
Abstract
Background:
With the increasing incidences of dementia in aging societies, attention should be paid to the social context in which people with dementia live. One of its aspects is language transmitting beliefs, perceptions, and behavioral patterns. An analysis of understanding the diagnostic label of dementia may reveal the role of semantics in the process of social cognition of this disease.
Objective:
The overall aim of this study was to investigate the understanding of the word dementia (otępienie) in the Polish language.
Methods:
Frame semantics approach was applied. The structure of semantic information was uncovered with the concept of frame utilizing The National Corpus of Polish (the biggest corpus of contemporary Polish language of 1,500 million words). Additional data was collected from Polish speaking adults in Poland.
Results:
The analyses allowed to identify the otępienie frame for Polish and verify how its elements are filled in by the general population, indicating the selectivity of colloquial knowledge about dementia. Dementia deviates from the prototypical disease. Need to care for the person with dementia outweighs treatment options. The cognitive symptoms and characteristics of the subject are salient. The perceptions of people with dementia embedded in semantics of the diagnostic label might create a basis for prejudicial attitudes among lay part of the society.
Conclusion:
Findings give foundation to further studies on relationship between semantics and social cognition of dementia which has a real impact on the social and clinical situation of people with dementia and may facilitate formulation of tailored messages aimed at building dementia-friendly society.
INTRODUCTION
The prevalence of neurodegenerative diseases such as dementias in aging societies is growing [1]. Therefore, it is important to be observant to the social context in which people with dementia live [2, 3] and ensure that the public beliefs do not induce stigma resulting in additional disability [4, 5]. Existing literature emphasizes that social perceptions and discourse around dementia are dominated by the “Prescribed Dis-engagement∑” [6]. This term, coined by Kate Swaffer, refers to repeated societal views, including the attitude of specialists, that once diagnosed with dementia, nothing can be done and the only option is to surrender and withdraw from the current life. These attitudes disempower people with dementia, ignore their personal experiences, and elevate the stigma [6]. One of the components contributing to this image of life with dementia is the language used for labeling a nosological unit and for referring to people with dementia in medical and lay communication [7].
Dementia and language
Language is perceived as a forceful transmitter of socially shared beliefs, perceptions and behavioral patterns [8–10]. Its power is bi-directional. Language usage mirrors stereotypes existing among speakers, and conversely, social category stereotypes are fueled by the language used in communication at all its levels [8]. Negative consequences of this feature of language are reported in studies on social cognition of mental illnesses [10–12] including dementia [13, 14]. Research shows that discourse built around dementia can be perceived as stigmatizing [5, 15]. This characteristic already manifests itself on the lexical level when looking at the diagnostic label of dementia— its understanding and connotations held by users of a given language [7, 16]. Due to its common meanings and usage, it can evoke specific perceptions and beliefs about people diagnosed with dementia [17]. Despite criticism of the term dementia [17, 18] and calls for its removal from the current DSM-V classification [19], dementia is still used both in professional and lay communication. Therefore, it is the word that shapes the perception of the disease and of people diagnosed with dementia.
In English, the medical term dementia is derived from Latin de mente what literally means a being out of one’s mind. The Latin stem demens stands for i.a. out of one’s senses, insane, foolish, reckless or mad [20]. In Poland, dementia prevalence is growing, but awareness is still low and the topic is unrecognized in a public discourse [21, 22], the diagnostic label of dementia (Polish otępienie) can be charged even more with its common understanding and connotations. Root word of Polish otępienie is tępy what can be translated as blunt, dull, stupid, dense, or foolish. The dictionary definition of the term otępienie [23, 24] refers not only to a natural process and a significant decrease in mental performance caused by brain damage. The second meaning of the word is linked to feelings and emotions domains: passive giving in to something, lack of will, or strength to act. The synonyms can be translated as: apathy, inertia, numbness, malaise, marasmus, lethargy, deadness, paralysis, torpor. All these connotations in both Polish and English might create the belief system about dementia among speakers and shape the dementia’s discourse in the society [25]. Insights into culturally specific dementia discourse is also critical to influence awareness raising campaigns and challenge barriers to help-seeking as well as other types of societal discrimination [21, 26].
Frame semantics
One of the prominent cognitive linguistics theories useful for the research on words’ meaning is the Fillmore’s frame semantics [27, 28]. Its basic premise is that the meaning of a word is embedded in understanding of the conventions and a cultural background encompassing its use [27, 28]. Thus, the semantics of a given word is described in relation to the wider structure of common experiences, beliefs, actions, and elements accompanying occurrence of a given word [29]. The structure of the related concepts that is activated to understand the meaning of a given word is called the frame [27, 28]. It is not possible to understand the meaning of a single word without also having access to knowledge that relates to that word. Limited knowledge of the background concepts will determine the complete or partial misunderstanding of a given word [28, 29]. Thus, frames impose a certain worldview and are deeply rooted in one’s experience and culture [27]. The structural elements of the frames are called slots. Slots can be seen as specific positions in a frame structure allotted for concepts that make up the frame [30, 31]. Developed frames, as the cognitive schemas or mental representations, serve as templates to which the words can be related and thus interpreted [31]. In the process of understanding of expressions, words activate frames which organize the contextual knowledge. Slots— structural elements of the frame— are pre-defined and labeled according to the categories their represent, i.e., the roles. A given, interpreted situation provides concrete details that fill the labeled slots of the frame. Having a pre-defined frame (with labeled slots which can be filled by specific instances) in memory is the basis of the process of understanding [27, 31]. As an example, the sentence He bought some bread activates the so called Commercial Transaction frame that includes slots for such roles as: buyer, seller, goods, money and additionally: price, place, time, etc. Each slot labeled according to its role can be filled with specific instances, as in the example: he fills the buyer frame slot and bread fills goods frame slot [29]. Each frame consists of the obligatory slots which are the core for the comprehension of the situation and have definitional value. Those elements are always the part of knowledge about the given concept and have the central position in the frame (as in the example where comprehension of a buying situation refers to understanding roles of the seller, buyer, good sold and means of payment). Frame, however, can relate to the more complex event and may include additional slots of non-definitional value. They may therefore be part of a given event, but they occupy a peripheral place in relation to the central elements (as a place of the transaction or price of the sold good which are not necessary to understand the concept of buying but outline a broader context allowing a better understanding of the situation). Peripheral elements in turn can form sub-frames grouped in relation to a specific concept or event (e.g., all elements relating to money such as currency or payment methods can be grouped in a smaller frame detailing the money element) [28–30]. In this paper, the expression frame element is used as a synonym for slot.
The disease category
To the authors’ best knowledge, the dementia frame has not yet been identified, neither in English nor in Polish. Uncovering of the structure of semantic information with the concept of frame is possible by analyzing the actual language use via corpus data [33] and reference to the broader context, i.e., the frame underlying the word disease (the hyperonym of dementia and its definitional meaning) [34]. The FrameNet [35, 36] (lexical on-line database annotated according to the frame semantics assumptions, mapping the lexical units into the semantic frames and marking their semantic roles) situates the disease within the Medical Condition frame and shows its central and peripheral elements, listing also lexical units belonging to this category (Fig. 1).
