
Abstract
Background:
Myeloperoxidase (MPO), a neutrophil-derived pro-inflammatory protein, co-localizes with amyloid-β (Aβ) plaques in Alzheimer’s disease (AD). Anti-dementia treatment may facilitate efflux of Aβ and associated plaque proteins from the brain to the peripheral circulation, therefore providing potential biomarkers for the monitoring of donor response to drug treatment.
Objective:
We investigated the diagnostic utility of MPO as a biomarker of AD, and how anti-dementia treatment alters plasma MPO concentration.
Methods:
Thirty-two AD patients were recruited, and plasma collected pre-drug administration (baseline), and 1- and 6-months post-treatment. All patients received cholinesterase inhibitors (ChEIs). At baseline and 6 months, patients underwent neuropsychological assessment. Forty-nine elderly healthy individuals with normal cognitive status served as controls. Plasma MPO concentration was measured by ELISA.
Results:
AD drug naïve patients had similar plasma MPO concentration to their control counterparts (p > 0.05). Baseline MPO levels positively correlated with Neuropsychiatric Inventory score (r = 0.5080; p = 0.011) and carer distress (r = 0.5022; p = 0.012). Following 1-month ChEI treatment, 84.4% of AD patients exhibited increased plasma MPO levels (p < 0.001), which decreased at 6 months (p < 0.001). MPO concentration at 1 month was greatest in AD patients whose memory deteriorated during the study period (p = 0.028), and for AD patients with deterioration in Cornell assessment score (p = 0.044).
Conclusion:
Whereas baseline MPO levels did not differentiate between healthy and AD populations, baseline MPO positively correlated with initial Neuropsychiatric Inventory evaluation. Post-treatment, transient MPO upregulation in ChEI-treated patients may reflect worse therapeutic outcome. Further studies are required to assess the potential of plasma MPO as an AD therapeutic biomarker.
INTRODUCTION
Myeloperoxidase (MPO), a myeloid specific enzyme produced and released from cells of the innate immune system during the early stages of the inflammatory response, generates free radical species that promotes oxidative damage and causes lipid peroxidation [1–3]. Oxidative damage to neurons and peroxidation of the highly polyunsaturated lipids in the post-mitotic stage of neurons also appears to be an early and crucial event in the pathophysiology and development of Alzheimer’s disease (AD) [4–6]. MPO gene polymorphisms have been associated with cognitive decline and aggravated AD development [7–10], with overexpression of MPO protein and mRNA being directly linked to both the development and progression of AD [11, 12].
MPO co-localizes with amyloid-β (Aβ) plaques and can be secreted by microglia where it can attract neutrophils to the zone of inflammation, and additionally mediate the delay of neutrophil apoptosis to prolong inflammation. In addition to its presence in Aβ plaques, the enzyme also plays a role in vascular inflammation and the progression of atherosclerosis which can contribute to the risk of development of AD [13–15]. Therefore, MPO and its derived oxidants and free radical species present potential targets for reducing the level of inflammation, and potentially reducing the risk of development of AD and slowing disease progression. Cholinesterase inhibitors (ChEIs) are the current therapeutic choice for the treatment of AD, enhancing cholinergic transmission. ChEIs can also facilitate the release of AβPP, the protein precursor of amyloid-β [16, 17], and therefore, potentially, the release of other proteins co-localizing in the Aβ plaque. Therefore, MPO may also be a useful therapeutic biomarker reflecting the level of inflammation or modifications in local inflammation in the brain in response to anti-dementia treatment. To determine whether plasma MPO levels change during the initial period of dementia treatment, this study assessed MPO concentrations in plasma from healthy elderly controls without cognitive impairment, and AD patients before and during anti-dementia treatment with ChEIs.
MATERIALS AND METHODS
Study population and design
A total of 50 patients diagnosed with AD (NINCDS/ADRDA criteria [16]) were recruited to the study, and 32 of these (53% female/47% male) completed all of the follow-up visits during the 6-month study period. The AD cohort was matched for age with 49 healthy donors (80% female/20% male) without cognitive impairment (Table 1). Exclusion criteria included the presence or history of psychosis, alcohol or drug abuse, consumption of any psychoactive or antioxidant medication, and patients with autoimmune disease. We noted 55.2% of the AD sample had hypertension, 48.3% had dyslipidemia, and 15.6% had type 2 diabetes mellitus (Table 1).
