
Abstract
Background:
Glucose metabolism and insulin signaling alterations play an important role in Alzheimer’s disease (AD) pathogenesis. Researchers have extensively attempted to characterize the exact pathophysiological mechanisms in the cerebrospinal fluid (CSF), as evidence concerning this fluid biomarkers is expected to enhance AD diagnosis’ specificity and accuracy and serve as an early disease detection tool. There is controversy about insulin levels in the CSF relationship with mild cognitive impairment (MCI) and AD.
Objective:
This systematic review provides an overview of the state-of-the-art knowledge about insulin-related CSF biomarkers in AD and MCI.
Methods:
We performed a qualitative systematic literature review of reported data of CSF glucose, insulin, or insulin-related molecules in humans with AD or MCI, consulting the electronic databases Medline, Scopus, Web of Science, Cochrane, and BASE until May 2022.
Results:
We selected 19 studies, 10 of them reporting data on CSF insulin and 8 on insulin-related molecules like growth factors or their binding proteins. They predominantly found decreased levels of CSF insulin and increased levels of CSF insulin-related growth factors and their binding proteins.
Conclusion:
Due to the studies’ protocols and results heterogeneity, we recommend a larger database of clinical trials with similar characteristics for a better understanding of this relationship.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a progressive neurologic disorder that causes a continuous decline in cognitive, behavioral, and social skills that affects a person’s ability to function independently. It represents the most common type of dementia worldwide and its incidence is increasing each year as the elderly population grows, being nowadays estimated to reach the 40.2 cases per 1000 habitants [1]. Mild cognitive impairment (MCI) is the stage before a serious decline of dementia and its amnestic subtype is regarded as a prodromal phase of AD [2].
At the present, it is not clear which tests are sensitive and specific enough to detect AD in early phases, being difficult to find a screening instrument that could be used in every population [3]. During the last two decades, multiple proteomic studies have identified a variety of potential biomarkers of AD in the cerebrospinal fluid (CSF) [4, 5]. The diagnostic criteria update from 2011[6] integrated body fluids biomarker evidence into the diagnostic formulations. Despite being generally limited for research settings nowadays, biomarkers are expected to enhance the pathophysiological specificity and the diagnostic accuracy of AD diagnosis.
Glucose metabolism alterations and their role in AD pathogenesis have been widely studied, as insulin has shown to have crucial effects on the correct functioning of synapses. Brain insulin resistance is the failure of brain cells to respond to this hormone. This leads to a cellular glucose hypometabolism, which results in the loss of their function and impaired clearance of amyloid-β (Aβ) and its precursor, which are considered typical features of AD at clinical stages [7–9]. In humans, the CSF/serum insulin ratio appears to be reduced in the presence of whole-body insulin resistance, even in the absence of type 2 diabetes mellitus (DM) [10, 11], as well as with increasing age [12]. Considering that similar Aβ deposits have been found both in the pancreas in type 2 DM as in the brain and that some of the target receptors of type 2 DM are also involved in the regulation of the expression and phosphorylation of tau protein, some scientists have suggested addressing this metabolic syndrome that impairs central insulin functioning as type 3 DM [9, 13].
There is controversy about CSF insulin’s relationship with MCI and AD. Several studies have found that these patients have lower insulin [14–18] and higher insulin-related growth factor, or their binding protein [19–27], CSF levels compared to cognitively normal individuals, whereas others reported contradictory findings [25, 28–30]. Consequently, this systematic review is intended to provide an overview of the state-of-the-art knowledge about insulin-related CSF biomarkers in MCI and AD. This line of research could additionally help to update some AD pathophysiological concepts and increase its therapeutical targets.
METHODS
This systematic review has been conducted and authored according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guideline [31].
Eligibility criteria
The inclusion criteria of this review were articles published in a peer-reviewed journal that reported data of CSF glucose, insulin, or insulin-related molecules in a human population and/or human specimens where at least one of the groups had a diagnosis of AD or MCI. We excluded reviews and conference abstracts.
Information sources
We consulted the electronic databases PubMed/Medline, Scopus/Embase, Web of Science, Cochrane, and BASE academic search engine until March 2022. Additional sources were bibliographic references of the included studies.
