability and Health (ICF) [5] recognizing the importance of gathering individual’s information about performance of activities and their potential abilities to carry them out. Identifying the discrepancy between reported and observed ADL performance could be the first step in recognizing the type of support a caregiver provides when a PwD performs a task, and which type of guidance caregivers may need. As such, several studies have identified discrepancies between the ADL performance [6–8]; however, gaps in knowledge remain. It is not known how extrinsic potentially modifiable factors affect this discrepancy in ADL performance and, importantly, the type of support the PwD may need when performing daily tasks.
Research into the discrepancy between ADL performance, as reported by the caregiver, and a standardized observed performance, has shown contradictory results. On one hand, some studies found that caregivers underestimate the PwD’s performance of ADLs [8], while others reported that caregivers overestimate what the PwD could do [6, 9]. Among factors associated with the caregivers’ appraisal of ADL performance, PwD’s higher level of cognition—an intrinsic factor, seemed to contribute to caregivers’ overestimation of ADL performance [6, 9].
Certain caregiver variables have also been associated with the discrepancy in ADL performance, such as caregiver burden [10, 11] and caregiver depression [7]. For example, caregivers who present with higher levels of burden tend to underestimate ADL performance [11]. Studies examining caregiver depression have shown varied results: a study found that caregivers with clinical depression underestimated ADL performance [7], while another found no associations between the caregiver’s appraisal of ADL performance and caregiver’s level of depression [6]. In addition, even though caregivers’ level of anxiety is a prevalent problem experienced by caregivers of PwD [12], little is known about the role it plays in the way caregivers report ADL performance.
Another possible factor that could influence the way caregivers report ADL performance is the management style that caregivers use daily, when dealing with dementia-related issues. Different styles have been identified, including criticism, active management, and encouragement styles [13]. Criticism describes a caregiver who yells, criticizes, and threatens the PwD. Active management includes engaging the PwD, stimulating and assisting them while encouragement refers to a caregiver who would praise the PwD using an emotional-based approach to solve problems. A recent study showed how the caregiver’s use of criticism and encouragement styles affected PwD’s ADL performance [14]. However, it is still unclear how caregiver management styles may influence the discrepancy between reported and observed performance. Investigating the role of caregiver management styles would contribute to our understanding of the type of support the PwD needs when completing daily activities.
The main goals of this study were to determine if 1) there is a discrepancy between PwD’s ADL performance as reported by their caregivers and a standardized observed performance. In addition, the study explored whether 2) caregiver management styles and the caregivers’ level of depression and anxiety have an effect on this ADL performance discrepancy.
METHODS
This was a cross-sectional exploratory study that followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations [15] to design and report the results of this study.
Participants and procedures
Participants included in this study were originally recruited to the parent project, TASKed, from September/2016 to July/2019 (n = 366). This project was a four-year long umbrella study funded by the Alzheimer’s Society and sponsored by the University of East Anglia, in England. Inclusion criteria comprised a diagnosis of dementia, according to the DSM-V [16] and the PwD had to be able to perform at least two daily tasks without help, such as washing their hands, brushing their teeth, or making a hot drink. Caregivers had to be a family member of the PwD, be older than 18 and be fluent in English and be providing more than seven hours of care per week.
PwD and their caregivers (dyads) were initially visited at home as part of the TASKed study and completed several questionnaires and assessments, including an informant-based interview on PwD’s performance of ADLs. All PwD were invited to complete a performance-based ADL assessment and, if they agreed to it, the assessment was carried out at their own home within six months of the first TASKed visit. Performance-based assessments were video recorded to enable scoring by two independently trained raters (JC and APT). Only PwD and caregivers who completed both the ADL informant-based interview (Disability Assessment for Dementia, DAD) and the performance-based ADL assessment (Assessment of Motor and Process Skills, AMPS) were included in the study. Sixty-eight PwD and their caregivers (n = 68 dyads) were eligible for inclusion. From these, four dyads were excluded because no comparable data across assessments was available (e.g., meal preparation tasks evaluated in the AMPS had not been evaluated with the DAD), leaving a total sample of 64 dyads for the analyses. All these participants were included in Sample 1. A smaller sample was used (Sample 2) for the second research question, as there was some missing data for the caregiver’s depression and anxiety measures (n = 61).