Demographic and clinical characteristics of study cohort
AD, Alzheimer’s disease; NSAID, non-steroidal anti-inflammatory drug.
On Visit 1 (baseline) all participants (AD patients and controls) completed a comprehensive clinical assessment including demographic information, clinical history, and physical and neurological examination. Standardized clinical assessments covered: neurology (Structured Neurological Examination), cognition (Cambridge Cognitive Examination which incorporates the Mini-Mental State Examination, MMSE) [18], fluctuation (One Day Fluctuation Scale and Clinician Assessment of Fluctuation) [19], mood (Cornell Depression Rating Scale) [20] and dementia-related behavioral symptoms (Neuropsychiatric Inventory, NPI) [21]. Blood was collected to establish baseline MPO levels in both groups. One month following initiation of ChEI inhibitor treatment (Visit 2), blood was collected from AD patients for MPO measurement. At 6 months of ChEI treatment (Visit 3), AD patients were re-assessed for cognitive and behavioral problems, and further blood collected for MPO analysis. The study was approved by the Local Regional Ethics Committee (13-NE-0239), and all participants gave written informed consent.
Blood collection
Venous blood samples were taken in the morning under standardized conditions and drawn into EDTA. The whole blood was centrifuged within 30 min of collection for 10 min at 12,500× g at room temperature, and the plasma transferred to a clean tube. Albumin was removed from the plasma using the protocol described by Colantonio [22], and the albumin-depleted plasma stored at –80°C until analysis.
ELISA measurement
Plasma MPO concentration was measured using a commercially available human MPO quantitative sandwich ELISA kit (cat DY3174, R&D Systems Inc, Abingdon, UK) as per the manufacturer’s instructions. Plasma from 32 AD patients was available from all 3 visits and therefore used for the study. All samples were assayed in duplicate.
Statistical analysis
Data are reported as mean±standard deviation (SD) of measurement. Continuous variables were tested for normal distribution with the D’ Agostino-Pearson test. The normally distributed data with equal variances were compared between groups using the paired t-test to analyze changes in MPO between different time points, and unpaired t test for between group comparisons. A value of p < 0.05 was considered to be significant. All data and statistical analysis were performed using Graph Pad Prism 8.0 (GraphPad Software Inc, CA, USA).
RESULTS
Analysis of baseline plasma MPO levels in study population
Controls and drug naïve AD patients had a similar range of baseline plasma MPO levels (p > 0.05, Fig. 1A). There was no association of baseline MPO levels with gender (Fig. 1B), and no statistical difference in baseline MPO levels in each age group (Fig. 1C). There was also no significant difference in baseline plasma levels of MPO between donors with hypertension, dyslipidemia, or type 2 diabetes mellitus (Fig. 1D), nor the number of cardiovascular risk factors (Fig. 1E). As expected, AD patients had significantly lower scores for MMSE (p < 0.001), CAMCOG (p < 0.001), CAMCOG memory (p < 0.001), and CAMCOG executive function (p < 0.001) (Table 2). Baseline MPO levels did positively correlate with NPI evaluation (r = 0.5080; p = 0.011) and Carer distress score (r = 0.5022; p = 0.012, Table 3).