Search strategy
Two independent investigators performed a systematic review of the literature with the keywords “Alzheimer’s disease, mild cognitive impairment, insulin, glucose and cerebrospinal fluid” combined in the following search code: (Alzheimer’s disease OR mild cognitive impairment) AND (insulin OR glucose) AND cerebrospinal fluid.
Selection process
Two independent reviewers without any automatization tool evaluated the studies to assess their eligibility. Finally, a full-text evaluation was performed before including them in the review.
Data collection and data items
Data was manually collected in an excel form by two independent reviewers without any automatization tool. We extracted the following items: first author, year of publication, study design, sample size, average age, groups, AD or MCI diagnostic criteria, detection technology used in CSF, biomarkers measured in any human fluid, other tests including neuroimaging, cognitive tests, and genetic analysis. Outcomes variables were glucose, insulin, and insulin-related molecule levels in CSF.
This systematic review has been registered at the PROSPERO International prospective register of systematic reviews.
RESULTS
Studies selection
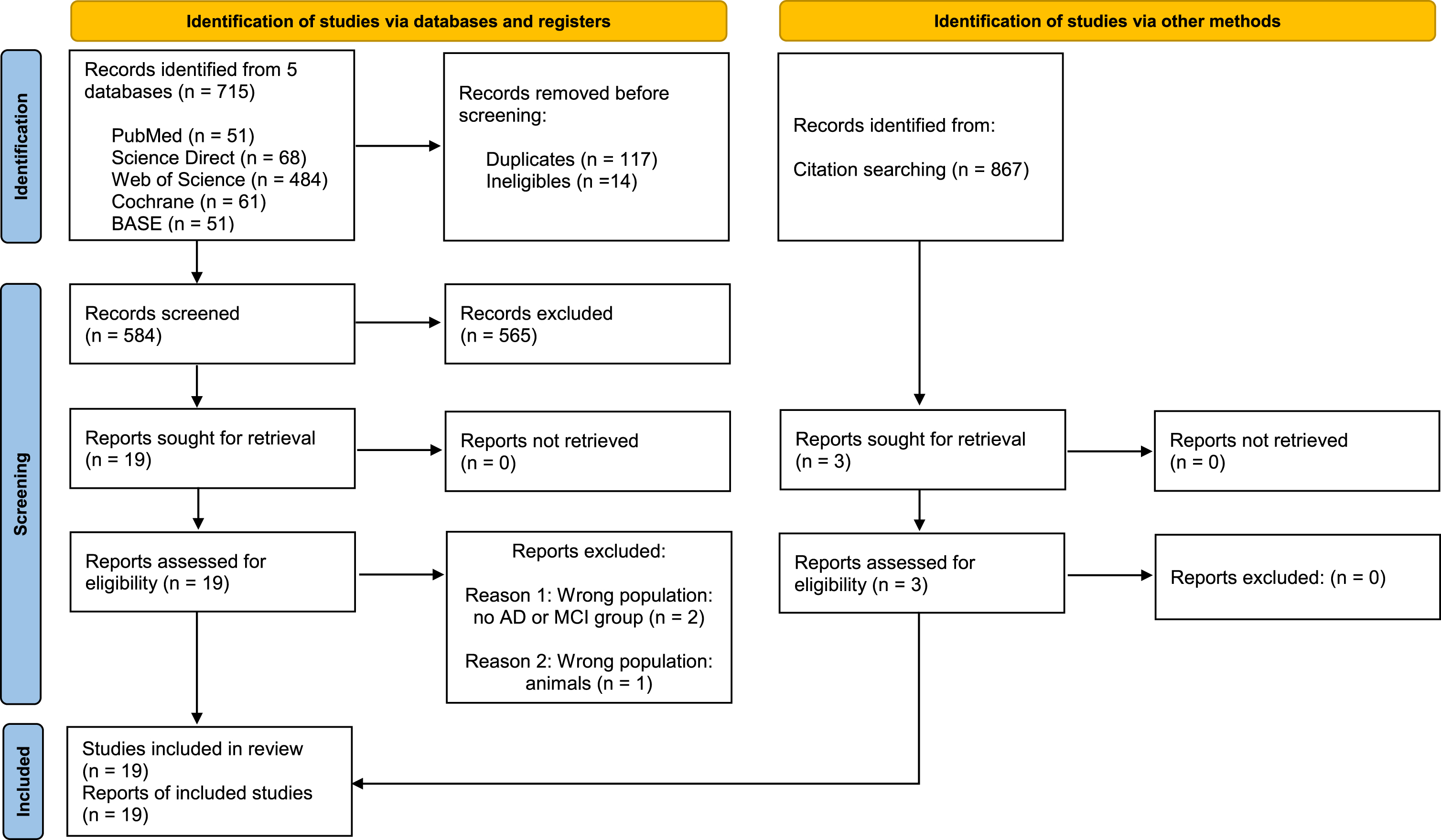
The initial search generated a total of 715 records: 51 from PubMed/Medline, 68 from Scopus/Embase, 484 from Web of Science, 61 from Cochrane, and 51 from the BASE. After removing 117 duplicates and 14 ineligible records and screening the results we selected 19 articles to assess for eligibility [14–26, 32–35]. Additionally, 3 more articles were obtained from bibliographic references [27, 36]. After a full text read, 3 articles were excluded, 2 of them because any of the groups contained AD or MCI population [33, 34], and the remaining one because it did not use human samples [32]. Therefore, we obtained a total number of 19 studies to include in our review [14–30, 36]. Figure 1 contains the flow diagram of the study’s selection.
Studies characteristics
Table 1 summarizes the 19 studies that proved eligible for inclusion, their characteristics, and the results obtained. The sample size ranged from 20 to 245 and the average age was 70 years old. They generally distributed their population in controls and AD patients [14, 35]. Additionally, some studies distinguished among the AD severity [16, 17] medication status [25], or set additional cognitive-impaired categories: MCI [15, 26], amnestic MCI (aMCI) [28], subjective cognitive impairment (SCI) [16, 28], and other dementias [19, 30]. The AD diagnosis was most commonly made by the NINCDS-ADRDA criteria [14–17, 36], though other methods were occasionally used: DSM-III [15, 35], DSM-IV [16, 20], CSF