
Abstract
Background:
Although acupuncture is widely used to improve cognitive and memory in the amnesic mild cognitive impairment (aMCI) patients with impressive effectiveness, its neural mechanism remains largely unclear.
Objective:
We aimed to explore functional magnetic resonance imaging (fMRI) mechanism of acupuncture for aMCI.
Methods:
A randomized, controlled, single-blind research was performed. A total of 46 aMCI patients were randomly assigned into verum and sham acupuncture group, who received a total of 24 times treatments (3 times/week, 8 weeks). Clinical evaluation and fMRI scanning were performed at baseline and after treatment for all aMCI patients. The interaction effects and inter-group effects of regional homogeneity (ReHo) were performed using mixed effect models, and the correlations between clinical improvement and neuroimaging changes before and after verum acupuncture treatment were analyzed using Pearson correlations.
Results:
As a result, interaction effects showed increased ReHo value in left dorsal lateral prefrontal cortex (DLPFC), increased functional connectivity between left DLPFC and left precuneus, and decreased functional connectivity between left DLPFC and left inferior temporal gyrus after verum acupuncture but inversely after sham acupuncture in the aMCI. Condition effects showed increased ReHo in right lingual gyrus, and bilateral post-central gyrus after verum and sham acupuncture in the aMCI. In addition, the changed Montreal Cognitive Assessment scores in verum acupuncture group were significantly correlated with changed ReHo values in left DLPFC.
Conclusion:
Together, our findings further confirmed that acupuncture could be used as a promising complementary therapy for aMCI by modulating function of left DLPFC to improve cognitive symptoms.
Keywords
INTRODUCTION
According to the World Alzheimer Report, around 46.8 million people are nowadays living with dementia, and the number of these patients will be approximate 131.5 million in 2050 [1]. Alzheimer’s disease (AD) is the cause of 60–70% of dementia, affecting 48 million people worldwide [2], leading to serious clinical, social, and economic problems [3]. Mild cognitive impairment (MCI), recognized as the prodromal stage of AD, refers to a transitional period between normal aging and dementia [4]. Among the subtypes of MCI, amnestic MCI (aMCI) carries a substantial risk for progression to AD, with an annual transition rate of 10–15% [5].
However, current medical treatment for aMCI is far from satisfactory [6], there are no approved drugs by the US Food and Drug Administration, European Medicines Agency, or Medicines and Healthcare products Regulatory Agency for preventing, curing or slowing the progression of aMCI to AD [7, 8]. Therefore, it is imperative to develop alternative non-drug strategies for memory recovery and improvement. Previous studies have shown that cognitive behavioral therapy, reminiscence, and acupuncture are considered as common non-drug treatments for MCI [9–11]. However, for patients with aMCI, the availability of cognitive behavioral therapy and recall therapy is limited and unaffordable [12], while acupuncture is frequently used due to its convenience and accessibility.
Acupuncture, as one of the most popular forms of complementary medicine, has been in practice in China for more than 3,000 years and is widely used by many populations for a variety of diseases. Several previous systematic reviews [13–15] indicated that acupuncture could considerably improve cognitive and memory function. However, whether and how acupuncture improve cognitive function and modulate abnormal brain function in aMCI patients remains largely unknown. Although several previous studies [16–18] have been performed to explore mechanism of acupuncture for aMCI using fMRI, there are some major limitations: 1) included patients were not pure aMCI patients; 2) no sham acupuncture group was set as a placebo control; 3) more immediate effect of acupuncture for aMCI were explored; and 4) no significant relationship between fMRI indexes and clinical scales were identified.
In rs-fMRI studies, regional homogeneity (ReHo), a data-driven developed model, is one of the commonly used methods to reveal brain activities. It describes the local connectivity of brain regions and synchronicity or similarity of time series of a given voxel with its immediate neighbors [19] and plays an crucial role in revealing mechanism of diseases. Moreover, it has high robustness to spatial rhythm noise and allow comparisons of subjects without any prior choice of regions of interest, which lay the foundation for revealing efficacy mechanism of acupuncture for aMCI using ReHo method.
Thus, in view of above aspects, overcoming the limitations of previous studies, we aim to reveal the cumulative effect mechanism of acupuncture for aMCI by applying randomized controlled design. Therefore, we hypothesized that 1) after verum acupuncture treatment, aMCI patients exhibited improved neural activity compared to those before treatment; and 2) after acupuncture treatment, changed of cognitive function scale was significantly correlated with improve brain activity in aMCI patients.
MATERIALS AND METHODS
This study was a single-center, single-blinded, placebo controlled, randomized parallel-group longitudinal neuroimaging study. The study was carried out in accordance with the Declaration of Helsinki and approved by Shenzhen Hospital of Traditional Chinese Medicine Evaluation Committee (K2021-012-01). All patients provided written informed consent.
