
Abstract
Background:
Patients with stroke are at a higher risk of cognitive impairment and Alzheimer’s disease dementia.
Objective:
To quantify the role of lifestyle pre-stroke, post-stroke, and changes in lifestyle before and after stroke with cognitive decline in community-dwelling stroke survivors.
Methods:
Utilizing data from the Chicago Health and Aging Project, a population-based cohort study, we studied 1,078 individuals with stroke (662 incident and 416 prevalent) who underwent cognitive testing during the study period. A healthy lifestyle score was defined by scoring four behaviors: non-smoking, exercising, being cognitively active, and having a high-quality diet. The global cognitive score was derived from a comprehensive battery of 4 standardized tests.
Results:
The mean age at incident stroke was 78.2 years, and 60.1% were women. A healthy lifestyle pre-incident stroke was associated with a slower rate of cognitive decline after stroke. Participants with 3–4 healthy lifestyle factors pre-incident stroke had a slower cognitive decline after stroke by 0.046 units/year (95% CI 0.010, 0.083), or 47.7% slower, than participants with 0–1 healthy lifestyle factor. Lifestyle score post-prevalent stroke was not associated with cognitive decline. Changes in lifestyle behaviors from pre- to post-incident stroke were related to cognitive decline after stroke. Individuals who deteriorated their lifestyle quality after stroke had a faster cognitive decline by 0.051 units/year (β –0.051, 95% CI –0.090, –0.012) than participants with no change in lifestyle score.
Conclusion:
A healthy lifestyle pre-stroke was associated with a slower rate of cognitive decline in stroke survivors, highlighting the importance of primary prevention. After the stroke, changes in lifestyle behaviors may influence the cognitive abilities of older adults as they age.
INTRODUCTION
According to the Center for Disease Control and Prevention in the United States, one of the ten great public health achievements of the 20th century is the remarkable decline in mortality risk after stroke [1]. With the increasing life expectancy after stroke [2, 3], more patients with stroke will be predisposed to the long-term consequences of stroke, such as cognitive impairment and Alzheimer’s disease dementia [4]. Alzheimer’s disease and related dementia entail tremendous social and economic burdens [5]; therefore, it is imperative to identify strategies that will simultaneously increase survival after stroke and lower the risk of cognitive impairment and Alzheimer’s disease dementia.
Stroke and dementia share a number of modifiable risk factors, including smoking, physical activity, and diet quality, which contribute to the risk of incident stroke [6], the risk of Alzheimer’s disease dementia [7, 8], and overall life expectancy [9, 10]. While growing scientific evidence supports the role of lifestyle in the primary prevention of Alzheimer’s disease dementia [10–14], it is unknown whether these lifestyle factors exert cognitive benefits among stroke survivors. To fill these critical knowledge gaps, we conducted a prospective study investigating the impact of a healthy lifestyle (a) pre-stroke, (b) post-stroke, and (c) changes in lifestyle pre- and post-stroke diagnosis, on the annual rate of cognitive decline among patients with stroke living in the community.
METHODS
Study design, settings, and population
The study sample consists of participants from the Chicago Health and Aging Project (CHAP), a large population-based cohort study that examines the risk factors for Alzheimer’s disease dementia [15]. Started in 1993, CHAP enrolled 10,802 participants— 6,158 were enrolled at the original cohort and 4,644 in successive cohorts until 2012, aged 65 years or older through a door-to-door census in four neighborhoods in the South Side of Chicago. Data on a wide range of social and clinical phenotypes, including lifestyle factors, medical history, genotypes, and cognitive performance, were obtained in-home by using structured interviewer- or self-administered questionnaires and assessments.
