
Abstract
Background:
Cognitive impairment is common in the elderly population. Exploring patterns of white matter damage at the microstructural level would give important indications for the underlying mechanisms.
Objective:
To investigate the spatial patterns of white matter microstructure and structural network alternations in relation to different cognition domains
Methods:
Participants from the community-based Shunyi Study were included to investigate the association between white matter measurements and cognition cross-sectionally, via both global and local analysis. Cognitive functions were assessed using digit span, trail making test (TMT)-A/B, Fuld object Memory, and 12-Word Philadelphia Verbal Learning Test (PVLT). White matter measurements including fractional anisotropy (FA), mean diffusivity (MD), and structural network parameters were calculated based on diffusion tensor imaging.
Results:
Of the 943 participants included, the mean (SD) age was 55.8 (9.1) years, and the mean (SD) education level was 6.7 (3.2) years. We found the whole set of cognitive measurements was related to diffused white matter microstructural integrity damage and lower global efficiency. Poor executive functions (TMTA/B complete time) were related to lower FA and higher MD predominantly on the anterior white matter skeleton, while verbal memory loss (PVLT test scores) was related to sub-network dysconnectivity in the midline and the right temporal lobe.
Conclusion:
The anterior brain is dominantly involved in executive dysfunction, while midline and right temporal brain disconnection are more prominent in verbal memory loss. Global and regional disruption of white matter integrity and network connectivity is the anatomical basis of the cognitive impairment in the aging population.
INTRODUCTION
Cognition impairment is common in the healthy elderly and poses a public health threat in light of the rapidly increasing aging population [1, 2]. Several theories were proposed that cognitive deficits in normal aging arise from alteration of subtle anatomical disconnection of cortical-subcortical linkages, known as the “disconnection” hypothesis [3]. Yet the detailed profile of white matter fiber bundle connectivity is difficult to measure in vivo. White matter hyperintensity (WMH) visible on conventional structural magnetic resonance imaging (MRI) has been long recognized as a sign of white matter macrostructural disruption [4]. However, the burden of WMH does not parallel cognitive deficits [5, 6], indicating the heterogeneity of its pathological texture and limitation on reflecting the anatomical basis of cognitive functions [7, 8]. Therefore, white matter damage at the microstructural level deserves investigation to reveal how white matter disconnection plays a role in the pathogenesis of cognitive impairment.
Diffusion tensor imaging (DTI), a promising tool measuring the diffusion properties of water molecules, provides measurements of white matter microstructural destruction [9]. In the elderly healthy population, decreased FA value is observed in widespread regions, especially in the frontal, parietal, and subcortical area [10], while their relationship with cognitive impairment is unexplored. Although regional alternations of diffusion metrics related to cognition have been found in patients with cerebral small vessel disease [6, 11] and Alzheimer’s disease [12], it has been barely discussed in a healthy aging population which deserves further investigation.
It has been recognized that, during executive and memory tasks, functional connections across broad brain regions are involved [13]. However, we still have no exact answer on where disconnection of white matter network leads to impairment of specific cognitive domains. Of note, a novel approach of brain structural network topography now permits the exploration of the topological organization of the different brain regions, based on white matter tracts extracted from DTI [14], whereas studies on regional structural network properties related to cognition impairment were mainly conducted in subjects with Alzheimer’s disease [15]. To identify the anatomical basis and underlying mechanisms of cognitive aging distinguished from pathological neurodegeneration, the spatial pattern of structural network related to cognition in healthy populations should be described.
In a large community-based and non-demented sample, we aim to investigate the spatial patterns of white matter microstructure and structural network alternations in relation to different cognition domains which would give important indications for the mechanism of cognitive impairment in the aging process.
MATERIAL AND METHODS
Study population
This study is part of the Shunyi Study, an ongoing prospective community-based cohort study designed to investigate the risk factors and associated brain imaging of age-related and cardiovascular diseases. The design and methods of the Shunyi study have been described previously [16]. Between June 2013 and April 2016, a total of 1,586 participants underwent a baseline assessment including structured questionnaires, physical examinations, and blood tests. Among them, a total of 1,222 participants had a baseline MRI with acceptable quality for brain structure measurements. We excluded individuals with a history of stroke (n = 43), and further excluded those with incomplete cognition data (n = 197). Also, 31 with dementia were excluded. Finally, a total of 943 participants were included in the present analysis (Study flow diagram provided in Fig. 1).