Participants
The aMCI was diagnosed based on the aMCI diagnostic criteria proposed by Petersen in 2004 [20]. The inclusion criteria for subjects were as follows: (a) Han nationality, right-handed, and 50–75 years old; (b) Self-reported memory impairment or insider complaints, and the course of disease > 3 months; (c) Objective impaired memory confirmed by a Mini-Mental State Examination (MMSE) of 24–28 and a Montreal Cognitive Assessment (MoCA) score of 19–26; (d) Clinical Dementia Rating scale (CDR) = 0.5 points; and (e) Not meeting the criteria of dementia in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-R). The patients who showed any one of the following exclusion criteria were excluded: (a) received acupuncture treatment or other cognitive function related treatment in the past one month; (b) unable to complete the neuropsychological scale test, such as severe hearing, aphasia or visual impairment; (c) evidence of brain injury, including severe trauma, stroke, and hydrocephalus; (d) a history of intellectual disability or severe neurological disease; (e) any serious mental illness (clinical diagnosis of major depression, bipolar disorder or schizophrenia); (f) unstable heart, kidney, lung, liver or other serious chronic diseases; (g) systemic diseases that may induce cognitive impairment (such as epilepsy, Parkinson’s disease, severe anemia, anthrax, HIV, alcohol and drug addiction, syphilis or thyroid dysfunction); and (h) MRI examination contraindications. At last, a total of 46 aMCI patients who met the inclusion criteria were enrolled, six of the patients were excluded due to not adhering to the treatment. As a result, 20 aMCI patients were treated with verum acupuncture and 20 were treated with sham acupuncture (Table 1 and Fig. 1).
Participant characteristics by treatment group
SD, standard deviation; MoCA; a represents two sample t tests; b, represents χ2 test; c represents paired t tests; d represents two sample t tests between MoCA scores before treatment; e represents two sample t tests of difference between MoCA scores after treatment.
Brain regions
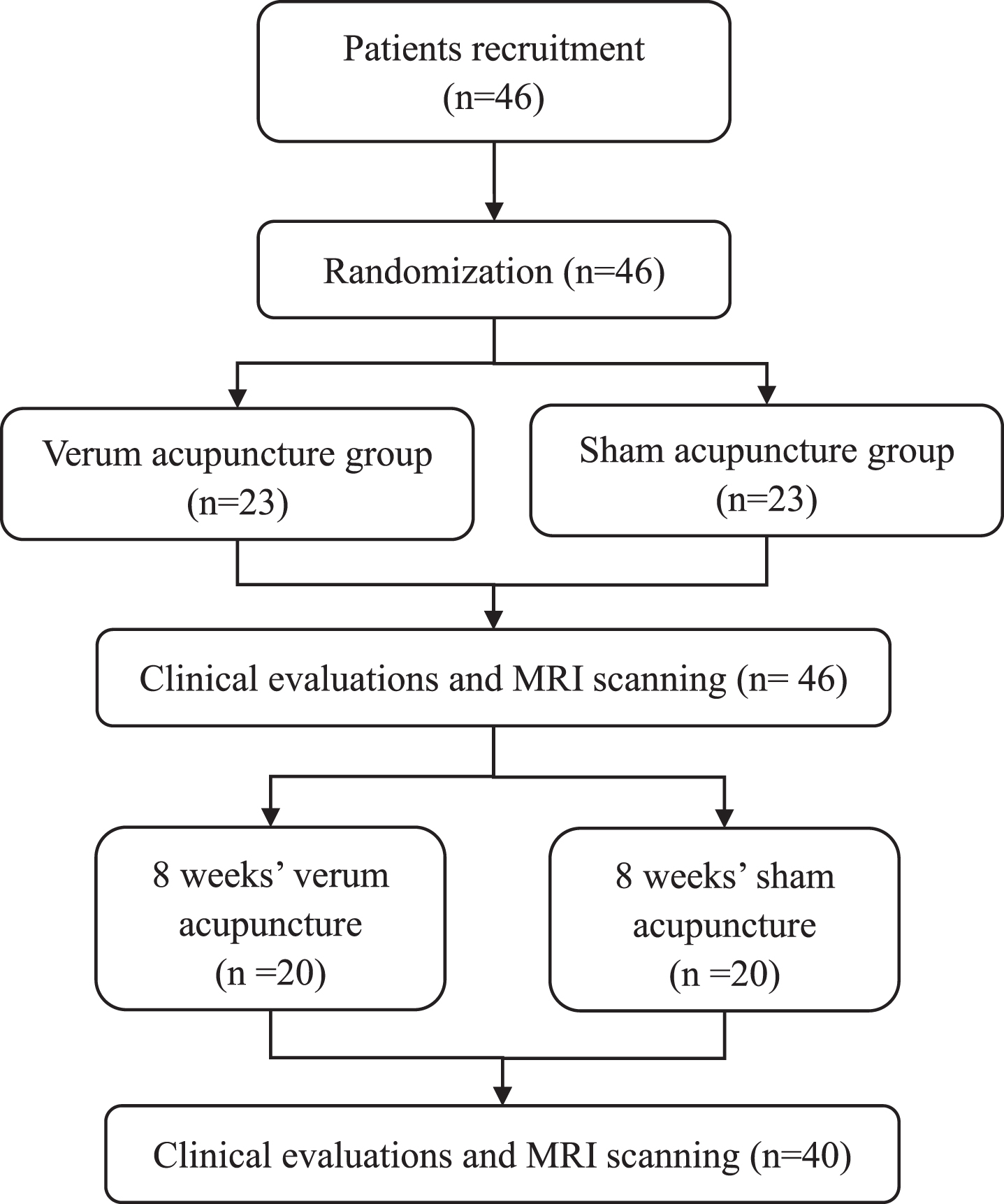
Flowchart of the study design.
