
Abstract
Background:
Lewy body dementia is the second most common neurodegenerative dementia, but data concerning the onset age and clinical features in the prodromal stage remain limited in China.
Objective:
To investigate the associations between onset age and clinical manifestations of cognitive impairment with Lewy bodies in a large-sample cohort.
Methods:
We included 74 patients with mild cognitive impairment with Lewy bodies (MCI-LB), 533 patients with dementia with Lewy bodies (DLB), 118 patients with Parkinson’s disease with MCI (PD-MCI), and 313 patients with Parkinson’s disease dementia (PDD) in this multicenter cohort from 22 memory clinics of China from 1 January 2018 to 31 March 2022. The onset age, clinical manifestations, and neuropsychological assessments were recorded and analyzed after reviewing the medical records.
Results:
The average onset age of memory loss was 68.28 (±7.00) years, and parkinsonism happened 2.00 (±1.24) years later for patients with MCI-LB. The average onset age of parkinsonism was 60.56 (±8.96) years, and the memory loss happened 3.49 (±3.02) years later for patients with PD-MCI. Rapid eye movement sleep behavior disorder and visual hallucinations were frequently reported in MCI-LB, DLB, and PDD, while visual hallucinations were least frequently reported in PD-MCI. Lower scores of MMSE and depression, and higher scores of activities of daily living and delusions, were independently associated with older onset age in DLB.
Conclusion:
The onset of PD-MCI precedes MCI-LB, and memory loss occurs 3 years after parkinsonism. The onset age is associated with cognition and neuropsychiatric symptoms in process.
INTRODUCTION
Lewy body disease is a neurodegenerative disease associated with alpha-synuclein aggregations, and cognitive impairment represents an important component of the clinical syndromes. Cognitive impairment with Lewy bodies includes mild cognitive impairment Lewy bodies (MCI-LB), dementia with Lewy bodies (DLB), Parkinson’s disease with mild cognitive impairment (PD-MCI), and Parkinson’s disease with dementia (PDD), which are characterized by a tetrad of visual hallucinations (VH), fluctuations in cognition, spontaneous parkinsonism, and rapid eye movement sleep behavior disorder (RBD) [1]. Despite considerable clinical overlap, their diagnosis is based on an arbitrary distinction between the time of onset of parkinsonism and cognitive impairment: cognitive impairment often preceding parkinsonism in MCI-LB and DLB, but with onset of cognitive impairment after onset of parkinsonism in PD-MCI and PDD [1, 2].
Although the main criterion for DLB and PDD is still the “one-year rule,” some clinical features might be useful for differential diagnoses. The average onset age of Lewy body dementia (LBD), consisting of DLB and PDD, is 68–81 years [3, 4], with men predominant over women [4, 5]. Cognitive impairments in PDD are similar generally but there is existing heterogeneity with those in DLB, and attentional fluctuations and hallucinations are more frequent in DLB [6]. The earlier onset of visual hallucinations is associated with limbic pathology [7] and seems to be a possible predictor for disease course, motor and non-motor function [8]. Features of RBD and spontaneous parkinsonian, such as bradykinesia and rigidity albeit not rest tremor, are common in both entities, eventually occurring in over 80% [9, 10]. The older onset age at parkinsonism contributes to more sensory and autonomic symptoms, sleep disorders, dementia, and psychosis [8]. Although much preceding work has been done on MCI as related to Alzheimer’s disease (AD), the prodromal stage as specifically designated in LBD has only recently emerged, with diagnostic criteria recently proposed [2]. Several studies with small samples [11–13] demonstrated inconsistent findings in MCI-LB and PD-MCI. There remain many unanswered questions regarding PD-MCI and MCI-LB, and their clinical features are still unclear. In addition, there is still a lack of Chinese data.
In this article, we provide a multicenter study to describe the onset age of parkinsonism and memory loss, the gap years between them and the frequency and combination of core clinical features in MCI-LB, DLB, PD-MCI and PDD. Moreover, we examine the associations between onset age and clinical manifestations in a large-sample cohort. A better understanding of the clinical features in MCI stage is essential for management, whether geared toward prodromal or dementia.
MATERIALS AND METHODS
Participants
A total of 1,159 consecutive patients with cognitive impairment with Lewy bodies (including MCI-LB, PD-MCI, DLB, and PDD) were recruited from 22 participating memory clinics of the China Lewy Body Disease Collaborative Alliance from 1 January 2018 to 31 March 2022. The inclusion criteria were (a) patients were 40–100 years of age and (b) the initial clinical diagnosis was probable MCI-LB, DLB, PD-MCI, or PDD. The final diagnoses were confirmed by two experienced neurologists following the criteria double-blindly. In other words, two experts independently verified the initial diagnosis, and neither knew the final diagnosis made by the other. Any patient with a questionable diagnosis or an inconsistent diagnosis given by the two experts was classified as “uncertain diagnosis” and excluded from the study. Finally, 121 patients were excluded because of incomplete demographic information (n = 43) or being classified as “uncertain diagnosis” (n = 78) and 74 patients with MCI-LB, 533 with DLB, 118 with PD-MCI, and 313 with PDD were included (Fig. 1).