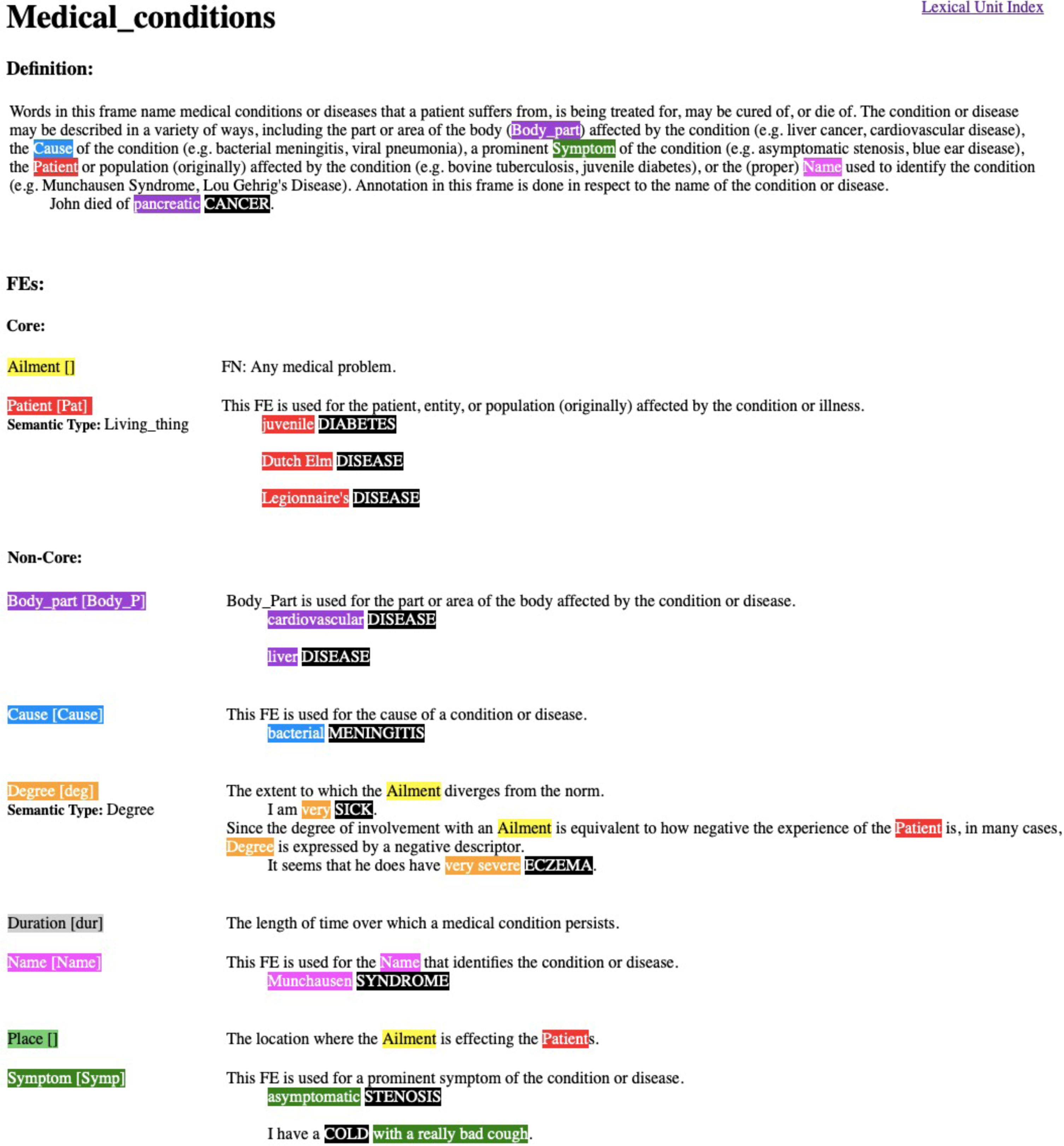
FrameNet Data: Lexical unit index for the Medical conditions. https://framenet.icsi.berkeley.edu/fndrupal/luIndex
Within the disease category based on common knowledge, dementia is peripheral as it deviates from the prototypical disease scenario [36]. The colloquial disease category encompasses a few central elements defining a typical disease scenario [36]: full health (as a reference point); attack of the external factor (an invisible germ or a sudden accident); evident and visible symptoms of the disease (perceived by the sick subject and the surrounding); treatment to eradicate the disease (recovery of the subject as a final stage).
Since dementia has been identified as a peripheral concept within the disease category, uncovering the structure of semantic information with the concept of frame may determine to what extent the understanding of dementia deviates from the prototype disease.
Frame approaches
Frame semantics is a specific application of the broader term frame used in cognitive approaches [27]. Fillmore’s theory enables the study of how words (and other linguistic forms) are associated with the cognitive structures (frames) which largely influence the process of understanding of the meaning [27]. Broader frame approach refers to the ways people use cognitive frames in conceptualizing their experiences not only through language [27].
Broadly understood cognitive frames are widely used in the analysis of mental representations of various medical concepts [37–40] including dementia [26, 41–43]. An insight into the implicit worldviews and common knowledge about dementia allow identification of perceptions, attitudes and behaviors related to this disease [43], all of which are important to inform public awareness campaigns aimed at reducing stigma and discrimination.
Despite the interest in identifying dementia frames in its broad sense [26], little attention has been paid to linguistically oriented approach to the dementia frame. Although frame semantics is used by linguists in the study of current medical issues [33, 39], it is less commonly applied in social science and medicine [44]. However, sparse scientific reports on merging the frame semantics with social and medical concepts (e.g., COVID-19 or risk) promises a new perspective for analyzing socio-cognitive understanding of dementia.
This study aims to investigate the understanding of the word dementia (Polish otępienie) in the Polish language among the general public in Poland in relation to the concept of the prototype disease. While much research has focused on the stigma around dementia and utilized the concept of frame in describing culturally anchored images of dementia, few have centered upon language and its impact on perceptions of dementia. To our knowledge, the current research is novel in its attempt to use Fillmore’s theory of frame semantics to study social cognition of dementia. In addition to applying the theory of frame semantics to a previously unexplored concept, our research adds to the still scarce literature on the perception of people with dementia living in Poland.
Importantly, the current article concerns only one of the existing Polish expressions relating to the phenomenon of dementia. The focus is put on word otępienie which is the name of the disease used in the ICD-10 [45], in force in Poland. Other expressions such as demencja or choroba otępienna used in colloquial language are beyond the scope of this study. Thus, the present analysis refers only to the selected aspect of the dementia semantics in Polish.
Nevertheless, studying the meaning of otępienie in Polish language promises to be useful in revealing the role that semantic plays in the process of social cognition of dementia in Polish. Further, combining the linguistic approach with medical issues may provide in-depth insights about the basis of the dementia discourse and its consequences for the treatment and perception of people with dementia in Polish society.