profile [18], and postmortem histological analysis [25]. MCI patients were selected in a more heterogeneous fashion, using the Petersen guidelines [19, 20], cognitive decline reports [16], or previously selected memory clinic populations [22, 28]. Basically, all the observational study designs were cross-sectional, except for one which longitudinally followed a memory clinic population for two years and reported any change from their initial diagnosis by the end of that period [16].
Characteristics and results of the studies
Aβ, amyloid-β; ADAS-COG, Alzheimer’s Disease Assessment Scale; AD, Alzheimer’s disease; ADNI, Alzheimer’s Disease Neuroimaging Initiative; Alb, Albumin; aMCI, amnestic mild cognitive impairment; APOE4, Apolipoprotein E4 genotype; AVLT, Auditory Verbal Learning Test; AQT, A quick test of cognitive speed; CDR, Clinical Dementia Rating; CDT, Clock Drawing Test; CGA, Cornell Scale for Depression in Dementia; C-Peptide, connecting peptide; CS, cross-sectional; CSF, cerebrospinal fluid; CSF-AD, Alzheimer’s disease-like cerebrospinal fluid profile; CSF-C, control-like cerebrospinal fluid profile; DCT, digit cancellation test; DF, drug-free; DSB, digit span backward; DSM, Diagnostic and Statistical Manual of Mental Disorders; EF, executive function; ELISA, enzyme-linked immunosorbent assay; FDG-PET, fluoro-deoxy-glucose positron emission tomography; GDetS, Global Deterioration Scale; GDS, Geriatric Depression Scale; GIP1, gastrointestinal peptide-1; GLP-1, glucagon-like peptide-1; I-FLEX, a short form of the Executive Interview; IGF, insulin growth factor; IGFBP, insulin growth factor binding protein; IgG, immunoglobulin G; IL-6R, interleukin 6 receptor; L, longitudinal; Mild AD, mild Alzheimer’s disease; MCI, mild cognitive impairment; MCI-AD, mild cognitive impairment that progressed to Alzheimer’s disease; MMSE, Mini-Mental State Examination; Mod-AD, moderate Alzheimer’s disease; MRI, magnetic resonance imaging; N, total number; NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association criteria for Alzheimer’s Disease; NINCDS-AIREN, National Institute of Neurological Disorders and Stroke and the Association Internationale pour la Recherche et l’Enseignement en Neurosciences criteria for VaD; PAI-1, plasminogen activator inhibitor-1; P-tau, phosphorylated tau; RIA, radioimmunoassay; SCI, subjective cognitive impairment; SMB, immunoreactive somatomedin B; SMI, subjective memory impairment; SMCI, stable mild cognitive impairment; STEP, stepwise comparative status analysis; TMT, Trail Making Test; T-tau, total tau; VaD, vascular dementia; WAIS-R, Wechsler Adult Intelligence Scale revised; WMHs, white matter hyperintensities; WMS, Wechsler Memory Scale.
