
Abstract
Background:
In the United States, dementia specialty centers affiliated with centers of excellence for research hold promise as locations to develop innovative, holistic care in care systems otherwise siloed by discipline or payer.
Objective:
We conducted foundational research to inform development of patient-and family-centered palliative care interventions for dementia specialty centers.
Methods:
We interviewed persons living with dementia (PLWD), current, and former care partners (CP) recruited from a specialty dementia clinic and purposively selected for variation across disease syndrome and stage. A framework method of thematic analysis included coding, analytic matrices, and pattern mapping.
Results:
40 participants included 9 PLWD, 16 current CPs, and 15 former CPs of decedents; 48% impacted by Alzheimer’s disease dementia. While help from family, support groups and adult day centers, paid caregiving, and sensitive clinical care were invaluable to PLWD, CPs, or both, these supports were insufficient to navigate the extensive challenges. Disease-oriented sources of distress included symptoms, functional impairment and falls, uncertainty and loss, and inaccessible care. Social and relational challenges included constrained personal and professional opportunities. The obligation and toll of giving or receiving caregiving were challenging. Clinical care challenges for PLWD and/or CPs included care fragmentation, insufficient guidance to inform planning and need for expert interdisciplinary clinical care at home.
Conclusion:
Findings highlight the breadth and gravity of gaps, which surpass the disciplinary focus of either behavioral neurology or palliative care alone. Results can inform the development of novel interventions to add principles of geriatrics and neuropalliative care to dementia care.
INTRODUCTION
In the United States, more than 1 in 9 people over the age of 65 are living with dementia syndromes and more than 11 million family and friends serve as care partners [1]. By 2050 over 12.7 million Americans will be living with dementia. While researchers work towards treatments and cures, given the increasing prevalence of people living with dementia (PLWD), we need to simultaneously develop evidence-based approaches to ameliorate suffering and support the specific needs of PLWD and their care partners (CPs).
PLWD are often shuttled between clinical silos: they may raise concerns to primary care clinicians, who may refer them to neurologists for diagnosis, to palliative care for help with advance care planning, to geriatrics or housecalls practices once homebound, and to hospice for end-of-life care. Dementia specialty centers, especially those affiliated with centers of excellence for research, hold promise as locations to develop innovative, holistic care in a care system otherwise siloed by discipline or payer. In the United States, there are 33 Alzheimer’s Disease Research Centers (ADRCs) funded by the National Institute on Aging that set standards for dementia care in the context of conducting research that advances understanding of prevention, diagnosis, and treatment [2]. Though ADRCs vary substantially in structure, disciplinary leadership, and goals based on their local clinical context, they participate in the collection of standardized data for a subset of patients and therefore share some similarities in assessment methods. The 2017 NIH Alzheimer’s Disease Centers Panel Recommendations newly recommended they engage PLWD and CPs with the goal of “improving services to patients and caregivers across the spectrum of disease” [3] to facilitate achieving the goals of the National Plan to Address Alzheimer’s Disease [4]. This makes specialty dementia centers affiliated with ADRCs crucial locations for developing evidence-based dementia care services tailored to the needs of PLWD and CPs that can be further adapted and disseminated to other sites in the future.
One promising path towards these goals is developing and implementing a robust model of dementia palliative care. Palliative care focuses on reducing suffering and improving quality of life by attending to multi-dimensional sources of distress for seriously ill individuals and families [5–7]. There is international consensus around the importance of integrating palliative approaches into the care of persons with dementia syndromes [8] and into the full scope of neurologic practice, often via the emerging subspecialty of neuropalliative care [9–18]. There are multiple potential avenues for integrating neuropalliative care principles into dementia care, including training dementia clinicians in practices like serious illness communication [12] or embedding a specialty palliative care outpatient clinic within a dementia clinic [19]. Yet to date, the majority of the evidence for dementia palliative care interventions come from facility settings or end-of-life care [20]. To build effective neuropalliative care interventions for dementia, we need to understand setting-specific sources of support, ongoing challenges that need to be addressed, and other opportunities to improve quality of life for PLWD and CPs.
We conducted a qualitative study to comprehensively explore challenges and supports experienced by PLWD and CPs associated with a specialty dementia center to understand strengths to build from and gaps to be filled. Prior qualitative research on the lived experiences of PLWD, current or former CPs worldwide detail the stigma and impact of a diagnosis on the PLWD, desire for additional support after diagnosis, lack of knowledge and support from primary care providers regarding how to find additional services and supports, appreciation when health care providers displayed sensitivity and validated feelings, and need for organizational structures that ensure PLWD are cared for in a dementia-friendly environment by a dementia-trained workforce [21–23]. A recent scoping review of evidence for community-based dementia palliative care services found the integration of dementia and palliative care services have been found to improve care for PLWD and CPs, but that research is needed to identify key components of dementia palliative care [20]. The design was informed by the National Consensus Project Clinical Practice Guidelines for Quality Palliative Care, which defines processes and practices for any clinician to attend to palliative care needs of seriously ill people and care partners using a biopsychosocial framework detailing biological and physical, psychological, social, spiritual, and cultural aspects of care [24, 25]. Our findings provide foundational data to develop novel palliative care-informed interventions to improve care within ADRCs.
METHODS
Design
We carried out a descriptive qualitative study [26] using in-depth interviews [27] with PLWD and CPs associated with a specialty dementia center to conduct foundational research to inform developing palliative care interventions within the ADRC-affiliated center. The study was approved by the University of California San Francisco (UCSF) Institutional Review Board and adheres to Consolidated Criteria For Reporting Qualitative Studies (COREQ; Supplementary Material 1) [28].