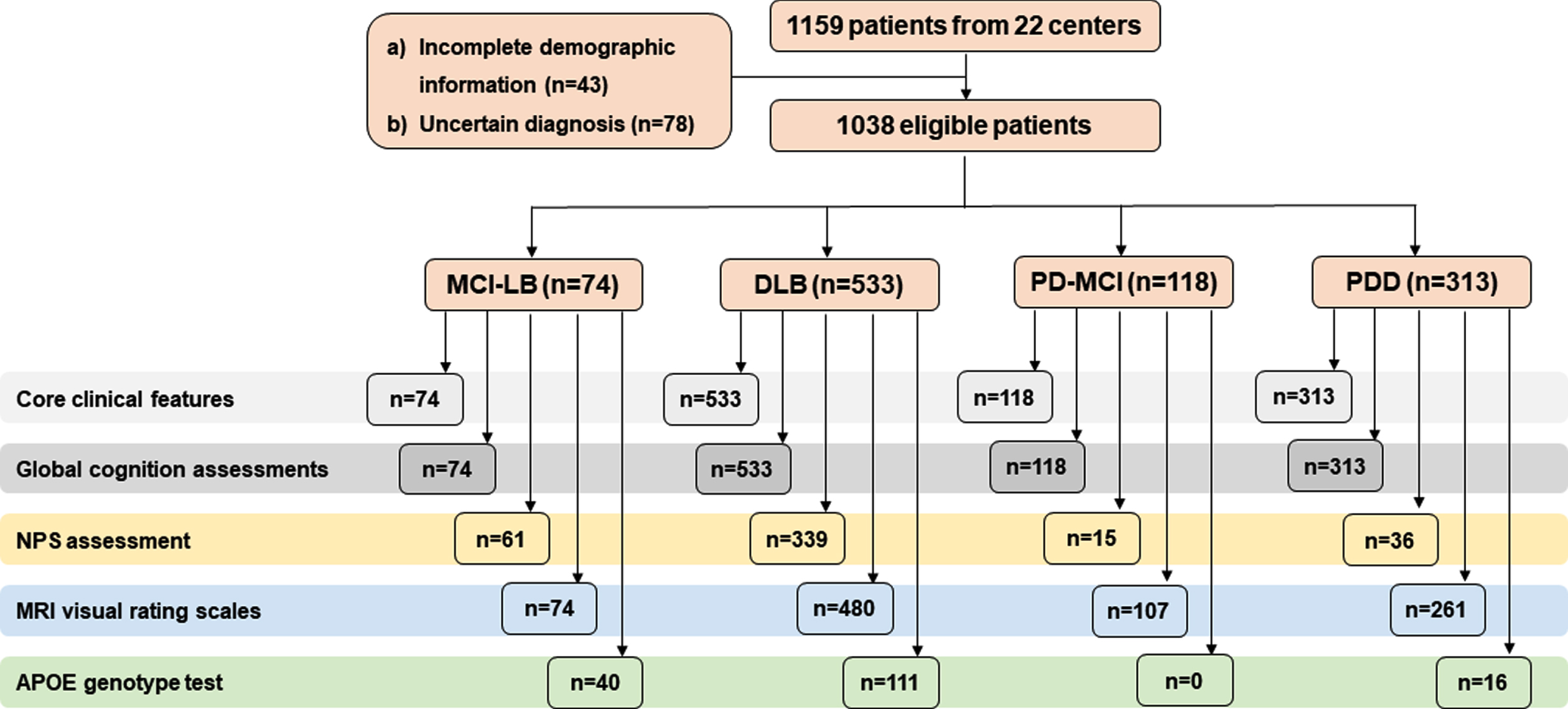
Flow diagram. Incomplete demographic information: lacking of sex, diagnosis/onset age, and educational years; uncertain diagnosis: the two experienced neurologists had questionable diagnosis; eligible patients: including patients diagnosed with probable MCI-LB, DLB, PD-MCI, and PDD; MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; PD-MCI, Parkinson’s disease with mild cognitive impairment; PDD, Parkinson’s disease dementia; NPS, neuropsychiatric symptoms; MRI, magnetic resonance imaging; APOE, Apolipoprotein E.
The Ethics Committees of 22 centers (Supplementary Material) approved all research activities in this cohort study and waived informed consent because the data were pseudonymized, and just with specific ID numbers from registers (ID: KYSQ 2021-068-01). The procedures were performed in accordance with the ethical standards of the Committee on Human Experimentation.
