
Abstract
Background:
The detrimental impact of tobacco smoking on brain health is well recognized.
Objective:
To evaluate whether smoking acts synergistically with hypertension and diabetes to influence cognitive performance.
Methods:
We performed a cross-sectional analysis using the US National Health and Nutrition Examination Survey. Participants were tested for serum cotinine, a validated cigarette smoking/exposure biomarker, and had standardized blood pressure and hemoglobin A1c measurements. Participants were administered four cognitive tests: Digit Symbol Substitution (DSST), Animal Fluency, Immediate Recall, and Delayed Recall. Multivariable linear regression models adjusted for demographics and confounders evaluated the association of cotinine with cognition. Interaction testing evaluated effect modification by hypertension, diabetes, and their continuous measures (systolic blood pressure and hemoglobin A1c).
Results:
For 3,007 participants, mean age was 69.4 years; 54% were women. Using cotinine levels, 14.9% of participants were categorized as active smokers. Higher cotinine levels were associated with worse DSST performance when modeling cotinine as a continuous variable (β, -0.70; 95% CI, -1.11, -0.29; p < 0.01) and when categorizing participants as active smokers (β, -5.63; 95% CI, -9.70, -1.56; p < 0.01). Cotinine was not associated with fluency or memory. Effect modification by hypertension and diabetes were absent, except that cotinine was associated with worse Immediate Recall at lower blood pressures.
Conclusion:
Higher levels of a smoking and secondhand exposure biomarker were associated with worse cognitive performance on a multidomain test. Overall, the relationship of cotinine with cognition was not contingent on or amplified by hypertension or diabetes; smoking is detrimental for brain health irrespective of these comorbidities.
INTRODUCTION
There are over 50 million people worldwide with dementia, and mild cognitive impairment impacts approximately 6–12% of the world’s population [1, 2]. Cognitive impairment and dementia are age-related conditions, with the risk of these conditions increasing dramatically after the age of 65 [3, 4]. A better understanding of modifiable risk factors for cognitive decline and dementia among at-risk individuals is thus critical from a public health perspective. Active cigarette smoking is a common lifestyle risk factor for cognitive decline and dementia among older adults [5, 6]. Secondhand exposure to cigarette smoking has a similarly detrimental impact on brain health [7–10]. Hypertension and diabetes are additional common comorbidities with known associations with cognitive decline and dementia [11]. Prior work has shown that smoking acts synergistically with genetic risk factors (Apolipoprotein E4) with respect to dementia risk [12]. Additionally, smoking acts synergistically with vascular risk factors such as diabetes and hypertension with respect to brain health outcomes, such as carotid atherosclerosis and white matter hyperintensity volume burden [13, 14]. While it is known that smoking, hypertension, and diabetes each negatively impact brain health, whether smoking acts synergistically with hypertension or diabetes to contribute to cognitive performance at the population level is less clear. Uncovering synergistic relationships may help identify high-risk individuals and inform efforts to target preventive interventions to such individuals. Therefore, in this study, we sought to evaluate the association of tobacco smoking and secondhand exposure, assessed biochemically based on serum cotinine levels, with cognitive function in a nationally representative sample of older Americans, while specifically testing for synergistic effects with hypertension and diabetes.
METHODS
Data source and study design
We performed a cross-sectional analysis using data from the National Health and Nutrition Examination Survey (NHANES) from 2011 through 2014. NHANES is a nationally representative health survey conducted by the US National Center for Health Statistics, Centers for Disease Control and Prevention [15]. NHANES participants undergo standardized interviews, physical examinations, and biological specimen collection in mobile examination centers. We utilized the 2011-2012 and 2013-2014 NHANES survey cycles as these are the most recent cycles that included standardized, objective cognitive assessments. NHANES data collection was approved by the National Center for Health Statistics Research Ethics Review Board. Each NHANES participant provided written informed consent. NHANES data are deidentified and publicly available on the Centers for Disease Control website. Analysis of these deidentified data was deemed exempt from review by the Weill Cornell institutional review board.
