
Abstract
Background:
The co-occurrence of apathy and executive dysfunction, a correlate of vascular cognitive impairment (VCI), is highly prevalent, yet facilitating factors are largely unknown.
Objective:
This study investigates the relationship between lipid peroxidation, apathy, and executive dysfunction in patients at risk for VCI.
Methods:
In participants with coronary artery disease, who are at a high risk of VCI, apathy (Apathy Evaluation Scale), and executive function (composite z-score based on age and education population norms from trails making test B, animal naming, and phonemic fluency tests) were assessed. Serum concentrations of an early (lipid hydroperoxide (LPH)) and late (8-isoprostane (8-ISO)) lipid peroxidation marker, were measured and the 8-ISO/LPH ratio was calculated.
Results:
Participants (n = 206, age±SD = 63.0±7.5, 80% men, total years of education = 15.9±3.4, AES score = 28.3±8.8, executive function = 0±1) demonstrated significantly different 8-ISO/LPH ratios between groups (F(3, 202) = 10.915, p < 0.001) with increasing levels in the following order: no apathy or executive dysfunction, only executive dysfunction (executive function composite score≤–1), only apathy (AES≥28), and both apathy and executive dysfunction. A model adjusting for demographics showed that lipid peroxidation was associated with both apathy (B(SE) = 4.63 (0.954), t = 4.852, p < 0.001) and executive function (B(SE) = –0.19 (0.079), t = –2.377, p = 0.018). However, when controlling for both demographics and vascular risk factors, lipid peroxidation was associated with only apathy (B(SE) = 3.11 (0.987), t = 3.149, p = 0.002).
Conclusion:
The results highlight a potentially important involvement of lipid peroxidation in the co-occurrence of apathy and executive dysfunction in those at risk for VCI.
Keywords
INTRODUCTION
Vascular cognitive impairment (VCI) is an umbrella term that encompasses all forms of cognitive impairments associated with vascular diseases and/or risk factors such as mild vascular cognitive impairment and majors form of VCI such as vascular dementia or mixed dementia like Alzheimer’s disease (AD) with vascular contributions [1, 2]. People with mild vascular cognitive impairment, the most prevalent form of VCI, display a combined etiology of cognitive impairment and vascular comorbidities [2, 3]. Hence, those with coronary artery disease (CAD) and other vascular risk factors/disorders are at a high risk for developing mild vascular cognitive impairment. VCI is highly prevalent in those with CAD and the presence of CAD also increases the risk of major cognitive impairment such as dementia [4, 5]. Decline in executive function is a hallmark of vascular dysfunction in cognitive impairment and dementia. Executive dysfunction is a decline in high-level cognitive processes that facilitate flexible behaviors [6], and it is prevalent in those with VCI and in those at risk for VCI, such as the CAD population [7, 8].
Apathy is a neuropsychological hallmark of vascular dysfunction [9–12] and is broadly defined as a loss of motivation, interest, and enthusiasm in daily activities [13]. Apathy symptoms often co-occur with executive dysfunction [14, 15] and are prevalent across neurocognitive disorders such as AD [13, 16–18] and cardiovascular disorders such as CAD [9–12]. Apathy is a risk factor for cognitive decline and has been shown to be negatively correlated with global cognition, verbal memory, verbal fluency, and activities of daily living in patients with AD [18]. A study in patients with mild cognitive impairment (MCI) found that those with either apathy alone or apathy and depression are at a significantly greater risk of developing AD compared to non-apathetic patients [19].
Oxidative stress is common in disorders with vascular contributions and cognitive impairment [20–22]. Free radicals are atoms or groups of atoms that are highly reactive due to the presence of an unpaired electron [23]. They are inevitable by-products of aerobic metabolism and generally have beneficial roles in normal physiological function [24]. However, any imbalance in pro-oxidants and antioxidants results in detrimental oxidative damage [23]. Reactive oxygen species (ROS) are a form of free radicals derived from oxygen that positively contribute to immunity, but in excess, negatively oxidize lipids, proteins, and DNA [25]. Increased levels of oxidation markers such as 8-isoprostane (8-ISO), a late lipid peroxidation marker, and decreased levels of antioxidant markers are found in CAD [26, 27]. The brain is a particularly vulnerable target to oxidative damage due to its high levels of free radical production and low levels of antioxidant defense [23, 28]. Accumulating evidence supports the contribution of oxidative damage to the pathogenesis of various cognitive and psychiatric disorders including AD, MCI, and depression [21, 28]. Studies found that a decline in executive function and memory was associated with increased oxidative stress markers, especially the ratio of late to early lipid peroxidation markers [20], which may be explained by decreased antioxidant levels in the brain [29, 30].