In this review, we identified other tests that were performed in the study population regarding neuroimaging, cognition, and genetics. Occasionally, this extended population analysis uncovered additional correlations with the biomarkers under investigation. Concerning neuroimage, MRI was the most widely used technique [18, 36]. In its absence, CT scans were performed [24, 35]. Exclusively one study conducted an FDG-PET [26]. In relation to cognitive assessments, 15 out of 19 studies, conducted the MMSE evaluation [15–22, 36]. A minority performed a more exhaustive exam including at least three other cognitive assessment batteries [21, 26]. Regarding genetical analysis, some authors decided to study the APOE4 allele status in their AD patients [16–18, 36] and just one of them analyzed the IGFBP-2 gene [26].
Results of the studies
Our main outcomes of interest were CSF biomarkers in relation to insulin metabolism. These biomarkers were additionally measured in part of the studies in plasma [15–17, 36] and occasionally the ratios between the values obtained in each fluid were made [15, 36]. The principal detection and quantification techniques utilized in the CSF were radioimmunoassay [16–18, 28–30] and enzyme-linked immunosorbent assay [14, 35], though 2 studies utilized mass spectrometry [26, 27].
Ten studies reported CSF insulin levels [14–20, 28–30], whereas 8 measured insulin-related molecules like growth factors or their binding proteins [19–26]. Other common CSF biomarkers measured were glucose [17, 36], pyruvate [35], cholesterol and its metabolites [18], albumin [16, 25], inflammatory molecules [14, 26], and other hormones closely involved in metabolism as ghrelin, leptin, and glucagon [15]. Habitually, they also determined CSF AD biomarkers Aβ142, T-tau, and P-tau [14–16, 36], in their majority with the aim of finding correlations between them and the new biomarkers under investigation.
CSF insulin
Of the 10 studies which analyzed CSF insulin, only 8 dragged statistically relevant conclusions. Their majority, 5 out of 8, found insulin decreased or negatively correlated with AD characteristics. In 3 studies CSF insulin was reduced in AD compared to controls [14, 15] or SCI [16]. de La Monte et al. [15] also found this in MCI. Moreover, it was found negatively correlated with cognition status in non-APOE4 carriers [17] and with parieto-occipital white matter hyperintensities (WMHs) among controls [18]; and positively correlated with CSF Aβ142 [16] among women.
Contrarily, CSF insulin was found elevated in AD compared to controls [30] and positively correlated with CSF P-tau [28] among women, though just among APOE4 non-carriers in one study [28], which additionally found a correlation with T-tau. Finally, Molina et al. [29] found neither a significant difference between AD and controls nor a correlation with MMSE scores.
Insulin growth factors
Of the 7 studies which measured insulin growth factors in the CSF, 6 have obtained statistically significant results. Most of these results dragged conclusions in relation to IGF-2, which was found to increase in AD compared to controls [21, 24] and stable MCI [19], and positively correlate with CSF P-tau and T-tau [19]. However, Tham et al. [25] found no relation to AD. CSF IGF-1 was also reported to increase in AD compared to controls [23] and positively correlate with CSF P-tau and T-tau [22].