Participants
NHANES performed cognitive testing only for adults ≥60 years old given the increased prevalence of cognitive dysfunction in this age group. Therefore, our study population consists of adults ages 60 years and older who participated in NHANES between 2011-2014. We excluded participants with missing serum cotinine data, and participants with incomplete or missing data for all four cognitive tests (Fig. 1). NHANES excluded participants from cognitive testing who were unable to be tested in the available six languages, declined audio recording necessary for test scoring, faced technical difficulties, refused testing, or did not understand test instructions. Additionally, NHANES did not collect laboratory data from participants with hemophilia and chemotherapy in the past 4 weeks due to theoretical risks related to phlebotomy. A full description of laboratory methods may be found in the NHANES manual [15].
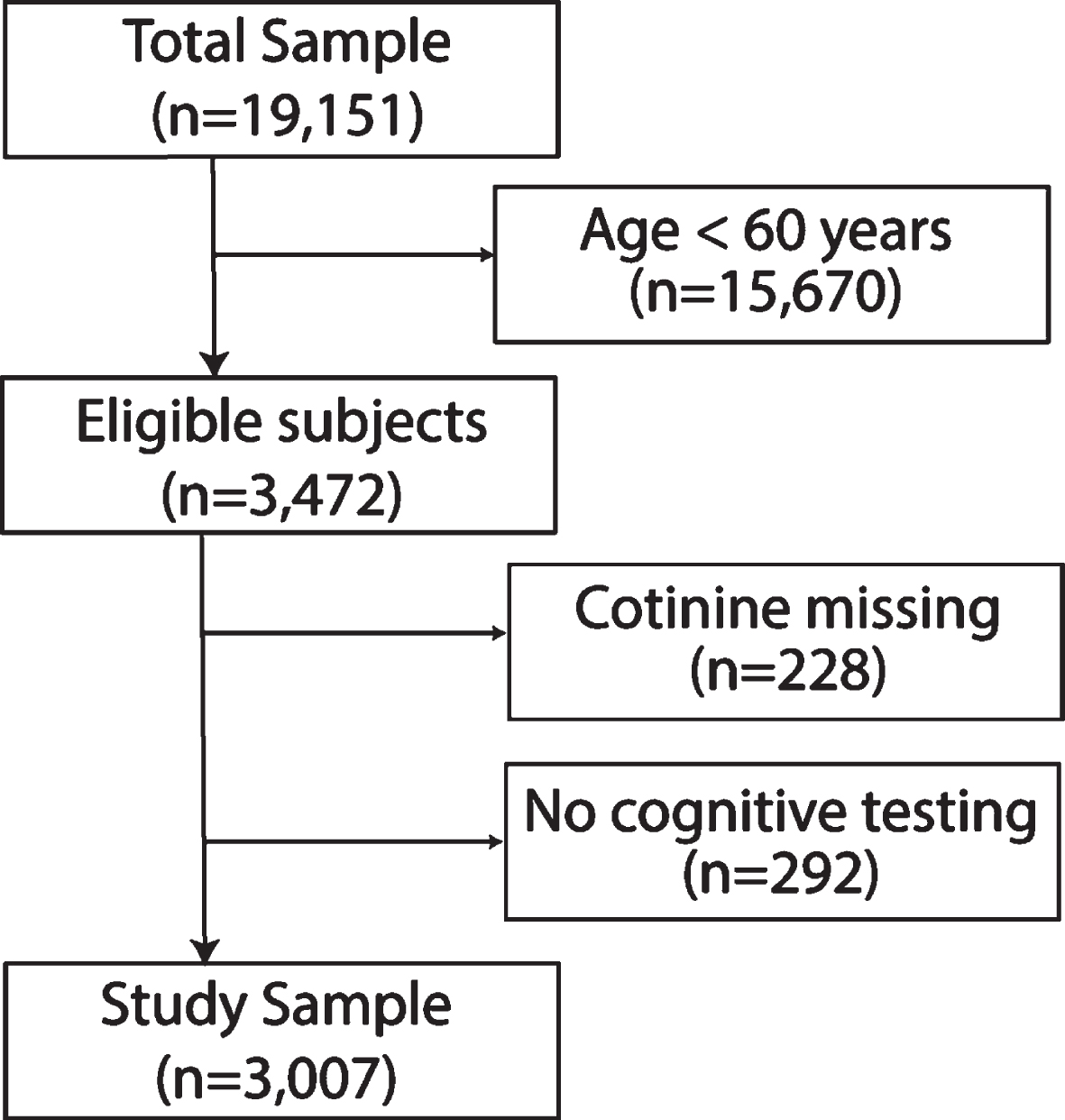
Patient selection diagram. We included participants > 60 years of age who had available serum cotinine levels and at least one complete cognitive test. Some individuals had multiple reasons for exclusion.