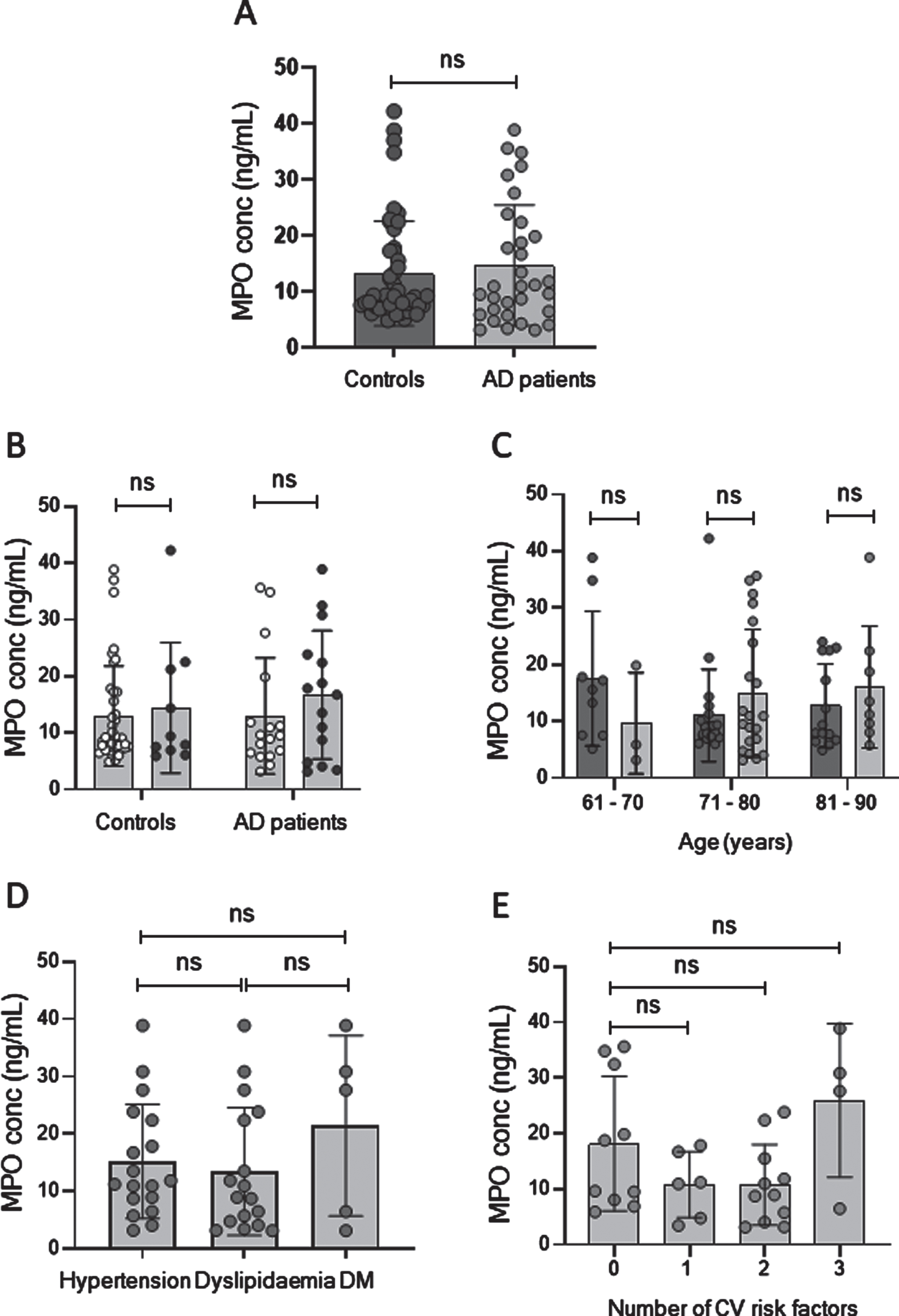
Baseline MPO concentration and initial patient characteristics. Baseline MPO concentration in A) plasma from patients with AD (light circles) and aged healthy controls (dark circles); B) plasma of controls and AD patients according to gender, female (white circles) and male (dark circles); C) plasma from controls (dark boxes) and AD patients (light boxes) according to age in decades; D) plasma MPO concentration of AD patients based on presence of individual cardiovascular risk factors; and E) plasma MPO concentration of AD patients based on donor number of cardiovascular risk factors. MPO concentration is measured in ng/mL, and data is presented as mean±SD; ns, not significant.
Cognitive, behavioral, and psychological evaluation
p-valueab derived from comparison of Control group versus Patients with Alzheimer’s disease at initial assessment (baseline). p-valuebc derived from comparison of Alzheimer’s patients at initial assessment compared to assessment score at 6 months post-drug. AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; CAMCOG, Cambridge Cognitive examination; NPI, Neuropsychiatric Inventory.
Correlation of baseline plasma MPO concentration with cognitive assessment scoring in patients with AD
AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; CAMCOG, Cambridge Cognitive examination; NPI, Neuropsychiatric Inventory. Carer distress, measured from the NPI inventory, was rated for each positive neuropsychiatric symptom domain on a scale anchored by scores from 0 to 5 points (0 = no distress; 1 = minimal distress; 2 = mild distress; 3 = moderate distress; 4 = severe distress; and 5 = very severe distress).