Of the 10,802 participants, 8,762 were enrolled in Medicare and Medicaid Services, of whom 1,731 were diagnosed with stroke through December 31, 2009 (Flowchart available in Supplementary Figure 1). We excluded 645 participants of 1,731 because they had no follow-up data after stroke and an additional 8 participants with missing data on all lifestyle factors. Of the remaining 1,078 participants with a diagnosis of stroke, comprising our study population, 662 were classified as an incident stroke since the event occurred during the follow-up, and 416 were prevalent given they had a stroke before being enrolled in the CHAP study (Supplementary Figure 1). The median [interquartile] time difference between stroke event (prevalent stroke) and baseline assessment was –1.6 years [–0.7, –2.6]. We compared the demographic differences of stroke participants excluded from the study (n = 645) with those included (Supplementary Table 1). On average, stroke patients excluded from the investigation due to no follow-up were 4 years older than those with follow-up (age at stroke 82 versus 78 years), and they had a higher mortality rate (85% versus 54% through December 31, 2009).
The Rush University Medical Center Institutional Review Board approved the CHAP study. All participants provided informed consent to be eligible to participate in this study.
Assessment of stroke hospitalizations
Stroke hospitalizations were determined by reviewing the medical reports obtained from the Center for Medicare and Medicaid Services (CMS) for stroke-related admissions. Utilizing the International Classification of Diseases Ninth Revision (ICD-9), we defined ischemic and hemorrhagic stroke following comparable studies on stroke patients in CHAP and literature [16–19]. The ischemic stroke comprised the following ICD-9 codes: 433.01, 433.1, 433.2, 433.21, 433.3, 433.31, 433.81, 434.01, 434.1, 434.11, 434.91, 435.2, 435.3, 435.8, 435.9, 436.0, 437.1, 437.7, 437.9, and 438.0. The hemorrhagic strokes codes included 430, 431, 432.1, and 432.9. These ICD-9 codes were previously validated by the co-author (Dr. Aggarwal), a board-certified neurologist and CHAP investigator. Overall, in CHAP, about 91% of all stroke hospitalizations were ischemic and 9% hemorrhagic. In our study, we conducted separate analyses for any strokes, including ischemic and hemorrhagic stroke, as well as specifically on ischemic stroke.
Assessment of lifestyle factors, demographics, other health measures
The lifestyle score included four modifiable risk factors: diet, cognitive activity, physical activity, and smoking history. The a priori selection of these lifestyle factors was based on the published evidence [10–14], guidelines [20, 21], and expert knowledge for the potential health benefits of these lifestyle factors in the prevention of dementia. The definition of these lifestyle factors has been described in our previous work [7]. In brief, dietary habits were assessed by using a validated 144-item food frequency questionnaire [22], and the quality of diet was determined using the Mediterranean-DASH Diet Intervention for Neurodegenerative Delay (MIND) diet score [23, 24]. The MIND diet score summarizes information on 10 brain-healthy food groups (green leafy vegetables, other vegetables, nuts, berries, beans, whole grains, seafood, poultry, olive oil, red wine) and 5 unhealthy food groups (red meats, butter/margarine, cheese, pastries/sweets, and fried/fast food) [23]. A low-risk (i.e., healthy) diet was defined as a MIND score (without alcohol; range 0 to 14) greater than 7.5, corresponding to the upper 40% of the cohort distribution [8] (a higher MIND score indicating a healthier diet). We used cohort-specific cutoff, following the suggestions from similar studies in the literature [25, 26], because there are no established thresholds for a healthy MIND diet and cognitive activity. Late-life cognitive activity is a composite score (range: 1 to 5) of seven activities (e.g., reading, writing letters, visiting a library, and playing chess or checkers) [27], and a low-risk (i.e., healthy) cognitive activity score was defined as greater than 3.43, corresponding to the upper 40% of the cohort distribution [8]. Physical activity was assessed using the 1985 U.S. Health Interview Survey where participants reported time spent in 6 types of activities (e.g., walking for exercise, gardening or yard work, calisthenics or general exercise, bicycle riding, and swimming) [28]. Individuals who engaged in more than 150 minutes/week before stroke (e.g., pre-incident stroke) and those who spent more than 75 min/week (e.g., post-prevalent stroke or post-stroke) in any of these 6 types of activities were considered healthy based on the guidelines for physical activity with [20] and without [21] stroke. Smoking status was self-reported (current, former, or never), and low-risk (i.e., healthy) participants were considered non-current smokers [29].