Measurements
Our primary exposure of interest was serum cotinine. Serum cotinine is a nicotine metabolite with an approximately 16 h half-life in the general population, and is used to estimate exposure to first and secondhand tobacco smoke [16]. It is a well-validated biochemical biomarker for smoking that circumvents limitations related to self-reported smoking status. Serum cotinine levels are measured using a standardized, quality-checked laboratory protocol in NHANES [17]. In our primary approach, we used serum cotinine as a continuous independent variable, natural log transformed due to its skewed distribution, as a quantitative measure of tobacco smoking and exposure. In the primary approach, we used serum cotinine as a continuous measure, allowing it to reflect both active smoking and secondhand exposure. However, in a secondary approach, we categorized participants as active smoker versus not active smoker using a serum cotinine cut-off specifically validated for the purposes of classifying individuals by smoking status: ≥3.30 nanograms per milliliter (smoker) versus < 3.30 (nonsmoker) [18]. The sensitivity and specificity of these thresholds for smoking status is > 95% [18].
Additional key exposures were hypertension and diabetes. Participants were classified as having hypertension if they self-reported a diagnosis of hypertension, were on anti-hypertensive medications, or had a mean measured blood pressure > 130/90. Participants were classified as having diabetes if they self-reported a diagnosis of diabetes, were on diabetic medications, or had a hemoglobin A1c (HbA1c) ≥6.5%. We additionally evaluated mean systolic blood pressure and HbA1c as continuous variables. In NHANES, blood pressure readings were collected in three consecutive measurements after having the participant rest quietly in a seated position for five minutes. HbA1c was measured using chromatography; a full description of these methods may be found in the NHANES Laboratory Procedure Manual [19].
The outcome measures were performance on the four NHANES cognitive tests: Digit Symbol Substitution test (DSST), Animal Fluency test (AFT), and Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) 10-item word list learning with both Immediate Recall Test and Delayed Recall Test. The DSST, a multidomain test that measures attention and processing speed, was specified as the primary outcome in our analysis because this test is sensitive to impairment regardless of origin [9, 20]. The AFT assesses semantic verbal fluency by asking participants to name as many animals as possible over one minute. The CERAD 10-word list measures immediate and delayed recall by having a participant repeat a 10-word list immediately after reading the list and then after completing intervening tests (AFT and DSST) [21]. These tests have had their validity established in epidemiological studies [22–24]. Tests were administered by trained examiners onboard the NHANES mobile examination center on a computer in participants’ preferred language.
We tabulated the following covariates. Demographic variables included age, gender, self-reported race/ethnicity, health insurance type, poverty, and educational attainment. Health insurance was grouped by uninsured, Medicaid, Medicare, private insurance, or other. Poverty was defined as a ratio of family income to local poverty threshold of < 1. Educational attainment was categorized as ≤12th grade education versus any college education or more. Medical comorbidities, in addition to diabetes and hypertension, were hyperlipidemia, heavy alcohol use, and depression. Hyperlipidemia was defined as total serum cholesterol ≥240 mg/dl or use of cholesterol-lowering medications. Heavy alcohol use was defined as ≥8 and ≥15 drinks per week for women and men, respectively. Depression was assessed by the Patient Health Questionnaire-9 (PHQ-9), which is a depression screening tool that generates scores ranging from 0 to 27 based on participants’ responses to questions regarding depression symptoms over the past two weeks. We categorized participants as having depression if their PHQ-9 scores were ≥10 at the time of the survey, which is a validated cut-off [25, 26].