Clinical measurements
Demographic and clinical data including age, sex, years of education, nationality, family history, and previous medical history were recorded. All participants received a standardized set of neuropsychological assessments. The MMSE and the Beijing version of the MoCA [21] were used as global measurement of cognitive status, the Chinese Version of Auditory Verbal Learning Test-Huashan (AVLT-H) [22] was used to evaluate episodic memory, the CDR scale was used to evaluate dementia severity [23], the Hamilton Depression Scale was used to evaluate depression severity [24], and the Chinese version of the Lawton and Brody’s Activities of Daily Living Scale (ADL) was used to assess daily functional status of older people living independently at home.
Interventions
All patients received 24 sessions of 30 min verum acupuncture treatments or sham acupuncture treatments over eight weeks (three times a week).
Acupuncturists applied manual acupuncture at 26 obligatory acupoints, included DU20, DU24, RN4, RN6, EX-HN1, EX-HN3, bilateral LI4, HT7, ST36, ST40, GB39, KI3, and LR3, the detailed manipulation procedure is as follows: DU20, EX-HN1, and DU24 were inserted 0.5–0.8 inches horizontally, EX-HN3 was inserted 0.3–0.5 horizontally; RN4, RN6 and ST40 were directly stabbed 1–1.5 inches; HT7 were inserted 0.3–0.5 inches vertically, LI4 was inserted 0.5–1 inches vertically, ST36 was inserted 1–2 inches vertically, GB39, KI3 and LR3 were all inserted 0.5–0.8 inches vertically. Details of location of acupuncture points are shown in Fig. 2. Then acupuncturists tried to elicit acupoints to obtain de-qi sensation (pain, soreness, swelling, heaviness, or numbness) by the manual manipulation of needles including lifting, pulling, twisting, or turning [25]. Over a 30-min period, manual manipulation for each acupoint lasted 10 s and was repeated four times with intervals of 10 min.
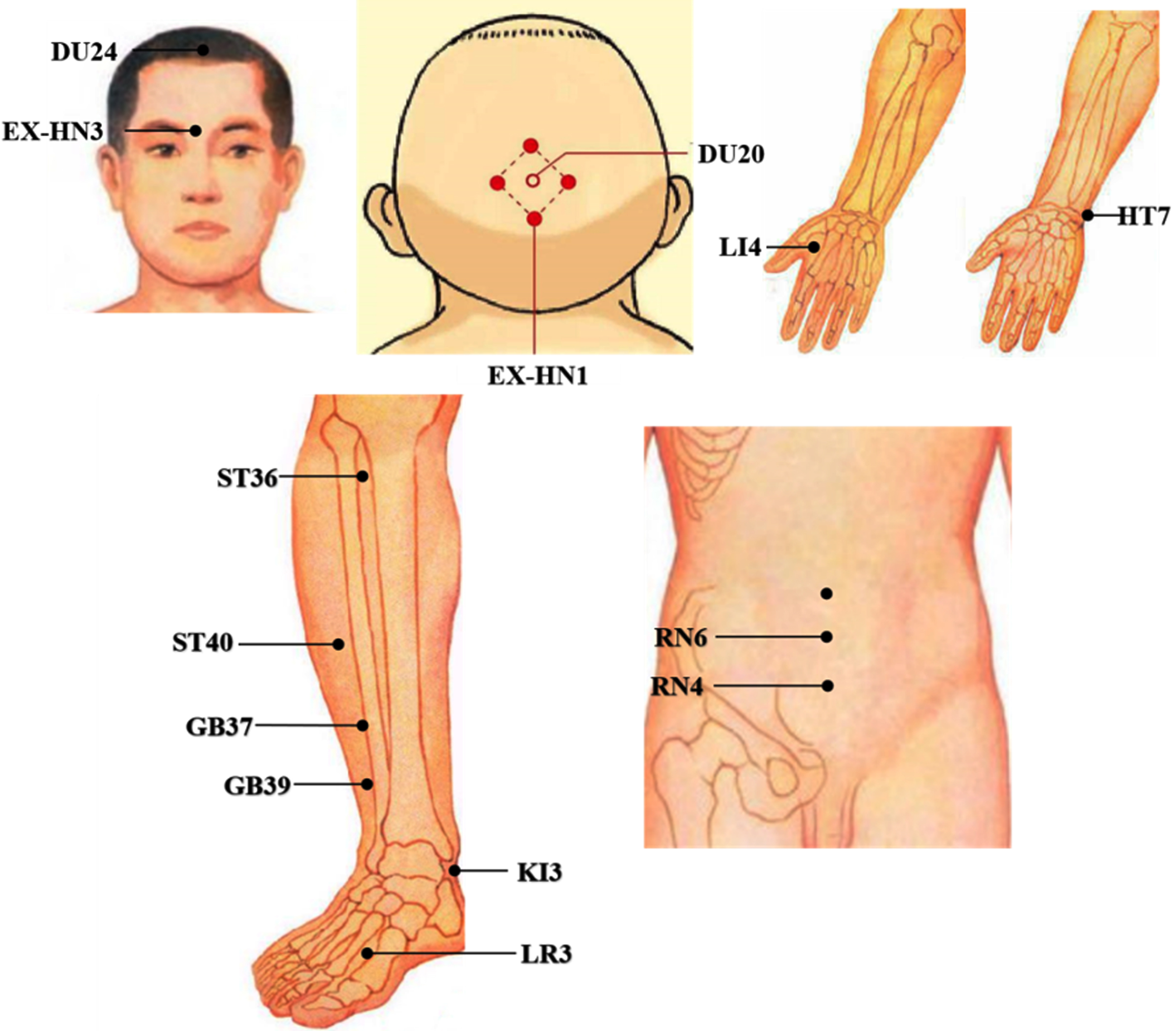
Location of verum acupoints.