Site
The specialty dementia center is located within a quaternary medical center and offers diagnostic and longitudinal care for persons with cognitive and behavioral symptoms and their families. Patients and families can choose to enroll in research through the affiliated ADRD or other research programs or can receive insurance-reimbursed clinical care. Most insurance carriers are accepted using Medicare; rarely, patients and families may pay out-of-pocket for consultative and clinical care, such as when they travel from abroad and have no insurance in the United States. Neurologists typically provide longitudinal clinical care, with additional evaluation and care available from specialists with expertise in neuropsychology, nursing, social work, genetics, geriatrics, geriatric psychiatry, physical therapy, occupational therapy, and speech therapy, depending on the needs of the patient. Patients are referred to the specialty dementia center by regional primary care physicians, general neurologists, or other specialists, or can self-refer if insurance carriers do not require provider referral. Patients have a median of 2 appointments at the specialty dementia center (range 1–30); approximately 20% of patients have only a single consultative visit [29].
Participants
We purposively sampled three perspectives among PLWD and CPs associated with the specialty dementia center: 1) PLWD with mild-to-moderate disease who could self-report; 2) current CPs of community-dwelling PLWD with mild-to-moderate disease; or 3) former CPs of a PLWD who had died 3–12 months earlier who could reflect on the entire disease journey. We aimed to recruit at least 50% with experience with Alzheimer’s disease dementia and the rest with less common syndromes. We identified potential participants through chart review and approached clinicians for referral and approval. The study coordinator contacted the associated clinic provider to request permission to approach and to review eligibility (including diagnosis and severity). Once approved, the study coordinator called the candidate up to three times. With all participants, we used a teach-to-goal informed consent process that assesses decisional capacity by asking the prospective participant to answer questions about or explain the main study elements [30].
Study setting
Between November 2018 and September 2019, a PhD sociologist (SBG) interviewed 9 PLWD, 16 current CPs, and 15 former CPs of decedents. Three current CPs and PLWD were dyads. Interviews were conducted by phone or in-person based on participant preference.
Interview topics
Questions focused on key experiences along the PLWD’s disease trajectory, challenges and sources of distress, and supports that did or could have helped (Supplementary Material 2). Probes related to domains of the guiding palliative care biopsychosocial framework [24]: challenges or supports related to physical, behavioral, psychological, social, cultural, spiritual/religious, legal, financial, ethical aspects of their experience, as well as memory care services or preparation for end-of-life. Interviews ended with a demographic survey to fulfill funder reporting needs and to facilitate descriptions of diversity in lived experience. An interdisciplinary team of social scientists and physicians in behavioral neurology, geriatrics, and palliative medicine developed the interview framework, which we piloted and refined before use.
Analyses
All interviews were recorded, transcribed, and identifying information removed. Our framework method [31] for thematic analysis included immersion in the data, coding to label units of meaning, examining patterns, writing memos, diagramming, and interpreting data [32, 33]. Methods to maintain transparency and rigor are detailed in Supplementary Material 1. Four authors (KLH, CSR, SBG, MH) iteratively developed and refined codes. We first coded all explicit statements of challenges, things that helped (empirical supports), or things participants thought might help or recommended for others (hypothetical supports). We then identified and coded the source of the challenges or supports. One author (MH) applied the final codebook (Supplementary Material 3) to all data using ATLAS.ti [34]. We used coded data to extract quotations for analysis and to map patterns across cases [35]. Throughout this process, we used analytic matrices [31] and memos [32] to reflexively summarize and analyze data and to consider disconfirming evidence [36, 37].
RESULTS
Participants
The 40 participants were predominantly white (75%), well-educated (55% with master’s degrees or more), and well-resourced (50% with annual incomes over $100,000); this is comparable to the demographics of the population of patients seen at the specialty dementia center [29]. The sample did, however, include 3 participants who self-identified as Black (one further specified Creole), 4 as Asian, 1 as Arab American, 1 as Italian; 3 who referred to a spouse or domestic partner of the same gender; 7 who self-identified as having less education than a college diploma; and 8 participants categorized as very low income based on their self-reported income category compared to the U.S. Department of Housing and Urban Development Income Limits for the San Francisco Metro Region (in 2019, $56,400 for a household of 1 and 64,500 for a household of 2) [38]. In accordance with our purposive sampling, 48% participants had experience (as PLWD or CP) with a primary diagnosis of Alzheimer’s disease (AD); the remainder had experience with less common syndromes: Lewy body disease (LBD); behavioral variant frontotemporal dementia (bvFTD), vascular dementia (VaD), corticobasal syndrome (CBS), logopenic variant or nonfluent variant primary progressive aphasia (lvPPA or nfvPPA), progressive supranuclear palsy (PSP), posterior cortical atrophy (PCA); 10 participants had actual or hypothesized copathologies (Table 1). CPs were comprised of spouses (n = 23), a domestic partner, and 7 adult children.
Demographics of interview participants: persons living with dementia (PLWD), current care partners (CPs) of PLWD, and former CPs of decedents who died with severe or advanced disease
1Race/ethnicity were collected to report per funder requirements and categorized based on NIH reporting categories. 2Represents all former caregivers. 3Other syndromes: PLWD: 1 nfvPPA/PSP (nonfluent variant primary progressive aphasia/progressive supranuclear palsy); care partners: 2 lvPPA (logopenic variant primary progressive aphasia), 2 PSP (progressive supranuclear palsy), 2 CBS (corticobasal syndrome - 1 mixed), 2 PCA (posterior cortical atrophy - 1 mixed); 3Mixed syndromes or copathologies: PLWD: 2 AD/VaD (Alzheimer’s disease/vascular dementia); care partners: 1 CBS/PCA (corticobasal syndrome/ posterior cortical atrophy), 3 AD/LBD (Alzheimer’s disease/Lewy body disease), 1 AD/PCA (Alzheimer’s disease/posterior cortical atrophy), 1 lvPPA/AD (logopenic variant primary progressive aphasia/ Alzheimer’s disease).