Insulin growth factor binding proteins
There are 7 studies which measured IGFBPs in the CSF. Almost all of them found statistically significant evidence linking the elevation of at least one of them, from IGFBP-1 to 6, with AD. Compared to controls, the binding proteins that were found to increase in AD in each of the studies were: all of the IGFBPs [23], specifically IGFBP-2 [19, 24] and IGFBP-3 and 5 [27]. Additionally, a positive correlation with CSF T-tau was found in 2 studies with IGFBP-2 [19, 26]. Contrarily to these results, Johansson et al. [20] found a positive correlation between CSF Aβ142 and IGFBP-3.
Other biomarkers
Of the studies which analyzed additional insulin-related molecules in the CSF, only 2 obtained statistically significant results. Parnetti et al. [35] found CSF pyruvate increased in AD compared to controls and negatively correlated with the dementia severity. Of the 5 studies with measured CSF glucose, only Dumurgier et al. [36] found that the CSF/plasma glucose ratio was negatively correlated with CSF Aβ142.
DISCUSSION
In this systematic review, marked heterogeneity was observed among the results obtained in the 19 studies included. Whereas some of them have found that these patients have lower insulin [14–18] and higher insulin-related growth factor, or their binding protein [19–27], in CSF levels compared to cognitively normal individuals, others reported contradictory findings [25, 28–30]. Similarly, we have found noticeable differences among the panel of insulin-related biomarkers selected to measure in the CSF by each of them. According to the study population, we have generally observed that a greater quantity of relationships were able to be made in those studies which carried a more detailed evaluation of their AD patients, mainly regarding neuroimaging, cognitive and genetic tests.
Regarding neuroimaging, only a few of the selected articles performed an MRI on AD patients. Several authors used the quantification of white matter hyperintensities by regions to range patients by their lesions severity or rule out other dementia types [18, 22]. Only McLimans et al. [26] used newer MRI segmentation tools to obtain grey matter maps and assessed regional cerebral glucose metabolism by fluorodeoxyglucose positron emission tomography (FDG-PET). In terms of cognitive evaluations, most of the studies used the NINCDS-ADRDA diagnostic criteria to identify their AD cases. We have noticed that only a reduced number of studies performed an extensive battery of tests in their population [21, 26], which could have allowed them to have information about the specific impaired cognitive domains and its correlations with CSF biomarkers. In relation to the APOE4 allele, among the 7 studies we reviewed that included its determination, 2 of them dragged different statistically significant results on APOE4 carriers compared to non-APOE4 carriers [17, 28]. Increasing evidence suggests that this allele, apart from being involved in neuronal and blood-brain barrier maintenance and repair [37], impairs proper neuronal insulin signaling by binding to its receptors in the brain and trapping them in endosomes [38].
Further research with more similar protocols would be needed to establish clear relationships and define useful clinical diagnostic parameters and thresholds. We think that at the time of designing a study, it could be considered useful for researchers to be able to find in this systematic review a summary of the techniques and variables’ stratification previously used by other researchers, taking into account the conclusions obtained by each of them. An additional way to tackle the variables heterogeneity would be to create a common bank with the patients’ samples to conduct large-scale studies. In that way, the variables could be homogenized or stratified as the researcher may consider in order to obtain more reliable conclusions.
Concerning the outcomes of the studies, we have become aware that IGFs and their binding proteins have been studied in a similar number of studies to insulin, and that is why we thought that their inclusion in this review would be useful in the light of future research decisions. Previous knowledge has already been analyzed in several reviews and meta-analyses, as opposed to insulin. Ostrowski et al. (2016) carried out a meta-analysis of 9 studies [39] which measured IGF-1 serum levels and did not find a significantly different trend in AD patients, although 8 of them individually detected statistically significant changes. Furthermore, Hu et al. in another review [40] mentioned that circulating serum IGFBP-3 levels in AD may decrease earlier than IGF-1. However, they did not find a significant difference in circulating IGF-1 and IGFBP-3 levels compared to controls, blaming for that the heterogeneity among mean ages and MMSE scores among the population. A replication study and meta-analysis from Ma et al. [41] supported statistically significantly higher serum insulin levels in AD patients than in controls.