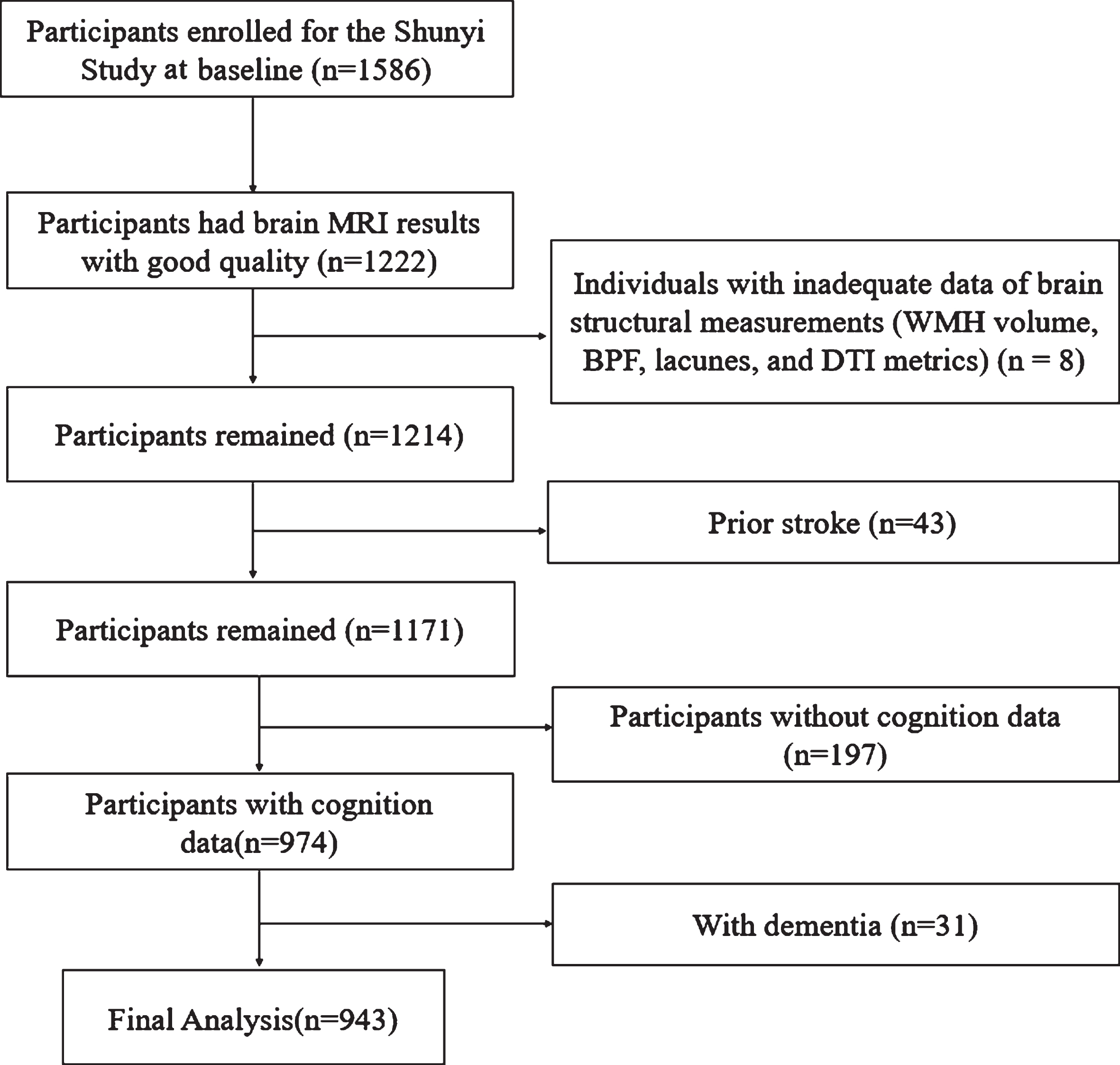
Study flow diagram. MRI, magnetic resonance imaging; DTI, Diffusion tensor imaging; WMH, white matter hyperintensities; BPF, Brain parenchymal fraction.