Both apathy and executive dysfunction decrease quality of life in those with vascular diseases while increasing their risk of progressing to major forms of neurocognitive disorders such as dementia. Despite these consequences, the physiological pathways underlying these behavioral and cognitive deficits and their co-occurrence in VCI are unknown. Current literature suggests a possible mechanistic relationship between oxidative stress, and both apathy and executive dysfunction, however, this relationship has not yet been investigated. This study aims to examine the relationship between lipid peroxidation, apathy, and executive dysfunction in those at risk of VCI. We hypothesize that patients with both apathy and executive dysfunction will have higher levels of peripheral lipid peroxidation markers as compared to those with apathy, and executive dysfunction alone, and those with neither apathy nor executive dysfunction. We also hypothesize that lipid peroxidation levels will be positively associated with apathy and executive dysfunction independently in patients at risk for VCI.
METHODS
Participants
Data were obtained from patients recruited during intake from a Cardiac Rehabilitation Program at the Toronto Rehabilitation Institute. All study participants had a history of CAD (defined as previous history of either myocardial infarction, coronary artery bypass graft, percutaneous transluminal coronary angioplasty, or at least a 50% stenosis in 1 or more major coronary arteries). All participants were between 45 and 85 years of age and spoke and understood English. Participants were excluded based on previously diagnosed neurodegenerative illness/neurological disorders (dementia, Parkinson’s disease, Huntington’s chorea, history of epilepsy, significant traumatic brain injury, clinical stroke, progressive supranuclear paralysis, brain tumor, subdural hematoma, multiple sclerosis), significant acute medical illness (severely disrupted liver/kidney/lung function), unstable angina, substance abuse, and if they were women of childbearing potential. Antidepressant use was permitted if used at a stable dose for at least 3 months before the study. Written informed consent was obtained from eligible participants and the studies were carried out in accordance with Good Clinical Practice guidelines. All studies and analyses were approved by the research ethics board of Sunnybrook Research Institute and Toronto Rehabilitation Institute.
Clinical characteristics
Participant interviews and physical assessments were used to collect physical and demographic characteristics, and medical history, including clinical diagnoses, concomitant medications, and cardiovascular risk factors.
Outcomes of interest: Cognitive and mood assessments
Apathy was assessed using the self-reported Apathy Evaluation Scale (AES). Apathy was defined as an AES score of 28 or above. To compare those with relatively higher apathy to those with lower apathy, the sample was divided at the mean AES score of 28. Executive function was assessed using the Trial Making Test B, FAS test for phonemic fluency, and Animal Naming Test for semantic fluency. The z-score was calculated based on published age- and education-matched norms for each cognitive test [31, 32]. An executive function composite score was computed by averaging the z-scores of Trial Making Test B, FAS test, and Animal Naming Test. Participants were described as having executive dysfunction if they performed 1 standard deviation (SD) below age and education norms on the executive function composite score [4].
Outcomes of Interest: Lipid peroxidation markers
ROS react with lipids to produce lipid hydroperoxides (LPH) which are normally detoxified by antioxidants [33]. However, as antioxidant defenses are altered, lipid peroxidation continues and LPH reacts to form more stable products including 8-isoprostane (8-ISO) [33]. Fasting blood was collected from participants and serum concentrations of early and late-stage lipid peroxidation markers (LPH, 8-ISO) were measured. LPH was measured using a calorimetric assay kit (Cayman Chemical; item 705003) according to manufacturer’s instructions. 8-ISO was measured using a standard competitive sandwich ELISA (Cayman Chemical; item 516351) according to manufacturer’s instructions. To describe oxidative stress more accurately, a ratio of late-stage to early-stage markers was computed (8-ISO/LPH) and used to evaluate all proposed hypotheses [20]. All lipid peroxidation parameters were log-transformed to ensure normality and therefore used for analyses [20].