Below we summarize themes within the four categories of challenges and supports shared by participants: the disease itself, relational or social changes, caregiving, or clinical care (Fig. 1). We provide a summary inventory and illustrative quotes in Tables 2 and 3; additional quotes are available in Supplementary Material 4. Quotes are cited by participant type (p = PLWD, ccp = current care partner, fcp = former care partner) and participant number.
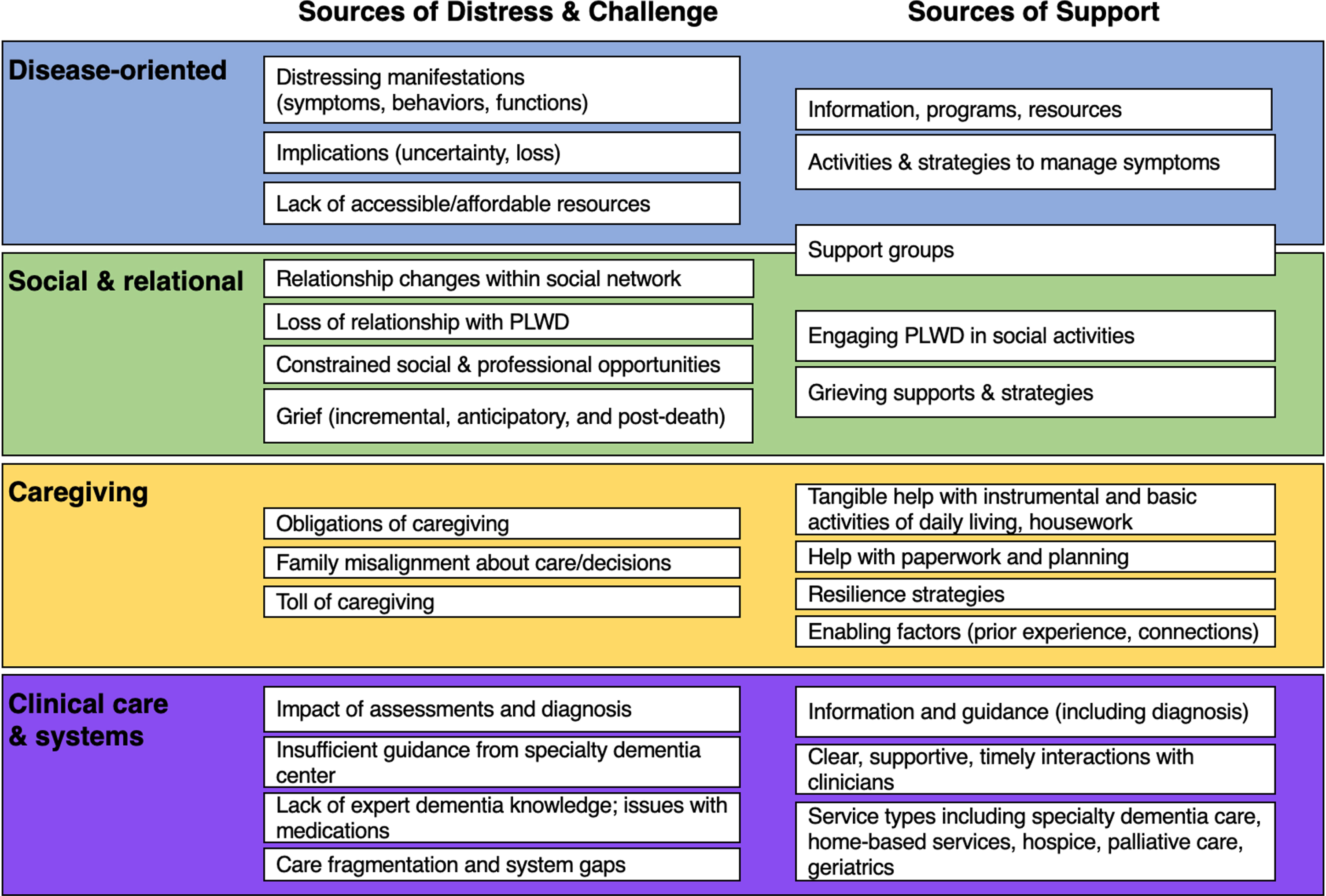
Visual summary of findings organized by theme. This figure summarizes qualitative findings from interviews with persons living with dementia, current care partners, or former care partners of people who died from dementia. We identified 4 major sources of challenge or support: related to the disease, social and relational changes, caregiving, and clinical care or care systems. Each box summarizes a subtheme within each category of challenges or supports.
Challenges or sources of distress reported by PLWD or care partners
Sources of empirical or hypothetical support reported by PLWD or CPs
Challenges
Every participant reported at least one type of challenge; over half the sample reported challenges from all four categories (Table 2, Supplementary Material 4). CPs identified more challenges than PLWD, and former CPs focused on challenges relevant to late-stage caregiving and caregiving burden.