All the participants provided written informed consent. The study was approved by the Ethical Committee at Peking Union Medical College Hospital (reference number: B-160). All clinical investigation has been conducted according to the principles expressed in the Declaration of Helsinki. Anonymized data will be shared by request from the qualified investigator after ethics clearance and approval by all members of the project group.
Cognitive assessment
The Chinese version of the Mini-Mental State Examination (cMMSE) and the Chinese version of the Montreal Cognitive Assessment (MoCA) adapted from Ziad Nasreddine were used to assess global cognition that evaluates a broad array of cognitive domains [17, 18]. Fuld object memory evaluation (FOM) was used to evaluate episodic memory and learning [19]. Trail Making Tests A and B (TMT-A and TMT-B) were used to assess executive function. The digit span test (forward and backward) was used to evaluate working memory and attention [20]. The 12-Word Philadelphia Verbal Learning Test (PVLT) was performed and scores of the instant recall, the short delay free recall, and the long delay free recall were used to evaluate the memory performance [21].
The total score of cMMSE, MoCA, and TMT-A/B complete times were recorded via a digital mental state detection system (patent NO. CN 103956171 B), a software system with a built-in digital program deployed on a commercial computer. The computer is connected to a Wacom pen display (Waco 2016) to present and conduct the test. When conducting the test, the system logs pen tip coordinates with a timestamp; thus, we can calculate the above measurements after the test.
Brain MRI acquisition
All the MRI data were obtained using a 3-T Skyra scanner (Siemens, Erlangen, Germany). Three-dimensional (3D) T1-weighted, T2-weighted, fluid-attenuated inversion recovery, susceptibility-weighted imaging, and DTI were performed as described in detail in the Supplementary Material.
Assessment of cerebral small vessel disease (CSVD) imaging markers
Definitions of CSVD markers were described previously by Zhai et al. [22]. The presence of lacunes was defined as dichotomous variables, rated by a trained physician (HF) who was blind to all clinical data. WMH volumes were automatically segmented by the lesion growth algorithm as implemented in the lesion segmentation tool toolbox (statistical-modelling.de/lst.html) for Statistical Parametric Mapping 12 (SPM 12, fil.ion.ucl.ac.uk/spm/). WMH volume was natural log-transformed to reduce the skewness. Intra-rater agreement for CSVD markers was provided previously by Zhai et al. [22].
The gray matter (GM), white matter (WM), and cerebrospinal fluid were automatically segmented on structure T1-weighted images using Statistical Parametric Mapping 12 (https://www.fil.ion.ucl.ac.uk/spm/) and Computational Anatomy Toolbox (CAT12; https://www.neuro.uni-jena.de/vbm/). WMH was automatically set as WM to minimize segmentation errors. Total intracranial volume (TIV) was the sum of the volumes of GM, WM, and cerebrospinal fluid. BPF was the ratio of brain tissue volume (GM+WM) to TIV. GM fraction and WM fraction were calculated as the GM and WM volume divided by TIV.
Assessment of covariates
Demographic and clinical information including age, sex, APOE ɛ4, years of education, smoking status, blood pressure, history of hypertension, diabetes mellitus, hyperlipidemia, body mass index, and current medication were collected using a structured questionnaire and physical examination. Blood pressure was measured 3 times and the mean value was used. Diabetes mellitus was defined as fasting serum glucose ≥7.0 mmol/L, self-reported diabetes mellitus, or the use of oral antidiabetic drugs or insulin. Smoking status was classified into a current smoker (at least within the past 1 month) and a noncurrent smoker.
DTI data processing
The DTI data were processed using the Pipeline for Analyzing Brain Diffusion Images toolkit (PANDA, https://www.nitrc.org/projects/panda), a software for fully automated processing of brain diffusion images [23]. FA and MD maps, representing WM microstructural integrity, were generated for each participant in the native space and the standard Montreal Neurological Institute space. Global mean DTI metrics were calculated by all the voxels within the WM mask generated with the threshold FA 0.2 using PANDA.
Network reconstruction
We performed whole-brain white matter tractography using deterministic fiber tracking via the Fiber Assignment by Continuous Tracking algorithm [24]. Streamlines were terminated when FA <0.2 or turning angle >60°. Two regions were considered connected if the endpoints of the reconstructed fiber buddle lay within both regions [25]. The above program has been widely used and robust in terms of identifying major WM tracts [26, 27].