Ethical considerations
Ethics approval was obtained through the national Health Research Authority (IRAS 199002, REC 16/LO/0544). Participation was voluntary and both PwD and caregivers’ consent was gained before the assessments were conducted.
Assessments
Demographic information for both the PwD and the caregivers was documented, including PwD’s age, gender, level of education, length of symptoms, marital status, and living situation. Caregiver’s age, gender, education, and relationship with the PwD were also recorded.
The AMPS [17] was used to assess ADL performance using direct observation of daily activities. The AMPS is a performance-based assessment of two tasks that can be selected from a list of more than 100 cross-cultural standardized activities. After the observation is completed, the performance of the participant is scored using 35 items. The raw scores are then entered into a computer program that converts them into linear measures using a Rasch model approach [17]. Two main logit scores are given: process skills and motor skills. The process skills score was used for the analyses due to the cognitive nature of its items. To check for inter-rater-reliability, 20% of the AMPS evaluations were scored by a second trained occupational therapist (OT) (APT), blind to the first set of scores (JC) (See more information in the Supplementary Material). Caregivers were not present during the AMPS assessment. In older adults with cognitive impairment, the AMPS has shown excellent test/retest reliability (Motor: r = 0.88 –0.9; Process: r = 0.86 –0.87) [18]. In this study, the AMPS process score was used to refer to observed ADL performance and was called ‘AMPS performance score’, which refers to the ability to perform activities.
The DAD [19] was used to assess ADL performance as reported by the caregiver. The DAD is an informant-based assessment which provides information about both personal care tasks and more advanced tasks, such as meal preparation, medication management and going out. The DAD consists of ten subdomains, including hygiene, dressing, continence, eating, meal preparation, telephoning, going out, finances and corresponding, medications and leisure and housework. Each subdomain contains different steps or components of the task. The items of the form are presented as questions and the scoring system offers three answers: yes (1), no (0) and not applicable (these exclude tasks that had never been performed by the person before the onset of dementia). The subdomain scores were converted to an individual percentage according to the number of subtasks of the subdomain the PwD still completes (yes = 1) or does not (no = 0). Higher scores on the DAD indicates better ADL performance. The DAD has shown to have high degree of internal consistency (Cronbach’s α= 0.96) and excellent interrater (ICC = 0.95) and test-retest (ICC = 0.96) reliability [19]. In this study, DAD subdomain scores were used to refer to the ADL performance as reported by the caregiver and called ‘DAD performance score’, which refers to the performance of activities.
Other instruments
The Frontotemporal Dementia Rating Scale (FRS) [20] was used to categorize PwD in regard to dementia severity [21]. The FRS is an interview questionnaire which comprises 30 items related to everyday functioning and behavioral symptoms. Items are scored as 0 (all the time and sometimes) and 1 (never). The FRS has been shown to detect disease progression also in other dementias [22], confirming suitability for use in this study. The FRS categories ‘very mild’ and ‘mild’ were combined, and so were the categories ‘severe’, ‘very severe’ and ‘profound’, resulting in three main categories of interest for this study: mild, moderate, and severe. The FRS has shown excellent internal consistency (Cronbach’s α= 0.93) and high interrater agreement (ICC = 0.99) [20].
The Dementia Management Strategies Scale (DMSS) [13] was used to identify caregivers’ management styles. This self-complete questionnaire contains 28 items that characterize three different styles of management when dealing with dementia-related problems: criticism, active management, and encouragement. Items are scored on a frequency scale that ranges from never to most of the time. Each style can be assessed independently. For this study, scores of each style were converted to a percentage to enable comparison between styles. Each style’s internal consistency was reported separately, where criticism’s Cronbach’s α was 0.85, active management’s Cronbach’s α was 0.77 and encouragement’s Cronbach’s α was 0.80 [13].
The Patient Health Questionnaire (PHQ-9) [21] was used to measure symptoms of depression. The scale comprises nine items that evaluate symptoms of depression over the previous two weeks. The items range from 0 (not at all) to 3 (nearly every day). Lower scores represent lower levels of depression, with scores between 5–9 considered mild depression, scores between 10–14 considered moderate depression and scores higher than 15 considered moderately severe to severe depression [21]. The PHQ-9 has shown excellent internal reliability (Cronbach’s α= 0.89) and excellent test re-test reliability (ICC = 0.94) [21].
