
Abstract
Background:
Previous studies have reported inconsistent associations between chronic kidney disease (CKD) and dementia.
Objective:
To evaluate whether CKD is a risk factor for dementia and compare the performance of different measures of calculating estimated glomerular filtration rate (eGFR).
Methods:
275,167 participants from UK Biobank were included and eGFR at baseline was calculated using serum creatinine (eGFRcr), cystatin C (eGFRcys), and creatinine-cystatin C equations (eGFRcr-cys). Restricted cubic splines and Cox regression models were performed to assess the relationship of eGFR with all-cause dementia, Alzheimer’s disease (AD), and vascular dementia (VaD).
Results:
We observed a U-shaped relationship between each eGFR and risk of all-cause dementia and VaD, with eGFRcys and eGFRcr-cys showing a closer linkage (peGFRcys <0.0001, peGFRcrhboxcys<0.0001 and peGFRcr = 0.0001). Lower and supranormal eGFR were related to increased risk of all-cause dementia. Compared to the reference category of 90–104 ml/min/1.73 m2, adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) of all-cause dementia for eGFRcr-cys 30–59, <30, and ≥105 ml/min/1.73 m2 were 1.26 (95% CI [1.05–1.50], p = 0.012), 2.62 (95% CI [1.54–4.47], p < 0.001), and 1.41 (95% CI [1.17–1.70], p < 0.001). No statistically significant association was observed between eGFR with risk of AD.
Conclusion:
This prospective study identified impaired kidney function as a critical risk factor for dementia and noted the application of cystatin C strengthened the relationship between CKD and dementia, underlining the significant value of preserving kidney function to reduce the risk of dementia and considering cystatin C measurement as part of clinical practice.
INTRODUCTION
Dementia, primarily characterized by a progressive decline in cognition and function [1], occurs predominantly in people older than 65 years [2]. Individuals with dementia tend to have disorders on memory, emotion, and behavior [3], and require health and social care as dementia progresses, leading to a considerable burden for families and social economy [2]. Alzheimer’s disease (AD) is the most common type of dementia, followed by vascular dementia (VaD) [2]. Over 50 million people worldwide were living with dementia in 2019 and the figure is expected to rise to 152 million by 2050 [3]. Given the limited value of available drug treatments [4], identifying potential modifiable risk factors of dementia is of extreme importance.
Chronic kidney disease (CKD), defined as structural or functional abnormalities of kidney persisting for at least 3 months [5], is a common disorder among human beings and poses a major public health issue [6], with a prevalence of 9.1% globally [7]. Estimated glomerular filtration rate (eGFR) and urinary albumin-creatinine ratio (uACR) are commonly used to assess renal function, with diagnostic thresholds of less than 60 ml/min/1.73 m2 for eGFR and 30 mg/g for uACR [5]. Previous studies have found that CKD is linked to increased risk of cardiovascular diseases [8, 9], anemia [10], and other noncommunicable diseases [8]. There is increasing evidence of a close linkage between impaired renal function and dementia [11–14]. However, previous studies have conflicting results [15–18] and limitations. Most cohorts investigated the relationship between reduced eGFR with risk of dementia, but that of supranormal eGFR with dementia remains unclear [11–18]. Previous studies used a single measure for eGFR, predominantly based on creatinine equation [11, 14–18]. Compared with serum creatinine used routinely in clinical conditions [7], cystatin C combined with creatinine improves accuracy for estimating GFR [19]. The use of cystatin C strengthens the association between eGFR with cardiovascular disease and mortality [20, 21]. However, this has not been well investigated in dementia.
This prospective study aims to explore associations between eGFR and dementia in 275,167 individuals from UK biobank, using serum creatinine (eGFRcr), cystatin C (eGFRcys), and creatinine-cystatin C equations (eGFRcr-cys) to assess kidney function.
MATERIALS AND METHODS
Study population
UK Biobank is a large-scale longitudinal cohort that recruited more than 500,000 participants (aged 37 to 73 years) from 22 assessment centers across England (89%), Scotland (7%), and Wales (4%) between 2006 and 2010. Informed consent confirmed by electronic signature was provided by all participants at baseline. The participants undertook physical measures, provided information on their health and lifestyle and donated blood, urine, and saliva samples for analysis and agreed to have long-term follow-up. UK Biobank has ethical approval from the North West Multi-centre Research Ethics Committee (11/NW/03820).
468,928 participants with complete information on serum creatinine and cystatin C at baseline were included in this study. Exclusion criteria were previous diagnosis of dementia (n = 823), missing covariates information (n = 128,510), previous history of renal replacement therapy including renal transplant, hemodialysis or peritoneal dialysis (n = 394) and lost to follow-up (n = 64,034). Data from 275,167 participants were included in the main analysis (Fig. 1). The present analyses were conducted under UK Biobank application number 19542.