Network nodes
We used the automated anatomical labeling (AAL) template [28] to parcellate the cerebral cortex into 90 cortical and subcortical regions (45 for each hemisphere).
Network edges
For each participant, a weighted edge was constructed via multiplying the number of reconstructed fibers by the mean FA along the fiber bundle connecting the two regions. [15, 27]. The connection strength was further normalized by the average volume of each pair of regions to correct for different sizes of the AAL regions and different brain sizes [27, 29]. This resulted in an undirected weighted 90×90 connectivity matrix for each participant. The average connectivity matrix was shown in Supplementary Figure 3.
Topological properties
The topological properties of the white matter network were performed using the software GraphVar 2.03a (https://www.nitrc.org/projects/graphvar/) [31], a toolbox running in MATLAB R2020b (https://mathworks.com), based on graph theory [14, 31]. Network density is defined as the total number of observed edges in a network divided by the possible number of edges. Total network strength is calculated as the sum of the weighted edges of a network. Global efficiency is defined as the inverse of the shortest path lengths, reflecting how efficiently information is exchanged over the network. The clustering coefficient is defined as the average “intensity” (geometric mean) of all triangles associated with each node. The nodal efficiency for a given node was defined as the inverse of the shortest path length between that node and all other nodes in the network, quantifying the importance of the nodes for communication within the network.
Statistical analysis
The correlation between cognitive performance and global white matter microstructural measurements was evaluated using general linear model analyses, with global mean diffusion metrics (global mean FA and MD) and global network measurements (global network strength, density, and efficiency) as determinants and cognition (cMMSE score, MoCA score, FOM score, digit span score, TMT-A/B complete time, PVLT instant recall, the short delay recall, and the long delay recall scores) as outcome variables. p values were false discovery rate (FDR) correction for multiple comparisons. The linear regressions were applied in the raw model (model 1), in adjustment for age, sex, education years (model 2), and additionally, for BPF, presence of lacunes, lg (WMHvolume), presence of cerebral microbleeds, hippocampal volume, and APOE genotype (model 3). Assumptions of the above models have been checked by residual diagnosis plots.
To evaluate the spatial distribution of white matter integrity damage associated with cognitive impairment, we performed a voxel-wise analysis of DTI metrics using tract-based spatial statistics (TBSS, FMRIB Center, Oxford, UK). General linear model analysis was performed via a permutation-based statistical interference tool for a non-parametric approach (’randomize’). A threshold of 0.2 was applied for the creation of the skeletonized FA image. The number of the permutation tests was set at 5000 and the threshold for significance was set at threshold-free cluster enhancement corrected p < 0.05, adjusted for age and sex. To avoid over-adjustment of the actual spatial distribution of WM structures alternations related to cognition, we did not adjust CVSD markers in the TBSS analysis. Data of 5 participants were excluded due to processing errors in tract-based spatial statistics analysis.
To investigate the regional features of network disconnection in relation to poor cognition performance, we performed general linear model analysis on the strength of each edge and cognitive variables using a permutation-based statistical tool in GraphVar 2.03a. The number of the permutation tests was set at 5000, and the threshold for significance was set at FDR corrected p-value <0.05. The sub-network containing the identified significant edges and the connected nodes was graphically displayed by BrainNet Viewer (https://www.nitrc.org/projects/bnv/) [32].
Statistical significance was defined as two-tailed p < 0.05. Statistical analyses were conducted using SAS version 9.4 (SAS Institute, Inc., Cary, NC).
RESULTS
Of the 943 participants included in the final analysis, the mean age was 55.8 years (SD 9.1), and 333 (35.3%) were male. The mean (SD) education level was 6.7 (3.2) years. Table 1 shows demographic, neuroimaging, and cognitive performance characteristics. Compared with the rest of the cohort (Supplementary Table 1), individuals included in this study were younger (55.8 years versus 57.9 years), comprised of more males (35.3% versus 27.4%), and had higher education level (6.71 years versus 5.72 years).