Non-meridian non-acupoint shallow acupuncture was manually positioned approximately 1-2 cm over all of the same acupoints used in verum acupuncture. Detailed location of sham acupoints is as follows: The non-acupoint of DU20 is located at 2 cm horizontally outward; the non-acupoint of EX-HN1 is located at 0.3 cm horizontally outward, between the bladder meridian and Du meridian; the non-acupoint of DU24 is located at 0.5 cm horizontally outward, between du meridian and bladder meridian; the non-acupoint of EX-HN3 is located at 0.5 cm of 45°, the midpoint of du meridian and bladder meridian; the non-acupoint of LI4 is located at the level of LI4, the midpoint of the ulnar side of the first metacarpal; the non-acupoint of LR3 is located at the midpoint of the line between liver meridian and stomach meridian, 0.3 cm horizontally outward; the non-acupoints of RN4 and RN6 are located 1 cm on the right of the horizontal side, between the kidney meridian and the stomach meridian; the non-acupoint of ST36 is located at 1–2 cm horizontally outward; the non-acupoint of HT7 is located at 0.5 cm horizontally to the ulnar side; the non-acupoint of ST40 non-acupoint is located 1 cm behind the horizontal; the non-acupoint of KI3 is located 0.5 cm behind the horizontal; the non-acupoint of GB39 is located 1 cm behind the level, between the bladder meridian and gallbladder meridian. Importantly, the needly was inserted shallowly, avoiding deqi, and held for 30 min.
MRI acquisition
Functional imaging data were acquired using a 3.0 Tesla MRI scanner (Siemens MAGNETOM Prisma 3.0 T). Functional images were acquired using an echo-planar imaging sequence, repetition echo time = 2000 ms/30 ms, flip angle = 90°, field of view = 220×220 mm2, matrix = 64×64, slice thickness = 3.2 mm, slice number = 37.
During each scanning session, subjects were instructed to rest with their eyes closed, not to think of anything in particular, and not to fall asleep during scanning.
MRI preprocessing
Images were preprocessed using Data Processing & Analysis of Brain Imaging toolkit (DPABI v6.0, https://www.nitrc.org/projects) and SPM12 (https://www.fl.ion.ucl.ac.uk/spm) software. 1) The first 10 functional images were removed; 2) Subsequent images were corrected by slice timing and realignment, excessive head motion (>2 mm of displacement or > 2° of rotation) were excluded; 3) Then functional images were spatially normalized to Montreal Neurologic Institute (MNI) space, these transformation parameters were then applied to functional images, which were resliced at a resolution of 3×3×3 mm3; 4) Head-motion parameters, the averaged signals from the CSF and white matter, and the global brain signal were regressed; and 5) Temporal band-pass filtering (0.01–0.1 Hz) was performed.
ReHo and FC analysis
The ReHo map was constructed by calculating the Kendall coefficient of the time series consistency between each voxel and its 26 neighboring voxels [19]. The ReHo value of each voxel was subtracted from the average ReHo value of the whole brain and then divided by the standard deviation for subsequent analysis. A Gaussian kernel with a full width and half height of 8 mm was used for smoothing. Finally, a z-transformation was conducted on the individual ReHo maps to generate normally distributed zReHo maps.
The statistical analysis for standardized FC maps of brain regions with statistical differences pre- and post- acupuncture treatment was conducted. Firstly, we extracted the brain areas with statistical differences between pre- and post- acupuncture treatment, which was used as ROI. Then the FC between ROI and the whole brain was analyzed by DPABI. Finally, Fisher’s r-to-z transformation was performed to improve the normality of FC maps for statistical analysis.
In addition, 2×2 mixed design repeated ANOVA with a between-subjects factor of group and a within-subjects factor of treatment was performed using DPABI software to identify the ReHo with the an interaction effect of group×treatment and main effect of group. Gaussian random field (GRF) of a voxel-level p < 0.01 and cluster level p < 0.05 was applied for all analysis. Post hoc paired t-tests were also applied.
Functional characterizations
Functional characterizations were used to determine the function of the brain region about behavioral domains using forward inference in the BrainMap database [26, 27] (http://www.brainmap.org). Behavioral domains include the main categories of cognition, action, perception, emotion, and interception, as well as their related sub-categories. False discovery rate (FDR) was employed to correct for multiple comparisons at p < 0.05.
Clinical data analysis
Clinical data analyses were performed using the SPSS software package version 24.0 (SPSS Inc, Chicago, IL, USA). To investigate the differences in the demographics and clinical characteristics of the patients, pre/post-treatment, the paired sample t-test was used for continuous variables, composition ratio and rate, chi-square test (χ2) or Fisher’s exact test was used for count data. The statistically significant level was set at p < 0.05.
Correlation analysis
Correlation analysis was carried out to calculate association values between the clinical scale scores and ReHo value, while controlling for age, gender, and education. The statistically significant level was set at p < 0.05.
RESULTS
Demographics and clinical measurements
There were no significant differences in age, gender, education, and ADL between verum and sham acupuncture group. Moreover, although both groups showed significant increased MoCA scores and decreased HAMD scores after treatment, there was significant differences in MoCA and no significant differences in HAMD between the two groups before and after treatment.