Effect of ChEI treatment on plasma MPO levels
Plasma levels of MPO increased in 28 of the AD patients (84.4%) at 1 month after starting cholinesterase inhibitor treatment (p < 0.001) and decreased (p < 0.05) to below baseline levels (p < 0.001) by 6 months (Fig. 2A). However, analysis of dot plots of individual donor response showed that in samples from 5 AD patients, changes in plasma MPO levels did not follow the same pattern; instead MPO levels were either reduced at 1 month and 6 months without any obvious rapid increase post initial drug treatment (n = 3; Fig. 2B), or MPO levels were similar to baseline at 1 month but were increased by 6 months (n = 2); Fig. 2C). Excluding these donors from further analysis, the mean fold change in MPO levels was 4.3-fold increase (baseline to 1 month) and 4.8-fold decrease (1 month to 6 months post-drug treatment); however, the amplitude of fold change in plasma for individual donors was variable.
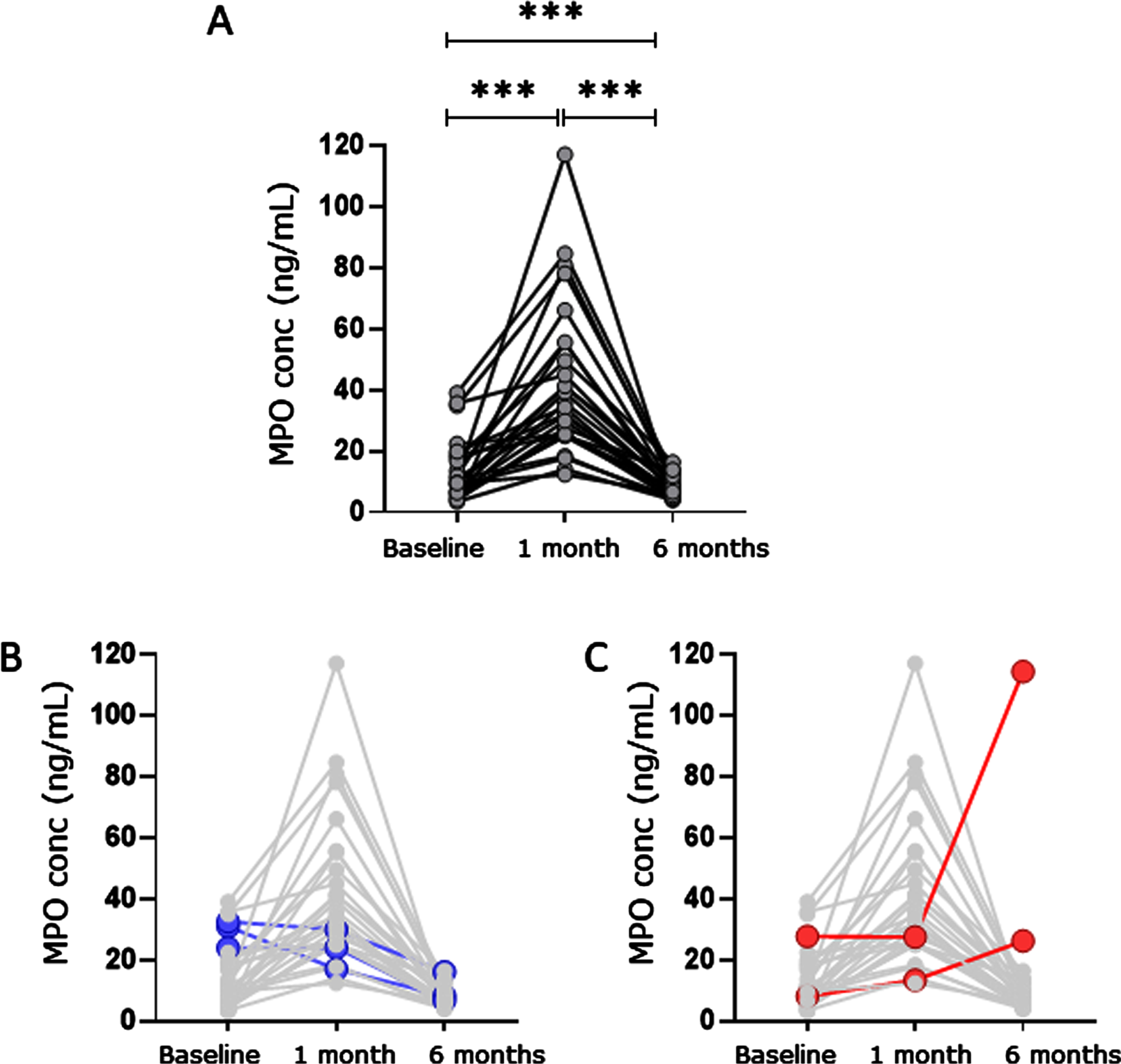
Effect of cholinesterase inhibitors on plasma myeloperoxidase concentration. A) Changes in MPO concentration (ng/mL) in plasma collected from AD patients at baseline (pre-drug treatment), and at one month and 6 months post starting antidementia treatment (n = 27). Data shows MPO levels for individual donors; p < 0.001***. B, C) Highlight plasma MPO concentrations from individual donors where changes in MPO did not follow the majority pattern of response.