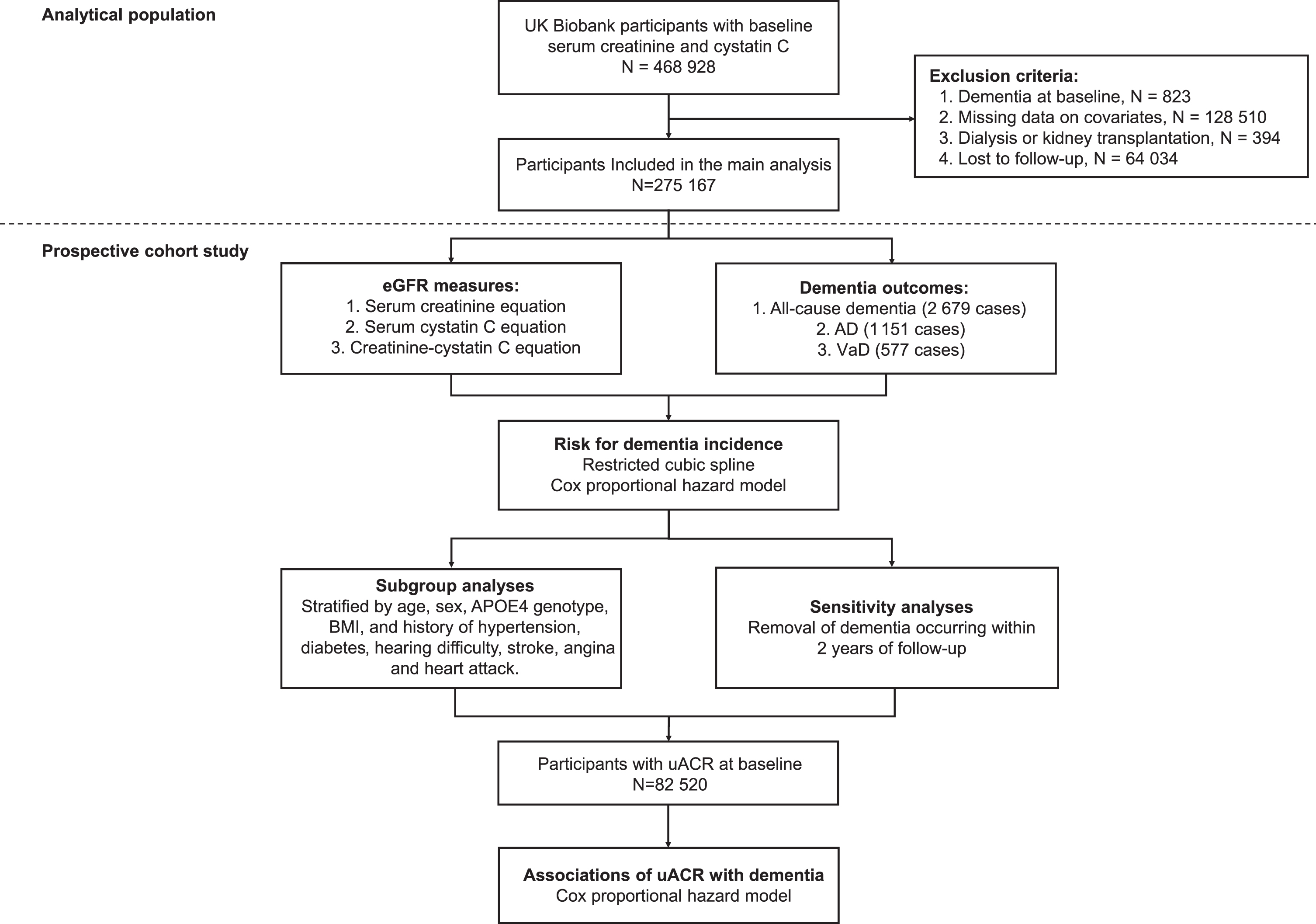
Analytical pipeline of the study. eGFR, estimated glomerular filtration rate; uACR, urinary albumin-creatinine ratio; AD, Alzheimer’s disease; VaD, vascular dementia; BMI, body mass index.
Exposures
Blood samples were collected at baseline and processed at UK Biobank’s central laboratory. Serum creatinine and cystatin C were measured using enzymatic analysis and latex enhanced immune-turbidimetric method, respectively. Full details of biochemistry assay quality procedures and assay performance have been described previously [22, 23].
eGFR at baseline was calculated based on serum creatinine, cystatin C or creatinine-cystatin C equations of Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI): eGFRcr = 141×min(Scr/κ, 1) α×max(Scr/κ, 1)–1.209×0.993Age [×1.018 if female] [×1.159 if black] (Scr: serum creatinine, mg/dl; κ: 0.7 for females and 0.9 for males; α: –0.329 for females and –0.411 for males; min: the minimum of Scr/κ or 1; max: the maximum of Scr/κ or 1), eGFRcys = 133×min(Scys/0.8, 1)–0.499×max(Scys/0.8, 1)–1.328×0.996Age [×0.932 if female] (Scys: serum cystatin C, mg/l; min: the minimum of Scys/0.8 or 1; max: the maximum of Scys/0.8 or 1), eGFRcr-cys = 135×min(Scr/κ, 1) α ×max(Scr/κ, 1)–0.601×min(Scys/0.8, 1)–0.375×max(Scys/0.8, 1)–0.711×0.995Age [×0.969 if female] [×1.08 if black] (Scr: serum creatinine, mg/dl; Scys: serum cystatin C, mg/l; κ: 0.7 for females and 0.9 for males; α: –0.248 for females and –0.207 for males; min: the minimum of Scr/κ or 1; max: the maximum of Scr/κ or 1) [19]. Each eGFR was categorized into 5 groups according to CKD staging of Kidney Disease: Improving Global Outcomes (KDIGO):≥105, 90–104, 60–89 (G2), 30–59 (G3), <30 ml/min/1.73 m2 (G4 and G5) [5]. Given small numbers with eGFR <15 ml/min/1.73 m2 (G5) in our cohort, participants with eGFR <30 ml/min/1.73 m2 were combined into one group.