MATERIALS AND METHODS
Study design
Frame semantics approach [27] was applied in this study to investigate understanding of the word dementia (Polish otępienie) in Polish language among the general public in Poland. The study obtained ethical clearance from Wroclaw Medical University Ethics Committee (KB –602/2019), and was performed in accordance with the Declaration of Helsinki [46].
Procedure and data sources
Understanding of otępienie in Polish was studied at two levels (see Fig. 2). The primary stage was to uncover the dementia frame for the Polish language by analyzing data from The National Corpus of Polish (NKJP; the biggest corpus of contemporary Polish language) [47]. The second stage was aimed at analyzing how general public fills the slots of the frame in question.
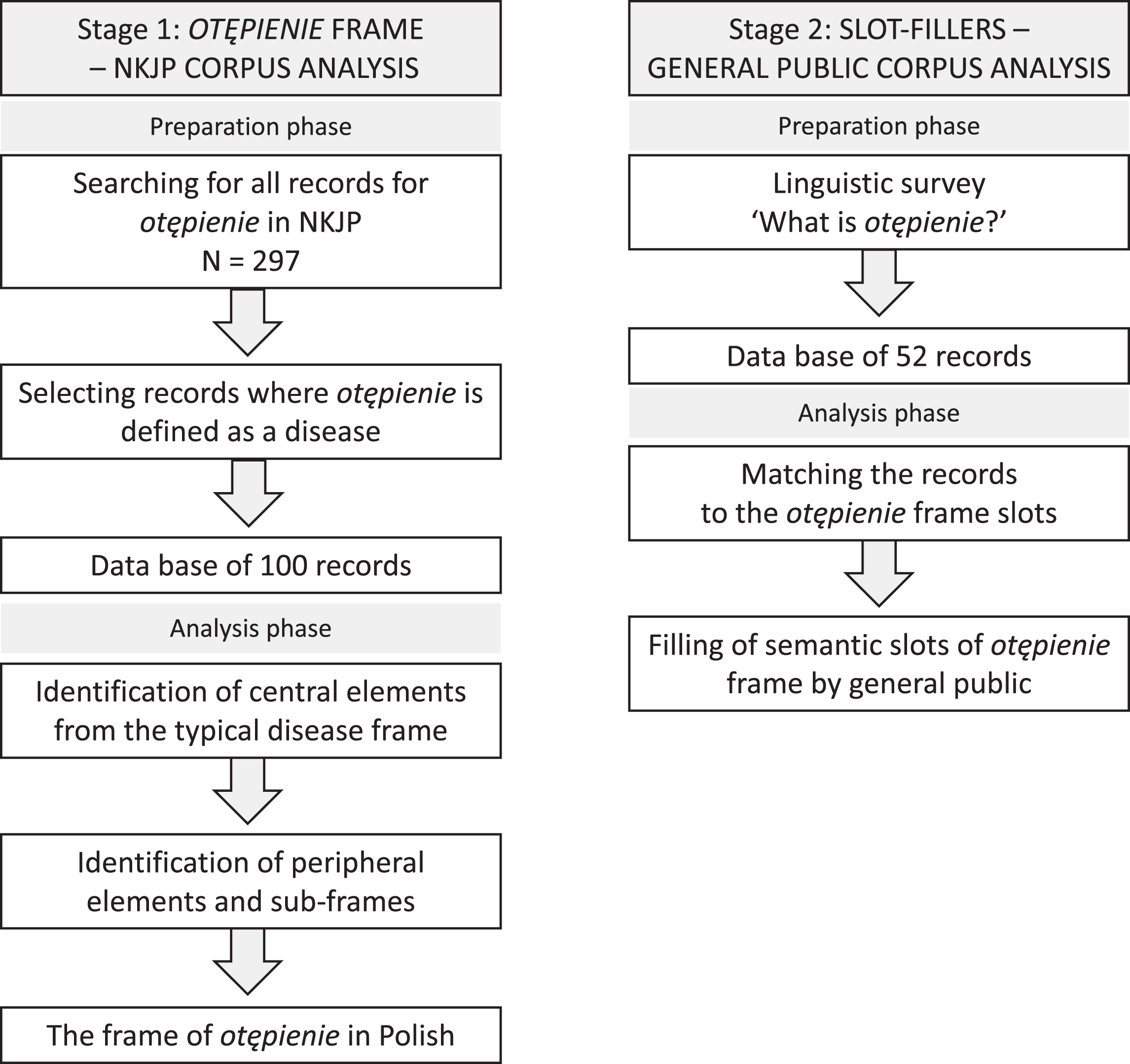
Two stages of data analysis –from the linguistic corpora to the structure of frame.
Stage 1. The otępienie cognitive frame –data collection
The first step to develop the otępienie frame for Polish was to search and identify the uses of the studied word in the NKJP.
NKJP is an over one and a half billion words collection of samples of written and spoken contemporary Polish language (from the beginning of the 20th century). The structure of the corpus ensures its representativeness and balance (thematic and genre diversity of texts, the representation of interlocutors of both sexes, ages, and from different regions) [48]. The corpus can be searched with the open-accessed PELCRA search engine [47]. Its functionality allows to search for various configurations of words: single words, proverbs, phrases, idioms. Search results are all examples of search word found in the corpus. Each item consists of the searched word with its context (text paragraph) and the metadata: source (title of the book, newspaper, etc.), channel (book, weekly newspaper, journal, Internet, spoken language etc.), type (fiction, journalistic writing, official letters, etc.), date of the publication. A more detailed specification of the NKJP and PELCRA is available elsewhere [48].
Exact matches of a single word otępienie including its inflected forms were searched in NKJP automatically via PELCRA search engine. 297 paragraphs from 206 different texts matching the query were found. All search results were exported to the.xlsx data base for further analysis.
Each record was analyzed separately for the meaning in which the word otępienie was used. The meanings were determined on the basis of dictionary definitions of the word otępienie in Polish. According to the Polish WordNet (a lexico-semantic network reflecting the lexical system of the Polish language) [23] the word otępienie can be defined as: (1) Disease, (2) Feelings, or (3) Actions. Manual analysis of each record was aimed at selecting text samples where the word otępienie could be defined as a Disease. Doubtful contexts were discussed between the authors with expertise in Polish linguistics and psychiatry until consensus was reached.
This procedure allowed preparation of the database of 100 corpus text samples with the word otępienie defined as a Disease. These data were used to uncover the frame of dementia for the Polish language.
Stage 2. Slot filling of the frame by the general public –data collection
To explore the slot filling of the otępienie frame by the general public samples of the written language collected among the study group were used. Linguistic data were obtained through the simple elicitation task— respondents were asked to write an answer to an open-ended question (with no word limit): “What is dementia (Polish otępienie)?”. The question was nested in a bigger questionnaire titled Health Belief Research. The linguistic task was initial for the questionnaire so that other scales’ items did not bias the answers. The sociodemographic section enabled to complete data with the variables such as: age, gender, nationality, native language, place of residence, education, and a degree of acquaintance with the person with dementia.