Clinical assessments
Demographic data (including sex, age at last visit, and education), history of cardiometabolic conditions (including history of hypertension, type 2 diabetes mellitus, heart disease and stroke), habits of smoking (with a history of smoking ≥5 cigarettes per day for >2 years), and alcohol consumption (with a history of drinking an alcoholic beverage ≥1 time per week for >2 years) [14], cognitive status (MCI or dementia), onset age of memory loss and parkinsonism, course of disease (age at diagnosis minus onset age), clinical diagnosis at last visit, and neuropsychological assessments [Mini-Mental State Examination (Chinese version) (C-MMSE) [15, 16], Montreal Cognitive Assessment (MoCA) [17], the activities of daily living (ADL) [18], Clinical Dementia Rating (CDR) [19]] were necessary; and the Neuropsychiatric Inventory (NPI) assessment [20], MRI visual rating scales [scale for Medial Temporal lobe Atrophy (MTA) [21], and Fazekas scales [22]], and APOE genotype test were optional. Hypertension (arterial hypertension in this study) was defined as an average systolic blood pressure of at least 140 mm Hg or an average diastolic blood pressure of at least 90 mm Hg, or self-reported use of an antihypertensive drug 2 weeks before the visit [23, 24]. Type 2 diabetes mellitus was defined as self-reported of a previous diagnosis, use of diabetic medications, or hemoglobin A1c of 6.5% or greater [25]. The history of heart disease, including cardiovascular diseases, heart failure, arrhythmia, valvular heart disease, and congenital heart disease was defined as self-reported of a previous diagnosis and/or use of related medications based on clinical records. Prior stroke history, including ischemic stroke and intracerebral hemorrhage stroke, was defined as clinical presentation with confirmation by computed tomography (CT) or MRI based on clinical records. The detailed range and function of neuropsychological assessments are shown in Supplementary Table 1.
Demographic and clinical characteristics
aUnless otherwise indicated, data are expressed as mean (SD).bGap years, the absolute value of onset age of memory loss minus onset of parkinsonism among the target patients.c40 patients with MCI-LB, 111 patients with DLB, 16 patients with PDD, whereas 0 patients with PD-MCI underwent APOE genotype tests;d74 patients with MCI-LB, 480 patients with DLB, 107 patients with PD-MCI, and 261 patients with PDD underwent MTA and Fazekas visual evaluation; e61 patients with MCI-LB, 339 patients with DLB, 15 patients with PD-MCI, and 36 patients with PDD underwent NPI assessment; P1 means the comparation between MCI-LB and PD-MCI groups, and P2 means the comparation between DLB and PDD groups by Mann-Whitney U test or chi-squared test, respectively. MCI, mild cognitive impairment; MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; PD-MCI, Parkinson’s disease with mild cognitive impairment; PDD, Parkinson’s disease dementia; SD, standard deviation; PARK, parkinsonism; T2DM, type 2 diabetes mellitus; APOE, Apolipoprotein E; MTA, medial temporal lobe atrophy; C-MMSE, the Mini-Mental State Examination (Chinese version); MoCA, the Montreal Cognitive Assessment; ADL, the Activity of Daily Living Scale; CDR, the clinical dementia rating; NPI, the Neuropsychiatric Inventory.
In the current study, clinician reports of Lewy body disease core clinical features (cognitive fluctuations, VH, RBD, and parkinsonism) at any visit during follow-up were included. All patients underwent C-MMSE, MoCA, ADL, and CDR evaluation, 451 patients (61 patients with MCI-LB, 339 with DLB, 15 with PD-MCI, and 36 with PDD) underwent NPI assessment to evaluate neuropsychiatric symptom (NPS); 922 patients (74 patients with MCI-LB, 480 with DLB, 107 with PD-MCI, and 261 with PDD) completed MRI visual rating scales; 167 patients (40 patients with MCI-LB, 111 with DLB, 0 with PD-MCI, and 16 with PDD) had the APOE genotype test.
Diagnostic criteria
Cognitive impairment included the diagnosis of MCI and dementia. Dementia patients were diagnosed according to the criteria for primary degenerative dementia in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) [26]. A probable DLB diagnosis can be made with two or more core symptoms with or without indicative biomarkers, or only one core symptom with one or more indicative biomarkers, according to the 2017 criteria by McKeith et al. [1]. The PDD patients were diagnosed according to the clinical criteria for probable PDD, developed by the Movement Disorder Society in 2007 [27]. International consensus suggests that DLB should be diagnosed when cognitive impairment precedes parkinsonism or begins within a year of parkinsonism, and PDD should be diagnosed when parkinsonism precedes cognitive impairment by more than one year. Consensus concerning the criteria for diagnosis of MCI-LB was in development at the time of first diagnosis, so probable MCI-LB was initially defined with a combination of MCI criteria using Petersen’s criteria in 2011 [28] and DLB criteria by McKeith in 2017 [1], with a MMSE ≥20 and CDR score of ≥0.5 [29]. Then the final diagnosis of probable MCI-LB was confirmed by two experienced neurologists double-blindly, if a patient had two or more core LB symptoms with or without the presence of a proposed biomarker (positive FP-CIT SPECT or dopamine transporter PET, and/or meta-iodobenzylguanidine scan, and/or polysomnographic confirmation of REM sleep without atonia) or only one core clinical feature plus one or more proposed biomarkers [2]. Patients with PD-MCI were diagnosed by the diagnostic criteria developed by the Movement Disorder Society Task Force [30]. Additionally, all patients with cognitive impairment with Lewy bodies mentioned in this study had a probable diagnosis.
