
Abstract
Background:
The uncompetitive NMDA antagonist, memantine (MEM), enhances prepulse inhibition of startle (PPI) across species. MEM is used to treat Alzheimer’s disease (AD); conceivably, its acute impact on PPI might be used to predict a patient’s sensitivity to MEM’s therapeutic effects.
Objective:
To begin to test this possibility, we studied MEM effects on PPI and related measures in AD patients.
Methods:
18 carefully screened individuals with AD (mean age = 72.8 y; M:F=9 : 9) completed double-blind order-balanced testing with MEM (placebo versus 20 mg), assessing acoustic startle magnitude, habituation, PPI, and latency.
Results:
Fifteen out of 18 participants exhibited reliable startle responses. MEM did not significantly impact startle magnitude or habituation. Compared to placebo responses, PPI was significantly increased after MEM (p < 0.04; d = 0.40); this comparison reached a large effect size for the 60 ms interval (d = 0.62), where maximal MEM effects on PPI were previously detected. Prepulses reduced peak startle latency (“latency facilitation”) and this effect was amplified after MEM (p = 0.03; d = 0.41; for 60 ms intervals, d = 0.69). No effects of MEM were detected on cognition, nor were MEM effects on startle associated with cognitive or clinical measures.
Conclusion:
MEM enhances prepulse effects on startle magnitude and latency in AD; these changes in PPI and latency facilitation with MEM suggest that these measures can be used to detect an AD patient’s neural sensitivity to acute MEM challenge. Studies in progress will determine whether such a “biomarker” measured at the outset on treatment can predict sensitivity to MEM’s therapeutic effects.
INTRODUCTION
The uncompetitive NMDA receptor antagonist, memantine (MEM), enhances measures of early auditory information processing, including prepulse inhibition of acoustic startle (PPI), in rodents and humans [1–3]. In humans, MEM increased PPI in both healthy participants (HP) and patients with schizophrenia (SZ) [4]; these effects were particularly robust among older participants in both groups. MEM also has positive and protective effects within early auditory processing circuitry [5, 6], and we reported that MEM enhanced auditory discrimination in both HP and SZ patients [7].
MEM is FDA-approved for the treatment of moderate-to-severe Alzheimer’s disease (AD); in the community, MEM is used more broadly [8]. Benefits of MEM in earlier (mild-moderate) AD are reported in some [9, 10], but not all [11], meta-analyses. While it slows progression of cognitive and behavioral disturbances in AD, this effect can be modest, short-lived, and heterogeneous [12]. Conceivably, the acute effects of MEM challenge, including changes in early auditory information processing, might predict clinical sensitivity to MEM in AD patients. We reported preliminary “proof-of-concept” results, describing an experimental medicine paradigm for using PPI and related measures as potential biomarkers of MEM sensitivity. As part of a planned interim analysis of this protocol, we now report in detail on the effects of initial MEM exposure on PPI and related startle measures in patients with AD.
METHODS
This study was approved by the UCSD Human Subjects IRB (protocol #172053), as part of a longitudinal study of physiological predictors of MEM effects on clinical symptoms in AD. Startle analyses described here were part of a planned interim analysis to confirm expected drug effects. Participants were 61–82 years old with established diagnoses of AD who met inclusion criteria [13] (Supplementary Table 1). Screening included a medical history, establishing course and nature of cognitive and other symptoms, review of systems, current and past medications, audiometry to detect hearing threshold, physical exam, and electrocardiogram. Participants were administered a 2-h battery of commonly used cognitive tests tapping several cognitive domains (i.e., visual and verbal memory, executive function, processing speed, attention, and visuospatial processing), in addition to the Montreal Cognitive Assessment (MoCA) [14], the Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-cog) [15], the Neuropsychiatric Inventory Questionnaire (NPI-Q) [16], and the Geriatric Depression Scale (GDS) [17]. Diagnoses of probable AD dementia were consistent with established criteria [18], based on results from the history, comprehensive neuropsychological assessment, neurologic exam, and brain MRI. Blood was obtained for future genetic analyses including APOE status.