Statistical analyses
We used linear regression to evaluate the association of serum cotinine levels with cognitive performance. Three models were created: 1) unadjusted for covariates; 2) adjusted for age, sex, race/ethnicity, poverty, health insurance, and educational attainment; 3) additionally adjusted for hypertension, diabetes, hyperlipidemia, alcohol overuse, and depression. We then evaluated whether the association of smoking with cognitive test performance is modified by hypertension or diabetes. To do this, the Wald test was used to calculate 2-sided p values for interaction terms for cotinine (and, separately, active smoking) X systolic blood pressure and hemoglobin A1c as continuous measures, and hypertension and diabetes as categorical variables. Where an interaction was identified based on the presence of a significant interaction (p < 0.05), stratified analyses were performed to evaluate the association of smoking with cognition among subgroups, and interactions were visualized to demonstrate heterogeneity of effect. The threshold for statistical significance was α=0.05. Survey procedures were used for all statistical analyses to account for the survey nature of NHANES data. Analyses were preformed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Among 3,007 participants, the mean age of our sample was 69.4 years (SD, 6.8), and 54% were women. Based on serum cotinine levels, 14.9% of participants were categorized as active tobacco smokers, whereas 11.3% self-reported active tobacco smoking. Overall, 50.2% reported having been smokers at some point in their lives. In addition, 77% had hypertension and 24% had diabetes. Individuals with biochemical evidence of active smoking were less likely to be female, have private insurance, or attend college; they were also more likely to overuse alcohol compared to non-smokers (Table 1). Active smokers had similar blood pressure (134 mmHg versus 133 mmHg; p = 0.32) and hemoglobin A1c (6.1% versus 6.1%, p = 0.13) when compared to non-smokers.
Study sample characteristics, stratified by biochemically defined active smoking status
NHANES, National Health and Nutrition Examination Survey; CI, confidence interval; HbA1c, hemoglobin A1c. Data are presented as percentage (95% confidence interval of percentage) unless otherwise specified. Percentages for any given characteristic may not sum to 100% because figures reflect weighted estimates. *Participants with both private insurance and Medicare were categorized as having private insurance. Those with both Medicare and Medicaid were categorized as having Medicare.
Higher levels of serum cotinine were associated with statistically significant worse performance on the DSST across all linear regression models including the most adjusted model (β, -0.70; 95% CI, -1.11, -0.29; p < 0.01). Compared to non-smokers, active smokers as defined by serum cotinine cut-offs, had worse performance on the DSST across all linear regression models including the most adjusted model (β, -5.63; 95% CI, -9.70, -1.56; p < 0.01). Serum cotinine levels were not associated with performance on AFT, Immediate Recall, and Delayed Recall (Table 2).
Associations between serum cotinine levels and cognitive measures in older adults, NHANES 2011-2014
NHANES, National Health and Nutrition Examination Survey; CI, confidence interval. †Multivariable linear regression for survey data used to evaluate the association between the serum cotinine and cognitive measures; associations reported as β, 95% confidence interval of β, and p value. In the primary approach, serum cotinine was log transformed and used as a continuous variable. In the secondary approach, participants were categorized based on validated serum cotinine cut-offs. Model 1 was unadjusted. Model 2 adjusted for demographics (age, sex, race, poverty, health insurance, and educational attainment). Model 3 was additionally adjusted for hypertension, diabetes, hyperlipidemia, alcohol overuse, and depression.