A survey was conducted online aiming at the general public in Poland. Inclusion criteria included: being a native speaker of Polish and not being primary carer nor health or social care provider for people with dementia. There were no additional exclusion criteria. The survey was created on the Google Forms platform and distributed online to potential participants using snowball sampling. Incentives to participate in the study were published on the department’s website and on Facebook. The online form included the consent form providing information about the purpose of the study, research procedures, and the information that submitting the form is tantamount to consenting to participation in the study. Data collection took place between June and September 2020 as a part of the international project Cognisance –“CO-desiGning dementia dIagnoSis And post-diagnostic CarE”.
Data analysis
Stage 1: The otępienie cognitive frame –analysis
To uncover the structure of semantic information on dementia in the Polish language a frame semantics approach [28, 49] was adopted. Analysis of the pre-prepared database from the NKJP was guided by the question: What elements (slots for the involved semantic roles) of otępienie are present? The first step was to identify if the central elements [50] fixed in the Medical Condition frame (slots for roles of: subject, disease, symptoms) [40] emerge from the selected corpus data on otępienie. Each record was analyzed and assigned to the relevant slot (one text sample may have matched more than one slot). Categorization were made independently by the two researchers and compared. Incompatibilities were discussed until the consensus was reached. The next step was to identify slots that are peripheral [50] in relation to the central elements (slots for roles of: subject, disease, symptoms). Each record was analyzed and denoted with the potential label independently by the two researchers. As part of discussions between researchers, labels were unified and relevant items were assigned to the slots. Based on the similarity some slots were further grouped into the clusters forming consecutive sub-frames.
The outcome of the analysis was the development of the frame of otępienie in Polish. The frame became a referential to analyze language of the general public and their understanding of otępienie.
Stage 2: Slot filling of the frame by the general public –analysis
Answers to the open-ended question collected by the linguistic surveys (n = 52) have created a text corpus which was used to explore the slot filling of the frame by the general public. The otępienie frame was used as a referential. Each record from the general public corpus was analyzed and matched to the relevant slots of the otępienie frame. Each record could fill several slots. Number of quotes each slot was counted and converted into percentages.
The results of the analysis indicate what slots of the otępienie frame are filled in and how dementia is represented in the common knowledge of Polish speakers.
RESULTS
All data were obtained and analyzed in Polish. All the quotes cited below were translated into English. Back translation was applied to ensure the correct transfer of meaning. The words denoting the frame slots are in italics.
Stage 1: Otępienie frame
The cognitive frame of otępienie in Polish language uncovered on the basis of NKJP is shown in the Fig. 3. Central elements include: subject (‘person experiencing symptoms of disease’), disease (‘the condition of the subject whose organism is malfunctioning’), and symptom (‘a feature which is regarded as indicating a condition of disease’). Each of the central elements link several peripheral slots.

Otępienie frame uncovered on the basis of the biggest corpus of the Polish language. The figure shows the interconnections between the central and peripheral elements of otępienie identified in the NKJP analysis.
Subject
Subject’s group encompasses characteristics (‘what the subject is’) showing that a person with dementia is dependent on the carer, confused and increasingly disoriented.
“If the dementia worsens, the sick person cannot live without help. Leaving the house should always take place in the company of the carer, because the sick person gets lost after a dozen or so steps; a person does not remember the address, telephone number or the names of the carers.”
Behavior (‘how the subject experiences disease and behaves’) corresponds primarily to the consequences of memory problems. It is related to inability of a person with dementia to perform daily activities without the supervision of others, getting lost, forgetting about basic issues or being dangerous to oneself and others.
“After a while the sick person forgets what he said or was asked about and is not able to realize, for example, whether he ate breakfast or dinner that day, or whether someone was visiting him.”
“[Caregivers] are in fear that the father or mother will hurt themselves and blow up the house.”
The difficulties manifested in characteristics and behavior are experienced by people with dementia on an affective level and involve different emotional responses to their cognitive decline. Feelings (‘what the subject experiences in relation to disease’) includes such emotional states as: regret, sadness, annoyance. People with dementia, despite their disabilities, are capable of feeling natural emotions.
“The patient perceives these disorders with regret: I have always had a good memory. What is happening now?”
“Age-related dementia does not cause the person affected by it to suddenly lose the ability to feel joy.”
Characteristics and behavior of the subject entail other elements, necessary for the person experiencing dementia’s symptoms. These are care (‘concern for the good condition of the subject’) and carer (‘the one who helps the subject in the disease’).
“I am a single mother of a permanently ill son and the only carer of my father suffering from multifocal brain damage (advanced senile dementia, dementia). I have not worked for two years, because my dad requires permanent care.”
Carer (‘the one who helps the subject in the disease’) correspond to people who are involved in the process of care. They are mostly children of the people with dementia. Representatives of the institutions are represented but as the experts, not directly involved in caring responsibilities.
“In 20 years, the number of patients will at least double. Virtually all the sick for the next 8–20 years will go to the care of their closest relatives: working 40–50-year-olds will take care of them –says Alicja Sadowska, president of the Polish Association for Assistance to Persons with Alzheimer’s Disease and a member of the board of the European Alzheimer Federation.”
Carer’s slot connects specific carer’s features such as carer’s behavior and carer’s feelings. Behaviors include helping out a person with dementia in basic daily activities but also efforts to ensure the dignity and to provide necessary stimulation.
“We did all the household chores for her, irritating that she was working too slowly. Patience is the most important thing in this disease.”
“Every day, Elżbieta from Łódź buys her mother Gazeta Wyborcza [newspaper] so that she can read it, even though she does not understand anything. Because with this newspaper, the mother feels like herself. Elżbieta Mazurek, the daughter-in-law of Mrs. Janina from Roztocze [region in eastern Poland], when guests come, always places her mother-in-law at the table and ties her with thick sticky tape to the chair so that her mother does not fall off. Mom doesn’t understand anymore, but Ela thinks she has a right to be with her family, which has always been important to her, even if she may not already be aware of it.”
The role of the carer and its burden triggers difficult emotions which have been grouped in carer’s feelings slot.
“I [carer of a father with dementia] lack not only money, but mainly strength and patience to bear this very heavy cross.”
“It’s not easy to live under the same roof with someone suffering from Alzheimer’s disease.”
Due to the similarities between process of care and carer with behavioral and emotional characteristics, those slots are grouped into the separate ‘care cluster’.
Care is also linked to the place in which a subject is located and where he or she is taken care of. The major location is home as the families have a tendency to take care of the person with dementia independently. The institutional care options (day and long-term care facilities, foundations) are lacking.
“The same applies to access to specialized care institutions –only a few percent of patients in Poland use them (more than half in Sweden and Finland). There is no tradition in Poland to leave loved ones to nursing homes.”