For each lifestyle factor (e.g., diet, cognitive activity, physical activity, and smoking), participants received 1 point if they met the criterion for the low-risk (i.e., healthy) category or 0 points otherwise. We summarized the four scores to yield a final lifestyle score which ranged from 0 to 4, with higher scores suggesting a healthier lifestyle.
We used the 1990 US Census questions to assess race/ethnicity. Education was measured as the number of years of formal schooling completed. History of comorbidities including heart disease, diabetes, and cancer was determined by self-report questions from the Established Populations for the Epidemiologic Study of the Elderly.
Assessment of global cognitive function
Cognitive function was evaluated by a brief battery of 4 tests, including 2 tests of episodic memory (immediate and delayed story recall) [27, 30], 1 test of perceptual speed [31], and 1 test of general orientation and global cognition (the Mini-Mental State Examination) [32]. Cognitive assessments were employed at three-year intervals during the study follow-up, enabling us to study the rate of cognitive decline. On average, individuals with stroke in CHAP had 3.1 cognitive assessments during the study period.
Each of these 4 cognitive tests were standardized (centered and scaled) to the population mean and standard deviation. Then, a composite z-score for global cognitive function was obtained based on the average standardized scores for the 4 tests. Compared with single cognitive tests, the composite measure is advantageous because it accommodates a broader range of individual cognitive performances. A participant whose composite global cognitive function is equal to the average for the population has a z-score of 0. Positive z-scores indicate a better cognitive performance relative to the population’s average performance, whereas negative z-scores indicate a poor cognitive performance [33].
Statistical analysis
We used a linear mixed-effects model to examine the association of the lifestyle score with the rate of cognitive decline after stroke. The linear mixed-effects model allows us to account for the baseline level of global cognition and estimate the annual rate of cognitive decline by adherence to lifestyle factors. Lifestyle score was examined as a continuous variable with a one-point increase (e.g., one additional healthy factor) in the lifestyle score (0–4) and as a categorical variable in which we grouped study participants into three groups, 0–1, 2, and 3–4 healthy (i.e., low-risk) factors with the reference category those with 0 or 1 healthy lifestyle factor. Models were adjusted for age, sex, race, education, and comorbidities. We also include in the model the follow-up time when cognitive tests were administrated and interactions between time and predictor variables. Time-interactions allow us to estimate the annual rate of change in cognitive function over the study period for our exposure as well as the impact of confounders.
To address our research question, we conducted three primary analyses. First, we investigated the association of the lifestyle score pre-incident stroke with the annual rate of cognitive decline after stroke. In this analysis, we focused on individuals who developed stroke during follow-up (e.g., incident stroke) for whom we had information about lifestyle factors before the stroke event. To limit measurement error from self-report questionnaires, we computed the cumulative average of each lifestyle factor assessed before the incident stroke [34, 35]. Second, we examined the relationship between the lifestyle score post-prevalent stroke and the annual cognitive decline rate. This analysis focused on participants who had a stroke before enrolling in the CHAP study (e.g., prevalent stroke). The lifestyle factors in these participants were assessed at the baseline (i.e., after stroke). Because the time from stroke event to lifestyle assessment (e.g., delay since stroke) may impact the lifestyle-cognition association, we adjusted for the duration in years from stroke to lifestyle assessment at the baseline in our multivariable-adjusted models. Third, we investigated the relationship between changes in the lifestyle score from pre-incident stroke to post-incident stroke with the annual rate of cognitive decline. For this analysis, we focused on participants who developed stroke during the follow-up (e.g., incident stroke) and computed the absolute difference of the lifestyle score for each individual by subtracting the lifestyle score post-stroke with lifestyle score pre-incident stroke. A positive difference in lifestyle score suggests that a participant with stroke improved the lifestyle after stroke; a negative difference shows that an individual deteriorated (decreased) the lifestyle after stroke. In this analysis, we examined the changes in lifestyle score as a categorical variable in which we grouped study participants into three categories, those who decreased (range –3 to –1), did not change (range 0–0), and increased (range 1 to 3) with a reference category those who did not change the lifestyle score from pre- to post-incident stroke [36]. Since the status in the lifestyle pre-incident stroke may impact the relationship between the change in lifestyle score and cognitive decline, we additionally adjusted for lifestyle score pre-incident stroke in our multivariable-adjusted models. We also adjusted for the time (e.g., years) from the incident stroke to lifestyle assessment post-incident stroke in multivariable-adjusted models. For the incident stroke analyses, linear mixed effects regression models with a change point were used to study the rate of change in cognitive function [37]. Each model allowed the rate of change in cognitive function to shift after the date of the first recorded stroke diagnosis. Each model included effects for the time before stroke (in years since study baseline) and time after stroke (in years since stroke diagnosis). An interaction term between time after stroke and lifestyle score was used to examine the effect of lifestyle score on the annual rate of cognitive decline after incident stroke.