Results of mixed effect analysis of ReHo
Mixed effect analysis showed interaction effects of ReHo in left dorsal lateral pre-frontal cortex (DLPFC.L). Specially, the ReHo values were significantly increased in verum acupuncture group but significantly decreased in sham acupuncture group (Fig. 3A). Mixed effect analysis showed condition effects of ReHo in left post-central gyrus (PostCG.L), right post-central gyrus (PostCG.R), and right lingual gyrus (LING.R). Specially, the ReHo values were significantly increased in both verum and sham acupuncture group (Fig. 3B).
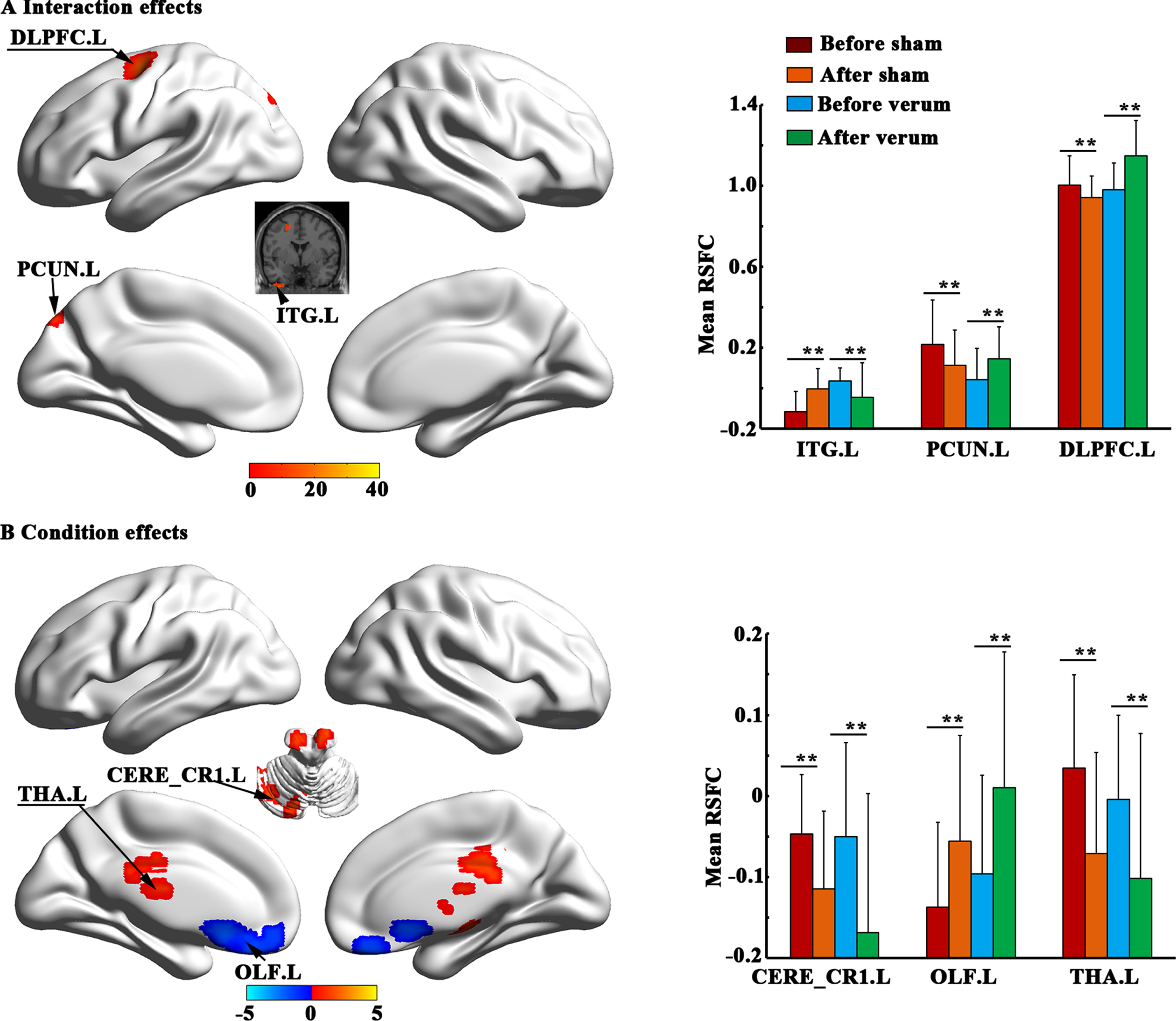
Brain regions showed significant interaction effects and condition effects of regional homogeneity (ReHo). **p < 0.001.
Correlation results
The changed MoCA scores in verum acupuncture group were significantly correlated with changed ReHo values in DLPFC.L (Fig. 4).

Correlation results. A) The MoCA scores were significantly increased in patients with MCI after sham and verum acupuncture. B) The changed MoCA scores in MCI patients after verum acupuncture were significantly correlated with changed REHO in the DLPFC.L. *p < 0.05, **p < 0.001.
Results of mixed effect analysis of RSFC
Interaction effects showed increased RSFC between DLPFC.L and DLPFC.L, increased RSFC between DLPFC.L and left precuneus (PCUN.L) in verum acupuncture group but decreased in sham acupuncture group, whereas decreased RSFC between DLPFC.L and left inferior temporal gyrus (ITG.L) in verum acupuncture group but increased in sham acupuncture group (Fig. 5).