Disease-oriented challenges were discussed by nearly all of the participants. Challenges related to disease manifestations such as symptoms, functional impairments (especially falls) and behaviors were common and distressing: “Last night, in the middle of the night, he was hitting me and kind of screaming in his sleep, and I tried to wake him up. It seemed, in his dream, only to provoke him more and he really became physically violent” (ccp25). PLWD and current CPs shared their fears about disease progression, including loss of independence, dependence in activities of daily living (ADLs), and distressing behaviors. Occasionally, participants talked about how other illnesses (e.g., cancer) interacted with and complicated living with dementia: “On top of it all, he can’t see” (ccp19).
Participants were frustrated by the uncertainty of the speed of decline, duration, symptoms, and intensity of the disease: many felt anxious not knowing. As a bereaved husband of a wife with CBS/PCA said, “I’m on call 24 hours a day. I’m dealing with something I am clueless about and I don’t know where it’s going and how fast it’s going and my wife is disappearing. It’s not an easy thing to navigate” (fcp05). The prognostic uncertainty made it difficult for participants to plan for retirement, job leave, or paid caregiving. Losses for PLWD included loss of control and privacy (e.g., help with bathing) and especially independence; loss of ability to drive was often lamented. Some PLWD expressed awareness, frustration, and shame at how the disease changes their mental and physical function: “it’s a big downer to know that I have Alzheimer’s. It’s embarrassing” (p04). CPs also expressed distress at the losses caused by the disease.
Many participants described a lack of accessible or affordable resources for navigating the disease. Participants often mentioned concerns about the cost of paid caregiving at home or in a facility, such as this husband of a wife with PSP: “my concern is if we had to send my wife to the nursing home . . . the financial . . . that would be a big burden” (ccp28). Navigating clinical settings became taxing as impairments grew, sometimes resulting in patient falls, distress, and missed appointments. Support groups and clinical appointments that occurred during work hours created challenges for employed participants such as PLWD with early-onset syndromes or adult children CPs. Many support or activity programs for PLWD could not accommodate later-stage disease.
Social and relational challenges were described by nearly all CP, and by multiple PLWD. Participants were particularly distressed about how the diagnosis and disease changed their relationships: “People, since they know that he has Alzheimer disease, they treat him differently. Like, you know, they think that he’s not capable of fellowship [at church] . . . and then they don’t want to get involved” (ccp02). A few participants indicated the stigma of dementia prevented them from telling friends; one person with AD perceived an acquaintance “thinking of me . . . in a way I don’t think of myself” (p08). As the PLWD lost communication and functional skills, CPs described the challenge of role changes and loss of their vision for the future. Spousal CPs grieved losing their prior relationship with the PLWD. Former CP experienced deep distress of grief after the PLWD died: “I’m grieving what I had. The way we were . . . the way he was . . . There’s times when I just, I literally hurt inside. I actually feel pain. I feel hurt and I can’t always make it go away and I’m trying to recreate my life. And how do you recreate your life when you’re 73?” (fcp06).
For most participants, the disease or caregiving constrained social and professional opportunities. For example, a wife CP of a person living with bvFTD said, “the social issues are what are the worst, because [my husband], he says inappropriate things in front of people, and he makes sometimes inappropriate remarks, especially when it comes to young women, and so we don’t do a lot of social things because of that reason” (ccp29). Some CP described friends and family becoming unwilling to engage the PLWD or adapt activities. PLWD or CP who were employed communicated distress about losing professional opportunities amid disease progression or mounting caregiving responsibilities: one bereaved husband CP of a man with AD/VaD noted: “You have to make your choices. Do you get your report at work in on time? Or do you run home at the end of your day to make sure your husband is okay?” (fcp04). Many of those who lost or reduced their employment expressed sadness about associated losses of meaning, travel, and income.
Challenges of caregiving were described by all CPs; these related to caregiving activities and the CP role. A common theme was the CP’s overriding sense of obligation: “Caregiving was not my big, not my strong suit,<laughs> and I really hated it, and I hated it and then I felt guilty about it and I was back and forth and then I would just–I would even cry, because I think I’m a terrible woman” (fcp06). A daughter CP of a mother spoke of cultural norms influencing her sense of obligation, “When Black people raise their children, they teach their children always take care of their mother. That’s a lot. It’s a lot. It’s a lot, and that means do whatever is necessary, and, you know, I don’t know if you know this, but a lot of Black people will not put their parents in nursing homes and leave them there” (ccp03). Participants described taking on a myriad of responsibilities as CP, including catching mistakes from clinicians with inadequate dementia expertise. Many faced steep learning curves at home, becoming solely responsible for decision-making, navigating legal issues, learning ADL support skills, and household and financial management. CPs additionally described the challenges of family disagreements about care and decisions: a current CP of a wife with LBD said, “The one place I wanted to move her to, it was in a house, in a home, right near the park . . . and she got it into her head those were the woods. “I don’t want to be near the woods,” and I couldn’t get through to her that it was the park . . . I could’ve practically walked to that place, and that’s what I really wanted. It would’ve been the right thing for me in terms of convenience. But I acquiesced to that, you know” (cc10).
For most, caregiving exacted a substantial toll. CPs spoke of losing their freedom and identity: “I actually thought about suicide at that time. . . . I was pretty sure where [Spouse] was going . . . and then having lost my job . . . I really kind of lost my identity” (fcp06). Many CPs became emotional describing physical (providing ADL help), mental (sleep disruption, managing behaviors), emotional (distress, grief, burnout, guilt) and financial (loss of work, exorbitant cost of paid care) challenges. One a daughter CP of a father said, “it was definitely a challenge. Moreso as he could give less back. You know, going over there and, like < chokes up > sitting and not feeling like you’re doing much or helping the situation or helping him. . . . Like, I wondered, like, sometimes he would yell at me and, you know, yell me out of the house, and it’s like I knew he didn’t mean it and I knew it was the disease, but did he, you know, maybe I should just not go, because I clearly agitate him, and yet if I don’t go, nobody goes” (fc08). The uncertainty of caring for a PLWD intensified these challenges.