The Generalized Anxiety Disorder questionnaire (GAD-7) [22] was used to assess and measure the frequency and severity of anxiety symptoms. The scale contains seven items with options that range from 0 (not at all) to 3 (nearly every day). Higher scores denote higher levels of anxiety, with scores higher than 16 considered severe anxiety, scores between 11–15 considered moderate anxiety and scores between 6–10 considered mild anxiety [22]. The GAD-7 has shown excellent internal consistency (Cronbach’s α= 0.92) and good test re-test reliability (ICC = 0.83) [22].
Data analyses
Statistical analyses were performed using the Statistical Package for the Social Sciences program (SPSS version 25, IBM Corp., Armonk, NY, USA). The statistical significance level was set at 0.05.
To characterize the sample, descriptive statistics were performed on demographic and clinical measures. Independent-samples t-test was used for comparison of continuous variables, while Chi-square test was used for categorical variables.
To investigate if there was discrepancy between the informant-based ADL assessment (DAD), which records ADL performance as reported by the caregiver, and the performance-based (AMPS) assessment, which entails the observation of ADL performance, a new continuous variable was created, named comparative ADL score. In this first step, each individual comparative ADL score created was a result from the comparison and subtraction between the AMPS and the DAD performance scores (see Table 1). Thus, the AMPS performance score, which comprises the observation of the performance of two tasks, was compared to the subdomain score of the DAD, which is equivalent to the two tasks that were observed with the AMPS. For example, when the PwD performed two kitchen-based tasks for the AMPS, the subdomain ‘meal preparation’ of the DAD was used in the generation of the comparative ADL score. Table 1 describes the score comparison used between both the AMPS and the DAD performance scores, to generate the comparative ADL score for each participant. Both these instruments measure two different constructs of activities of daily living. For the purpose of this study, and following the ICF classification [5], the DAD is used to record what a person does in their daily routine, while the AMPS is used to measure potential ability to complete activities.
Table with stratification of impairment on ADL performance and score comparison used to analyze consistency between performance as reported by the caregiver (DAD) and performance scored using direct observation of tasks (AMPS)
Table with stratification of impairment on ADL performance and score comparison used to analyze consistency between performance as reported by the caregiver (DAD) and performance scored using direct observation of tasks (AMPS)
ADL, activities of daily living; DAD, Disability Assessment for Dementia: informant-based assessment; AMPS, Assessment of Motor and Process Skills: performance-based assessment. *AMPS’ cut-off 1.0 [17].
It was then established whether there was overestimation, underestimation, or perfect agreement between the informant-based and the performance-based assessments. Overestimation was determined when the ADL performance score reported by the caregiver was better than the ADL performance observed. For example, if the participant scored 100% in the DAD (no change in ADL performance) and obtained a score between 0 to 0.9 in the AMPS (marginal to mild ADL impairment) their comparative ADL score was 1 (Table 2). Agreement was determined when the same level of ADL impairment was reported by the caregiver and during the observation of the same tasks. As such, when a participant obtained the same ADL score in both the AMPS and the DAD performance scores, the comparative ADL score was zero (0). Underestimation was determined when the ADL performance reported by the caregiver was poorer than the observed ADL performance (Table 2). For instance, if a participant scored between 70 to 99% in the DAD (marginal to mild ADL impairment) and scored more than 1.0 in the AMPS (no change in ADL performance) their comparative ADL score was –1. The range of scores in the comparative ADL score goes from +3 to –3. See Table 2 for more details. To determine the level of agreement, overestimation and underestimation of our cohort, Cohen’s Kappa was used.
Description of how each comparative ADL scores (overestimation, agreement and underestimation of ADL performance) were computed and clinical interpretation
ADL (Activities of daily living); DAD (Disability Assessment for Dementia; informant-based assessment); AMPS (Assessment of Motor and Process Skills; performance-based assessment).
To investigate if there was a relationship between the severity of dementia and the comparative ADL score, Spearman’s rank order correlation was applied.