We also investigated whether the participant’s age, sex, and race modify the relationship between lifestyle score and cognitive decline by evaluating the significance of the interaction between lifestyle score, age, sex, and race in multivariable-adjusted models.
Furthermore, we conducted additional analyses on participants who underwent magnetic resonance imaging (MRI) [38, 39] assessments after incident stroke to explore the role of stroke severity in our associations. We focused on white matter hyperintensities (WMH) volumes as a proxy of stroke severity because of their role in cognitive impairment of vascular origin [40]. We did two analyses: First, we adjusted our multivariable model by WMH volumes when we investigated the association of lifestyle score pre-incident-stroke with cognitive decline after stroke. Second, we evaluated the interaction term between WMH volumes and the lifestyle score in relation to cognitive decline.
About one-third of participants with incident stroke did not respond to dietary study prior to stroke introducing missing data for the MIND score in our investigation, while information on other lifestyle factors (e.g., cognitive activity, physical activity, and smoking history) was available in all study participants. To avoid potential selection bias by excluding people with no dietary information as well as avoiding decreasing the power of our study, we imputed the missing values using a single imputation method through Multivariate Imputation by Chained Equations (MICE) [41]. To maximize the accuracy of our imputation, we employed a wide range of predictors related to the MIND diet, such as age, sex, race, education, physical activity, cognitive activity, and smoking status in the imputation matrix. In addition, we conducted sensitivity analyses evaluating the relationship between the lifestyle score and cognitive decline in the sample without missing/imputed data of MIND score given statistical uncertainty of the imputation method. In these sensitivity analyses, we repeated three primary analyses (e.g., lifestyle score pre-incident stroke, lifestyle score post-prevalent stroke, and changes in the lifestyle score from pre- to post-incident stroke) in participants with no missing data in the MIND diet score.
Analyses were performed using R statistical computing, version 4.1 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Table 1 presents the demographic and lifestyle characteristics of participants with the incident and prevalent stroke in CHAP. Lifestyle factors in participants who developed stroke during the study follow-up (e.g., incident stroke) were assessed before the stroke event. In participants who had a stroke before being enrolled in the study (e.g., prevalent stroke), lifestyle factors were assessed after the stroke. In the incident stroke group, participants were on average 78.2 years old, 39.9% were men, and in addition to stroke, 63.4% had another a comorbidity (e.g., heart disease, diabetes, or cancer). About 17.5% of participants in the incident group were current smokers before the stroke event and engaged in physical activity an average of 75 minutes per week. In the prevalent stroke group, the mean age at stroke was 74.9 years, 39.7% were men, and 55.3% had another comorbidity in addition to stroke. The median of physical activity was 25 minutes per week, and 11.8% were smokers. The contribution of each lifestyle factor pre-incident stroke and post-prevalent stroke to the lifestyle score are shown in Supplementary Table 2.