Evaluations of core clinical features
Fluctuating cognition: The Mayo Fluctuations Composite Scale was used to confirm the presence of cognitive fluctuations, with three or more “yes” responses required for structured questions from caregivers [31].
Visual hallucinations: Specifically formed and detailed VH and illusions, that were complained about by the patient and/or caregiver were determined by confirmation and quantification according to the hallucinations item of the NPI [20].
Spontaneous cardinal features of parkinsonism: One or more spontaneous cardinal features of parkinsonism included bradykinesia (defined as slowness of movement and decrement in amplitude or speed), rest tremor or rigidity, diagnosed by the motor section (Part III) of the Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) [32].
RBD: This was confirmed by caregivers who mentioned five or more behaviors that are mentioned in the RBD screening questionnaire (RBD-SQ) [33] or someone who was diagnosed using overnight video polysomnography [34]. In total, 48 patients with MCI-LB, 51 patients with PD-MCI, 202 patients with DLB, and 99 patients with PDD underwent polysomnography to confirm RBD.
Imaging acquisition and APOE genotyping
Multiplanar oblique coronal (perpendicular to the axis of the hippocampus), transverse and coronal position reconstructions were made of 3D T1-weighted images for diagnostic multisequence MRI. All of the MRI readings were reviewed by two experienced neuroradiologists double-blindly, and the final rating scores were averaged. The details are described in the Supplementary Material. For APOE genotyping, genomic DNA was extracted from peripheral blood stored at –80°C, and the APOE gene was amplified by polymerase chain reaction, as described in our previous study [35]. We determined all genotypes without knowledge of the patient’s status.
Statistical analyses
Quantitative variables were described as mean [±standard deviation (SD)] or median (interquartile range) after normality tests. Qualitative variables were conducted by number (proportion, %). For comparisons of two independent groups (MCI-LB versus PD-MCI or DLB versus PDD), Student’s t-test was used for normally distributed data and a Mann–Whitney U test for nonparametric data. Qualitative variables were assessed using a chi-squared test. The comparisons among the four groups (Fig. 2) were conducted using Mann–Whitney U tests and Bonferroni corrections were also applied. Multiple linear regressions were used to assess the associations between onset age, gap years, and neuropsychological assessments, the confounding variables included sex, education, course of disease, and disease severity, which are considered to be the traditional and significantly different factors.
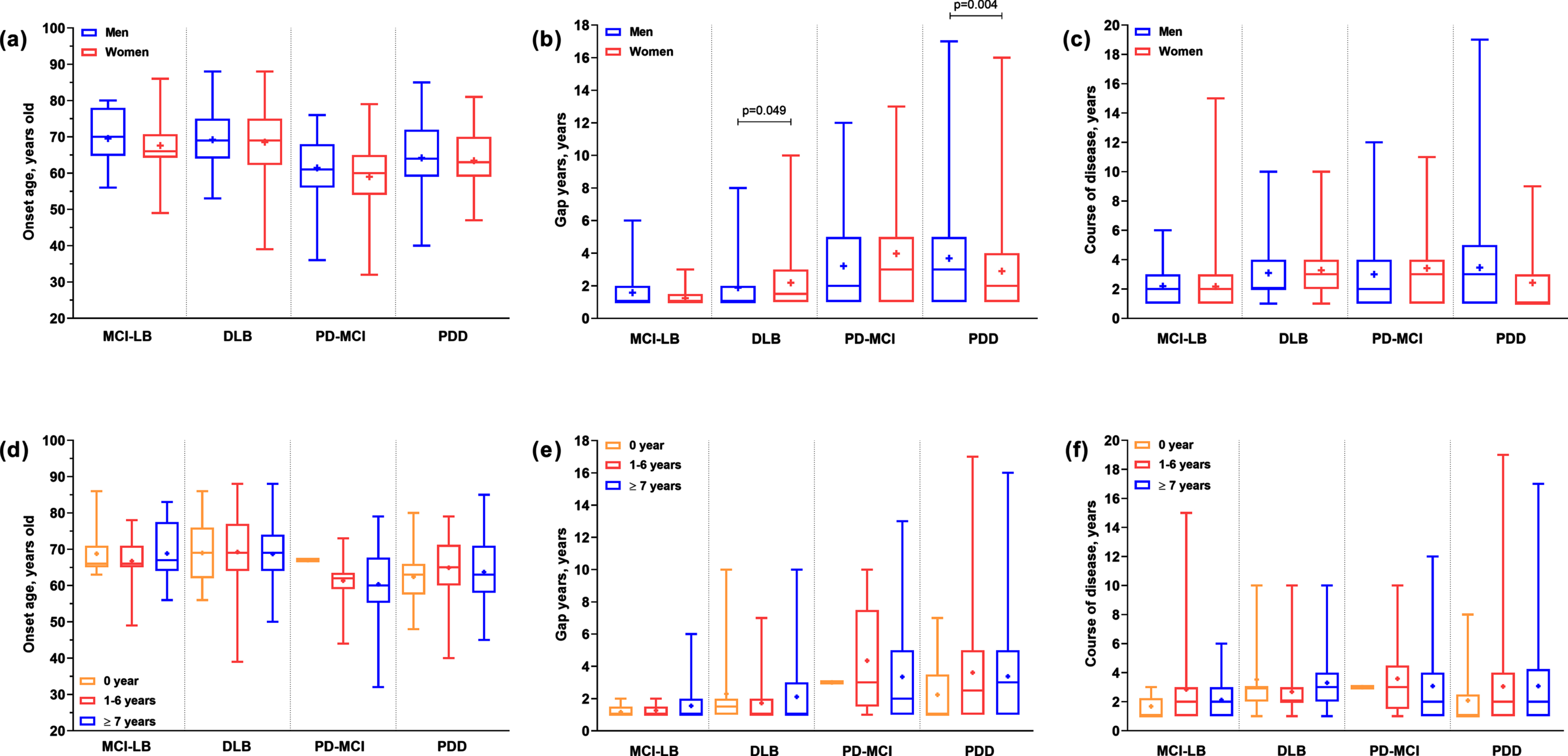