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics (version 23; Armonk, NY). Statistical significance was set at two-tailed p < 0.05. Patient demographics including cognitive characteristics, vascular risk factors, markers of lipid peroxidation, and mood and cognitive scores were computed. Continuous variables were expressed as means and SDs and categorical variables were expressed as percentages.
Pearson’s and Spearman’s correlations were used to test correlations between variables of interest: markers of lipid peroxidation, apathy, and executive function. A One-Way Analysis of Variance was used to evaluate the primary hypothesis. Patients were divided into those with apathy, those with executive dysfunction, those with both apathy and executive dysfunction, and those with neither apathy nor executive dysfunction. To evaluate the secondary hypothesis, multivariate linear regression models were used. Three models were developed: 1) an unadjusted model, 2) a model adjusted for demographics, and 3) a model adjusted for demographics, vascular, and clinically important factors with oxidative stress as the independent variable, and apathy score and executive function composite score as dependent variables. Demographic covariates included age, sex, and total years of education. Vascular and clinical factors included body mass index (BMI), hypertension, dyslipidemia, diabetes, and depression. Depression was evaluated using the Center for Epidemiologic Studies Depression Scale (CES-D) and patients with CES-D scores greater than or equal to 20 were considered as having a current depressive episode [34, 35]. The independent variables were checked for multicollinearity using tolerance (acceptable threshold > 0.1) and variance inflation factor (acceptable threshold < 10) statistics. A post-hoc mediation analysis with total AES as the independent variable, executive function composite score as the dependent variable, and log-transformed 8-ISO/LPH as the mediator was conducted to examine the relationship between the three variables. The analysis was adjusted for age, sex, years of education, BMI, hypertension, dyslipidemia, diabetes, and depression. Mediation effects between AES, executive function composite scores, and lipid peroxidation were computed using a bias corrected inferential bootstrapping method with 10,000 permutations to obtain a 95% confidence interval (CI) for the indirect effect. The mediation was performed using PROCESS macro version 3.5 for SPSS.
RESULTS
Demographics
Clinical characteristics and demographics of participants are reported in Table 1. Pearson correlation coefficients between markers of lipid peroxidation, apathy and executive dysfunction are presented in Table 2. Most study participants were male and over the age of 60. Vascular risk factors commonly included hypertension and a BMI suggesting obesity.
Participant demographics
CES-D, Center for Epidemiologic Studies Depression Scale; BMI, body mass index; AES, Apathy evaluation scale; MMSE, Mini-Mental State Examination; LPH, lipid hydroperoxide; 8-ISO, 8-isoprostane; 8-ISO/LPH, ratio of 8-isoprostane to lipid hydroperoxide.
Correlations between log transformed lipid peroxidation markers (LPH, 8-ISO, 8-ISO/LPH) and outcomes of interest: executive function (executive function composite score) and apathy (AES score)
aValues displayed are Pearson’s correlations; bValues displayed are Spearman’s rho. AES self-reported apathy evaluation scale; LPH lipid hydroperoxide; 8-ISO 8-isoprostane; 8-ISO/LPH ratio of 8-isoprostane to lipid hydroperoxide.
Correlations between markers of lipid peroxidation, apathy, and executive function
There were significant correlations between executive function and LPH, and 8-ISO/LPH (Table 2). Apathy was significantly correlated with both early and late-stage markers of lipid peroxidation, in addition to their ratio (Table 2).
Lipid peroxidation levels in those with and without apathy and executive dysfunction
In the primary analysis, differences in lipid peroxidation markers were observed among the four groups using a one-way ANOVA. All assumptions for a one-way ANOVA were met. Log-transformed 8-ISO/LPH was significantly different between the four groups, F(3, 202) = 10.915, p < 0.001 (Fig. 1). Log-transformed 8-ISO/LPH increased from the no apathy or executive dysfunction group (n = 106, mean±SD = 0.17±0.55), to the executive dysfunction only (n = 17, mean±SD = 0.24±0.63), apathy only (n = 74, mean±SD = 0.46±0.57), and both apathy and executive dysfunction (n = 9, mean±SD = 1.20±0.81) groups, in that order. A Tukey-Kramer post-hoc test revealed that the group with both apathy and executive dysfunction was significantly different from all other groups. Additionally, the group with neither executive dysfunction nor apathy was significantly different from the group with apathy alone.