Demographic and clinical characteristics of study population
CHAP, Chicago Health and Aging Project; MIND, Mediterranean-DASH Diet Intervention for Neurodegenerative Delay diet score. For continuous variables, data are show as mean (SD) or median [inter-quartile range]; for categorical variables, data are given as absolute numbers (proportions). Comorbidities includes heart disease, cancer, and diabetes. The assessment of lifestyle factors in the incident group was pre-incident-stroke and in the prevalent group was post-prevalent-stroke.
Table 2 presents the association of the lifestyle score pre-incident stroke with the annual rate of change in global cognition after stroke. A healthy lifestyle score pre-incident stroke was associated with a slower rate of cognitive decline. One additional healthy behavior in the lifestyle score was associated with 0.021 (95% CI 0.006, 0.036) standard units’ slower decline in global cognition per year. In addition, participants with 3–4 healthy lifestyle factors pre-incident stroke had a slower cognitive decline by 0.046 units/year (95% CI 0.010, 0.083) after stroke compared to participants with 0–1 healthy lifestyle factor. A similar pattern of association was observed for the lifestyle score pre-incident stroke and cognitive decline after ischemic stroke.
Association of a lifestyle score pre-incident stroke with the annual rate of change in global cognition
All strokes includes both hemorrhagic and ischemic. Continuous refers to one additional healthy behavior in the lifestyle score. Models were adjusted by age, sex, race, education, comorbidities, and time. Lifestyle pre-incident stroke is cumulatively averaged of each lifestyle factor before the stroke.
Table 3 presents the association of the lifestyle score post-prevalent stroke with the annual rate of change in global cognition after stroke. A healthy lifestyle score post-prevalent stroke was not significantly associated with a slower rate of cognitive decline. The β estimate (95% CI) for participants with 3–4 healthy factors compared to those with 0–1 were 0.004 (–0.045, 0.052). Similarly, no associations between lifestyle score post-prevalent stroke and cognitive decline were observed when we focused on participants with ischemic stroke.
Association of a lifestyle score post-prevalent stroke with the annual rate of change in global cognition
All strokes includes both hemorrhagic and ischemic. Continuous refers to one additional healthy behavior in the lifestyle score. Models were adjusted by age, sex, race, education, comorbidities, time, and duration in years from stroke to lifestyle assessment.
Table 4 presents the association of changes in the lifestyle score from pre-incident stroke to post-incident stroke with the annual rate of change in global cognition after stroke. The absolute difference in lifestyle scores before and after incident stroke is shown in Supplementary Figures 2A and 2B. About 56.5% of the sample had a different lifestyle score after incident stroke, with 33.5% having a lower score. Individuals who deteriorated their lifestyle quality (i.e., decreased the lifestyle score) after the stroke had a faster decline in their global cognitive abilities by 0.051 units per year (β –0.051, 95% CI –0.090, –0.012) compared to participants who did not change the lifestyle score. Increasing the adherence to healthy factors after stroke event was not associated with significant changes in global cognition when we compared to participants who had no changes in lifestyle score pre- and post-incident stroke (β 0.007, 95% CI –0.028, 0.042). A similar pattern of association was observed for changes in lifestyle score before and after ischemic stroke with cognitive decline.
Association of a change in healthy lifestyle before and after incident stroke event with the annual rate of change in global cognition
All strokes includes both hemorrhagic and ischemic. Models adjusted by age, sex, race, education, comorbidities, time, lifestyle score pre-stroke, and duration in years from stroke to lifestyle assessment after stroke.