Sex and education differences in onset age, gap years, and course of disease among cognitive impairment with Lewy bodies patients. (a-c) The sex difference of onset age, gap years, and course of disease among four subgroups, respectively; (d-f) the education difference of onset age, gap years, and course of disease among four subgroups, respectively. The bars in the figures mean the min to max of the numbers, and “+” in the box is the median number. The Mann–Whitney U tests were used to compare the sex-difference (a–c) or education-difference (d–f) among the four subgroups, and the significant p-values are labeled in figures (Bonferroni corrections were applied in d–f). Gap years are the absolute value of onset age of memory loss minus onset of parkinsonism among the target patients. MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; PD-MCI, Parkinson’s disease with mild cognitive impairment; PDD, Parkinson’s disease dementia.
The IBM SPSS for Windows (version 25.0; IBM Corporation, Armonk, NY, USA) was used for statistical analyses, with p < 0.05 considered significant at the two-tailed α level.
RESULTS
Demographic and clinical features
Demographics and clinical features are presented in Table 1. Compared with patients with PD-MCI, those with MCI-LB were older (70.46±7.30 versus 64.69±8.26 years, p < 0.001), more likely to be women (64.48% versus 36.44%, p < 0.001), had higher scores of MTA and Fazekas scales, lower scores of C-MMSE and MoCA and higher total-NPI score. The same results were found when comparing patients with DLB to those with PDD. Moreover, DLB patients had significantly greater frequency of delusions, agitation, depression, anxiety, and irritability than PDD patients (Supplementary Figure 1).
The frequency and combination of core features in patients with cognitive impairment with Lewy bodies are shown in Table 2. Generally, 44.59% patients with MCI-LB had one core clinical feature, 66.95% PD-MCI had two features, 42.21% DLB had two features, and 60.06% PDD had three features. For MCI-LB or DLB patients, RBD and VH were the most common core clinical features. Parkinsonism, VH, and RBD were the most common core clinical features of PD-MCI and PDD patients.
The combination of core clinical features in cognitive impairment with Lewy bodies
MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; PD-MCI, Parkinson’s disease with mild cognitive impairment; PDD, Parkinson’s disease dementia; FC, fluctuating cognition; PARK, parkinsonism; RBD, rapid eye movement sleep behavior disorder; VH, visual hallucinations.
Onset age and associations with clinical manifestations
The average onset age of memory loss was 68.28 (±7.00) years, and parkinsonism happened 2.00 (±1.24) years later, at the average age of 69.64 (±6.98) years for patients with MCI-LB (Table 1). Similarly, the onset age of memory loss was 2.46 (±1.82) years earlier than parkinsonism for DLB patients. The average onset age of parkinsonism was 60.56 (±8.96) years and the memory loss happened 3.49 (±3.02) years later for patients with PD-MCI. The parkinsonism (mean = 63.85, SD = 8.39 years) had onset 3.31 years earlier than memory loss (mean = 67.22, SD = 7.86 years) for patients with PDD. There were no significant sex or education differences in onset age and course of disease among MCI-LB, DLB, PD-MCI, and PDD patients (Fig. 2).