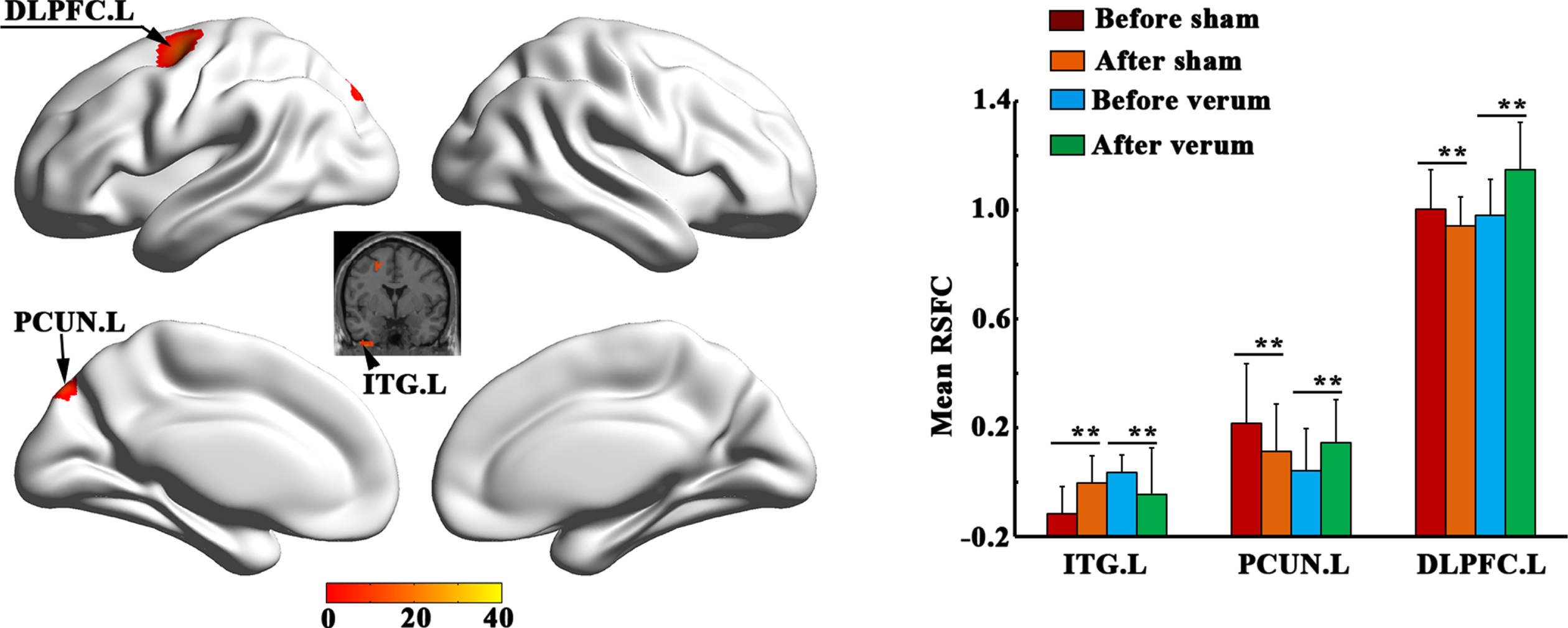
Brain regions showed significant interaction effects resting-state functional connectivity (RSFC) with DLPFC.L. **p < 0.001.
Functional characterizations
DLPFC.L was significantly associated with action (imagination, motor leaning, and execution), perception (vision shape and vision motion), and cognition (soma and space) (Fig. 6).
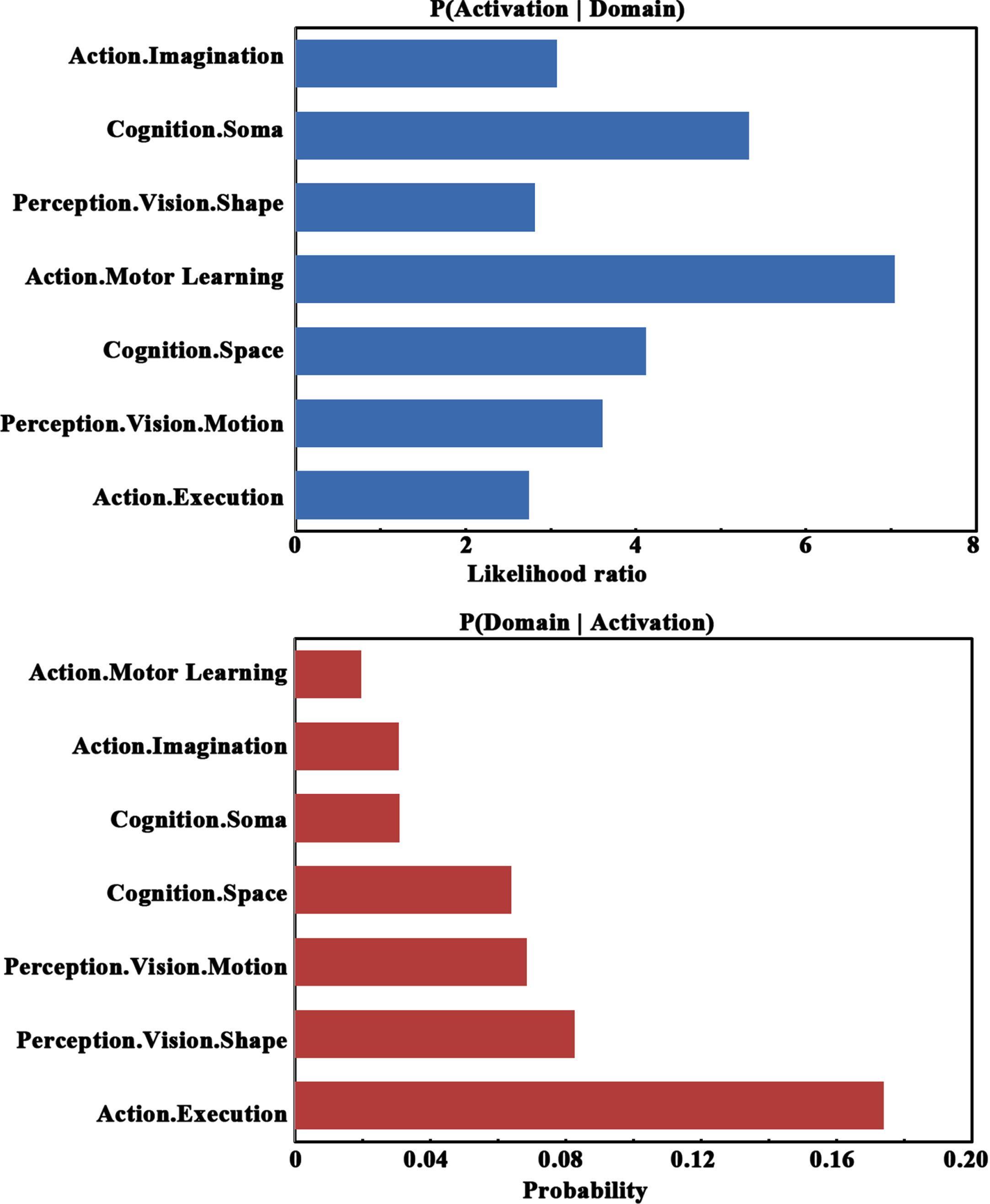
Functional characterization of DLPFC.L.
DISCUSSION
In the present study, we identified that both verum acupuncture and sham acupuncture could significantly improve cognitive function. Further fMRI analyses showed that ReHo value in left DLPFC, FC between left DLPFC and left PCUN were significantly increased in aMCI after verum acupuncture. Moreover, correlation analyses showed that the changed MoCA scores in verum acupuncture group were significantly correlated with changed ReHo values in left DLPFC. Finally, analysis of functional characterizations of left DLPFC further verified that it was associated with action and cognition. Together, these findings demonstrated that acupuncture might be modulate function of left DLPFC to improve cognitive symptoms of aMCI, suggesting that acupuncture could be used as a promising complementary therapy for improving cognitive function of aMCI.
We found that although verum acupuncture and sham acupuncture all could improve cognitive symptoms, verum acupuncture is more effective than sham acupuncture, suggesting that verum acupuncture has specific clinical effect on aMCI.
Based on traditional Chinese medicine theory, the pathogenesis of aMCI is the imbalance of Yin and Yang. Acupuncture plays a vital role in balancing Yin and Yang, regulating the functions of meridians and viscera, therefore improves cognitive function of aMCI. Moreover, according to modern medicine research, acupuncture could stimulate related nerve endings of aMCI, regulate nerve electrophysiological functions of cerebral cortex, improve the energy metabolism level of damaged neurons, and improve cognitive function [28, 29]. Definitely, we also analyzed the reasons in detail about that why sham acupuncture is also effective, which may be explained from the following several aspects: One reason may be that the symptoms of cognitive impairment of included aMCI were relatively mild, resulting in less obvious acupuncture specificity. As