Figure 1 presents the predicted 15-year rates of change in global cognition for a typical stroke survivor in CHAP. Figure 1A shows the trajectories of global cognition after stroke by lifestyle score pre-incident stroke, where an individual with 0–1 healthy lifestyle factor pre-incident stroke had a rate of cognitive decline by –0.097 units/year, and a participant with 3–4 healthy factors had a rate of –0.051 units/year or 47.7% slower (p-value 0.01). Figure 1B shows no statistical differences in trajectories of cognition by categories of lifestyle score post-stroke (p-value 0.83) among prevalent strokes. Figure 1C shows trajectories of global cognition by changes in lifestyle score before and after incident stroke. A study participant with 0–1 healthy lifestyle factor who had no changes in healthy lifestyle score before and after the incident stroke had a rate of cognitive change of –0.108 units/year, and those who decreased the lifestyle score (range: –3 to –1) had a rate of decline by –0.159 units/year or 47.1% faster (p-value 0.01).
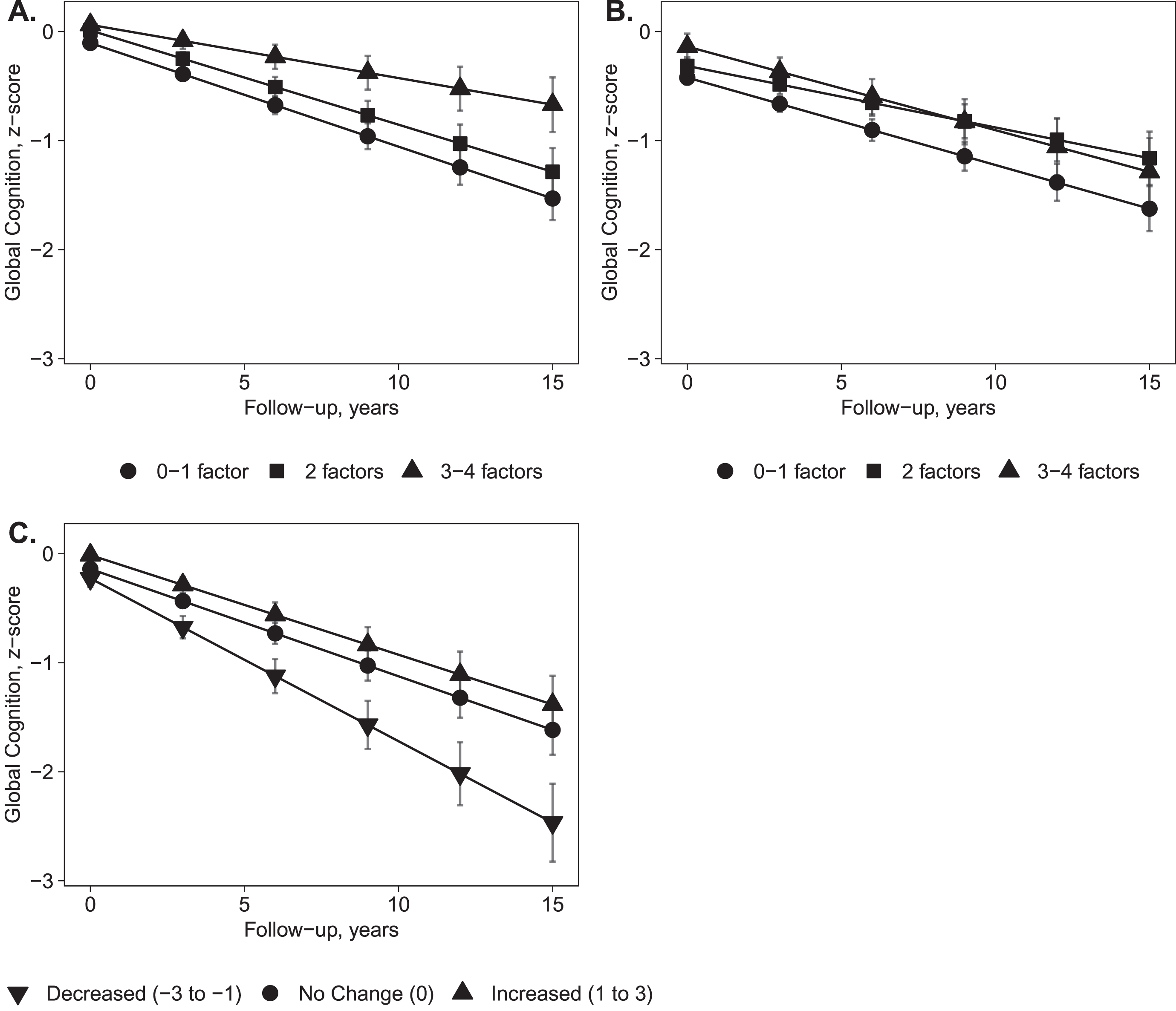
Predicted 15-year rates (SE) of change in global cognition for a typical stroke survivor in Chicago Health and Aging Project. A) Trajectories of global cognition after stroke by lifestyle score pre-incident stroke. Participants with 0–1 low-risk lifestyle factors pre-incident stroke had a rate of cognitive decline by –0.097 units/year, and those with 3–4 low-risk factors had a rate of –0.051 units/year or 47.7% slower (p = 0.01). B) Trajectories of global cognition by lifestyle score post-prevalent stroke. Participants with 0–1 low-risk lifestyle factors post-prevalent stroke had a rate of cognitive decline by –0.071 units/year, and those with 3–4 low-risk factors had a rate of –0.066 units/year or 7.5% slower (p = 0.83). C) Trajectories of global cognition by changes in lifestyle score before and after incident stroke. Participants with 0–1 low-risk lifestyle factors and no changes in lifestyle score before and after incident stroke had a rate of cognitive change of –0.108 units/year, and those who decreased the lifestyle score (range: –3 to –1) had a rate of –0.159 units/year or 47.1% faster (p = 0.01).
We found no evidence that the impact of lifestyle pre-incident stroke on cognitive decline differed by age at a stroke, sex, and race (p-values for interaction term > 0.10). Adjusting by WMH did not attenuate the relationship between lifestyle score pre-incident-stroke and cognitive decline after stroke (β 0.023, 95% CI 0.001, 0.044). Also, there was no significant interaction term (p-value 0.85) between WMH. Excluding participants with imputed/missing data on the MIND score did attenuate the β-estimates to a small degree and broadened the confidence interval since the sample size became smaller (Supplementary Tables 3–5), but results remained similar and significant in people with ischemic stroke.