“A large part of the caregivers, for lack of other option, will lock the sick person at home, go to work, and then spend eight hours in the office with their heart in their mouth, in fear that the father or mother will hurt themselves and blow up the house. In many cases, care will be limited to serving a plate of soup, washing clothes and persuading people to enter the bathtub every day. When you need to combine work with this care, it is still heroism. But for a sick person it is not enough.”
Comprehension of a subject— person experiencing symptoms of dementia— entails a wider context related to his or her characteristics, behaviors, and feelings. Disorientation, memory problems resulting from the dementia symptoms, make it difficult for the person to function daily and make them dependent on the carer. The definition of a person with dementia thus extends to the concept of care and carer. Carer’s behaviors and feelings reflect person with dementia needs and result from the specificity of the disease.
Disease
Disease is defined as ‘the condition of the subject whose organism is malfunctioning’. In dementia, the linguistic definition focuses primarily on the brain which fills the frame’s slot: organ (‘the part of the body affected by the disease’).
“Alzheimer’s disease can be diagnosed with absolute certainty when two criteria are met: a clinical examination diagnoses dementia, and amyloid plaque and damaged neurons are present in the brain.”
Cause (‘what causes the disease’) of dementia is ambiguous therefore this frame element features various components such as: age, organic changes, genetic cause, and also inconclusive scientific results.
“In most patients, the causes still cannot be determined.”
Frequent features of the disease are grouped into time slot (‘when the disease occurs and how long it lasts’) and strength slot (‘to what extent does the disease affect the subject’). Temporal aspects of dementia are linked to the older age, gradual course and slow progress.
“Dementia occurs primarily in the elderly, but not exclusively.”
“Alzheimer’s disease has several stages. There is an initial stage, slight, moderate and deep and very deep dementia.”
Strength is metaphorically defined as ‘height’, ‘depth’ or ‘area’. The disease’s symptoms can growth or increase, can be more or less extensive or deeper.
“As organic changes increase, memory deficits become more extensive and the ability to remember almost completely disappears, aggravating disorientation.”
Evaluation of the disease (‘how it is assessed’) weights the dementia up as a social problem and a serious health threat.
“Diseases of the nervous system are a huge problem, posing a serious health threat.”
Assessing dementia as a social challenge is closely related to its dissemination (‘how many subjects experience the disease’). The dissemination slot is filled with the statistical estimates of the number of dementia’s cases around the world and in the specific countries (especially Poland and USA as a reference point).
“The prevalence of dementia in the United States is estimated at approximately 10% of people over the age of 65 and increases with age.”
Prevalence of dementia and its recognition as a social challenge steam from the treatment possibilities. Treatment slot refers to ‘measures and actions that are to diagnose and stop the disease or restore health’. In dementia a full recovery is non-feasible. Thus, the treatment takes a peripheral place within the otępienie frame which deviates from the prototypical disease scenario. Nevertheless, diagnosis and access to treatment options to slow the development of symptoms are possible. Treatment process is further divided to the diagnosis and post-diagnostic therapy. Diagnosis slot refers to steps necessary to make a diagnosis and to difficulties in the diagnostic process.
“It is not easy to get them [people with dementia] out of the crowd. In Poland, it is even more difficult because— according to specialists— 9 out of 10 GPs are not able to diagnose Alzheimer’s disease. It is better in large cities, but also here no more than 10% of patients are treated. sick. The diagnosis process requires knowledge, a serious approach to the patient and time.”
Post-diagnostic treatment slot contains quotes reflecting organizational barriers to effective treatment (uneducated medical staff, high costs, time, and serious approach to the patient) and its effects (although the dementia is still not curable, treatment can relieve symptoms).
“Although Alzheimer’s disease is incurable, its symptoms can be suppressed –provided the doctor recognizes dementia early and the family can afford the best treatment possible.”
Medical staff involved in the treatment and care (neurologists, psychiatrists, psychologists, nurses) is grouped under the doctor’s slot (‘the one who heals the disease’). Healthcare professionals are described in terms of their tasks as well as gaps in knowledge in relation to dementia.
“Doctors and nurses from the Neurological Department of the Wołomin hospital struggle with such diseases (dementia, Parkinson’s disease, and peripheral nerve damage) on a daily basis. Thanks to them, the patient is provided with quick diagnostics and then intensive treatment.”
“According to specialists - 9 out of 10 GPs are not able to diagnose Alzheimer’s disease.”
Treatment possibilities— although limited and not able to fully heal— encompass medication slot (‘what heals the disease’). It is mainly focused on the researchers’ efforts to find the best remedy and the expectancies of the patients and their families. The available drugs are difficult to use and have questionable effectiveness.
“In a monograph on tea published in the journal Lek w Polsce [Medication in Poland] researcher from Medical University in Warsaw lists nine diseases that can be helped in treatment (especially green tea): atherosclerosis, obesity, dementia, certain cancers, diabetes, caries, digestive disorders, androgenetic alopecia, infections.”
“There are three drugs that are available on the market: Aricept, Exelon and Reminyl –says Alicja Sadowska. –The family has to pay PLN 120–150 for them every month and only 4 percent. sick people benefit from this therapy.”
Due to the close interrelations and lack of exclusivity, all slots linked to the treatment are grouped into the separate ‘treatment cluster’.
Central disease element (’the condition of the subject whose organism is malfunctioning’) refers to many contextual characteristics of dementia. They mainly focus on the brain as an organ affected by the lesions, the progressive nature of the symptoms, and the old age as typical time when people develop symptoms. The context of dementia covers many unrecognized areas— the specific causes of the disease are unknown and there is no treatment to completely remove symptoms. For this reason, treatment is present in the dementia frame, but occupies a peripheral place in the understanding of dementia. Dissemination of dementia and no cure option result in evaluating the disease as a significant social problem.
Symptoms
Last central element of the dementia’s frame is symptom (‘result of the disease’). It is divided into two sub-groups: invisible and visible. Invisible symptoms are related to the causes and organ of the disease and are described by the brain and neurons damages.
“Amyloid senile plaques and damaged neurons are present in the brain.”
Visible symptoms are grouped into three sub-categories. Cognitive symptoms slot contains references to intellectual disability and severe, progressive decline in all cognitive processes resulting in overall deterioration of person’s functioning. Memory problems and disorientation are the most frequent symptoms.
“The decrease in intellectual efficiency consists mainly in the impairment of the ability to think logically, and thus to perform such mental operations as: analysis, comparison, generalization, inference and others.”
Another group of visible symptoms are those emotional. They are listed along cognitive deterioration and are characterized mainly as emotional lability. They are dominated by the overall disorientation of the person with dementia. However, generally emotional sphere is preserved and the person with dementia maintain the ability to express emotions despite cognitive changes.
“Despite reduced intellectual performance, memory and orientation disorders, patients generally maintain good emotional contact with family and friends.”
Behavioral symptoms are described as the flagship signs of dementia and the first symptoms that allowed to distinguish dementia from other medical conditions.
“The patients are unable to clean up themselves. They lose orientation, stop talking, and their walking and movement disorders increase.”