Outcomes
Outcomes were ascertained through algorithmic combinations of coded information from hospital admissions and death registries, using ICD 9 and ICD 10 codes (Supplementary Table 1) [24]. The primary outcomes were incident all-cause dementia. The secondary study outcomes were incident AD and VaD.
Covariates
The following covariates were selected at baseline, including: age, sex (female or male), ethnicity (White or others), APOE4 genotype (ɛ4 carrier or non-carrier), education level (high or low, high included (1) college or university degree, and (2) other professional qualifications; low included (1) Advanced (A) levels/Advanced Subsidiary (AS) levels or equivalent, (2) Ordinary (O) levels/General Certificate of Secondary Education (GCSE) or equivalent, (3) Certificate of Secondary Education (CSE) or equivalent, and (4) National Vocational Qualification (NVQ) or Higher National Diploma (HND) or Higher National Certificate (HNC) or equivalent), Townsend deprivation index, body mass index (BMI: <25, 25–29.9, and ≥30 kg/m2), smoking status (never, previous, and current), alcohol status (never, previous, and current), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and history of hypertension, diabetes mellitus, hearing difficulty, stroke, angina and heart attack [25].
Statistical analysis
Continuous variables of baseline characteristics were displayed as mean and standard deviation (SD). Categorical variables were displayed as percentages. Baseline characteristics across eGFR categories were compared using ANOVA tests for continuous variables and chi-squared tests for categorical variables. Kaplan-Meier curves were used to plot cumulative incidence rate of all-cause dementia, VaD, and AD for each GFR category, and the difference was tested using log-rank test. We calculated person-years (py) from the date of baseline assessment to the date of dementia diagnosis, death, loss to follow-up, or the end of this study (April 2021).
Cox regression models were performed to evaluate the associations of each eGFR categories with incident all-cause dementia, AD, and VaD. In model 1, we adjusted for age, sex, ethnicity, APOE4 genotype, and education level. In model 2, we further adjusted for Townsend deprivation index, BMI, smoking status, alcohol status, TC, HDL-C, LDL-C, and history of hypertension, diabetes mellitus, hearing difficulty, stroke, angina, and heart attack. Restricted cubic splines based on model 2 were used to visualize the relationships between levels of each eGFR and dementia on a continuous scale, with 5 knots at the 30, 45, 60, 90, and 105 ml/min/1.73 m2.
Several additional analyses were conducted to check the results. First, stratified subgroup analyses were conducted by age (<65, ≥65 years old), sex (female, male), APOE4 genotype (ɛ4 carrier or non-carrier), BMI (<25, 25–29.9, ≥30 kg/m2), history of hypertension (yes or no), history of diabetes mellitus (yes or no), history of hearing difficulty (yes or no), history of stroke (yes or no), history of angina (yes or no), and history of heart attack (yes or no). Second, to reduce the possibility of reverse causality and detection bias, we performed sensitivity analyses excluding dementia cases occurring within the first 2 years of follow-up. Third, eGFR 30–59 ml/min/1.73 m2 (G3) was divided into 45–59 (G3a) and 30–44 ml/min/1.73 m2 (G3b) to investigate a more refined relationship between different degrees of kidney dysfunction with dementia and whether the association between G3a and dementia risk would be significantly different depending on different measurements (eGFRcr, eGFRcys and eGFRcr-cys). Fourth, to explore the relationship between eGFR and albuminuria and risk of dementia, Cox regression models were further adjusted for uACR, which was categorized into three groups aligned with the KDIGO guideline for CKD: <30 (A1), 30–300 (A2), >300 mg/g (A3) [5]. Fifth, logistic regression models were performed additionally. Finally, depression, schizophrenia, and bipolar disorder were further adjusted in Cox models of 275,097 individuals with complete information on these mental diseases.
All analyses were conducted using R software version 4.1.3 and p < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
Among 275,167 participants in the study cohort, 53.45% were women and the mean baseline age was 56.07 (SD 8.03) years. Baseline characteristics across five categories of three eGFR groups (eGFRcr, eGFRcys, eGFRcr-cys) are shown respectively (Table 1, Supplementary Tables 2 and 3). In eGFRcr-cys groups, 40,913 (14.9%) participants had eGFR ≥105 ml/min/1.73 m2, 109,372 (39.7%) participants had eGFR 90–104 ml/min/1.73 m2, 119,201 (43.3%) participants had eGFR 60–89 ml/min/1.73 m2, 5,420 (2.0%) participants had eGFR 30–59 ml/min/1.73 m2, and 261 (0.1%) participants had eGFR <30 ml/min/1.73 m2. Participants with lower levels of eGFR tended to be older, male, less educated, higher BMI, lower HDL-C, and to have a history of hypertension, diabetes, stroke, angina, heart attack, and hearing difficulty.