Lee et al. [30] found that verum acupuncture and sham acupuncture were found to be effective for mild constipation, but different for refractory constipation. Therefore, the author considered that acupuncture may produce non-specific effects on mild symptoms, while has a specific effect in refractory constipation. The second reason may be the selection of sham acupuncture as control group. In order to successfully blind patients well, the penetrating sham control will produce the piercing sensation and easily lead to the blindness of participants. However, based on Traditional Chinese Medicine theory, acupoints are everywhere in the human body, and shallow insertion is also an effective treatment. Moreover, clinical studies have also found that non-transcutaneous and non-acupoint superficial acupuncture is clinically effective [11, 31]. Thus, we may need to rethink the appropriateness of the sham acupuncture control. The third reason may be that included aMCI patients have a positive attitude towards acupuncture therapy, and such high expectations may over-optimize the response. Studies have found that the expectation effect does affect clinical outcomes and can improve patients’ symptoms [32]. In addition, it may be that the evaluation scale in this study is not sensitive to the effect of acupuncture intervention. Although the Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog) was previously used to evaluate efficacy differences between the AD treatment group and the placebo group [33], its utility in MCI has been shown to be limited. Therefore, it is imperative to develop the sensitivity outcome indicators suitable for MCI intervention. In terms of ADL scale, due to the mild symptoms of the included aMCI, there was no statistically significant difference in ADL. With regard to HAMD scale, it is found that even the mildest depressive symptoms were associated with an increased risk of progression from MCI to dementia [34], thus HAMD scale was used to explore depressive symptoms of aMCI and the efficacy of acupuncture for aMCI in this study. Results showed that although the aMCI patients included did not meet the criteria for depression, acupuncture did significantly improve the symptoms of depression. In addition, the non-obvious depressive symptoms made no significant difference between verum acupuncture and sham acupuncture.