Log-transformed 8-ISO/LPH in different apathy and executive dysfunction groups in patients at risk of VCI. Values displayed are means with standard error bars. Bar brackets and * display groups with significantly different mean log 8-ISO/LPH ratio values as tested using Tukey-Kramer post-hoc test (p ≤ 0.05). n, number of participants in each group.
Lipid peroxidation as a predictor of apathy and executive dysfunction
The unadjusted multivariate linear model (Wilks Lambda = 0.853, F(2, 203) = 17.54, p < 0.0001), the model adjusted for demographics (Wilks Lambda = 0.753, F(8, 400) = 7.61, p < 0.0001), and the model adjusted for both demographics and vascular risk factors (Wilks Lambda = 0.581, F(18, 382) = 6.62, p < 0.0001) showed that lipid peroxidation was significantly associated with apathy and executive function (Table 3). Overall model fit statistics for multivariate linear regressions investigating the associations of log 8-ISO/LPH ratio with apathy and executive function can be found in Supplementary Table 1. Log 8-ISO/LPH ratio was significantly associated with apathy (B(SE) = 4.81 (0.944), t = 5.099, p < 0.001) and executive function (B(SE) = –0.21 (0.078), t = –2.665, p = 0.008) in the unadjusted model 1. After controlling for age, sex, and years of education, log 8-ISO/LPH ratio was still significantly associated with apathy (B(SE) = 4.63 (0.954), t = 4.852, p < 0.001) and executive function (B(SE) = –0.19 (0.079), t = –2.377, p = 0.018) in model 2. Model 3 was adjusted for age, sex, and years of education, BMI, hypertension, dyslipidemia, diabetes, and depression and showed significant associations between log 8-ISO/LP and apathy (B(SE) = 3.11 (0.987), t = 3.149, p = 0.002). However, the relationship between log 8-ISO/LPH and executive function (B(SE) = –0.15 (0.084), t = –1.781, p = 0.076) was no longer significant in model 3.
Associations of log 8-ISO/LPH ratio with apathy (AES) and executive function (executive function composite z-score)
1) Model 1- not adjusted for any covariates; 2) Model 2- adjusted for age, sex, and years of education; and 3) Model 3- adjusted for age, sex, years of education, BMI, hypertension, dyslipidemia, diabetes, and depression *Log 8-ISO/LPH was no longer significantly associated with executive function. AES, self-reported apathy evaluation scale; 8-ISO/LPH, ratio of 8-isoprostane to lipid hydroperoxide.
Lipid peroxidation as a mediator of the relationship between apathy and executive dysfunction
A post-hoc mediation analysis examined whether lipid peroxidation mediates the association between apathy and executive function. Controlling for age, sex, years of education, BMI, hypertension, dyslipidemia, diabetes, and depression, the ratio of late to early lipid peroxidation markers (log 8-ISO/LPH) mediated a significant indirect association between apathy and executive function (–0.0030, 95% CI [–0.0078, –0.0001]; Fig. 2).