“She treated her doctor as a guest, excusing herself that she had not finished her work yet. After a while, she screamed loudly that she wanted to hurt her with a knife. She was throwing sheets of bedding, screaming in a monstrous voice for hours. Eventually she became completely apathetic, she went to bed with her clothes on, she did not observe personal hygiene. [Alois Alzheimer’s description of the patient with dementia]”
Symptoms are directly related to the characteristics of the disease and are inherent in the conceptualization of the subject. In understanding of dementia visual symptoms are most salient. They focus on cognitive problems in various domains as well as general disorientation and unusual behavior. Changes in emotional expression are also vivid, but importantly, affective sphere is preserved in people with dementia.
Stage 2: Slot filling of the frame by the general public
Participants’ demographics
Overall, 52 participants completed the survey. 41 were women (78.8%). All participants were native users of Polish language currently living in Poland. 31 participants (almost 60%) did not know a person with dementia. The general characteristics of the sample are presented in Table 1.
Demographic structure of the study sample
General public frame
Filling of frame slots by the general public is presented in the Fig. 4. All central elements of the otępienie frame are represented. Subject group links three peripheral elements: characteristic (‘what the subject is’), behavior (‘how the subject experiencing the disease, behaves’), feelings (‘what the subject experiences in relations to disease’) with omission of whole care cluster and place slot.
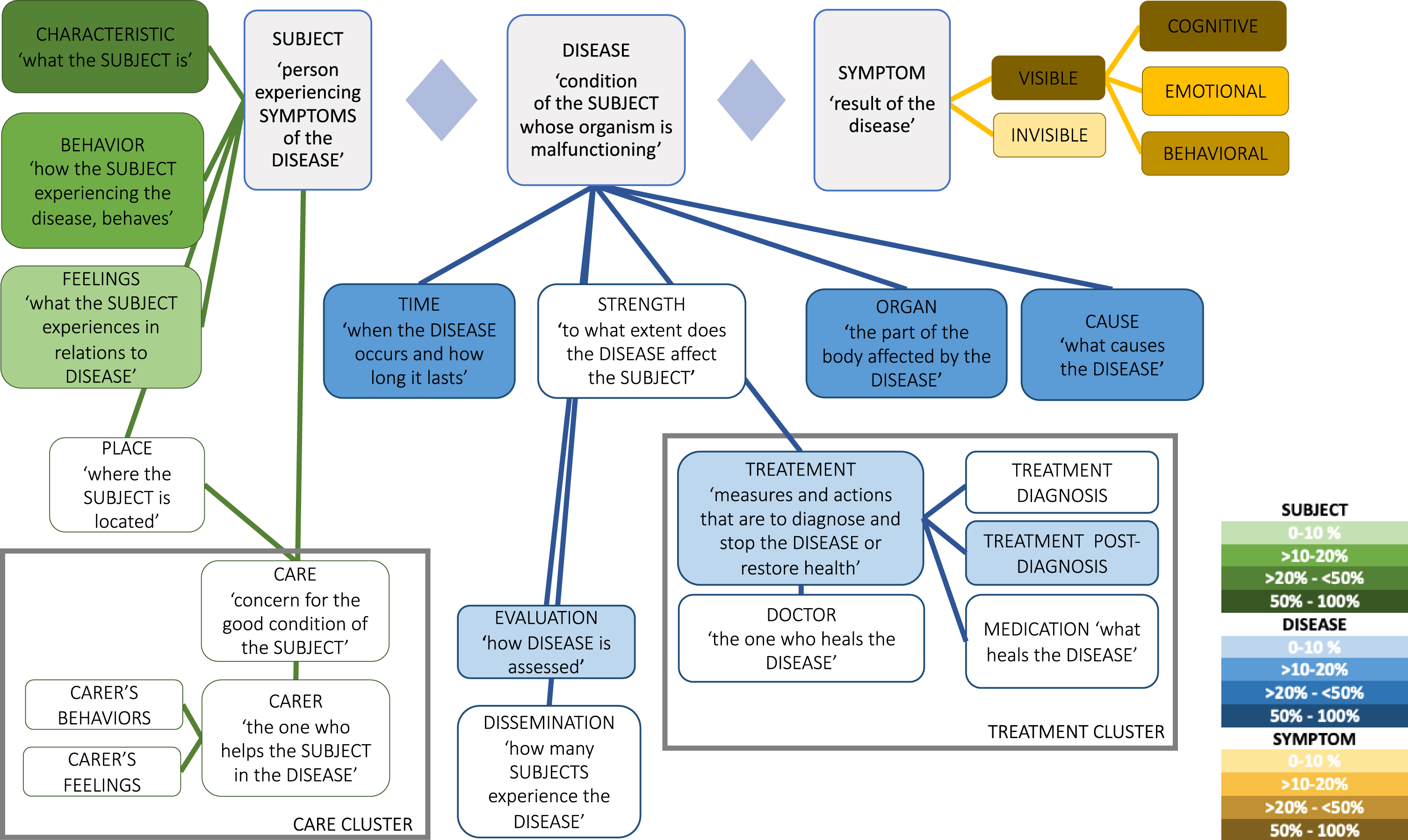
Slot filling of the frame by the general public. The figure shows the filling of semantic slots of otępienie frame by the general public with reference to the percentage of the slots’ filling. The color intensity indicates the frequency of a given category within the studied corpus.
Subject
Subject’s characteristics listed in the corpus of general public quotes include such features of a subject as: indifference to surrounding, unresponsiveness, exclusion from normal feeling. Person with dementia is described as sleepy, apathetic. Dementia makes the person infantile and is described as a loss of one’s self.
“A state during which a person is different than usual when he was younger. For me, dementia is a deprivation of free and learned social skills. It is difficult to establish real contact with a person with dementia, their needs and messages are treated more like a child.”
“A person who is unresponsive or has a reduced response to external and internal stimuli.”
“Dementia, asking the same questions several times, not recognizing loved ones, lack of empathy.”
“Lack of mental acuity, delayed reactions, no reaction.”
“When the loved one disappears. She is still physically present, but ceases to be her old self.”
Behavior of the subject is related to disorientation and general assumption that a person with dementia does not understand what is happening around. Typical behaviors of a person with dementia are related to the general inability to perform tasks, to being slow and getting lost in daily activities.
“Dementia is asking the same questions several times, not recognizing loved ones; lack of empathy.”
“The person is not able to fully perform all the basic activities or is able to, but it takes her or him more time. He or she is not fast, but rather slow. He or she is not 100% mentally fit.”
Feelings of the subject are also strongly interlinked to the disorientation of the subject. In the majority of the quotes the confusion prevents people with dementia from feeling emotions in natural way. Person with dementia is therefore emotionally flatten or blunted. At times, a confusion causes anxiety and fear that a person with dementia can feel.
“Loss of full awareness and discernment in one’s own situation, loss of many skills, feeling of living in the past, eternal fear related to not understanding the situation, behaving in an irrational way for an outsider.”