Baseline characteristics (N = 943)
SD, standard deviation; cMMSE, the Chinese version of the Mini-Mental State Examination; MoCA, the Chinese version of the Montreal Cognitive Assessment; FOM, Fuld Object Memory; PVLT, Philadelphia Verbal Learning Test; TMT, trail making test; MCI, mild cognitive impairment; WMH, white matter hyperintensities; Missing data: Body mass index, 8; Systolic blood pressure, 2; Diastolic blood pressure, 2; FOM score, 19 (all <2.5%). a791 participants completed the TMT-A and 689 participants completed the TMT-B tests.
Global white matter microstructural measurements and cognitive performance
Associations of cognitive performances with white matter microstructure integrity as well as network parameters are shown in Table 2. Poor performance in cMMSE and MoCA, executive functions (TMTA, TMTB complete time and digit span score), and memory assessments (FOM and PVLT tests) were found related to lower global mean FA and higher MD values, indicating diffused white matter integrity loss. Similar associations were found between the whole set of cognitive measurements and lower global network strength, density, as well as global efficiency. All the above associations survived an FDR-corrected threshold of P(FDR) = 0.05.
Associations of cognitive performances with white matter microstructure integrity and network parameters
WMH, white matter hypertension; FA, fractional anisotropy; MD, mean diffusivity; cMMSE, the Chinese version of the Mini-Mental State Examination; MoCA, the Chinese version of the Montreal Cognitive Assessment; FOM, Fuld Object Memory; PVLT, Philadelphia Verbal Learning Test; TMT, trail making test; β, standard regression coefficient. Model 1 is univariate. Model 2 is adjusted for age, sex, and education years. Model 3 is adjusted for brain parenchymal fraction, log WMH volume, presence of lacunes, presence of cerebral microbleeds, hippocampus volume, and ApoE ɛ4 in addition to model 2. *Surviving a false discovery rate (FDR)-corrected threshold of P(FDR) = 0.05.
After adjusting for age, sex, and education years, the significant association of MoCA score, TMTA and TMTB performance with the global white matter microstructural measurements largely remained. However, after further adjustment for brain parenchymal fraction, log WMH volume, presence of lacunes, presence of CMB, hippocampus volume and APOE ɛ4, the association between TMTA/B performance and global white matter microstructural measurements was greatly weakened.
Regional white matter microstructural integrity and cognitive performance