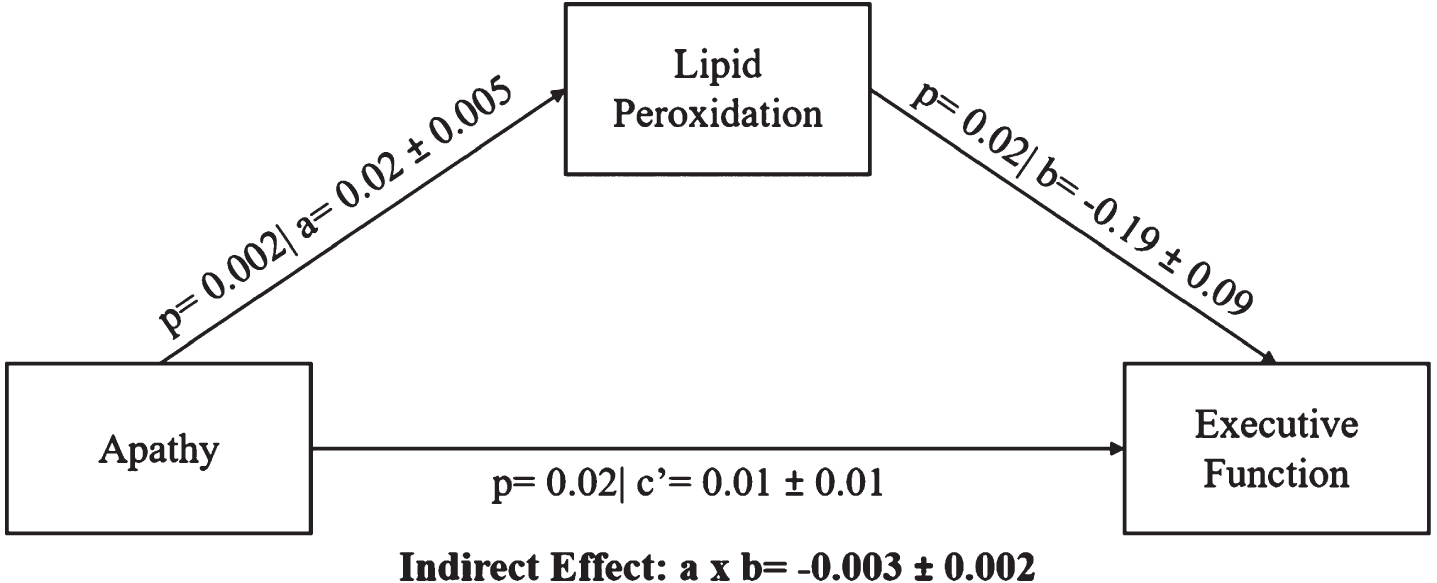
A mediation pathway between apathy (AES score), lipid peroxidation (ratio of 8-ISO to LPH), and executive function (executive function composite z-score) in a population at risk for VCI. Age, sex, years of education, BMI, hypertension, dyslipidemia, diabetes, and depression were used as covariates. a = regression coefficient between AES and log 8-ISO/LPH (±standard error), b = regression coefficient between log 8-ISO/LPH ratio and executive function composite z score (±standard error), a×b = indirect effect, c’ = c –a×b where c is the regression coefficient between AES and executive function composite z-score, CI = 95% bias corrected bootstrap (10,000 permutations) confidence interval for the indirect effect. Significant path coefficient at p < 0.05, significant indirect effect when the CI does not cross 0.
DISCUSSION
The present study demonstrates a relationship between lipid peroxidation, apathy, and executive dysfunction in patients at risk for VCI. Participants with both apathy and executive dysfunction had significantly higher levels of peripheral lipid peroxidation markers compared to those with apathy, and executive dysfunction alone, and to those with neither apathy nor executive dysfunction. Significant associations were found between lipid peroxidation, and both apathy and executive dysfunction in multivariate models that were unadjusted, adjusted for demographics, and adjusted for both demographics and vascular risk factors. We also explored the facilitating role of lipid peroxidation between the two outcomes of interest in a post-hoc analysis and found that lipid peroxidation significantly mediates the relationship between apathy and executive dysfunction in patients at risk for VCI. These findings are consistent with the growing body of literature that suggests a pathogenic role of oxidative stress in disorders with vascular contributions including cognitive disorders [20, 28], psychiatric disorders [23], and cardiovascular disorders [20].
Regional oxidative stress variations in the brain result from differences in oxygen consumption and levels of antioxidants [36]. One of the major ROS producers in the brain are the mitochondria, predominantly due to a leakage of electrons from the electron transport chain [37]. These escaped electrons interact with nearby molecules to produce free radicals [37]. The highest lipid metabolism rate found in the body is in the brain, making it a highly susceptible target to oxidative damage [23, 38]. Current literature suggests a clear link between excess oxidative stress and altered central nervous system function, especially in neurodegenerative diseases [39]. Elevated oxidative stress markers and decreased antioxidant activity have been found in many at-risk populations including MCI [40, 41], AD [38, 42], vascular dementia [43], and CAD [44]. Our study evaluated the early-stage lipid peroxidation marker, LPH, and late-stage marker, 8-ISO. LPH plays an important role in cell signaling and housekeeping, and in excess, causes necrosis, apoptosis, and eventual neurodegeneration [45, 46]. The ratio of late-stage to early-stage markers is more informative than early- or late-stage markers alone because it can explain the accumulation and severity of disease [20, 33]. Oxidative stress negatively affects vascular growth and integrity, which can lead to the breakage of the blood-brain barrier, neurotoxicity, necrosis, and increased downstream issues [47]. The present findings add to the growing literature that supports the role of lipid peroxidation in microvascular dysfunction, a mechanism that may also play a role in the pathogenicity of apathy and executive dysfunction.