Baseline characteristics of 275,167 patients by eGFRcr-cys categories
eGFR, estimated glomerular filtration rate; BMI, body mass index; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; uACR, urinary albumin-creatinine ratio; SD, standard deviation.
Only 82,520 (29.99%) participants had information on uACR at baseline. The proportion of uACR >300 mg/g increased with reduced eGFR by all measures.
Incident dementia
During a median follow-up of 8.97 years (Q1-Q3 7.00–10.52 years), 2,679 participants developed dementia, including 1,151 cases with incident AD and 577 cases with incident VaD. The overall incidence rate of all-cause dementia was 1.13 per 1,000 person-years (py). Incidence rates per 1,000 py were higher with decreased eGFR: 6.54 in eGFRcr-cys <30 ml/min/1.73 m2, 3.36 in eGFRcr-cys 30–59 ml/min/1.73 m2, 1.52 in eGFRcr-cys 60–89 ml/min/1.73 m2, 0.84 in eGFRcr-cys 90–104 ml/min/1.73 m2, and 0.41 in eGFRcr-cys ≥105 ml/min/1.73 m2. Same trend was noted in AD and VaD, excluding eGFR <30 ml/min/1.73 m2 for AD (Supplementary Table 4). Kaplan-Meier curves indicated decreased eGFR categories with higher cumulative incidence rate of all-cause dementia (Logrank test p < 0.0001), VaD (Logrank test p < 0.0001), and AD (Log-rank test p < 0.0001) for 3 measurements (Fig. 2).
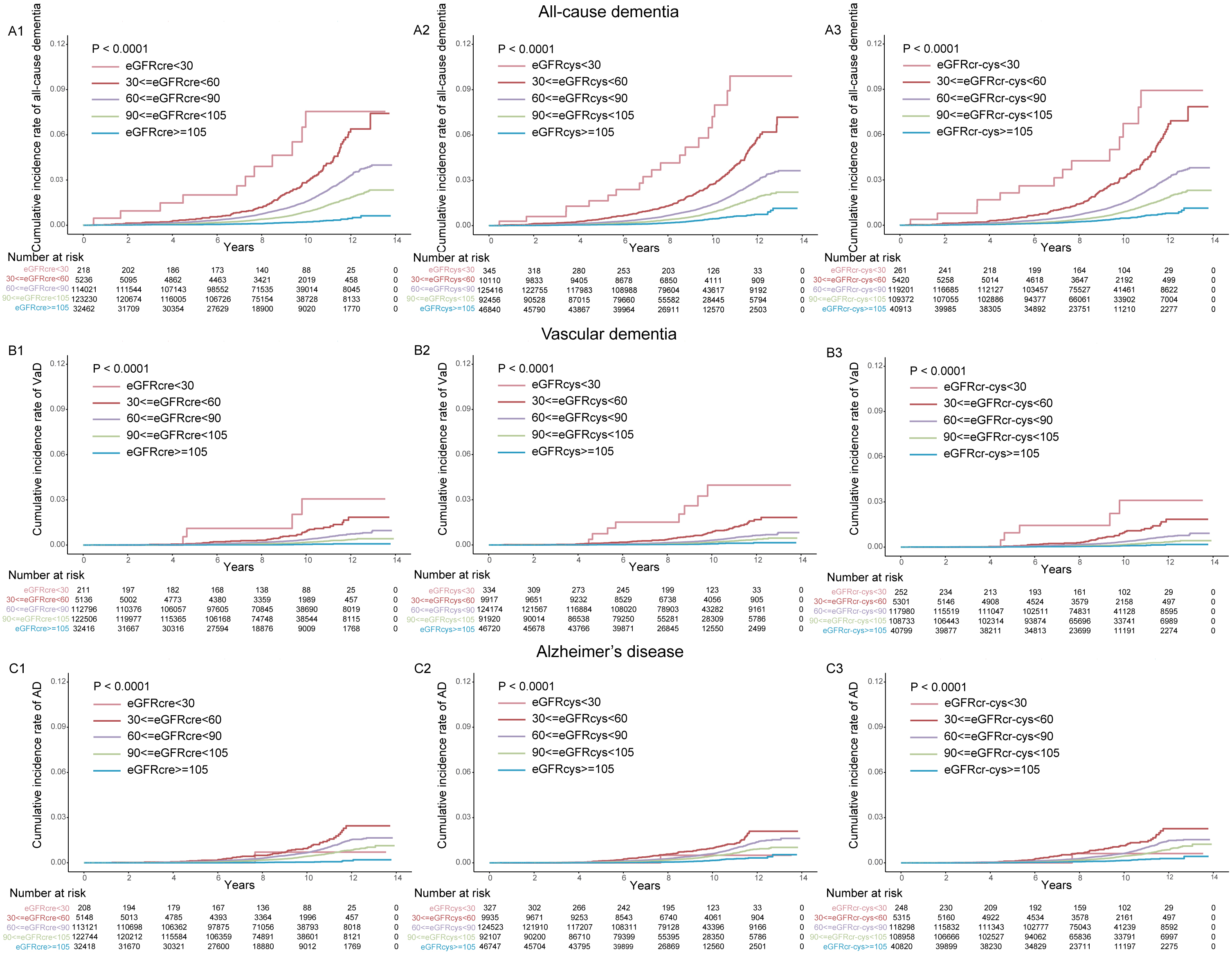
Kaplan-Meier curves of dementia for each eGFR category. (A1) eGFRcr and all-cause dementia. (A2) eGFRcys and all-cause dementia. (A3) eGFRcr-cys and all-cause dementia. (B1) eGFRcr and vascular dementia. (B2) eGFRcys and vascular dementia. (B3) eGFRcr-cys and vascular dementia. (C1) eGFRcr and Alzheimer’s disease. (C2) eGFRcys and Alzheimer’s disease. (C3) eGFRcr-cys and Alzheimer’s disease. p was for Log-rank test. eGFR, estimated glomerular filtration rate; VaD, vascular dementia; AD, Alzheimer’s disease.