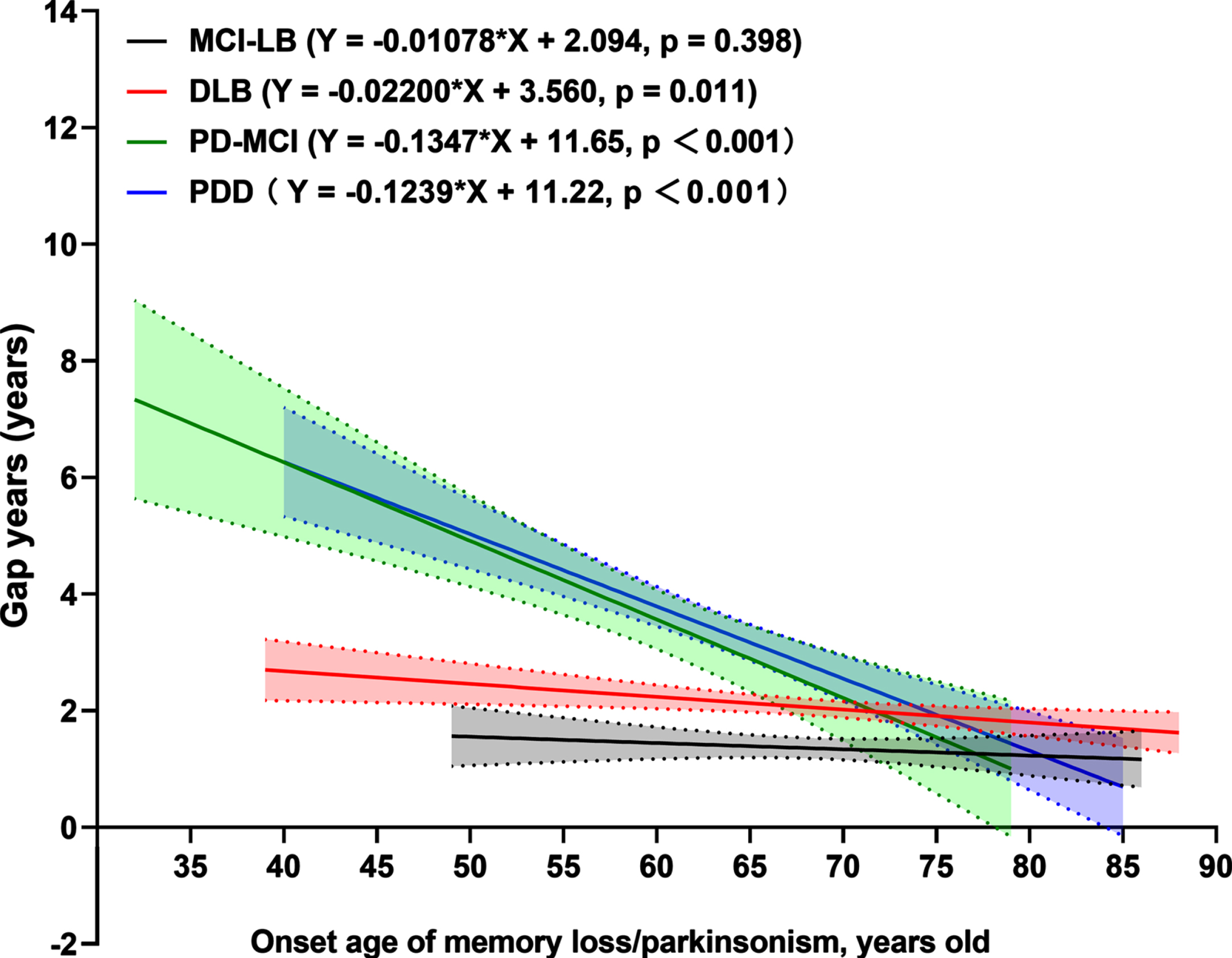
The linear regressions (Fig. 3) showed significant positive relationships between the onset age of memory loss and gap years for patients with DLB (R2 = 0.012, p = 0.011), and the onset age of parkinsonism and gap years for patients with PD-MCI (R2 = 0.160, p < 0.001) and PDD (R2 = 0.123, p < 0.001). In other words, the older the onset age, the shorter the gap years between memory loss and parkinsonism.
Associations between onset age and gap years in cognitive impairment with Lewy bodies patients. Gap years, the absolute value of onset age of memory loss minus onset of parkinsonism among the patients. MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; PD-MCI, Parkinson’s disease with mild cognitive impairment; PDD, Parkinson’s disease dementia.
The onset age was associated with scores of C-MMSE [Coefficient B = –0.064, 95% confidence interval (95% CI) = –0.122 to –0.005, p = 0.033 for patients with MCI-LB; Coefficient B = –0.108, 95% CI = –0.186 to –0.030, p = 0.007 for patients with PDD] and ADL scores (Coefficient B = 0.175, 95% CI = 0.036 to 0.313, p = 0.014 for patients with DLB; Coefficient B = 0.143, 95% CI = 0.007 to 0.278, p = 0.039 for patients with PDD) at diagnosis. Moreover, the onset age had significant associations with the scores of delusions (Coefficient B = 0.043, 95% CI = 0.008 to 0.078, p = 0.016) and depression (Coefficient B = –0.040, 95% CI = –0.071 to –0.008, p = 0.014) in patients with DLB (Fig. 4).