Clinical care and care system-oriented challenges were described by most participants, whose experiences illustrated the challenges of navigating a fragmented care system: “we would see a social worker, or a therapist, and they were wonderful. We’d sit there and talk and everything. And they said they would follow up with us, and they never did. We never heard from anybody” (fc06). PLWD and CP described the assessments and diagnosis at the specialty dementia clinic as difficult for the PLWD: ““it was distressing to see my loss, say, remembering words and repeating them back” (p08). Most said that receiving a diagnosis was surprising and concerning; two PLWD considered suicide in reaction to the diagnosis.
Many participants reported that specialty dementia clinicians supplied less guidance than they wanted about disease progression or stage: “I would like to ask [his doctor], you know, “What’s the end game? What’s going to happen?” and nobody’s able to tell me, and maybe they can’t” (ccp10). Some participants also described frustration with clinicians whom they felt had inadequate dementia expertise. Many CPs reported problems with prescribed medications or side effects. A few participants worried that they received lower-quality care in hospitals because of the dementia diagnosis and/or their signed do-not-resuscitate order.
Supports
All participants discussed empirical or hypothetical sources of support across at least 3 challenge areas; most (30 of 40) discussed supports across all 4 (Table 3, Supplementary Material 4). We report hypothetical supports only if they are not already represented among empirical supports.
Disease-oriented supports. Many participants discussed their appreciation for information, programs, and resources (especially websites and support groups) that enabled them to learn about the disease and symptom management strategies. These were offered by the Alzheimer’s Association, local organizations focused on aging or caregiving, and the specialty dementia clinic. One CP of her mother said, “what I appreciated was being able to read and see what kinds of symptoms and science, hearing other people’s stories. Granted you might learn that going to a group, but the last thing I want is another appointment. I’m going to be home holding her hand” (fc14). Participants affected by rarer syndromes appreciated disease-specific support groups; for example, one CP of a person with LBD said the center, “had an early-onset group, and I’m very grateful for that. That was what I was in. We have some different needs because our partners are younger, and often generationally interested in different things” (cc09). Participants recommended these types of resources for other CPs.
Most participants described activities and strategies that they felt helped to manage symptoms (particularly exercise and social opportunities for PLWD), and to maintain wellness as their or their loved one’s disease progressed. PLWD described benefits of writing things down (e.g., in an appointment book) and having a routine: “I belong to [local running group], it’s a social organization, too. Afterward, we always meet for coffee and talk. And solve all the problems of the world” (p07). CPs described myriad practical techniques to manage caring for PLWD and to manage negative emotions.
Many participants benefited from engaging the PLWD in social activities, including those that were meaningful prior to the diagnosis, adapting as needed as the disease progressed: “we had priests coming by regularly to see my dad, since he couldn’t go to mass anymore–it became harder. . . . Hospice brought people to talk to him . . . the caregivers would play the mass for him, every day, from Rome” (fc08). Others discussed the benefits of new social activities such as an adult day center.
Former CPs shared strategies for managing and honoring grief for the deceased PLWD: “I’d say for the last three months of his life, he was never without [stuffed animal name]. So now I sleep with [stuffed animal name] and it’s kind of comforting” (fcp15). Many appreciated support from family and friends. Multiple CP reported that hospice had offered bereavement services but few had engaged it.
Supports for caregiving included those for CP and for PLWD seeking help with everyday life. As dementia progressed, both PLWD and CPs described appreciating household services for activities that the PWLD used to do or to enable time and energy for caregiving activities: “I now have a housekeeper. He [PLWD] used to do all the housekeeping. I now have a gardener. He used to do most of the heavy gardening, still does light gardening. I have ordered a food service . . . so I rarely go to the grocery store anymore” (ccp19).
Participants received tangible help with caregiving and basic ADL support, such as bathing the PLWD, through friends, family, paid caregivers, or facilities. One current CP of a person with LBD expressed appreciation that a local LGBTQ+organization had received funding to partner with area nursing facilities “doing active education for the providers, you know, just about our needs and our culture . . . We’ve always lived in a straight world, but it’s wonderful to just have that little tiny fishbowl for [Spouse] that I don’t have to explain what my being her partner is and all of that every time” (cc09). Participants also appreciated help navigating programs and paperwork such as disability benefits, Medicaid, and advance directives: “Well, legally I started out by trying to find out what was Medi-Cal, could I qualify for Medi-Cal and that was a labyrinthian procedure . . . There is no way to navigate it without a very, very smart lawyer” (fcp05). Several CPs expressed gratitude they had taken care of financial, legal, and advance care planning prior to the diagnosis, or that they had long-term care insurance for paid caregiving.
Some supports made caregiving easier or more sustainable for the CP. They sustained their resilience through mindset (e.g., living in the present), strong religious faith, counselors and therapists, meditation, exercise, journaling, re-engaging in professional work, and flexible working arrangements. Some CPs benefited from day programs and respite care. Many CPs wished for caregiving supports they did not have, such as a person to stay with the PLWD while the partner traveled, someone to help with activities of daily living, and more (affordable, trustworthy) paid caregiving. As a current CP said, “I’d like to have extra help. For instance, like one or two days, you know, someone could take him out and then I be able to rest, and I know that in realistic, in real life, you cannot keep giving and giving all the time and then not take care of yourself” (ccp02). CPs appreciated resources that facilitated access to needed services, such as prior training in health or dementia care or social connections to healthcare leadership. For example, a person living with nfvPPA/PSP said, “I speak Chinese, and the Chinese community have a lot of help” (p10).