Fluctuations in plasma MPO level and relationship to cognitive decline
Neuropsychological assessment at 6-months post-cholinesterase inhibitor treatment showed a significant level of cognitive decline in CAMCOG score in the AD patient population (Table 2). When comparing fluctuations in plasma MPO levels with or without cognitive and psychological decline, MPO concentration at 1 month was significantly elevated in AD patients measuring decline in assessment scores for CAMCOG-Memory (mean 53.0±30.1 and 31.5±13.6 ng/mL for AD patients showing decline and no decline, respectively; p < 0.028) and Cornell Depression assessment (53.42±29.2 and 33.9±18.6 ng/mL; p < 0.044) during the period of the study (Fig. 3A, B). The amplitude of increase of MPO levels at 1 month was significantly higher in AD patients with increased number of CV risk factors (Fig. 3C), and these individuals also had the greatest level of decline in CAMCOG_Memory measures (Fig. 3D). Finally, the fold increase in MPO levels between baseline and 1 month was positively correlated with diastolic (r = 0.5961; p = 0.002), but not systolic, blood pressure (Fig. 3E, F).
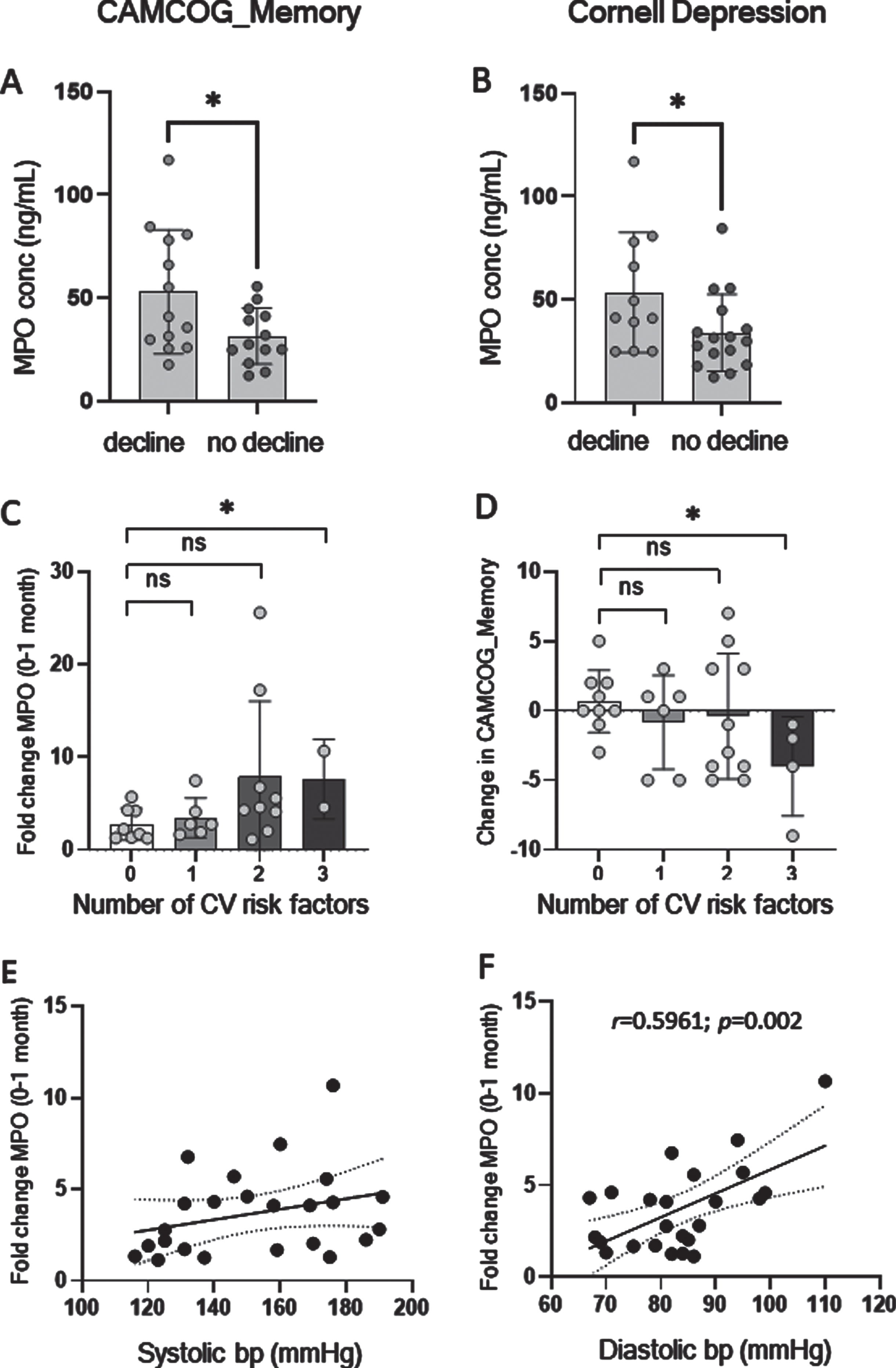
Fluctuation in MPO levels and cognitive decline. Plasma MPO concentration (ng/mL) at one-month post-antidementia treatment in AD patients stratified by change in A) CAMCOG_Memory assessment and B) Cornell Depression Rating Scale assessment score during the 6 months of the study; (light circles represent patients with decline, and dark circles represent AD patients with no decline). C) Fold change in MPO concentration between plasma from baseline and one-month post-drug treatment in donors with increasing number of cardiovascular risk factors. D) Change in CAMCOG_Memory assessment score in relation to number of cardiovascular risk factors. Data in figures A–D is presented as mean±SD; p < 0.05*, ns, not significant. Fold change in MPO concentration between plasma from baseline and one-month post-drug treatment in relation to E) systolic blood pressure, and F) diastolic blood pressure (mmHg).
DISCUSSION