Thereafter, multiple linear regression analysis, enter method, was used to investigate which factors may influence the discrepancy between observed and reported ADL performance. The new comparative ADL score was used as the dependent variable and caregiver management styles (criticism, active management, and encouragement), caregivers’ level of depression and anxiety, were used as independent variables in the regression model.
To examine agreement between raters (JC and APT) on the AMPS assessment, Intraclass Correlation Coefficient (ICC) [23], two-way mixed models, absolute agreement, was determined. Raters reached excellent agreement for AMPS Process Skills scores (0.967 with a 95% CI from 0.895 to 0.990 (F (12,12) = 29.272, p≤0.000). For the Motor Skills scores, good agreement was reached (0.877 with a 95% CI from 0.611 to 0.962 (F (12,12) = 8.094, p≤0.000).
The sample size calculation for a regression analysis included three caregiver management styles, caregiver depression and caregiver anxiety as independent factors. The power calculation used R-squared increase [24]. The minimum sample size required, in order to achieve a power level of 0.80, a significance level of 0.05, and a medium effect size of 0.15 was 55.
RESULTS
Demographics
PwD were on average 77 years old, mostly male, married, and lived with their family. PwD were mostly in the severe stage of the disease (53.1%), followed by those in the moderate stage (37.5%); they had an average of four years of disease duration (Table 3).
Demographic characteristics and clinical variables of the whole sample and grouped by dementia stage. Comparisons were done between moderate and severe stages; mild group not included due to small sample. SD in brackets
Demographic characteristics and clinical variables of the whole sample and grouped by dementia stage. Comparisons were done between moderate and severe stages; mild group not included due to small sample. SD in brackets
Activities of Daily Living (ADLs) were measured with the Disability Assessment for Dementia (DAD) and the Assessment of Motor and Process Skills (AMPS). Independent Sample t-test was used for continuous variables. χ2 Test was used for categorical variables. Statistically significant difference *p≤0.01. †Missing data for the length of symptoms (n = 60/64) and ADLs (DAD) (n = 63/64).
Caregivers were 72 years old on average, mostly female and were spouses of PwD. As a group, their average anxiety score fell under the category of ‘no anxiety’. Caregivers reported mild symptoms of depression (Supplementary Table 1). In addition, caregivers’ responses showed that they used an active management style (71.4%) more frequently than encouragement (66.7%). None of them selected criticism style as their main approach when managing dementia-related problems (Fig. 1).
Do caregivers overestimate or underestimate the person with dementia’s ADL performance?
The majority of caregivers underestimated PwD’s performance of ADLs, as they reported poorer performance when compared with the score obtained during the observation of the same tasks (71.9%). Less than a quarter of caregivers overestimated PwD’s performance of ADLs (17.2%), i.e., reporting better ADL performance than the one actually observed. Finally, only 10.9% of caregivers reached perfect agreement between ADL performance scores, where caregivers’ report of ADL performance (DAD) was at the same level as the one obtained during the observation of the tasks (AMPS). As such, Cohen’s kappa [k = –0.025 (95% CI –0.123 –0.073)] indicated a poor level of agreement between DAD and AMPS performance scores.
Overall, caregivers from the agreement, overestimation or underestimation groups were similar. There were no significant differences between the comparative ADL score on the age of the caregiver, relationship with the PwD, caregiver’s level of depression and anxiety. Supplementary Table 1 describes demographics and clinical variables of PwD, and their caregivers grouped by overestimation, agreement, or underestimation of ADL performance. In addition, there was no significant association between the comparative ADL score and the dementia severity (Rs (61] = 0.216, p = 0.089).
Preliminary analyses were conducted to ensure that assumption of normality, linearity and homoscedasticity were met. Visualisation of the Normal P–P Plot and the scatterplot of the standard residuals, suggest that these assumptions were not violated. Tolerance and VIF’s values were all within accepted limits, confirming that multicollinearity was not a concern. Outliers were also checked using Mahalanobis and Cook’s distances. Mahalanobis distance scores (MD = 17.42) were below its critical value of 20.52 for five independent variables [25], and Cook’s distance value was below one (Di = 0.25) thus, we can conclude that no outliers were found within our data.