“State in which a person is reluctant to act, shows no interest, as if he was sleepy. She is also indifferent to external stimuli.”
“Lack of orientation in the field, frequent failure to recognize relatives, lack of focus, fear.”
“Impossibility of full perception. Indifference to the environment, own needs and reality.”
Subject in general public comprehension is defined through the prism of deficiencies in cognitive, behavioral and emotional abilities. In contrast to the conceptualization of the subject in NKJP, general public understanding does not involve the issue of care and does not acknowledge the role of the carer in people with dementia functioning.
Disease
The most frequent elements grouped around to the disease encompasses time, organ and cause. Dementia is unequivocally associated with old age.
“Mental illness of the elderly.”
“A state in which a person is different than usual when he or she was younger.”
“The disease usually appears in old age.”
The organ affected by the disease is a brain or mind. Due to the damages in the brain structure its functioning is stopped or switched off.
“Dementia is a state of limbo. We are not receiving any information at that moment, because our brain is as if turned off.”
“A person who does not perceive reality properly due to brain damage.”
Cause of dementia is attributed mainly to the organ and time of its occurrence. These are: the brain damage with other neurological problems and the older age.
“Dementia is a general decrease in mood and mental abilities caused by a factor beyond our control, usually caused by an illness. It manifests itself as general apathy, weariness, lack of thinking.”
“A disease that usually appears in old age due to the impairment of cognitive processes. Factors may be genetic background, stress, incorrect lifestyle (sleep, diet, exercise).”
Less frequently filled slot is evaluation of the disease. It is related to the characteristics of a subject who is assessed as a childlike and disabled to maintain meaningful social contacts.
“A state in which a person is different than usual when he was younger. For me, dementia is a deprivation of free and learned social skills. It is difficult to establish real contact with a person with dementia, their needs and messages are treated more like a child.”
The treatment cluster is filled only partially. There is only one quote suiting the post-diagnostic treatment slot. This is a referral to the lack of possible treatment for the causes of the disease.
“It is a neurological disorder that is associated with senior age and may be vascular in nature. It manifests itself as deterioration of cognitive functions, dysfunction, and memory problems. It progresses over time and causal treatment is rarely possible.”
Contextual knowledge about the disease emerging from general public corpora focuses mainly on damages in brain or mind and on old age when dementia occurs. Treatment options are not recognized. Evaluation refers to evaluating functioning of a person with dementia. Dementia is not considered in a broader social context.
Symptoms
Corpus built with the general public quotes contains references to both visible and invisible symptoms. The invisible symptoms are closely related to the organ in the disease’s group and are focused on the degenerative processes in the brain.
“Degenerative process of brain tissue.”
“A person who does not perceive reality properly due to brain damage.”
Although invisible processes are described, the visible symptoms prevail. The cognitive problems are especially emphasized. The most frequent are deficits in memory and thinking, however quotes contain referrals also to other cognitive domains. Description of the cognitive symptoms in some cases are metaphorical and are compared to switching off, zoning out or dropping off.
“A disease associated with a decrease in the level of functioning of cognitive processes –in particular memory and thinking.”
“Mental activity is kept to a minimum compared to its glory years.”
“Dementia is the loss of contact with reality, the inability to choose the right words or express thoughts.”
“Problems with memory, to zone out to another world.”
Cognitive disorders are also linked to emotional symptoms. They are mostly associated with general mood drop and apathy. The quotes show that dementia deprives a subject of the ability to feel emotions— it narrows the range of emotional states or exclude the person from being empathetic toward outside world.
“Dementia is a general decrease in mood and mental abilities caused by a factor beyond our control, usually caused by an illness. It manifests itself as general apathy, weariness, lack of thinking.”
“Dementia, asking the same questions several times, not recognizing loved ones, lack of empathy.”
“Inability to fully assess the psychophysical situation in which the individual is and expressing the full spectrum of emotions.”
Also, behavioral symptoms are represented in studied corpus. They are focused on irrational, not adequate to the age behaviors of the subject and to the apathy, withdrawal and anxious reactions to the incomprehensible stimulus from the surrounding.
“Loss of full awareness and discernment in one’s own situation, loss of many skills, feeling of living in the past, eternal fear related to not understanding the situation, behaving in an irrational way for an outsider.”
“Lack of short memory, lack of logical thinking, forgetting about physiological needs, indifference.”
Conceptualization of the symptoms by the general public comprises of both invisible and visible indications of dementia. The most prominent signs in recognizing dementia are cognitive deficits, often characterized in a metaphorical way. Unlike NKJP, emotional symptoms are treated as the disappearance of this sphere, not its lability.
DISCUSSION
This study is the first attempt to apply Fillmore’s theory of frame semantics [28, 49] to investigate the meaning of dementia in the Polish language. Its results are the identification of the cognitive frame of otępienie for Polish language and exploration of how the frame slots are filled by the general public. The described linguistic meaning of the word otępienie unveils the contextual knowledge determining its comprehension. The beliefs, attitudes, and experiences reflected in the language allow to infer about the social perception of dementia. The results highlight that dementia stereotype is burdened with negative traits that may perpetuate stigma and indicate which common beliefs should be addressed to support the creation of a more dementia-friendly society in Poland.
The frame of otępienie represents the background knowledge which constitute the understanding of dementia as a disease in Polish language. Interpretation of the studied frame can be referred to the concept of the prototypical disease identified by Wright [36]. As Libura and colleagues [51] argue, if the course of a given disease differs from the prototype script a regular language user (i.e., not a specialist in linguistics and/or dementia) may perceive it disrespectfully, as less threatening and urgent [51]. This conclusion is anchored in the prototype theory of Eleanor Rosch claiming that prototypes are easier to recognize and quickly processed [53]. As the current analysis showed, dementia deviates from the prototypical scenario at the level of the central elements. Due to its chronic course recovery is not possible. The treatment cluster is therefore peripheral and the process of treatment does not eliminate the disease but serve to diagnose and possibly modify the course of it. Additionally, the subject group, includes also the care cluster, indicating the chronic course of the disease and the dependence of the person with dementia on the external sources of support. Subject characteristics, behaviors, and emotions are strongly influenced by the symptoms of the disease— as if the real subjects had changed irreversibly and are no longer themselves. Also, the cause of the disease differs from the prototypical scenario— its location in the frame is peripheral as the cause is not fully recognized. These observations are consistent with the conceptual structure of the disease category conducted by Wright [36] where the dementias are located peripherally to the central concepts. Its linguistic picture is therefore similar to the non-communicable chronic diseases analyzed in Polish [51]. Conclusions drawn from that analysis suggest that diseases which differ from the prototype disease are less pronounced in popular discourse. They are less appealing to the public and therefore unattractive for the media coverage. Furthermore, regular language users can neglect its seriousness and treat as less time-critical [51]. The current results may thus reflect the belief still popular in the society that dementia is an inherent part of aging, the inevitable loss of keenness of perception and typical in old age weirdness [54]. Consequently, people with dementia can be perceived as excluded from the normal society [55]. Such socially shared beliefs form a basis for stigma and disengagement of people who are diagnosed with dementia [6, 7].