The more invasive measurement of biomarkers in CSF [23–25] and neuroimaging are used routinely in the diagnosis and classification of dementia, and in monitoring disease progression. However, the measurement of proteins in peripheral blood is a less invasive option and offers the potential for screening a panel of biomarkers in a short timeframe. Previous studies of neutrophil-associated proteins in AD have suggested that peripheral blood of AD patients contains higher concentrations of these pro-inflammatory proteins than CSF [26]. Therefore, more studies which include measurement of MPO and other pro-inflammatory proteins in blood are required to assess their potential as disease biomarkers.
This study assessed the potential utility of the neutrophil-associated protein MPO as a diagnostic and/or therapeutic marker in AD. Whereas MPO levels have previously been reported to be higher in plasma from AD patients compared to healthy controls [27], we found no significant difference in baseline MPO plasma levels of drug naïve AD patients and those of the healthy, aged controls. Our assays were performed using albumin-depleted plasma and in drug naïve patients, avoiding the potential bias arising from altered MPO measures due to plasma protein binding (EML, unpublished). Similarly, MPO activity has been reported to be altered in patients with diabetes, and due to statins treatments [28], thus higher prevalence of these conditions in AD subjects could have had an impact on the reported findings in previous studies. Whereas there was no correlation of baseline MPO levels with age, gender, or specific cardiovascular risk factors, AD patients who had higher NPI assessment scores also had elevated levels of baseline MPO, and this was reflected in the positive correlation of MPO levels and carer distress score. Therefore, although our findings suggest that measurement of plasma MPO levels may not aid the differentiation between healthy elderly individuals and AD, plasma MPO levels may reflect the level of accumulation of pro-inflammatory proteins which in turn may be facilitating AD non-cognitive changes.