Supports from clinical care or care systems. All participants expressed appreciation for information and guidance from their clinicians: “[Clinician] was really clear about how, “Oh, this is happening neurologically and she can’t perceive the distances right or can’t perceive stepping right or she shuffles stepping instead of stepping normally and so she’s likely to trip on rugs and stuff like that” (fcp26). Many wanted more guidance than they received. Some participants described receiving a diagnosis as helpful for enabling planning: “it’s helpful to know, to not just be in this gray zone . . . Also so we could begin to plan, think about the future” (ccp01). Participants particularly appreciated clear and timely interactions with the clinical team. Many additionally wished that clinicians gave more, earlier, or more frequent advice about planning ahead, advance care planning and CP support.
Clinical services that participants found helpful included the specialty dementia clinic (especially a behavioral symptom clinic), home-based care, hospice, and, occasionally, specialty palliative care. For example, one former CP of a wife with CBS/PCA said, “the medical group had a geriatric doctor come and visit [[Wife]] once a month, very nice guy and that was helpful. I felt like I needed somebody to be helping observe [[Wife’s]] condition because it went up and down” (fc05). Participants wished for more home-based services, having care co-located with other services, care provided to both PWLD and CPs simultaneously, and/or local satellite offices for the dementia specialty center. One current CP said “I would recommend [palliative care]. I think that a chronic illness involves the family. And the quality of the interactions in the home life effect the person. And I think [clinicians] have to deal with the whole system. They have to address the whole system” (ccp25)
DISCUSSION
This qualitative study illuminates the breadth and gravity of the needs reported by PLWDs and CPs associated with a specialty dementia center (summarized in Fig. 1). While support from family and friends, social programs like support groups and adult day centers, paid caregiving, and sensitive, timely, interdisciplinary clinical care were invaluable, these supports were insufficient for navigating the extensive challenges participants faced, which multiplied with disease progression. Sources of distress stemmed from four main sources: the disease, social/relational changes, caregiving, and clinical care/systems. Patients shared distress at the uncertainty of the progression and symptoms of the disease, constrained professional or social opportunities and relationship with spouse, and inaccessible care or support groups (especially if they still worked). Care partners also found these challenging, and additionally shared distress at the obligation and toll of caregiving, desire for clinician guidance to inform planning. Former caregivers articulated appreciation and/or desire for expert interdisciplinary clinical care at home, hospice care to help with imminent death, and distress at incremental anticipatory grief while the PLWD was alive and grief after they died. Both sources of distress and support provide data to inform the development of interventions to reduce suffering and improve quality of life within specialty dementia centers.
Every year, the Alzheimer’s Association publishes a “Facts and Figures” updated aggregation of data on the public health impact of dementia in the United States [1]. Many of our findings among participants associated with a specialty dementia center mirror those in nationally representative data or systematic reviews of qualitative research, such as the distressing symptoms of dementia, challenges with the stigma and impact of diagnosis [21, 22], the desire for prognostic estimates and anticipatory guidance [21, 39–41], the gaps in advance care planning [20, 42], the intensifying demands of caregiving— including negative impacts on CP mental, physical, and financial wellbeing [1, 43–46]— and challenges accessing paid help [47]. Our work also aligns with scoping reviews of qualitative research on dementia end-of-life care, including challenges of caregiving that include loss of relationship with the PLWD and social isolation and impact of caregiving on CP sense of self and wellbeing [48].
Our findings add to the body of qualitative research across the dementia disease course [20, 49]. Using a palliative care lens for study design and analysis, we provide more specific findings and offer concrete, practical guidance for developing interventions in dementia specialty centers. Our work augments prior research by demonstrating both the persistence of common challenges like stigma, falls, progressive functional impairment, desire for prognostic information, and insufficient attention to caregiver wellbeing even among the well-resourced population able to access care within a specialty dementia center and associated services; yet we also highlight how supports and services can reduce these challenges. Notably, system gaps and care fragmentation were ubiquitous. Even when PLWD and CPs attempted to find the best quality care through an ADRC-affiliated specialty dementia center, they experienced further care fragmentation.
Moreover, many participants expressed an unmet desire for home-based care and services. Nationally representative data indicate over 50% of completely or homebound older adults in the United States have dementia, and only 12% of homebound older adults receive home-based services annually, with access being even more tenuous in rural settings [50–54]. Recognition of the importance of including CPs as well as PLWD in the provision of home-based care (either in parallel or sequentially may have increased during the COVID pandemic. For example, home-based health care clinicians vaccinated both homebound patients and CP during the same visit in recognition that the health of the household is essential to the health of the PLWD, and that CPs are limited in their ability to leave the home to obtain their own healthcare [55]. A recent systematic review indicates few studies investigate the impact of home healthcare on outcomes for PLWD [49]. Gaps in access to care could be addressed through targeted outreach to PLWD/CPs, care augmentation in the community or home setting [56–58], depending on risk and management needs, and training and support for home healthcare providers in decision-making and initiating palliative and hospice care [49].