As expected, hypertension and diabetes were generally associated with worse cognitive performance. In the most adjusted models used to evaluate the impact of serum cotinine on cognitive test performance, hypertension was non-significantly associated with worse performance on the DSST (β, -1.74; 95% CI, -3.50, 0.01; p = 0.054) and worse performance on the AFT (β, -1.32; 95% CI, -2.13, -0.51; p < 0.01 and Immediate Recall (β, -0.83; 95% CI, -1.61, -0.06; p = 0.04), but not Delayed Recall (-0.29; 95% CI, -0.67, 0.10; p = 0.14). Similar patterns, consistent in direction but not statistically significant for DSST, were seen for each 1 mmHg increase in systolic blood pressure when this continuous variable was substituted for hypertension: DSST (β, -0.02; 95% CI, -0.07, 0.02; p = 0.31), AFT (β, -0.02; 95% CI, -0.03, -0.003; p = 0.02), Immediate Recall (β, -0.02; 95% CI, -0.04, -0.01; p = 0.01), Delayed Recall (β, -0.01; 95% CI, -0.01, -0.001; p = 0.02). Diabetes was also associated with worse performance on the DSST (β, -3.98; 95% CI, -5.80, -2.15; p < 0.01), and Delayed Recall (-0.33; 95% CI, -0.64, -0.01; p = 0.04), but not AFT (β, -0.54; 95% CI, -1.51, 0.43; p = 0.27) or Immediate Recall (β, -0.46; 95% CI, -1.06, 0.14; p = 0.13). Similar patterns in terms of direction of effect, again not all statistically significant, were seen for each 1.0% increase in Hemoglobin A1c: DSST (β, -1.60; 95% CI, -2.34, -0.85; p < 0.01), AFT (β, -0.44; 95% CI, -0.83, -0.06; p = 0.02), Immediate Recall (β, -0.27; 95% CI, 0.60, 0.07; p = 0.11), Delayed Recall (β, -0.20; 95% CI, -0.36, -0.03; p = 0.02).
We then tested whether the relationship between smoking and cognition is modified by hypertension and diabetes. A statistically significant interaction was observed for systolic blood pressure with serum cotinine (p = 0.01 for interaction) and with active smoking (p = 0.03 for interaction) for Immediate Recall. We visualized this interaction by plotting the slope of the association of cotinine with Immediate Recall along a range of systolic blood pressures, showing that the association of cotinine level with worse Immediate Recall was absent at higher blood pressure (Fig. 2). However, this interaction was not observed for hypertension as a categorical variable; when simply stratifying by hypertension status, the association of cotinine with immediate recall was similar among hypertensives (β, -0.08; 95% CI, -0.19, 0.03; p = 0.13) versus not (β, -0.09; 95% CI, -0.29, 0.11; p = 0.37). There were no other statistically significant interactions for DSST, AFT, or Delayed Recall with systolic blood pressure, hypertension, diabetes, or hemoglobin A1c (Table 3).