Associations between onset age and neuropsychological assessments. The linear regressions were used to determine the associations between onset age (age of memory loss for patients with MCI-LB and DLB; onset age of parkinsonism of patients with PD-MCI and PDD) and the scores of C-MMSE, MoCA, ADL, and NPI and its sub-items, after adjusting for sex, education, course of disease, and disease severity. The results were recorded as Coefficient B with 95% CIs (bars). MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; PD-MCI, Parkinson’s disease with mild cognitive impairment; PDD, Parkinson’s disease dementia; C-MMSE, the Mini-Mental State Examination (Chinese version); MoCA, the Montreal Cognitive Assessment; ADL, the Activity of Daily Living Scale; NPI, the Neuropsychiatric Inventory.
DISCUSSION
In the current study, we presented the demographic and clinical characteristics of cognitive impairment with Lewy bodies patients. We found that women were predominant in MCI-LB and DLB. The average onset age of PD-MCI was younger than MCI-LB, and memory loss occurred 3 years after parkinsonism in PD-MCI. The onset age was positively associated with scores of ADL and delusions, but negatively associated with scores of MMSE and depression in DLB. We also provided a characterization of clinical core features, of which RBD and VH were the most frequently reported in MCI-LB, DLB and PDD, while VH was least frequently reported in PD-MCI.
Onset age and sex difference
This multicenter cohort study showed that over half of patients with MCI-LB and DLB were women, and there was a significant sex difference in MCI-LB. Similarly, a cross-sectional study from the French National Alzheimer database (Banque Nationale Alzheimer) presented a slight predominance of women (54.7%) in the DLB population [36]. Although previous studies of clinical DLB prevalence in men and women are inconsistent, the majority report a higher clinical prevalence in men [3, 5]. Multicenter research including nine participating psychiatry of old age/memory clinic services in the UK revealed that prevalence and incidence of DLB were higher in men [5]. Inconsistent findings may be attributed to differences in sample size, race, methodology, neuropathology, or severity of cognitive impairment. Nelson et al. supposed clinically DLB tended to be underdiagnosed in men and overdiagnosed in women [37] on the basis of their findings: women were more predominant in the mixed pathology of “AD + DLB” than in pure DLB [38], with less likely neocortical (“diffuse”) or intermediate (“limbic”) LB pathologies [37]. Because we obtained clinical diagnosis rather than anatomopathological results, this may explain the clinical predominance of women in DLB. However, there have been no studies on sex ratio of MCI-LB with a large sample, and future studies should focus on this sex difference.
Our findings showed that DLB patients were significantly older than PDD patients at the time of diagnosis (72.05 versus 68.06 years) and both onset ages of memory loss and parkinsonism were also higher for DLB compared with PDD patients. Similar conclusions were also drawn by Fereshtehnejad et al. [39], who reported that PDD tends to affect younger patients than does DLB. A 15-year prospective population-based elderly cohort study in south-western France showed the mean age for incidence of suspected DLB was also higher than for PDD [40]. Similarly, nine PDD and DLB patients showed that the mean age when dementia appeared was higher in DLB than PDD patients (73 versus 71 years) [41]. However, few previous studies have conducted a complete comparison of the onset age of memory loss and parkinsonism in DLB and PDD, especially in MCI-LB and PD-MCI.
Our study confirmed that the onset of DLB was older than PDD, both in terms of memory loss and parkinsonism. We firstly demonstrated that the average onset ages of memory loss (68.28 versus 64.07 years) and parkinsonism (71.05 versus 60.56 years) were higher for patients with MCI-LB compared with PD-MCI. Moreover, the gap years of PD-MCI patients were much longer than MCI-LB patients (3.49 versus 2.00 years). Memory loss is a frequent problem throughout the entire progress of PD. Longitudinal cohort studies reported that 15–20% of PD patients had dementia after 5 years and about 50% after 6–10 years [42], and 30.3% of patients could develop MCI within 2 years [43]. Unfortunately, there is still a lack of comparative studies on clinical symptoms between MCI-LB and PD-MCI in large samples, and little is known about their respective demographic characteristics.
Clinical characteristics
Of the four core clinical features, RBD and VH were the most frequently presented in MCI-LB, DLB, and PDD. High prevalence of RBD was also known from previous literature [12]; RBD might also be the most characteristic sign of MCI-LB [44], and is helpful for an early differential diagnosis of LBD from late-onset psychiatric disorders, even before parkinsonism or dementia appears [45]. More than two-thirds of DLB and PDD patients in our cohort had VH, and mainly reported seeing vivid animals, plants, or people. A meta-analysis showed that VH were prevalent, with an estimated pooled prevalence of 28.2% and 61.8% in PDD and DLB, respectively [46]. Oliveira [8, 47] reported a much higher proportion (24/25, 96.0%) and more severe VH (mean score of hallucinations in NPI, 5.20±4.35) in Brazilian DLB patients, possibly because they were more severe cases than our patients. In our study, VH was the least frequently reported with a proportion of 27.97% compared to other features in PD-MCI. Parkinson’s disease psychosis, such as hallucinations and delusions, is one of the debilitating non-motor symptoms of PD [48]. The estimates of complex VHs range within 22–38% [49], and about 50–60% of PD patients report the presence or passage of VH in their processes [50]. The prevalence rates of VH tend to be associated with other NPS. When a LBD patient has delusion, agitation, RBD or other types of NPS, they usually have a higher frequency of VH [51]. Moreover, the prevalence rate of VH is related to visual function, medication effects, cognition, and Lewy bodies burden [52, 53]. Thus, MCI stage might be a potential explanation for this discrepancy. In addition, 62.10% of DLB patients had signs of parkinsonism, consistent with findings in the DEvELOP cohort [12].