Clinical implications
Though clinical care is often divided into disciplinary silos, the needs of PLWD and CPs are not. This insight appears throughout the interviews with PLWD and CPs here, as well as in a constellation of related quantitative and qualitative studies designed to inform the development of interventions in specialty dementia clinics ([29, 59–61] and Adrion et al., unpublished data). Many sources of distress expressed by CPs and PLWD in this study involved lack of symptom management and guidance around care decisions— gaps that palliative care is well-suited to fill. Yet participants described needs that require expertise traditionally found in clinical disciplines such as behavioral neurology and geriatrics. Participants in our study appreciated the expertise of behavioral neurologists and their interdisciplinary colleagues in the specialty dementia clinic (e.g., geriatric psychiatry, neuropsychology, nursing, social work) in explaining the source of behaviors and management strategies, dementia-appropriate medication, diagnosis of rare diseases, and referring to syndrome-specific support groups. A 2022 position paper on neuropalliative care from the American Academy of Neurology [16], and a 2021 position paper on ethical considerations in dementia [62] highlight the importance of serious illness communication, advance care planning, decision-making in light of changing capacity, and support for hospice transitions. Participants in our study also commonly mentioned challenges from loss of independence, falls, functional impairment (including incontinence), multimorbidity, and polypharmacy/medication issues, problems that are often addressed in geriatric care. Importantly, no single discipline encompasses all domains of needs expressed by participants, even in a well-resourced study population able to obtain care from a top medical center. As such, future interventions in specialty dementia centers must draw on all of these disciplines. Integrating a geriatric neuropalliative care approach to specialty dementia care may provide care that is most aligned with the needs described by PLWD and CP in this study [63, 64].
Drawing on our findings, we recommend an integrated, biopsychosocial geriatric neuropalliative care approach to improve care within specialty dementia centers associated with ADRCs (Fig. 2). Clinical geriatric neuropalliative care interventions tailored to the needs of PLWD and CPs would include the following biopsychosocial elements. 1) Biologic and physical components: calibrated assessments of, and interactions with, CP/PLWD to minimize strain; thoughtful diagnostic disclosure and anticipatory guidance [40], education about and optimal management of disease-related distressing symptoms; advice on adapting to functional changes over time; and provision of accessible home-based services to both CP and PLWD. 2) Psychologic components: regular provision of support groups, including options for CPs caring for severe or advanced-stage disease; encouraging CP attention to their own well-being [65] through self-care and respite, while acknowledging the associated challenges; providing dyadic and individual behavioral health support; and grief support [66]. 3) Social components: ensuring social resources for CP/PLWD are tailored to needs and made accessible; providing help obtaining ADL and IADL assistance; facilitation of meaningful activities for PLWD; and provision of care navigation and help with paperwork. Ideally these trainings and services would be provided in multiple venues (including the home) and formats (in-person, online, in-print, etc.). New functional roles within the dementia specialty care infrastructure will need to be developed within ADRCs that can iteratively identify and address needs, assemble tailored care teams of clinicians, coordinate care across settings, and smooth the dysfunctions of the healthcare delivery system. One such example might be the Care Ecosystem, a telephone and web-enabled intervention to enable health systems and clinics to provide dementia-competent care [67–70].
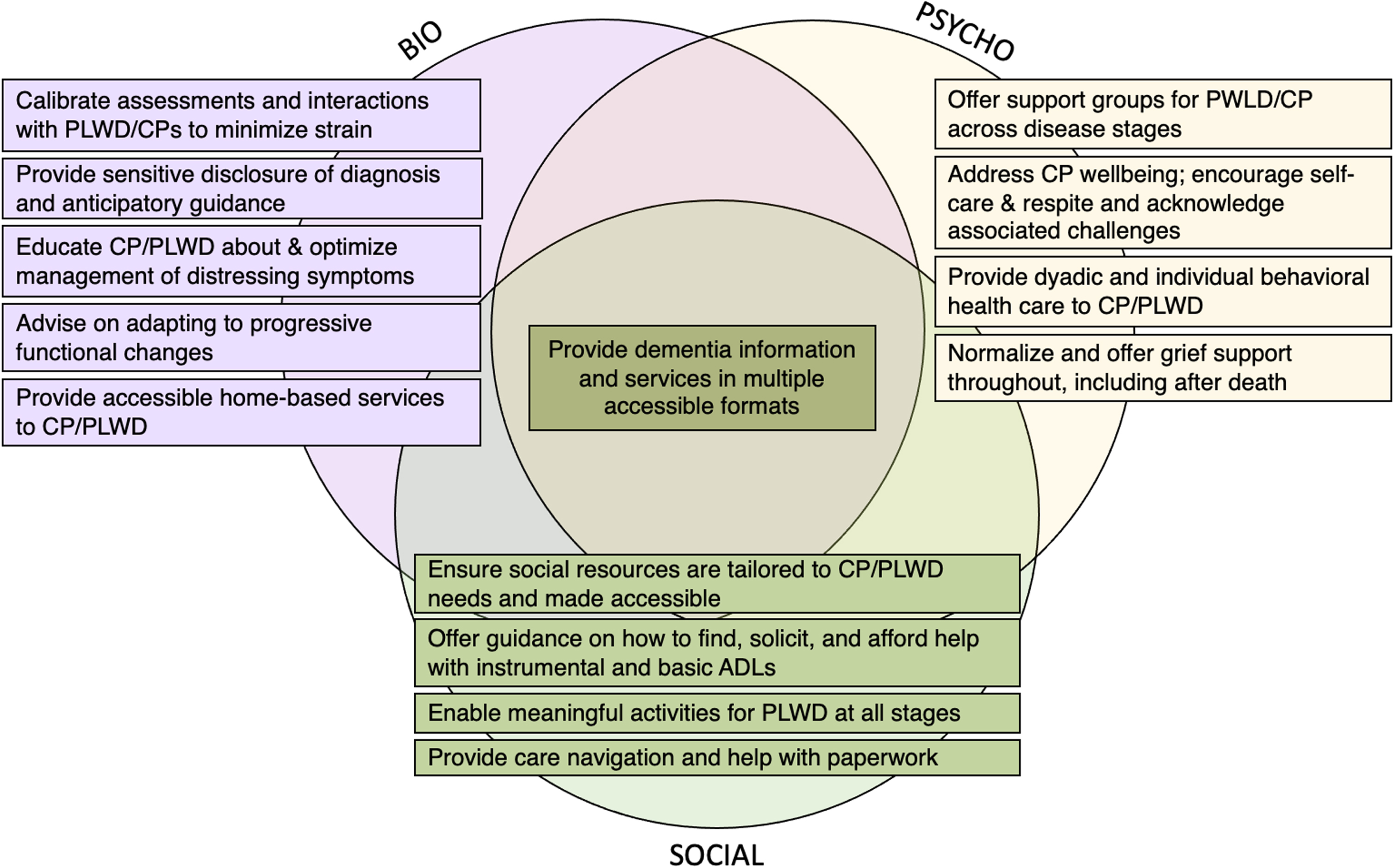
Recommendations for an integrated, biopsychosocial, geriatric neuropalliative care approach to improve care within specialty dementia centers associated with Alzheimer’s Disease Research Centers. This figure summarizes empirically-based, person-and family-centered recommendations for improving care within specialty dementia centers and Alzheimer’s Disease Research Centers, organized around a biopsychosocial framework for geriatric neuropalliative care. Recommendations related to a biological or physical dimension are noted in purple, those related to a psychological dimension are noted in yellow, and those related to the social dimension are noted in green.