The only meta-analysis that included studies with CSF IGF-1 measurements was published by Xu et al. [42]. They found that CSF IGF-1 levels were significantly lower in AD only with 3 articles pooled. In serum, the IGF-1 was as well significantly decreased in AD and showed a decreasing trend in MCI in studies with a total sample size higher than 80, but an increasing trend in AD in studies with a total sample size smaller, suggesting that age differences might explain that incongruity.
Despite these results, in our review we predominantly found increased CSF levels of insulin growth factors and their binding proteins in AD and MCI, or in correlation with lower CSF Aβ142 or higher T-tau and P-tau. Since there are no systematic reviews or meta-analyses analyzing insulin in CSF to our knowledge, we can just compare our results to the pathophysiological explanations of the brain insulin resistance phenomenon. It has been hypothesized that during systemic insulin resistance states, the blood-brain barrier receptor-mediated insulin transport is altered, leading to relatively lower CSF insulin concentrations, compared to the serum [10]. This theory correlates with the results of most of the studies we included in our review, which found a significant decrease of CSF insulin in AD, though only one of them found the same in MCI [15].
Other metabolic alterations that could be manifested in the CSF may come from the signal the brain triggers when decreased glucose is sensed, which leads to compensatory activation of alternative sources to fuel the tricarboxylic acid cycle such as amino acids and fatty acids. Velpen et al. [5] found that tricarboxylic acid cycle and beta-oxidation intermediates were higher in CSF in AD compared to controls, while amino acid concentrations were significantly lower. The association of CSF creatinine and Aβ1–42 suggests its involvement in amyloid accumulation. Lastly, tryptophan CNS-specific pathway alteration in AD resulted in significantly higher concentrations of the neuroprotective kynurenic acid and neurotoxic quinolinic acid in CSF.
Current research is working hard in consolidating evidence to recommend antidiabetic agents to treat dementia caused by AD, as most of the clinical trials are still in phase II. Optimistic results have been not only obtained with intranasal insulin administration, which has shown the best and most consistent outcomes for the moment, but also with most of the commonly used antidiabetic medication [43–45]. The extension of the knowledge concerning AD pathophysiologic routes in terms of insulin metabolism could serve as a source of information to improve these new treatment lines or address the inconveniences they may elucidate. The more specific these neurodegeneration routes are defined, the more suitable the drug format could be designed regarding the receptors and cellular mechanisms for drug absorption or maintenance in the CSF.
By other hand, an earlier diagnosis of AD is essential to improve patients’ life quality and expectancy. Moreover, clinicians would be able to make further adjustments to patients’ habits or treatments to tackle comorbidities in these earlier stages to potentially ameliorate the disease course. Therefore, it is crucial to identify new potential biomarkers in early stages of the disease.
The main limitation we found in this review is that we were not able to perform a biased analysis of the studies selected. In relation to the reviewed studies, we have identified several factors that may explain the variability among their results. Firstly, the usage of populations with different mean ages or MMSE scores, which indicates different stages of the disease. Additionally, CSF samples’ time of extraction was not recorded in most of the articles we included in our review, and in their majority, they did not take into account the medications patients were taking at that moment. Different quantification laboratory techniques used in CSF may as well influence the results obtained. Finally, the APOE4 allele status was neither analyzed in most of them.
Conclusion
This systematic review analyzes and summarizes the current state-of-the-art of changes in insulin and insulin-related molecules in CSF in AD and MCI. Interesting conclusions are dragged from the studies we selected, that predominantly have found decreased insulin levels and increased insulin-related growth factor levels and their binding proteins in the CSF of these patients. These results are in connection with modern pathophysiology theories and the positive results obtained from new antidiabetic treatments. Therefore, these biomarkers could be a potential clinical tool for the early diagnosis of MCI and AD in the future. We recommend a larger database of clinical trials with more resembling protocols and the creation of banks with the patients’ samples for an easier variables’ stratification to achieve a better understanding of this relationship.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0688r1).