Literature consistently shows increased lipid peroxidation in diseased regions of the brain in AD patients [48]. These brain regions are common to those related to apathy and executive dysfunction, suggesting potential anatomical similarities that may be causing these symptoms together. Across many pathologies including AD and Parkinson’s disease, apathy is associated with disruptions in the frontal cortex, particularly the anterior cingulate cortex and orbitofrontal cortex [49, 50]. Executive function has been linked to the prefrontal cortex and frontal sub-cortical areas [51, 52]. Ultimately, increased apathy and impaired executive function are hallmarks of frontal-subcortical circuit dysfunction [51]. Previous findings have also shown that the frontal cortex is subject to large amounts of oxidative stress and decreased antioxidant function [53]. The significant association between apathy and executive dysfunction can be explained by degradation of functional connectivity between the frontal cortex and ventral striatum [14]. Additionally, in AD brains, synapse loss and amyloid-β deposition is apparent in the frontal cortex [54–56]. Previous literature and the findings of this study support a pathogenic role of oxidative stress, particularly lipid peroxidation, in the frontal cortex of patients at risk of VCI, which may potentially contribute to the etiology of apathy and executive dysfunction, ultimately leading to the progression to dementia. Our findings provide important support for potential oxidative damage in vulnerable regions of the brain involved in apathy and executive function and its downstream effects. These results may motivate the search for a targeted therapeutic technique that reduces oxidative damage in the frontal cortex and therefore prevents cognitive impairment. Brain penetrating antioxidants such as N-acetyl cysteine may be of interest. N-acetyl cysteine is a precursor of L-cysteine, a component of glutathione, the most prevalent antioxidant in the brain [57]. Cysteine availability is the limiting factor in glutathione production; therefore, the administration of N-acetyl cysteine may counteract oxidative stress by maintaining or increasing antioxidant availability [58]. Other brain penetrating antioxidants may also be beneficial in neurodegenerative disorders like AD and Parkinson’s disease [59, 60]. Antioxidants are a promising avenue of treatment for oxidative damage, however further investigations and clinical studies are needed to provide more robust results.
Apathy is significantly associated with executive dysfunction, and historically, AD patients with apathy perform significantly worse on executive function tests [14, 61]. The co-occurrence of apathy and executive dysfunction often occurs in at risk populations and results in additional challenges to patients and caregivers. As shown by our mediation analysis, apathy may be exacerbating the vascular dysfunction in patients with vascular disorders leading to the production of even more lipid peroxidation, which can then put these patients at risk of executive dysfunction and cognitive decline. These findings, in line with current literature, suggest that apathy may be a marker for increased risk of cognitive decline and progression to major neurocognitive disorders. It has been previously shown that apathy increases the risk of MCI patients progressing to AD [19, 62–65]. Apathy has shown to be associated with increased risk of dementia progression up to 7-fold in those with MCI [62]. Additionally, apathy but not depression was associated with increased risk, and this finding has been replicated in several cohorts of MCI patients displaying its importance in this population [19, 65]. Although apathy is an important risk factor for dementia, there are no approved treatments for apathy in cognitive disorders to date. Therefore, it is crucial to look for diagnostic and prognostic biomarkers of apathy that can be used as targets for future therapeutics. Previously, hypometabolism in various brain regions detected via FDG-PET [66, 67] and cortical atrophy [68, 69] have been linked to apathy in pre-dementia stages however no cerebrospinal fluid biomarkers have shown such associations with apathy in this population [50]. In AD populations, apathy has been linked to hypometabolism, cortical atrophy, cortical amyloid-β and tau deposits, and various neurotransmitter systems in the brain [50]; however, research on apathy and more accessible and economical blood-based biomarkers is scarce. This study established a novel link between apathy and peripheral oxidative stress, specifically lipid peroxidation. Apathy has previously been associated with cholesterol and inflammation, factors that affect vascular function in the body, in healthy elderly [70] and in those with dementia [71]. Both cholesterol [72] and inflammation [73] are also known to produce oxidative stress, which may be the link between these vascular processes and apathy. The individuals in our study were not severely apathetic, as reflected via their scores on the AES. As such, our study suggests that lipid peroxidation is associated with even mild apathy in those at risk of VCI and may be important to screen for.