Association between eGFR and risk of dementia
Restricted cubic spline models demonstrated a strong U-shaped association between each eGFR measure and risk of all-cause dementia and VaD (Fig. 3). The risk of all-cause dementia reached the nadir at eGFRcr of 74 ml/min/1.73 m2, eGFRcys of 84 ml/min/1.73 m2, and eGFRcr-cys of 85 ml/min/1.73 m2, respectively. Adjusted hazard ratios (HR) and 95% confidence intervals (CI) between eGFR and all-cause dementia and VaD below or above the reference eGFR point of 90 ml/min/1.73 m2 and change points were shown from piecewise two-line models (Supplementary Tables 5 and 6). No significant relationship was observed between eGFR and AD.
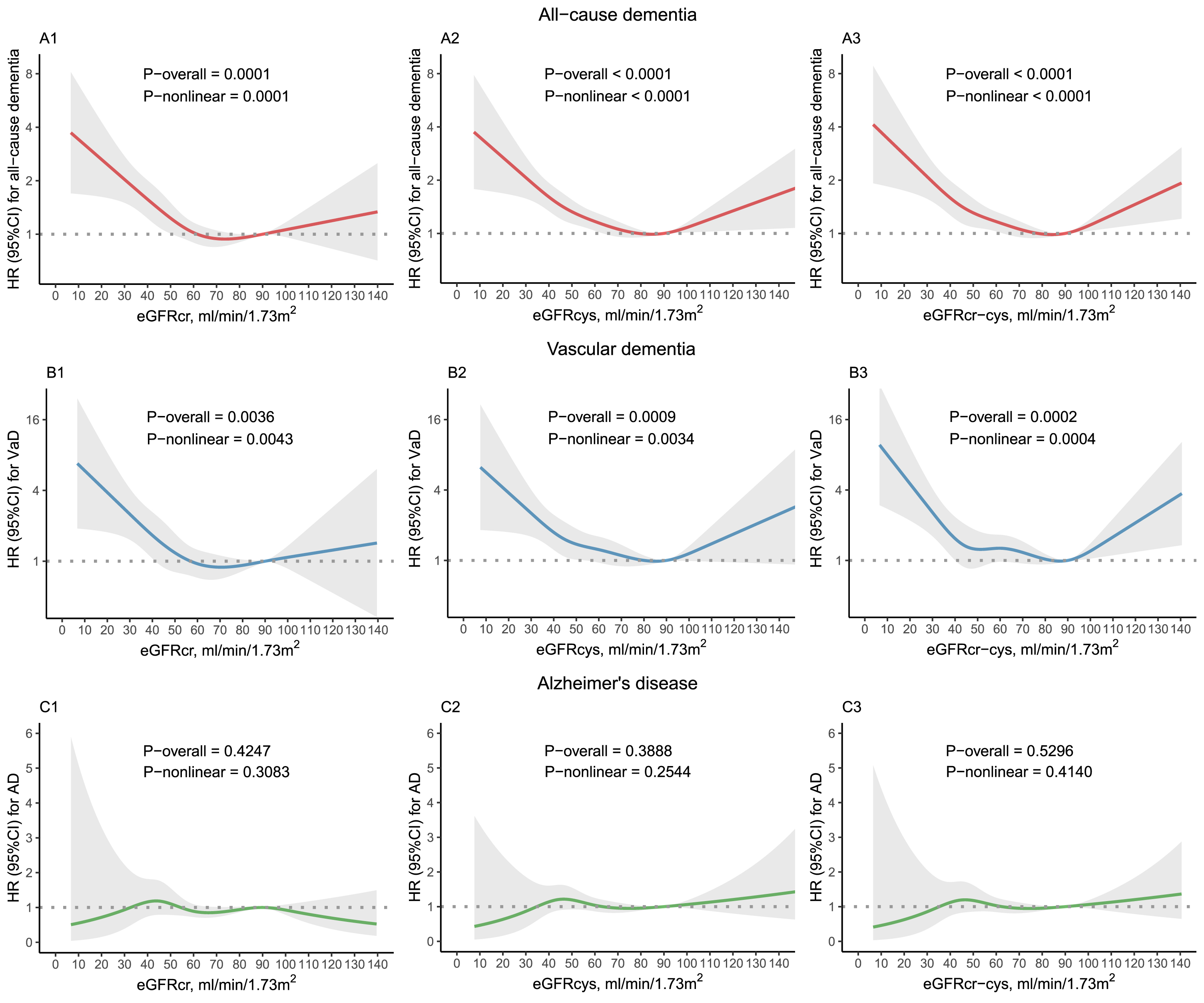
Restricted cubic spline models for the relationship between each eGFR with dementia. (A1) eGFRcr and all-cause dementia. (A2) eGFRcys and all-cause dementia. (A3) eGFRcr-cys and all-cause dementia. (B1) eGFRcr and vascular dementia. (B2) eGFRcys and vascular dementia. (B3) eGFRcr-cys and vascular dementia. (C1) eGFRcr and Alzheimer’s disease. (C2) eGFRcys and Alzheimer’s disease. (C3) eGFRcr-cys and Alzheimer’s disease. HR was adjusted for age, sex, ethnicity, APOE4 genotype, education level, Townsend deprivation index, BMI, smoking status, alcohol status, TC, LDL-C, HDL-C, hypertension, diabetes mellitus, hearing difficulty, stroke, angina, and heart attack. eGFR, estimated glomerular filtration rate; AD, Alzheimer’s disease; VaD, vascular dementia; BMI, body mass index; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; HR, hazard ratio; CI, confidence interval.