In our cohort, NPS presented frequently, even in the MCI stage. Night-time behavior disturbance was the most frequent and severe NPS in MCI-LB and PD-MCI. Moreover, NPS of PD-MCI was more severe than of MCI-LB, particular in night-time behavior disturbances and appetite and eating abnormalities. Hallucinations, appetite and eating abnormalities, depression, and anxiety were also frequently reported, albeit not significantly different between MCI-LB and PD-MCI. These findings were consistent with previous cross-sectional [29] and longitudinal [11] studies of prodromal DLB and PD. We first reported NPS of PD-MCI and compared them with MCI-LB patients in this research. Similar to previous studies [6, 54], patients with DLB had significantly more frequent and severe NPS than PDD patients, such as delusions, agitation, depression, anxiety or irritability. However, some studies [8, 47] have shown that DLB patients were more likely to have aberrant motor behavior than PDD patients, and we considered that this inconsistency was related to differences in sample size, race, educational level, and disease severity.
Associations between onset and clinical assessments
Both NPS and cognitive impairment are common non-motor features of cognitive impairment with Lewy bodies and can occur across the disease course during the prodromal or dementia phases. We demonstrated that late-onset age was associated with worse cognitive performance and daily life function. Evidence, mostly cross-sectional and longitudinal studies, showed late-onset PD patients had a more rapid progression of cognitive decline [55]. Moreover, the onset age had significant associations with the scores of delusions (Coefficient B = 0.043) and depression (Coefficient B = –0.040) assessed by NPI in patients with DLB. Although conflicting results (e.g., higher, equal, or lower incidences and severity of NPS) have been reported in LBD patients, the general consensus is that depression is more common in patients with early onset of LBD [56]. A retrospective neuropathological cohort with 2,422 participants supported that patients with “AD+LB” pathology and greater age had higher risk of delusions [56]. In addition to age and sex, the prevalence and severity of NPS in LBD are associated with disease severity, neuropathy, excessive daytime sleepiness, RBD, dyskinesias, and dopaminergic therapy [55].
Temporo-parietal atrophy on MRI (which is indicative of AD pathology) is associated with cognitive decline in dementia patients [57]. In current research, the degree of atrophy on MRI was relatively mild but greater than that of PDD in both MCI and dementia stage, indicating more severe cognitive impairment in DLB. We also found that DLB showed more severe white matter hyperintensities than PDD, consistent with previous research investigating atrophy and white matter hyperintensities in LBD [58].
Strengths and limitations
The main strength of this study is that this is the first multicenter study in China utilizing a large sample size, with delineation of onset age of memory loss and parkinsonism. However, the onset ages in the analysis are limited by clinical assessments by doctors or reports by caregivers at diagnosis, which increases the likelihood of recall bias. And the significant differences of cognitive and functional performance between DLB and PDD groups might affect the accuracy of analysis, such as leading to more frequent NPS in DLB or affecting the distributions of core clinical features, even though we corrected for these confounders. In addition, the diagnoses of patients were not subsequently validated by autopsy, which is the gold standard for a diagnosis. Moreover, the lack of UPDRS records further affects our research on motor symptoms in cognitive impairment with Lewy bodies. Finally, the cohort was all Chinese patients in memory clinics, which will lead to differences with other regions and so limits the generalizability.
Conclusions
In this first study investigating onset age and clinical characteristics of cognitive impairment with Lewy bodies patients in a large-sample cohort, the results suggest that 1) women were predominant in MCI-LB, 2) memory loss and parkinsonism occurred earlier in PD-MCI and PDD than MCI-LB and DLB, and memory loss occurred 3 years after parkinsonism in PD-MCI, and 3) onset age was associated with cognition and NPS in cognitive impairment with Lewy bodies patients. Awareness of these characteristics could be helpful in LBD management. With ongoing data collection from multidisciplinary teams, we aim to further investigate the motor and other non-motor symptoms in their entire progresses, particularly in prodromal stages, then to formulate demography-specific management plans for LB patients.
Footnotes
ACKNOWLEDGMENTS
The authors thank the neurologists and neuropsychological scale evaluators who coordinated data collection from all centers. The authors thank all the participants, and the Tianjin Key Medical Discipline (Specialty) Construction Project for their help.
This work was supported by the National Natural Science Foundation of China (grant numbers 82171182 and 81571057), Science and Technology Project of Tianjin Municipal Health Committee (grant numbers ZC20121 and KJ20048), the Tianjin Science and Technology Project (grant number 16ZXMJSY00010), and Tianjin Key Medical Discipline (Specialty) Construction Project (grant number: TJYXZDXK-052B).