Interaction effect reveals the specificity of acupuncture on aMCI. A finding that supports our hypothesis is that verum acupuncture could activate ReHo of left DLPFC, which is consistent with previous study that showed DLPFC has significant causal interaction with acupuncture for aMCI [16]. As we all know, DLFPC is considered to be the main pathological mechanism of aMCI and AD [35, 36]. Previous systematic review found that aMCI patients showed decreased neural activity in DLPFC of ReHo compared with healthy controls [37, 38]. In addition, Uemura et al. showed that aMCI showed reduced activation in the bilateral DLPFC in the retrieval period than healthy control subjects [39] and abnormal neural activity in DLPFC [40, 41], which indicated that abnormal activity of DLPFC may be an early indicator of aMCI. In terms of function, the DLPFC is considered to be an important part of the executive control network and frontoparietal network. As a modulator of cognitive function, plays an important role in cognitive functions, such as attention, working memory, and executive function [42]. Moreover, the DLPFC has been demonstrated to play a key role in memory formation [43], retrospective short-term memory [44], and space attention/attention selection [45, 46]. Importantly, several studies showed stimulation of DLPFC could enhance encoding of episodic memory or the continuation effect of a stimulus that affects the retrieval process, or both, leading to improved recall [47, 48].
Interaction effects reveal the specificity of acupuncture for aMCI. In this study, results suggested that verum acupuncture could increase ReHo value of left DLPFC, whereas sham acupuncture showed opposite results, which demonstrate that verum acupuncture ameliorates cognitive symptoms by improving DLPFC function and had significant specificity on aMCI. Condition effects reveal non-specificity of acupuncture for aMCI, which refers to the placebo effect of acupuncture for aMCI or comment effect of verum acupuncture and sham acupuncture, results showed that verum acupuncture and sham acupuncture all could increase ReHo in bilateral PostCG, and right LING. The PostCG has been known for its central role in processing sensory information from various parts of the body [49]. The LING is part of occipital lobe and is associated with visual processing [50] and cognitive function [51]. Thus, the activation of brain of PostCG may be relevant to penetration sensation of a needle, while the activation of LING may be related to improvement of cognition.
Moreover, we found that verum acupuncture could increase FC between left DLPFC and left DLPFC, between left DLPFC and left PCUN significantly, and decrease FC between left DLPFC and left ITG. ITG plays an important role in visual processing and spatial working memory [52], its activities may protect the memory function of MCI patients [53]. PCUN is the central node of the default mode network and the key node of the parietal memory network, which plays a crucial role in visual spatial integration and memory encoding and retrieval tasks [54–56]. Interaction effect suggested that increasing FC between DLPFC and PCUN was found in verum acupuncture for aMCI, which indicated that acupuncture could enhance connectivity in brain areas associated with cognition and memory. Decreasing FC between DLPFC and ITG suggested that verum acupuncture could reduce the compensatory function between them. This revealed that acupuncture can normalize abnormal functions.
Another encouraging finding is that the changed MoCA scores in MCI patients after verum acupuncture were significantly correlated with changed ReHo in the left DLPFC. Previous studies found that DLPFC with stimulation of repetitive transcranial magnetic stimulation could improve MoCA values in AD patients [57], picture naming [58], and working memory [59]. Moreover, excitability of DLPFC in AD was associated with global cognition and executive function [60]. Above findings that stimulation of DLPFC could improve MoCA and cognition function are consistent with the results of this study. In addition, this result also demonstrated that DLPFC could be used as a biomarker of acupuncture efficacy.
Finally, it should be noted that function characterizes of left DLPFC was significantly associated with action, perception, and cognition, which is line with previous studies [61–63]. It is well known that that there was a close correlation of MCI with visual and emotional perception [64], executive function [62] and cognition [65], which, even if mild, can impact some aspects of a patient’s ability to deal with everyday life. Function characterizes of left DLPFC further verified the neural mechanism of acupuncture on the improvement of cognitive symptoms ofaMCI.
Limitations to our study should also be noted. First, small sample size and single center collection reduce the reliability of results; In addition, due to time constraints, the follow-up was not completed. Therefore, further multi-center, large-sample longitudinal data collection is necessary for further verify the findings. Second, the selection of sham acupuncture as a placebo control may be not appropriate. In the future, patients’ disease and severity of their condition, as well as their expectation of acupuncture, should be considered to further adjust the placebo control method. Third, the selection of clinical scale may not be comprehensive enough, further detailed assessment can better reflect the clinical manifestations and efficacy mechanisms of aMCI patients from different aspects.
Conclusion
In summary, this study supports the hypotheses that acupuncture could increase ReHo of DLPFC and modulate FC between left DLPFC and left ITG, between left DLPFC and left PCUN, which is associated with improvement in cognitive function. Taken together, these findings not only provide a visual theoretical basis for the clinical efficacy of acupuncture for aMCI, but also provide new ideas for the treatment of aMCI. Larger samples, multicenter clinical research with acupuncture for aMCI are necessary and forthcoming. Future efforts will consider focusing on biomarkers of aMCI in acupuncture therapy using large data for individualized treatment.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all participants who contributed samples to this study.
This work was supported by Shenzhen Science and Technology Research Program (No. JCYJ20200109114816594 and No. JCYJ20180507182441903), National Key R&D Program of China (2017YFC1703600), Study on the effect mechanism of acupunc-ture-moxibustion in dominant diseases (2017YFC1703606), the National Natural Science Foundation of China (62006220), Shenzhen’s Sanming Project (SZSM201612001), Special Innovation Project of the Guangdong Provincial Department of Education (2021WQNCX068) and the Special Innovation Project of the Guangdong Provincial Department of Education (2021WQNCX068).