As is shown in Fig. 2, poor performance in digital span tests and PVLT tests was associated with lower FA at almost all voxels on the white matter skeleton. Also, longer TMTA complete time was related to lower FA in the bilateral internal capsule, external capsule, inferior longitudinal fasciculus, corpus callosum, left posterior thalamic radiation, and superior longitudinal fasciculus, while longer TMTB complete time was related to decreased FA in the bilateral internal capsule, right inferior longitudinal fasciculus, and corpus callosum. These associations were independent of age, sex, and education level. The MD maps showed a similar pattern. The TBSS result maps presenting all cognitive measures in relation to FA and MD in both raw model and the above adjustment model are shown in Supplementary Figures 1 and 2.
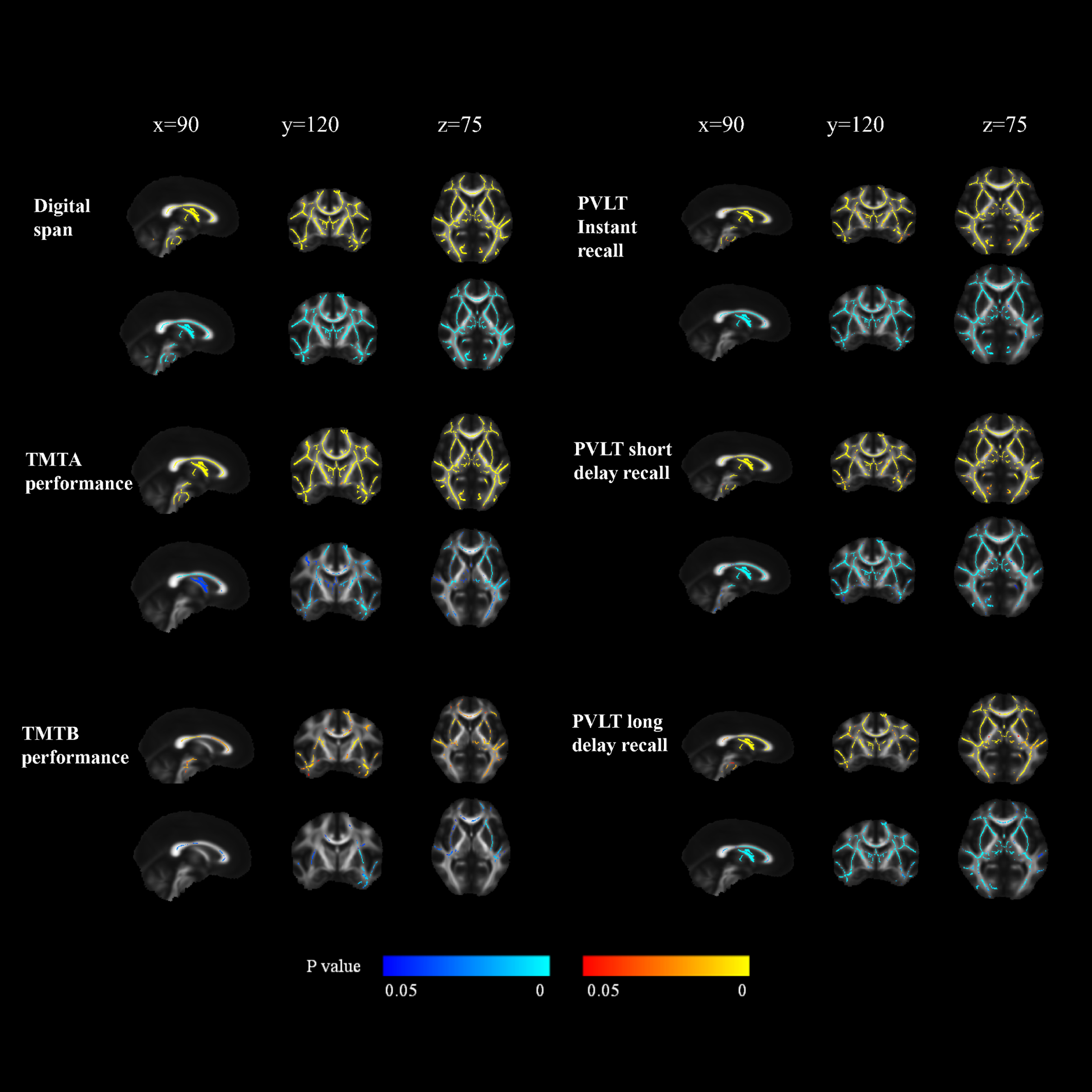
The relationship between the cognitive performance and fractional anisotropy. TMT, trail making test; PVLT, Philadelphia Verbal Learning Test. The upper and lower row of each transversal brain slices panel shows the regions on the white matter skeleton where cognitive performance is related to the fractional anisotropy and mean diffusivity, respectively (threshold-free cluster enhancement corrected p < 0.05, adjusted for age, sex, and education years). The TMTA/B performance were demonstrated as the inverse of TMTA/B complete time. The red color map indicates a positive relationship and the blue color map indicates a negative relationship. x, y, and z indicate the coordinates. We found a strong correlation between a better performance in digital span score, executive speed, and PVLT scores and increased fractional anisotropy across various regions on white matter skeleton.
Regional network connectivity and cognitive performance
In the whole-brain network connectivity analysis, connecting strength of several brain regions was identified to be related to memory performance (FWE corrected p < 0.05) (Supplementary Table 2). The sub-networks constructed by the identified significant connections are presented graphically in Fig. 3. For PVLT instant recall score, a 4-node network in the bilateral frontal lobe and a 3-node network in the right temporal and occipital lobe were detected. For PVLT short delay recall score, a 3-node network containing bilateral rectus gyrus and right lingual gyrus were detected. For PVLT long delay recall score, a 3-node network in the bilateral frontal lobe was detected. To test the robustness of the detected sub-networks, scatter plots of the test scores and the mean connectivity strength of the corresponding networks were done and all showed significant results (p < 0.0001, 0.018, 0.002, respectively). No significant sub-network was detected in relation to TMTA/B, digital span, or FOM tests.