DISCUSSION
In this study, we focused on individuals with stroke, part of a large population-based cohort study in the U.S., to investigate the influence of a healthy lifestyle— defined by maintaining a high-quality diet, being physically and cognitively active, and abstaining from smoking— on the rate of cognitive decline. We found that an overall healthy lifestyle pre-stroke was associated with a slower rate of cognitive decline after the stroke event. Specifically, stroke patients with 3–4 healthy lifestyle factors pre-incident stroke had an annual rate of cognitive decline 47.7% slower than those with 0 or 1 healthy factor. In contrast, a higher lifestyle score post-stroke was not associated with a slower rate of cognitive decline. However, deteriorating the lifestyle quality from pre- to post-stroke was associated with a faster cognitive decline.
To date, studies investigating the impact of lifestyle factors on people living with stroke have been centralized on the prevention of recurrent stroke [42, 43], whereas research on cognitive impairment and dementia is largely absent. The American Heart Association recommends lifestyle modification as part of the comprehensive post-stroke care to reduce the risk of recurrent stroke and premature mortality in people living with stroke [44]. Our investigation extends the current literature on stroke outcomes by showing that adherence to an overall healthy lifestyle may also be beneficial in slowing the rate of cognitive decline in people living with stroke. However, our data suggest that the benefit of a healthy lifestyle on cognitive decline after stroke is attributed to lifestyle factors pre-incident stroke since lifestyle post-prevalent stroke was not associated with cognitive performance in our study. These results emphasize the importance of primary prevention (e.g., lifestyle before the stroke). Our findings align with an early investigation in Europe, the Rotterdam Study, showing that pre-stroke cardiovascular risk factors accounted for a large proportion of recurrent stroke and dementia after stroke [45]. In this study, pre-stroke cardiovascular risk factors included diabetes, body mass index, smoking, and hypertension, and the authors followed 1,237 patients with incident stroke for recurrent stroke and dementia [45]. However, we should not undervalue the role of lifestyle after stroke. Our analysis of lifestyle changes pre- and post-stroke showed that stroke survivors who deteriorated their lifestyle quality after the stroke had a faster cognitive decline. However, additional studies are necessary to evaluate the role of lifestyle factors post-stroke, as well as changes in lifestyle factors from pre- to post-stroke on cognition and risk of dementia.