Five factors were included in the regression model: the three caregiver management styles, caregiver depression, and caregiver anxiety. The comparative ADL score was used as the dependent variable. Further information can be found in the Supplementary Material.
This overall model comprising the three caregiver styles, caregiver depression and caregiver anxiety, explained 18% (R2 = 0.18, F (5,55) = 2.52, p≤0.05) of the variance of the comparative ADL score. Active management (β= –0.037, t (60) = –3.363, p = 0.001) and encouragement (β= 0.025, t (60) = 2.018, p = 0.05) styles were the two factors that made the largest and statistically significant contribution to the model (Table 4).
Independent variables included in the multiple regression analysis. Dependent variable: comparative ADL score (Sample 2: n = 61)
F (5,55) = 2.52, p≤0.05, R2 = 0.18; Df for the T column is 56. β represents the standardized regression coefficients. Depression was assessed with the PHQ-9 (Patient Health Questionnaire). Anxiety was assessed with the GAD-7 (Generalized Anxiety Disorder). Criticism, active management, and encouragement are the three caregiver’s styles described in the DMSS (Dementia Management Strategies Scale).
For each point that the caregivers scored on the active management subscale, the comparative ADL score decreased by 0.4%. This indicates that the use of active management strategies may decrease the comparative ADL score along the scale. For each point that the caregivers scored on the encouragement subscale, the comparative ADL score increased by 0.25%. This means that the more the caregiver uses encouragement style, the more the comparative ADL score increases along the scale.
To facilitate clinical interpretation of the findings, Fig. 1 was created, and examples are described next. For instance, if a caregiver’s comparative ADL score was –3 (underestimation, bottom of y axis), this caregiver could use more encouragement strategies in order to get closer to ADL agreement, and to reduce the gap between reported and observed ADL performance. If the caregiver’s comparative ADL score was +3 (overestimation, top of y axis), this caregiver could use more active management strategies to reduce the comparative ADL score and move closer to zero, i.e., ADL agreement.
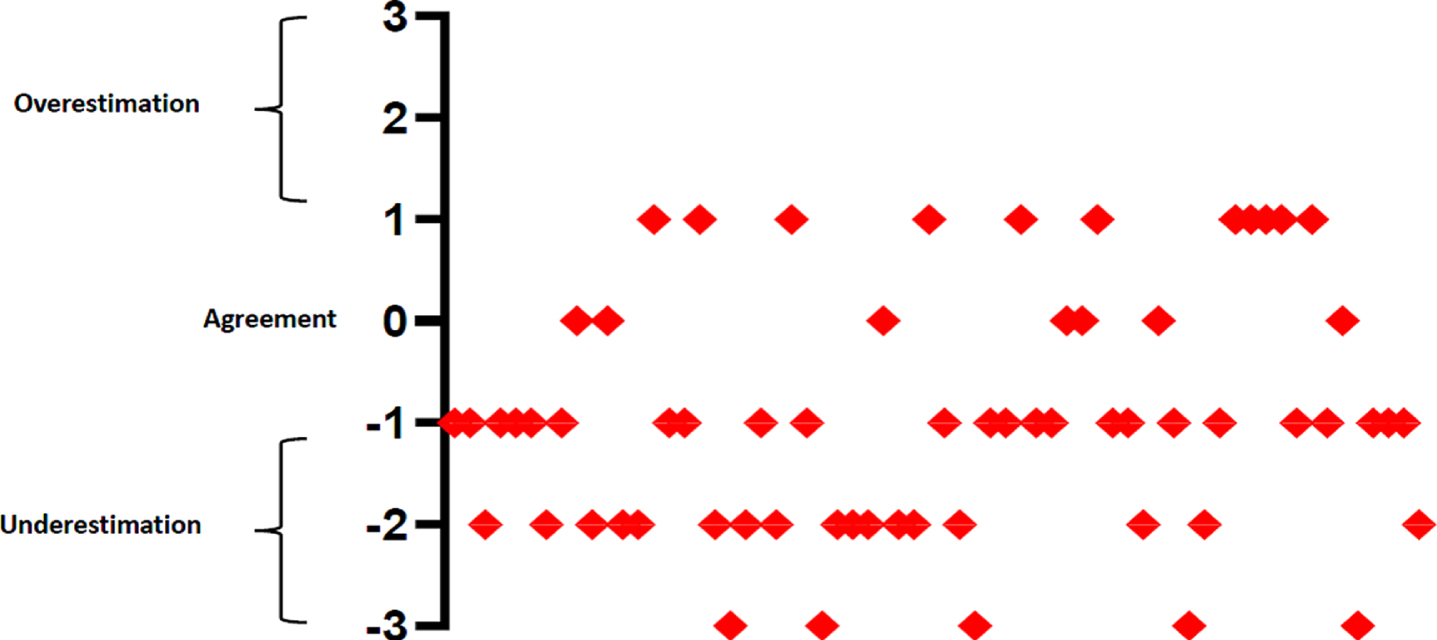
Distribution of caregivers according to their comparative ADL score, to facilitate clinical interpretation of results of the regression analysis. Each caregiver is represented as a red diamond on the figure above (n = 61). Y axis represents the comparative ADL score. X axis represents the caregivers. Overestimation occurred when the ADL performance reported by the caregiver was better than the one observed. Agreement was reached when the participant obtained the same ADL performance as reported by the caregiver and the observed. Underestimation occurred when the performance reported by the caregiver was poorer than the one observed.