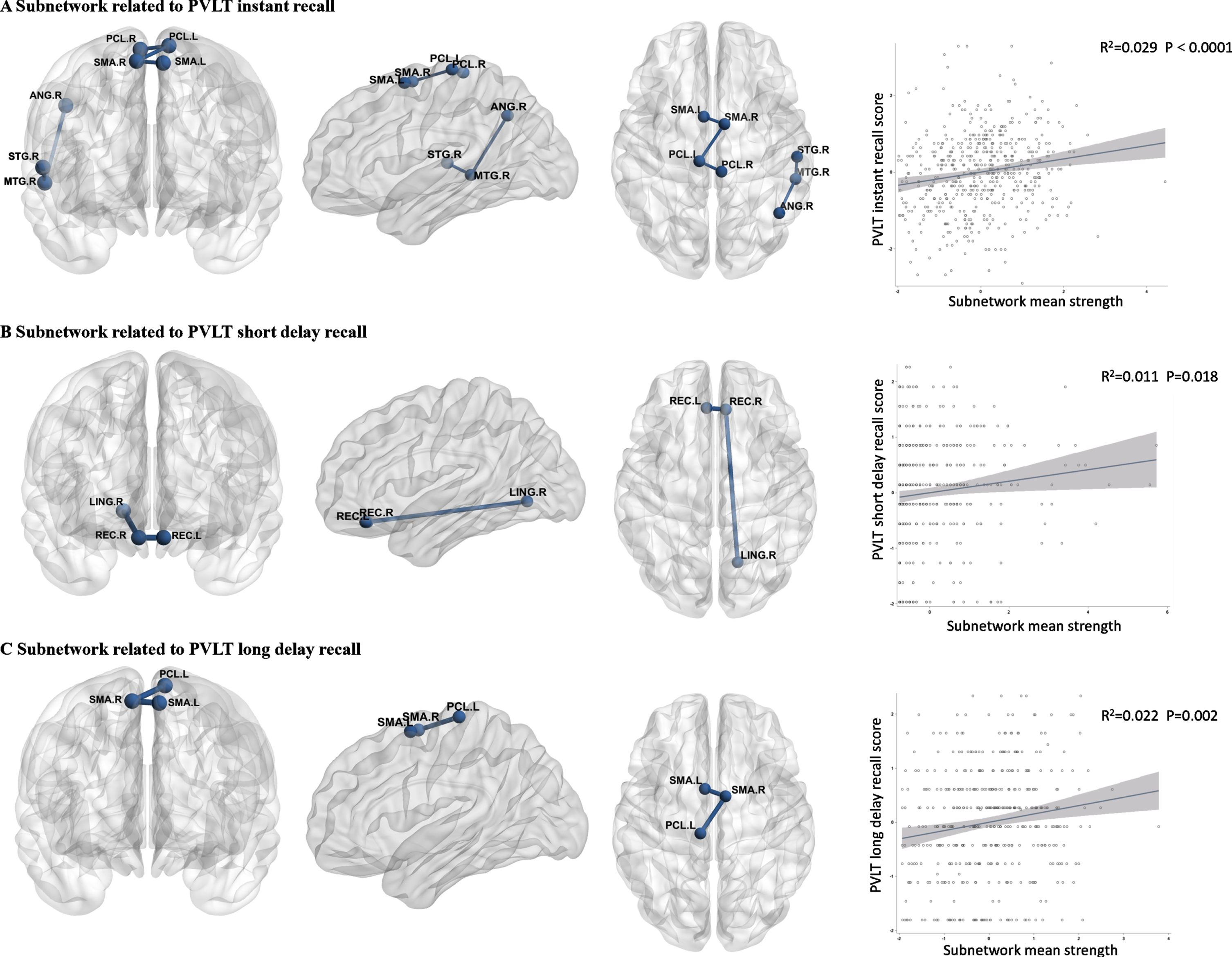
Sub-networks connectivity related to Philadelphia Verbal Learning Test (PVLT) scores. The connectivity strength of all the presented edges is significantly related to the PVLT scores, after correction for multiple testing using the Benjamini–Hochberg procedure at a false discovery rate of 0.05. Nodes with at least one significant edge were also shown. The left column shows scatter plots of the mean strength of the significant sub-network versus the PVLT scores. The best-fitting linear regression line is displayed on each scatter plot. R2 = coefficient of determination.