The frame of dementia depicts the general image of dementia in Polish language. In turn, filling of semantic slots of the frame by the general public, due to the Fillmore’s theory [28, 49], presumably reflects averaged resources of colloquial knowledge about dementia available to Polish speakers. The central elements identified by NKJP analysis, subject, disease, and symptoms, are present in the general public knowledge structure. The peripheral slots of each of the central categories are filled selectively so that some peripheral elements present in the otępienie frame are absent or underrepresented in the structure of the general public knowledge. Subject’s category within the common knowledge structure covers primarily subject’s characteristics and behaviors. The common picture of a person with dementia is a someone who has lost him or herself, is different than in the past, and is unable to perform actions typical for adult, and therefore as a consequence, is perceived as a big child. It is coherent with the language patterns observed also in English [56]. The dementia discourse connotates the images of non-persons or empty shells from which the disease sucked out or blanched a personhood or a being [56, 57]. These metaphorical images preserved in language were also reflected in the subject’s emotions slot. This category was underrepresented and emerging quotes depicted the inability of people with dementia to experience emotions. Analysis underlined that the stereotypical images of people with dementia are embedded in the lexical level and are part of the common knowledge in Polish. Literature suggests that a similar situation occurs also in English. Despite public efforts to build more dementia-friendly environments [21, 59], negative language patterns exist and govern common understanding of dementia [56]. This in turn has a real impact on the social reality and stigma toward people with dementia [5, 13]. This motivates endeavors to exclude the word dementia from medical communication and replace it with terms such as major neurocognitive disorder [19]. Otherwise, it prompts dementia advocacy organizations to issue language guidelines offering more respectful and non-stigmatizing language patterns when referring to dementia and people living with dementia [60–62].
Common knowledge about dementia includes also information about its most frequent symptoms, affected organ and timing. However, most of these aspects are simultaneously linked to the subject’s characteristics such as: cognitive and emotional states, expected behaviors and old age. Many responses of the participants to the question “What is dementia?” directly referred to the subject: “It is a person who . . . ”. Interpretation can be twofold. Positively, the use of the personal form shows that behind the label there is a person with some characteristics. However, it can be also attached to reversed explanation. Such profile of the general public realization of otępienie frame may be related to the current cultural conceptualization of dementia [43, 63]. During the last decades of 20th century biomedical progress has delineated the dementias as a group of pathophysiological symptoms in a brain, not a normal age-related changes and typical image of senility. Dementia started to be promoted as “a dread disease and major public health crisis in an aging world” [43]. Efforts to focus public attention on the seriousness of dementia have resulted in emphasizing the severity of the symptoms and losses suffered by the diagnosed person. Paradoxically, advocacy endeavors deepen the stigma by perpetuating in a society an image of dementia symptoms consuming the person whole, depriving the subjectivity and agency. In the presented analysis, although some of the biomedical aspects of the general public frame are well represented, the treatment cluster is slightly filled. It is in line with the observable low public awareness of possible therapeutic options and understanding that dementia is irreversible and progressive condition [22, 64].
The identification of the elements of the otępienie frame and their slot fillers among general public enabled a reference to a socio-cultural context described in existing literature on dementia, e.g., to the sociological understanding of dementia framing and cultural metaphors, to the matter of medical nomenclature used in disease classifications or to issuing linguistic guidelines that shape public debate around dementia. The interdisciplinary approach adopted in our study emphasized that the phenomenon of dementia goes beyond medicine and its analysis from different theoretical angles, including linguistics, might brought practical implications beneficial both for clinical practice and for actual life of people with dementia and their carers within the society. The presence of stigma and negative image of people with dementia rooted in language highlights the need to change the language used when talking about dementia. In the absence of effective treatment, it would be important to shift the emphasis from the biomedical context, focused on psychopathology, to the psychosocial dimension. As the evidence show, the social factors have a real positive impact on the quality of life and functioning of people with dementia [59]. Psychosocial initiatives, such as social campaigns, should therefore be aimed at changing concepts anchored in a common knowledge. The limitations and burden of the disease should be counterbalanced with the aspects resulting from the social health concept, presenting opportunities and potential for a good quality life with dementia. It will be another step towards creating an inclusive and dementia friendly society.
Our analysis provides a new perspective on studying the understanding of dementia by the public and constitute the first stage of studying semantics of dementia in the Polish language. However, several limitations need to be acknowledged. First of all, it should be noted that our analysis pertains to only one selected word (otępienie) relating to dementia used in Polish. Aside from otępienie, there are also: demencja or choroba otępienna. While the term otępienie is the name of a nosological unit, demencja or choroba otępienna are the colloquial terms. Consequently, the study of common understanding of dementia is not complete if these two concepts are not taken into account. Hence, the conclusions only apply to the word otępienie. Moreover, as this is the first study using the frame semantics theory in investigating the concept of dementia, its results must be analyzed cautiously, bearing in mind the limited number of previous research related to the topic. Limitations include also the specificity of the studied general public corpus which was small-sized and therefore its representativeness is limited. Another issue, important in psychosocial and linguistic studies, is the context [65, 66]. The current study utilized a simple elicitation method (open-ended question) in an unnatural context which could lower the ecological validity of the study [67] and did not allow for researching into discourse of dementia in Poland. The selected data collection tool could also activate social desirability bias [68] which was evident in a few responses. Some participants answered using specialized language or medical terminology, probably making use of the Internet resources, what could show the fear of giving the wrong answer and tendency to hide knowledge gaps.
Conclusions
Current research for the first time utilized the frame semantics to describe social cognition of dementia through the prism of language. The theoretical findings on the constituents of contextual knowledge underlying the image of dementia in Polish allowed to relate the semantics of dementia to clinical, social, and cultural contexts. The outlined implications for better dementia support may be convincing in broadening the interdisciplinary approach to dementia research. Further research should focus on replication of the presented analysis with the focus on other words relating to the phenomenon of dementia in Polish. Alternatively, the study can be extended with additional eliciting tasks applicable for cognitive linguistics, also allowing for investigating word’s connotations. Further studies may also include testing of other corpora such as media coverage or social media posts, as in previous research using the frame semantics [39, 44]. It would be valuable to confront the conclusions of the research on the semantics of dementia with the results of research into discourse of dementia, involving a deeper contextual analysis. It would be also beneficial to replicate the study in different language and among more diverse study groups. Followingly, cross-lingual comparisons would be valuable to establish differences between languages and assess social awareness of dementia in different regions [69].
Footnotes
ACKNOWLEDGMENTS
The research was funded by the EU Joint Programme –Neurodegenerative Disease Research (JPND) and The National Centre for Research and Development (contract no. JPND/05/2020). We would like to thank all the participants who agreed to take part in the study. We acknowledge the Consortium of the Cognisance project under which this research was performed.