Studies that focus on secondary prevention of stroke outcomes often assess risk factors at the time of stroke [46]. However, this approach could be problematic because stroke itself may promote changes in lifestyle factors [45, 47–49]. In addition to lifestyle changes, the type of stroke (e.g., ischemic, hemorrhagic) may impact cognition differentially [50, 51]. For example, a recent study investigating the risk of dementia among stroke survivors of ischemic or hemorrhagic stroke showed that the risk of dementia was 1.72 times higher after ischemic stroke, 2.70 after intracerebral hemorrhage compared to a general population [50]. In our investigation, we studied the lifestyle factors pre-incident stroke, post-prevalent stroke, and changes pre- and post-incident stroke on cognitive decline. We also focused our investigation separately on ischemic stroke.
Strengths of our study include a large study population of stroke survivors, availability of lifestyle factors pre- and post-stroke, the long-term follow-up after stroke, and the determination of cognitive functioning by trained technicians who employed objective assessments of cognition. Our study is advantageous compared to hospital-based studies because we were able to determine the adherence to lifestyle factors years before stroke development and study lifestyle pre-stroke with cognition. Several limitations of this study must be noted. First, individuals included in the analysis may have had a mild stroke because they had survived the stroke and could be part of our population-based study, which required them to respond to several questionnaires and cognitive tests. Therefore, the results of this study cannot be generalizable to all stroke populations. Stroke severity may impact our results since the association we observe could be attributed to the type of stroke. We conducted a series of analyses to explore this limitation, including: 1) adjustment by WMH volumes after stroke (although the sample size was limited n = 51), 2) the interaction of lifestyle score with WMH volumes, 3) controlling for comorbidities (e.g., diabetes, heart disease, and cancer), and 4) separate analyses for ischemic stroke, excluding hemorrhagic stroke. Second, assessments of lifestyle factors were based on self-reports, which are prone to measurement errors; however, these questionnaires have been validated [22, 28], and additionally, we computed the cumulative average of each lifestyle factor to account for the misclassification [34, 35]. Third, we imputed our missing dietary data, which may lead to misclassification; however, we repeated our analysis in participants with no missing data. Fourth, our results and conclusions are based on an observational study, and we must not assume causality. Based on the observation data, we cannot determine the exact date after stroke when the lifestyle change occurred or whether the change in lifestyle from pre- to post-stroke was intentional or unintentional, demanding an intervention study design. Fifth, while we focus on combining lifestyle factors into a composite score, investigating these factors individually may provide valuable information on the mechanisms concerning lifestyle, cognition, and dementia. Furthermore, in light of these mechanisms, future research shall focus on individual cognitive tests (e.g., episodic memory) in addition to global cognition or dementia. Sixth, although we adjusted our multivariable models for a wide range of potential confounders, residual (or unmeasured) confounding may still be present in our study.
In conclusion, a healthy lifestyle pre-stroke was associated with a slower rate of cognitive decline in stroke survivors, highlighting the importance of primary prevention. After the stroke, changes in lifestyle behaviors may influence the cognitive abilities of older adults as they age.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the National Institutes On Aging of the National Institute of Health under Award Number: R21AG070287, R01AG051635, RF1AG057532, R01AG058679, and R01AG073627; and the Rush University (Cohn Fellowship). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health or Rush University.