In Cox proportional hazard model adjusted for age, sex, ethnicity, APOE4 genotype, and education level (model 1), there was an increased risk of all-cause dementia with lower eGFR levels (Table 2). Compared to reference category of eGFR 90–104 ml/min/1.73 m2, HRs for eGFRcr measure of 60–89, 30–59,<30, and ≥105 ml/min/1.73 m2 were 0.95 (95% CI [0.87–1.04], p = 0.276), 1.30 (95% CI [1.08–1.56], p = 0.005), 2.78 (95% CI [1.53–5.05], p < 0.001), and 1.34 (95% CI [1.01–1.77], p = 0.043), and the HRs were greater when measures of eGFRcys and eGFRcr-cys were used to assess the relationship between eGFR and dementia. After further adjusted for Townsend deprivation index, BMI, smoking status, alcohol status, total cholesterol, HDL, LDL, history of hypertension, diabetes mellitus, hearing difficulty, stroke, angina and heart attack (model 2), the associations were attenuated but a U-shaped relationship between eGFRcr-cys with all-cause dementia remained significantly (Table 2). Compared to the reference category of 90–104 ml/min/1.73 m2, HRs for eGFRcr-cys of 60–89, 30–59,<30, and ≥105 ml/min/1.73 m2 were 0.98 (95% CI [0.90–1.08], p = 0.738), 1.26 (95% CI [1.05–1.50], p = 0.012), 2.62 (95% CI [1.54–4.47], p < 0.001), and 1.41 (95% CI [1.17–1.70], p < 0.001).
Associations of eGFR categories with all-cause dementia outcome, for 3 measures: eGFRcr, eGFRcys, and eGFRcr-cys
Model 1: adjusted for age, sex, ethnicity (White or others), APOE4 genotype (ɛ4 carrier or non-carrier), and education level (high or low). Model 2: model 1 + BMI (<25, 25–29.9, and ≥35 kg/m2), Townsend deprivation index, smoking status (never, previous, and current), alcohol status (never, previous, and current), TC, HDL-C, LDL-C, and Comorbid conditions (hypertension, diabetes, stroke, angina, heart attack and hearing difficulty). HR, hazard ratio; CI, confidence interval; eGFR, estimated glomerular filtration rate; BMI, body mass index; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
GFR <30 ml/min/1.73 m2 was related to higher risk of incident VaD (Supplementary Table 7). Compared to the reference category, HRs for eGFR of <30 ml/min/1.73 m2 were 3.02 (95% CI [1.11–8.21], p = 0.030), 4.00 (95% CI [1.94–8.28], p < 0.001), and 3.35 (95% CI [1.36–8.24], p = 0.008) for eGFRcr, eGFRcys, and eGFRcr-cys, respectively. No statistically significant association was observed between each eGFR measure with risk of incident AD (Supplementary Table 7).
Subgroup and sensitivity analysis
When subgroup analyses were performed by stratifying age, sex, APOE4 genotype, BMI, hypertension, diabetes mellitus, hearing difficulty, stroke, angina, and heart attack, the associations between eGFR and the risk of dementia showed no substantial difference, although some of the results were not statistically significant, probably caused by small number of participants in some categories after stratification (Supplementary Table 8). In the sensitivity analyses excluding cases during the first 2 years of follow-up, the results were consistent with those of initial analyses (Supplementary Table 9). When eGFR 30–59 ml/min/1.73 m2 was divided into two groups (30–44 and 45–59 ml/min/1.73 m2), the linkage between eGFR 45–59 ml/min/1.73 m2 and risk of all-cause dementia reached borderline significance for eGFRcys (p = 0.069) and eGFRcr-cys (p = 0.066), while not for eGFRcr (p = 0.321) (Supplementary Table 10). Further, Cox proportional hazard model was conducted for uACR categories (Supplementary Tables 11–13). Compared to participants with uACR of <30 mg/g, those with uACR of >300 mg/g had an increased risk of all-cause dementia. In logistic regression models, odds ratios (ORs) for eGFRcr-cys of 60–89, 30–59,<30, and ≥105 ml/min/1.73 m2 were 0.99 (95% CI [0.90–1.08], p = 0.750), 1.24 (95% CI [1.03–1.48], p = 0.023), 2.17 (95% CI [1.17–3.71], p = 0.008), and 1.43 (95% CI [1.18–1.71], p < 0.001) (Supplementary Table 14), compared to the reference category. Finally, the results of Cox models further adjusted for depression, schizophrenia, and bipolar disorder were consistent with the main analyses (Supplementary Tables 16 and 17).