DISCUSSION
This original study investigated the discrepancy between PwD’s ADL performance as reported by the caregiver, and the observed ADL performance, while introducing novel caregiver-related factors to investigate what influences this discrepancy. Two main findings arose: the level of agreement between the caregiver’s appraisal of ADL performance and the observation of the same tasks was low; and the strategies that caregivers use daily when dealing with dementia-related problems, namely the encouragement and active management styles, affected the identified discrepancy in ADL performance.
The majority of the caregivers in this study underestimated PwD’s ADL performance, reporting lower performance than the one observed during the completion of the same tasks. This is in accordance with other studies [8, 28] that used both informant and performance-based assessments and found that caregivers mostly underestimated PwD’s ADL performance. A possible explanation would be that family caregivers might require specific training to appropriately appraise PwD’s remaining abilities to perform ADLs. These difficulties progress slowly over time in dementia [29] and caregivers may be adapting to a situation without having enough information on how to enable the person with dementia to engage in activities of daily living for longer. As such, caregivers may report PwD’s ADL performance based on the help they provide instead of the real assistance that the PwD requires. This study suggests that the optimal support provided to the PwD could be identified if the caregiver is offered training on how to recognize the level of assistance a person needs.
The number of caregivers in this study who reached perfect agreement between reported and observed performance was quite small, i.e., caregivers reported the same level of ADL performance as the one that was formally observed during assessment. A possible reason why the agreement was low in this group of caregivers may have been related to the methodological differences between the performance-based assessment and informant-based questionnaire used in this study. For example, the PwD may be able to prepare a sandwich when observed but they may present with other difficulties when preparing a full cooked meal. Thus, the scores on the DAD may have been lower than the AMPS results due to the scoring system of the informant-based assessment. In future, studies comparing single tasks would contribute further to the understanding of the discrepancy of ADL performances. An important factor that could also affect the agreement between reported and the observed performance may lie in the fact that caregivers may need to provide constant motivation to the PwD for them to complete certain tasks. Future studies could target the dynamics that underpin the relationship between PwD and their caregivers.
Similarly, the proportion of caregivers who overestimated PwD’s ADL performance was also low in the current study. These caregivers reported that the PwD had a higher performance that the one observed during the completion of the same tasks. One possible reason may be that these caregivers minimized the difficulties the PwD had when carrying out daily tasks, or they may not have been present when the PwD performs tasks and are unable to identify difficulties. Another possible interpretation is that caregivers may think that the PwD’s everyday problems are not caused by the dementia-related decline and they may accept changes in day-to-day activities as part of other circumstances, including ageing itself.
Another important finding was that there were no differences among those caregivers who underestimated, reached an agreement, or overestimated ADL performance, in terms of their age and relationship with the PwD. This contrasts with other studies where it was found that discrepancy was higher if the informant was a spouse of the PwD [11]. In addition, dementia severity was not associated with the comparative ADL score. This is in agreement with other studies, where dementia severity did not affect the difference between observed and reported performance [30]. This finding suggests that potential interventions to promote independence in dementia could be applied in all stages of dementia.