A recent study investigating the use of Anserine, a scavenger of hypochlorous acid which is produced as a result of MPO-mediated inflammatory response, found that the drug protected against further cognitive decline in an elderly population with mild cognitive impairment [29], therefore developing therapeutic targets of MPO may be important. In addition, we need to further understand how different drugs may affect plasma MPO levels and how this relates to cognitive decline or stability. This is the first study to measure plasma MPO levels at different time points after starting ChEI treatment, revealing that in 84% of the patients there was a significant transitory increase in plasma MPO levels at one month, which had decreased to baseline or below baseline levels by 6 months of treatment. The frontal cortex of AD patients has been reported to have an increased presence of MPO-positive cells, and MPO concentration is high in extracellular plaques where it can co-localize with Aβ [3]. ChEIs can facilitate the release of AβPP [16, 17] and affect the AD amyloidogenic pathway via the activation of the phosphoinositide 3 kinase (PI3K)/Akt pathway, inhibition of glycogen synthase kinase-3, and the activation of nicotinic acetylcholine receptors (reviewed in [30]). MPO, therefore, may be released into the bloodstream alongside other extracellular plaque proteins, resulting in a transient increase of MPO into the peripheral circulation until either the build-up of pro-inflammatory proteins in the brain ceases, or the drug becomes ineffective, for example due to depletion of drug target. Alternatively, MPO may be induced by ChEI treatment, since the cytokine system is affected by ChEI treatment [30].
In this study, AD patients that demonstrated cognitive and behavioral decline over the 6-month study period, as assessed by CAMCOG-memory and Cornell assessments, had significantly higher MPO levels at 1 month than for AD patients with no decline for these parameters. Since there is a close relationship of cognitive decline with the neurofibrillary pathology, but not the extent of extracellular amyloid deposits [31], ChEI activity may have only a brief period of being neurobiologically effective, targeting the AD-accompanying inflammation associated with Aβ deposits [2], but not the intraneuronal MPO activity. This opens the possibility that the enzyme continues to contribute to the cumulative oxidative stress promoting neurofibrillary pathology and neuronal cell death in AD.
AD pathology contributes to cardiovascular disease via Aβ accumulation resulting in cardiac dysfunction due to thickening of the left ventricle wall in AD patients [32]. Conversely, the development and progression of late onset AD has been linked to metabolic and cardiovascular risk factors [33], whereby the presence of cardiovascular risk factors including diabetes, hypertension, and dyslipidemia [34-38] may facilitate AD onset and progression [39]. Similarly, in our study AD patients with an increased number of cardiovascular risk factors had the greatest decline in memory during the study period. In support of this, we report that the amplitude of increase in MPO levels after 1 month of ChEI treatment was positively correlated with diastolic blood pressure. In a neuroradiological study on ageing, higher diastolic blood pressure has been related to biomarkers of both cerebrovascular (white matter hyperintensity) and AD (smaller hippocampi) dementias [40], and Aβ brain burden measured by Pittsburgh Compound B-positron emission tomography (PiB-PET) studies [41]. This brings together again MPO and Aβ processing in AD and highlights the need to develop reliable peripheral biomarkers for the screening for AD in at-risk populations.
Not all AD patients showed the same pattern of change in plasma MPO levels during the course of ChEIs treatment. Three AD patients had no increase at one month, followed by further decrease at 6 months, and 2 AD patients showed little or no change at one month but increased MPO levels by 6 months. In the case of the latter pattern, the increase MPO levels at 6 months perhaps suggests a slower response in these individuals to ChEIs, whereas those who showed no increase in MPO levels may either have no response to ChEI treatment, or alternatively, have a rapid response to ChEIs that has been missed by the sample collection time-points included in this study. This is the first study to investigate the effect of ChEIs on plasma MPO levels, and more studies are now required that include intermediate sample collection points to facilitate analysis and interpretation of the relevance of changing MPO levels and other biomarker candidates, during therapeutic treatment of AD, and for the monitoring of populations at risk of developing AD. The heterogeneity in donor response may be due to a multitude of factors, including the type of ChEI and dosage used, and therefore the potential of MPO as a therapeutic biomarker during antidementia treatment warrants further investigation to determine any potential diversity in AD clinical phenotypes that may facilitate clinical management of these patients. These findings alongside with correlative neuroradiological studies (i.e., MRI, amyloid and tau tracer PET studies) will help change both the diagnosis and management of AD.