DISCUSSION
In this study, we investigated associations between eGFR of full spectrum and incident dementia and compared the relationship of different measures for calculating eGFR with dementia in the same cohort. Our results demonstrated that CKD increased the risk of all-cause dementia. We observed a strong U-shaped association between each eGFR with all-cause dementia and VaD. eGFRcr and eGFRcr-cys were more closely related to dementia than eGFRcr, which is used routinely in recent clinical conditions. We also indicated that supranormal eGFR was linked to a higher risk of dementia, particularly when using eGFRcr-cys.
Previous studies reported inconsistent results on the relationship between eGFR and incident dementia [11–18]. The IQVIA Medical Research Data-The Health Improvement Network (IMRD-THIN) retrospective cohort, including 2,797,384 participants in the eGFR cohort and 641,912 participants in the ACR cohort, showed that decreased eGFR and increased albuminuria had graded associations with dementia among patients aged ≥50 years, while CKD G5 was not significantly related to incident dementia [11]. Although we did not group eGFR strictly by CKD staging as in the IMRD-THIN study, we observed a similar pattern in all-cause dementia, and in addition, important confounders such as education level and APOE4 genotype were adjusted in our models, which facilitated a more accurate evaluation of the relationship between renal function and dementia without overestimation. Likewise, the Stockholm Creatinine Measurements (SCREAM) register-based cohort, which included 329,822 participants aged ≥65 years, reported that reduced renal function and steeper kidney function decline were consistently associated with incident dementia, particularly in VaD, and the population attributable fraction (PAF) of CKD was 10% [12]. While the SREAM study used the traditional creatinine formula to estimate CKD, we calculated eGFR based on 3 CKD-EPI equations and the performance of different eGFR measures suggested that the application of cystatin C strengthened the linkage between CKD and incident dementia. Our findings reinforced the important role of eGFR as a risk factor for dementia, consistent with aforementioned studies.
However, some studies had converse conclusions [15–18]. The Systolic Blood Pressure Intervention Trial (SPRINT) study, including 8,563 adults with hypertensive, indicated that baseline eGFR <60 ml/min/1.73 m2 and uACR ≥30 mg/g were not associated with dementia or MCI, while eGFR decline ≥30% was associated with a higher risk for probable dementia [16]. Similarly, the Three-City (3C) study, involved 7,839 individuals aged >65 years, reported no relationship between risk of dementia and lower eGFR, but faster eGFR decline was related to incident dementia and cognitive decline [17]. The discrepancy between these studies and our findings was probably due to the inadequate sample sizes in these studies, which may weaken the validity of detecting a significant association between impaired renal function and dementia, as well as differences in eGFR measures and outcomes ascertainment.
Our study demonstrated that calculating eGFR based on cystatin C or creatinine-cystatin C equations strengthened the relationship of CKD with incident dementia. There was a pronounced flattening of dementia risk for eGFRcr, while the change points for both eGFRcys and eGFRcr-cys were estimated to be higher. eGFRcys and eGFRcr-cys showed stronger associations with all-cause dementia and VaD below the reference eGFR point, compared to eGFRcr. The using of cystatin C led to lower estimation values of GFR and therefore a group of individuals who were considered normal when using eGFRcr would be identified as having reduced kidney function when using eGFRcys or eGFRcr-cys, providing benefit to some of those at potential risk of dementia. Several studies have reported the advantages of using cystatin C and creatinine-cystatin C equations to calculate eGFR [19, 21]. Compared to serum creatinine derived from breakdown of skeletal muscle and consumption of cooked meat [26, 27], cystatin C is less affected by muscle mass [28], diet [29], age [19], gender [19], and ethnicity [19]. This represents that the application of cystatin C would improve the accuracy of renal function estimates.
Several mechanisms could explain the relationship between renal impairment and dementia. Firstly, brain and kidney share many common vasoregulatory features and both are susceptible to vascular damage [30]. Secondly, traditional vascular risk factors, such as diabetes mellitus, hypertension, and hypercholesterolemia, have a higher prevalence in CKD, compared to that among general population [31]. Thirdly, nontraditional vascular risk factors related to kidney damage, such as chronic inflammation, hypercoagulable states, oxidative stress, and hyperhomocysteinemia, could cause vascular injury and endothelial dysfunction and have direct neuronal toxicity, contributing to the development of cognitive impairment [32]. In addition, the accumulation of various uremic toxins in CKD, such as hyperhomocysteinemia, guanidine compounds, and cystatin C, are also associated with cognitive disorders [33].