The use of the caregiver styles affected the comparative ADL score in different directions (i.e., overestimation or underestimation) and this may be explained by the type of strategies these styles comprise. Caregivers using active management strategies take an active role stimulating and prompting their family member through the adaptation of the environment, repetition and anticipating problems and thus may underestimate PwD’s ADL performance. The strategies belonging to encouragement style, on the other hand, are based on an approach where caregivers praise the PwD and motivate them to discuss their feelings and to do activities for themselves, so perhaps overestimating PwD’s ADL performance. Therefore, the active management places the caregiver in an active and practical role, perhaps resolving all issues for the PwD before they have a chance to try resolving them, while the encouragement style characterizes a caregiver who focuses on an approach where the PwD is encouraged to resolve the issues by themselves before support is provided.
The criticism style did not affect the discrepancy between reported and observed ADL performance. This was a surprising finding given that the use of criticism style was found to negatively affect PwD’s performance of daily tasks [14]. One way to explain this finding may be that criticism strategies are based on communication-related interactions, rather than providing actual support, and therefore its use had no effect on the comparative ADL score. Another reason could be the fact that this sample of caregivers reported seldomly used criticism, which can explain why it did not affect the discrepancy between reported and observed performance.
Caregivers’ level of depression and anxiety had no effect on the comparative ADL score either. This can be attributed to the nature of the PwD’s performance of daily tasks which is based on how their skills are affected by intrinsic dementia factors [14] and extrinsic factors such as the environment [31], rather than on the way the caregivers feel. Other studies have published contradictory results on the way depression affected caregivers’ reports of ADL performance [6, 11] and, to date, none of those studies measured the effect of caregiver level of anxiety on the discrepancy between informant and performance-based measures. Furthermore, the low incidence of depression and anxiety in this cohort of caregivers may explain the lack of effect on the discrepancy between reported and observed ADL performance. Future studies could be conducted with caregivers with a different range of symptoms of depression or anxiety to investigate whether these affect the discrepancy between ADL performances.
One limitation of this study was the composition of the sample, which was comprised of PwD in the more severe stages of the disease. The investigation of everyday functioning in older adults in the mild stages of dementia and how their caregivers appraise ADL performance is an important area requiring further research. Investigating ADL changes early in the post-diagnostic phase may enable identification of the type of support the PwD needs, reducing underestimation or overestimation of caregivers when appraising ADL performance. It is also important to mention the methodological complexity of comparing two different elements of ADLs, namely performance (DAD) and ability (AMPS). We can only conduct this comparison by using two different types of ADL assessments, i.e., an interview-based questionnaire and a performance-based assessment. Finally, it needs to be acknowledged that our model explained 18% of the variance of the comparative ADL score, so future studies could investigate the role of other variables that may influence the discrepancy between reported and observed ADL performance in PwD.
Our results are promising for those working in the dementia field, as it highlights the prominent role of the styles that caregivers use when dealing with dementia-related problems on PwD’s ADL performance, and provide knowledge on how to improve caregivers’ skills to support independence for the PwD. Novel caregiver-based interventions and clinical advice should take into account the type of strategies caregivers use to enable optimal support for activity participation in dementia.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all our participants across the East of England. We are also grateful to our colleagues who collaborated with this study: Kayte Rowe, Emma Talbot, Lauren Wright, Zoe Inman, Prof. John O’Brien, Judy S. Rubinsztein, Gloria Calderon, Siobhan Rust, Rachel Winson, Allan Bregola, Chelsea Radakovic, Carmel Moore, Trish Boyton and Kaitlin Dudley. This work was supported in part by a grant awarded to EM for the TASKed Study, funded by the Alzheimer’s Society (AS-SF-241). JC is a recipient of a School of Health Sciences PhD Scholarship. APT is a recipient of an MND Scotland PhD Scholarship. TB is a recipient of an Alzheimer’s Society Fellowship. EM, JC and APT are also supported by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration East of England (NIHR ARC EoE) at Cambridge and Peterborough NHS Foundation Trust. The views expressed are those of the authors, and not necessarily those of the NIHR, NHS or Department of Health and Social Care.