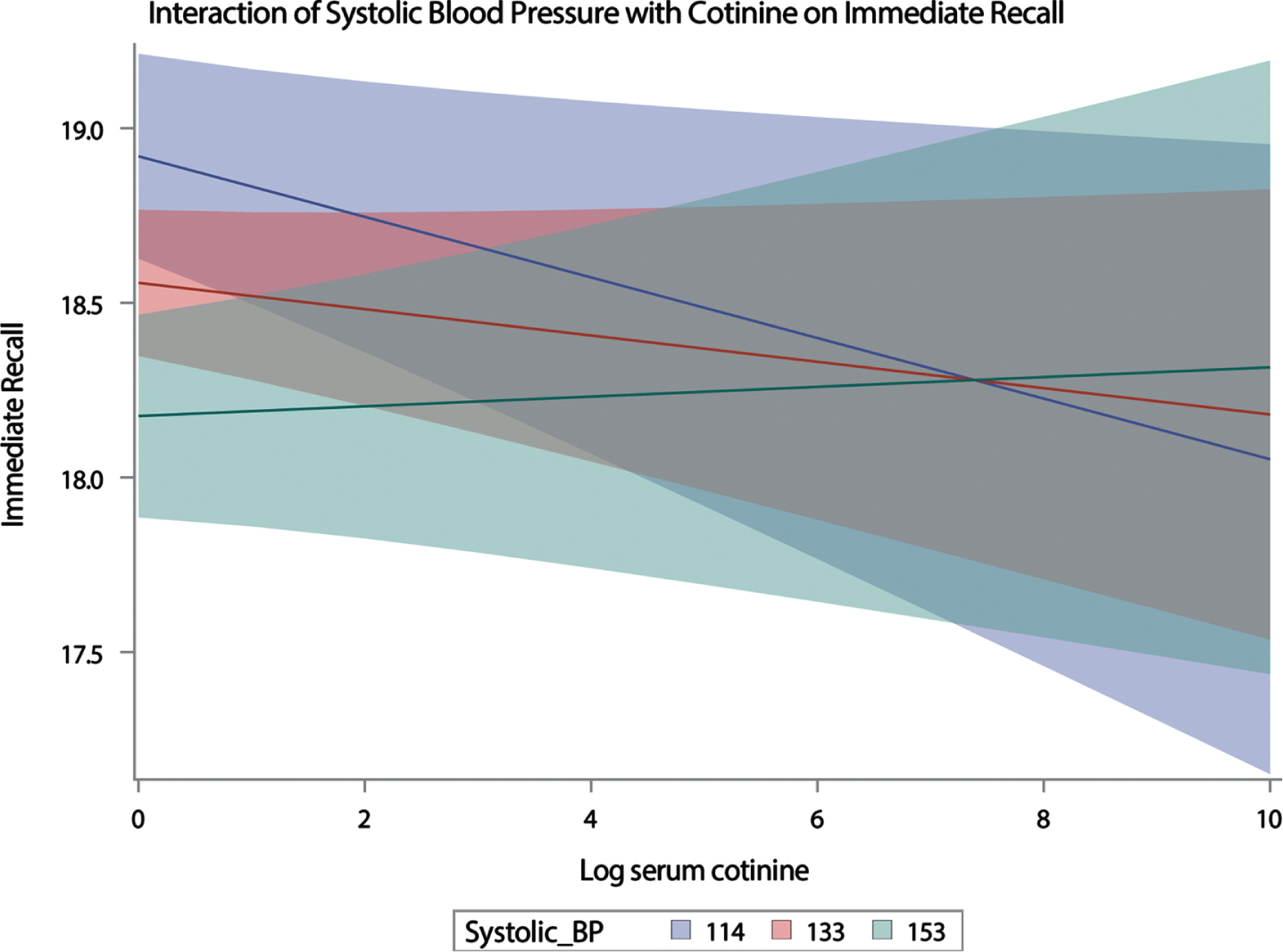
Interaction of systolic blood pressure with cotinine on immediate recall. We visualized the association of serum cotinine with performance on a test of immediate recall. Higher cotinine levels appeared to be associated with worse performance on immediate recall testing for participants with low (114 mmHg; 1 standard deviation below mean) and average (133 mmHg) but not high (153 mmHg; 1 standard deviation above mean) systolic blood pressure.
Interaction term testing to determine effect modification on cognitive test performance by hypertension and diabetes
A1c, Hemoglobin A1c (%). Interaction term testing was used to determine whether hypertension, systolic blood pressure, diabetes, and hemoglobin A1c modified the association of serum cotinine with performance on the Digit Symbol Substitution Test. In the primary approach, serum cotinine was log transformed and modeled as a continuous variable. In the secondary approach, participants were categorized as active smoker versus not based on validated serum cotinine cut-offs. All models were also adjusted for demographics and potential confounders (Model 2 as defined in manuscript).