In concert with the development and refinement of clinical geriatric neuropalliative care interventions for PLWD/CP affiliated with specialty dementia centers, clinical teams will need supplementary trainings. For example, clinicians in specialty dementia care centers will need training in basic principles of geriatrics and neuropalliative care tailored for dementia [59] and guidelines for referring patients to specialty palliative care and hospice services. Similarly, primary care, palliative care, geriatrics and hospice [71–73] clinicians will need training in how to effectively address specific needs of people with dementia (such as distressing behavioral symptoms) and guidelines for making referrals to specialty dementia centers [74]. All clinicians may need training in grief support. Community outreach groups associated with health care organizations or specialty dementia centers can provide training in normal brain aging and reduce stigma of dementia. Development, implementation, and refinement of these clinical and training interventions in specialty dementia centers, in the context of research, could allow for the development of financial models, business cases, and recommended policies that could enable the spread of geriatric neuropalliative dementia care in community organizations.
Limitations
Our study sample from this single academic medical center lacked nationally representative racial/ethnic and socioeconomic diversity; participants were largely advantaged and well-resourced so their experiences likely do not represent the full breadth of issues PLWD and CPs face. Our participants were heterogenous in other ways, representing different dementia syndromes, disease stages, and roles. The sample size was not sufficiently large to analyze challenges or supports related to family structure, community, or culture. Relatedly, PLWD were under-represented in our study due to recruitment difficulties; several could not complete teach-to-goal consent processes. The COVID pandemic disrupted our ability to engage in member checking to validate findings with participants or other PLWD or CP; we did not return transcripts to participants because of the burden of correcting transcripts amid ongoing decline of the PLWD, caregiving challenges, or grieving. Finally, the study setting (in the United States, associated with an ADRC funded by the US National Institutes of Health) means findings may be less transferable to an international audience with different structures for health care systems.
Conclusions
In this comprehensive qualitative interview study of PLWD and CPs receiving care at a specialty dementia clinic, we describe the value of resourcefulness and assistance from family and friends as well as profound challenges and needs for greater support. Integration of geriatric neuropalliative care-informed services into specialty dementia care has the potential to vastly improve quality of life for PLWD and their care partners, and enhance the robust services already provided.
Footnotes
ACKNOWLEDGMENTS
We appreciate the time and expertise of our study participants who contributed data.
Global Brain Health Institute dementia palliative care team members (who participated in team meetings where preliminary analysis was conducted yet did not meet criteria for authorship) included Talita D’Aguiar Rosa, MD, MS; Brenda Perez-Cerpa, MD, Shamiel McFarlane, MD; Maritza Pintado Caipa, MD; Tala Al-Rousan, MD, MPH; Adi Shafir, MD. Nicole Boyd, study coordinator, helped with study administration and participant recruitment.
This study was funded by the Global Brain Health Institute, NIA/NIA K01AG059831, and National Center for Advancing Translational Sciences of the NIH KL2TR001870. Author time was additionally supported by:
Krista Lyn Harrison - National Institute on Aging (K01AG059831), Career Development Award from the National Center for Advancing Translational Sciences of the NIH (KL2TR001870); UCSF Hellman Fellows Award; National Palliative Care Research Center Junior Faculty Award; Atlantic Fellowship of the Global Brain Health Institute.
Sarah B. Garrett - AHRQ T32HS022241.
Alissa Bernstein Sideman - National Institute on Aging (K01AG059840).
Theresa A. Allison - National Institute on Aging (K23AG062613).
Daniel Dohan - National Institute on Aging (1DP1AG069809, 1K07AG066814)
Alexander K. Smith - National Institute on Aging (K24AG068312)
Christine Ritchie - Funded by the John A Hartford Foundation, Centene Foundation, Johns Hopkins University/Humana, Inc.