DISCUSSION
In a population-based non-demented sample, we observed patterns of white matter integrity damage and network dysconnectivity related to cognition impairment. Poor executive functions (presented by TMTA/B complete time) were related to lower FA and higher MD predominantly on the anterior white matter skeleton, while verbal memory loss (presented by PVLT scores) was related to sub-network dysconnectivity in the midline and the right temporal lobe.
Our findings of global mean diffusion metrics associated with executive and memory functions are consistent with previous studies in the healthy elderly population [33–35], suggesting that the diffuse white matter microstructural pathology underlying cognitive aging. We also found global efficiency to be associated with the whole set of cognitive measurements, which is in line with previous studies in patients with CSVD [26, 37] and Alzheimer’s disease [15, 38]. The association seemed greatly weakened after adjusting for age. This could be explained by the strong co-linearity of age and global network measurements, indicating that in a non-demented community-dwelling sample, structural network disruption is dominantly contributed by aging rather than another pathological status. In all, our findings on global microstructural properties added evidence to the hypothesis that disruption of WM tracks and secondary disorganization of complex networks play a role in the cognitive aging process.
In TBSS analysis, we observed that microstructural integrity damage related to lower executive speed is more stable in the anterior brain than the posterior part, which is in accordance with an early DTI study in the elderly population [3]. This pattern is also consistent with the distribution of macrostructural damage reported in convention MRI studies, that WMH related to impaired executive function is mainly located in the frontal lobe [39]. This provides evidence that white matter tract disruption of the anterior brain is mainly involved in age-related executive dysfunction.
Based on task-state functional network, Hermundstad et al. discovered that memory tasks broadly activate long intra-hemisphere connections, in bilateral temporal, frontal, and occipital lobes [40]. Our study recognized several segments of the memory network as the anatomical basis of memory functional impairment. We found that nodal dysconnectivity related to PVLT performance was predominantly located in the midline of the brain, while an extra sub-network in the right temporal lobe was identified in relation to instant recall. This is in line with Lo et al.’s findings in patients with Alzheimer’s disease, that decreased nodal efficiency in the right temporal lobe, middle and superior frontal lobes is associated with poor performance in California Verbal Learning Test [15]. Although the memory test battery and population were different from our study, both studies highlight the importance of those regional disconnections in the context of verbal memory loss during healthy aging and pathological neurodegeneration. The asymmetry of the identified sub-network related to poor verbal memory indicated that the right hemisphere network potentially plays a different functional role in the linguistic impairment of the aging process. As the evidence on regional structural networks related to cognition is still lacking, our findings need to be confirmed and replicated in Chinese samples and other populations.
The strengths of this study include the quantitative evaluation of multiple cognitive domains and the high-resolution MRI protocol in a large size population-based sample, ensuring the accuracy and validity of the study. Some limitations also need to be considered. First, since the relationship between the pattern of changes in the DTI metrics and pathological changes is yet to be verified in the human brain, the DTI changes cannot be precisely translated into histological processes. Second, limitations of the structural network method should also be considered, such as failure in reconstructing tracts in complex WM architecture, identifying long-distance tracts due to noise, partial volume effects, and unequal-sized brain regions using AAL regions [41, 42]. Third, the deterministic tractography methods we used do not capture uncertainty in fiber orientation and are incapable of resolving multiple fiber orientations within a voxel [43]. Despite this, several measures are taken in our study to improve the accuracy and credibility of the structural network, including a quality check of DTI for each subject, normalizing connection strength by the connecting AAL region volumes, as well as applying a correction for multiple comparisons in regional connectivity.
In conclusion, in a community-based and non-demented sample, diffusely disrupted white matter integrity and reduced cerebral network connectivity were associated with poor cognitive performance. The anterior brain is stably related to executive dysfunction, while midline and right temporal brain disconnection are more prominent in verbal memory loss. These findings supported that global and regional disruption of white matter integrity and network connectivity is the anatomical basis of the cognitive impairment in the aging population. Hopefully, DTI-derived microstructural properties may be applied as predictors of decline in specific cognitive domains.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (CIFMS) (CIFMS 2021-I2M-1-025) and the Strategic Priority Research Program “Biological basis of aging and therapeutic strategies” of the Chinese Academy of Sciences (grant XDB39040300).