Our results noted supranormal eGFR of ≥105 ml/min/1.73 m2, a state of kidney hyperfiltration, was related to a higher risk of all-cause dementia in our cohort, in accordance with the results of several previous studies [12, 34]. The alterations in kidney hemodynamics of hyperfiltration are reflected in the systemic circulation including response to COX2 inhibition and may reflect general endothelial dysfunction in diabetic individuals [35]. Besides, glomerular hyperfiltration has been found to be associated with subclinical cardiovascular disease including carotid atherosclerosis and left ventricular hypertrophy in nondiabetic population [36]. Many previous studies have reported that glomerular hyperfiltration is associated with cardiovascular risks, which may be explained by endothelial dysfunction as well as activity of the sympathetic nervous system [36–39]. Taken in combination with the above evidence and risk factors for dementia, vascular damage may explain the association between hyperfiltration and increased risk of dementia. However, in the present cohort, the proportion of patients with common clinical complications of renal hyperfiltration, such as diabetes and obesity, showed no increase in eGFR category of ≥105 ml/min/1.73 m2 compared to the reference category of 90–104 ml/min/1.73 m2, on the contrary, the proportion of individuals with BMI <25 kg/m2 was higher in eGFR category of ≥105 ml/min/1.73 m2 than in any other category. Hence, the interpretation of the significantly association between kidney hyperfiltration and dementia risk should be made carefully, given the estimated value of eGFR could be affected by nontraditional risk factors including weight loss and malnutrition [12, 40].
In this study, no statistically significant association was observed between eGFR with risk of incident AD. The abnormal deposition of amyloid-β (Aβ) in the brain is a major hallmark of AD pathogenesis, and the periphery takes about half of the burden in Aβ clearance [41, 42]. Some studies have supported the important role of renal in the clearance of Aβ accumulation [43], and the use of thiazide and potassium-sparing diuretics could reduce the risk of AD [44], suggesting renal dysfunction may have contributed to the pathological advancement of AD. The SCREAM cohort and the Shanghai Aging Study have also reported worse eGFR is related to higher AD risk [12, 13]. However, the similar relationship was not observed in the IMRD-THIN cohort as well as this study [11]. In this cohort, the relatively small number of AD cases in eGFR <60 ml/min/1.73 m2 (only one patient with AD in eGFR <30 ml/min/1.7 3m2) may have influenced the results of the analyses.
The evidences about albuminuria (uACR ≥30 mg/g) being associated with increased risk of dementia are more consistent than eGFR [11, 45–48]. Albuminuria is a result of endothelial damage in kidney and studies have supported moderately increased albuminuria as a risk marker of cardiovascular disease [49, 50]. The linkage of albuminuria with cerebral small vessel disease has been validated [51, 52], and common microvascular pathology in renal and brain may contribute to the development of dementia, especially vascular dementia [45, 48].
Advantages of this study lie in the large sample size, prospective design, analyses on complete cases, 3 measurements of eGFR, standard eGFR and uACR categories according to the classification of CKD, and long-time follow-up. Several potential limitations of this study should also be considered. First, there is a “healthy volunteer” selection bias. Participants in UK Biobank were less likely to be obese, smoking, and drinking alcohol on a daily basis and self-reported fewer health conditions [53]. Second, eGFR was calculated using baseline data of serum creatinine and/or cystatin C, representing a specific moment of kidney function but not long-term. Potential changes of eGFR levels during the prolonged follow-up were not captured, which may introduce misclassification bias. Third, only one-third of population in our cohort had data for ACR at baseline, which led to absence of ACR as a covariate to be adjusted in the main analyses. Fourth, some cardiomebabolic conditions related to higher cystatin C levels, such as cancer, thyroid disease, and glucocorticoid therapy were not considered in our models. Finally, as we did not restrict the inclusion population to the older adults, the duration of follow-up (median 8.97 years, Q1–Q3 7.00–10.52 years) may not be sufficient to detect the onset of dementia for those younger than 60 years, which potentially attenuates the association between CKD and incident dementia.
In conclusion, we demonstrated a strong U-shaped association between eGFR with all-cause dementia and VaD. Impaired kidney function was identified as a critical risk factor for dementia and the application of cystatin C strengthened the relationship between CKD and dementia, underlining the significant value of preserving kidney function to reduce the risk of dementia and considering cystatin C measurement as part of clinical practice. Future study is warranted to investigate whether protection of renal function in clinical practice lowers dementia risk and the pathological mechanisms underlying.
Footnotes
ACKNOWLEDGMENTS
We thank the participants and professionals of UK Biobank. This study was supported by grants from the National Natural Science Foundation of China (82071201, 81971032), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX01), Shanghai Talent Development Funding for The Project (2019074), Research Start-up Fund of Huashan Hospital (2022QD002), Excellence 2025 Talent Cultivation Program at Fudan University (3030277001), and ZHANGJIANG LAB, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University. W.C. was supported by grants from the National Natural Sciences Foundation of China (No. 82071997) and the Shanghai Rising-Star Program (No. 21QA1408700).