DISCUSSION
In this analysis of nationally representative data for older Americans, we found that a biomarker of active smoking and secondhand exposure was associated with worse performance on the DSST, which is a multidomain cognitive test. Higher levels of serum cotinine were not associated with worse performance on tests of fluency or memory. We found that the detrimental impact of cigarette smoking on DSST performance is not contingent on the presence of hypertension or diabetes, two conditions strongly linked with worse cognition. Rather, interaction testing revealed that serum cotinine’s relationship with Immediate Recall test performance may be present in those with low-normal blood pressure.
The harmful impact of vascular risk factors, including cigarette smoking, hypertension, and diabetes, on brain health is well established [11]. In fact, 14% of dementia worldwide is attributable to cigarette smoking [2]. Our findings make two important contributions to the extant literature. First, we demonstrated in noninstitutionalized older Americans that cigarette smoking, confirmed biochemically, is associated with worse cognitive performance in an age range that imparts vulnerability to cognitive impairment and dementia. Second, the availability of standardized blood pressure measurements and hemoglobin A1c testing allowed us to explore complex interactions between cigarette smoking, hypertension, and diabetes. In doing so, we found that the impact of cigarette smoking on DSST performance was not modified by hypertension, diabetes, or their more direct measures. For the only test for which an interaction was observed— the Immediate Recall test— we found that cotinine appeared associated with worse performance in those with lower blood pressure. This suggests that individuals not otherwise susceptible to cognitive impairment due to hypertension may nonetheless be vulnerable to the effects of smoking.
These findings suggest that promoting smoking cessation may be one method for preserving cognitive health at the population level, independent of diabetes and hypertension status. Smoking cessation in middle-age and older adults has been shown to reduce the development of cognitive dysfunction [27–31]. This highlights the importance of smoking cessation across all stages of adulthood, even in late adulthood. Yet, older adults who smoke tend to smoke more than younger counterparts and are less likely to make smoking cessation efforts due to increased duration of cigarette dependency, denial that smoking is associated with poor health outcomes, or beliefs that smoking cessation will not lead to improved health [32, 33]. Despite this, smoking cessation interventions targeting older adults are lacking [33]. Additionally, effective smoking cessation pharmacotherapy are less likely to be used in older adults [34]. This is due, at least in part, to the lack of inclusion of older adults in studies of effective smoking cessation pharmacotherapy [35]. Our findings underscore the importance of developing and implementing effective smoking-cessation interventions in older adults. The association of smoking on DSST performance was found in models adjusted for alcohol overuse. However, given the higher prevalence of alcohol overuse, a known risk factor for cognitive impairment [36], in smokers in our sample, smoking cessation interventions may also need to address concomitant alcohol overuse.
Strengths of this study include the utilization of nationally representative health survey data replete with a serum biomarker of cigarette smoke exposure, which mitigates issues of misreported smoking status, for example due to social desirability bias. An additional strength of the study is the availability of detailed covariates that help account for measured confounding. However, the findings of this study should be considered in light of its limitations. First, the cross-sectional study design precludes causal linkage of smoking with poor cognitive function. Second, the cross-sectional study design of this study does not allow us to understand how exposure to cigarette smoke affects cognitive function over time. Third, in our secondary analysis we categorized individuals as smokers and nonsmokers. While the cut-off we used to categorize participants has been validated specifically for this purpose, it is possible that some individuals with very high secondhand exposure had cotinine levels exceeding the cut-off and were thus misclassified as smokers. However, we expect this to be rare given the relatively high cut-off threshold, and this limitation does not materially detract from our overall finding regarding the relationship of serum cotinine, however modeled, and cognitive performance. Finally, as serum cotinine was only measured at one point in time, cumulative smoking exposure is not reflected in our findings.
Conclusions
Higher levels of a biomarker of smoking and secondhand exposure were associated with worse cognitive performance on a multidomain cognitive test at the population level, regardless of hypertension or diabetes status. These data suggest an independent negative impact of cigarette smoking and secondhand exposure on cognition and underscore the broad importance of promoting smoking cessation in public health efforts to preserve cognitive health.