As possible limitations, this study did not account for antioxidant medications in our analysis and our sample mostly consisted of male, Caucasian, and highly educated individuals and hence future studies should aim to account for these effects and to generalize our findings to a larger and a more diverse cohort. The cohort for this study was recruited from a cardiac rehabilitation clinic and due to the exclusion criteria for severe cognitive impairment and severely disturbed organ function, the sample was slightly younger than cohorts previously used in literature investigating the relationship between apathy and cognition [14, 74]. This was in line with the aim of investigating the role of oxidative stress in apathy and executive dysfunction in a prodromal patient population in order to contribute to the literature on early biomarkers for apathy and cognitive impairment. Apathy in younger individuals is a risk factor for cognitive decline as shown by Clarke et al., who had a community dwelling sample of elderly participants with age (65.56 years) and baseline cognition (MMSE = 28.04) that was similar to that of this study. They reported that those with apathy had a higher risk of cognitive decline following one year, after adjusting for demographics and covariates. Additionally, those with apathy at baseline also had a higher risk of functional decline post one year and for 13 years follow-up [75]. Hence, more studies should be conducted in a younger prodromal population to find biomarkers that can be targeted earlier to stop or slow down behavioral and cognitive dysfunction in the elderly. As an additional limitation, this study defined higher apathy using average scores as a cut-off, which corresponded to a lower cut-off than those previously used to define apathy [76, 77]. The cut-offs used in the literature are meant to define clinically significant apathy and were chosen by comparison to clinical diagnoses of apathy. However, those definitions have not been validated against biomarker changes, and a lower cut-off may be important to discover novel pathological biomarkers of apathy. Furthermore, there have been inconsistencies regarding cut-offs for the self-reported AES depending on cognitive status [78]. As such, definitions are arbitrary. This study suggests that a lower cut-off may be important. Future efforts may investigate localized lipid peroxidation through studies of central oxidative stress markers rather than peripheral ones, as well as incorporating brain imaging. Since the sample size for the executive dysfunction and the combined apathy and executive dysfunction groups were relatively small in the current study, future research should investigate lipid peroxidation as a biomarker of apathy and executive dysfunction in a bigger sample with a more variable range of apathy and cognitive dysfunction. Although the role of oxidative stress has been previously recognized in neurocognitive and psychiatric disorders [39], a larger study will be able to better establish the role of oxidative stress specifically in the symptoms of apathy and executive function and in their combined occurrence. Lipid peroxidation, apathy, and executive dysfunction are common in cerebrovascular disorders [8, 20], therefore factors such as white matter integrity, fractional anisotropy, and cerebral blood flow should be explored as they may serve facilitating pathogenic roles. Longitudinal studies of oxidative stress markers in patients with varied vascular and cognitive disorders may quantify the degree at which lipid peroxidation increases through the progression to dementia, and pin-point key time-points in which preventative measures and treatment should be introduced. Lastly, we also suggest that future investigations should evaluate the efficacy of targeted oxidative stress therapeutics as well as antioxidant therapy in this population. In conclusion, our results highlight the relationship between lipid peroxidation and the co-occurrence of apathy and executive dysfunction in those at risk for VCI. We propose that, particularly in those with apathy, the progression to dementia may be facilitated by vascular damage and a subsequent build-up of lipid peroxidation markers, which may lead to a decline in executive function and cognitive impairment, but future longitudinal studies are required to evaluate this.
Footnotes
ACKNOWLEDGMENTS
The authors would like to acknowledge the project student, Fei Li, for her help in formatting the manuscript. The authors gratefully acknowledge support from Canadian Institute of Health Research (PJ2-179753, PJT-183584) , Pooler Charitable Fund, Canadian Consortium for Neurodegeneration in Aging (CNA 163902), Alzheimer’s Association Part the Cloud (PTCG-20-700751, PTC-18-543823), Weston Foundation (CT190002), and Alzheimer’s Drug Discovery Foundation (201808-2016354).