Tests of acute MEM sensitivity followed approximately 7 and 14 days later. Participants arrived at 0800; after a brief review of systems, vital sign check, and standardized breakfast, participants ingested either placebo or MEM (20 mg) in a double blind, pseudorandomized balanced order. Vital signs (blood pressure and heart rate) and symptom ratings were collected at regular intervals. The optimal dose- and time course for MEM effects on specific measures were selected based on past studies in HP and psychiatric patients [2,4,7,19, 2,4,7,19].
At 210 min post-pill, acoustic startle was measured as previously described (e.g., [4]). Participants were seated comfortably with Ag/AgCl electrodes (Sensor Medics) positioned over and lateral to the orbicularis oculi beneath both eyes, and a ground electrode behind the left ear (R < 10 kΩ). Eyeblink magnitude was measured using EMG recordings (San Diego Instruments). EMG activity was band-pass (100–1000 Hz) and 60 Hz notch filtered, digitized, and 250 1 ms readings were recorded starting at startle stimulus onset. The startle test began with 3 min of 70 dB(A) broad band noise, which persisted as a background noise during the test session. A variable inter-trial interval averaged 15 s (range 10–20 s). The session included 42 trials with 6 conditions: a 115 dB(A) 40 ms noise burst (pulse alone) and the same burst preceded 10, 20, 30, 60, or 120 ms by a 20 ms noise prepulse 15 dB over background. To measure startle habituation, 3 pulse alone trials were presented at the session beginning and end.
At 275 min post-pill, neurocognitive testing was completed (Repeatable Battery for the Assessment of Neuropsychological Status (RBANS)) [20]. Electroencephalography (EEG) measures of mismatch negativity, auditory steady state response and excitatory/inhibitory balance will be reported elsewhere. On completing each test day, participants “guessed” whether they received placebo or MEM but were not given feedback.
Statistical analyses
Startle data were analyzed in participants whose mean pulse alone startle magnitude was ≥5 startle units (n = 15); preliminary startle results of 6 participants from this sample were qualitatively described in a “proof of concept” report for this larger clinical trial [13]. Missing startle data (<0.14% of trials) was replaced by the corresponding value from the other eye side. % PPI and % peak latency facilitation were calculated as “100 x (pulse alone value –prepulse trial value) / pulse alone value;” thus, for a pulse alone startle value of 100 units, and a prepulse trial value of 30 units, % PPI=100 x (100–30)/100 = 70.
Startle magnitude, habituation, % PPI, % peak latency facilitation and neurocognitive measures were analyzed by RM-ANOVA, with MEM dose (placebo versus 20 mg) and measure-specific parameters (e.g., prepulse interval) as within-subject factors and sex as a between-subject factor (based on known sex differences in PPI [21]). Exploratory analyses examined impact on MEM-induced startle changes by demographic (age), experimental (pill order), medication (anticholinesterase use, psychotropic medication use, anticholinergic burden [22]), and clinical variables (cognitive deficits and other symptom severity). Alpha was set at 0.05. Effect sizes (Cohen’s d) are provided for relevant comparisons.
RESULTS
All participants (Table 1) were impaired by AD symptoms (MoCA mean 16.4; range: 6–23). Half of the participants (n = 9) were taking an acetylcholinesterase inhibitor (AChE-I; donepezil or galantamine); six participants took antidepressants, and one also took a mood stabilizer.
Participant characteristics (Mean (SEM or range))
* “Mild” = MoCA > 20; “Moderate” = 11-20; “Severe” = MoCA < 10 **1 or more antidepressants (n = 5), antidepressant + mood stabilizer (n = 1) MoCA, Montreal Cognitive Assessment; AChE-I, acetylcholinesterase inhibitor.
Startle data are seen in Fig. 1. Neither startle magnitude, peak latency on pulse alone trials (Fig. 1A) nor reflex habituation (Fig. 1B) were significantly impacted by MEM (pulse alone magnitude: main effect of pill (F = 1.32, df 1,14, ns); peak startle latency: main effect of pill (F = 2.24, df 1,14, ns); habituation: pill x trial block interaction (F < 1)). ANOVA of PPI revealed a significant main effect of pill (F = 5.21, df 1,13, p < 0.04; d = 0.40), no significant main effects of sex (F = 2.19, df 1,13, ns), prepulse interval (F = 1.17, df 4,52, ns) or eye side (F < 1) and no significant 2- or 3-way interactions. Inspection of the data (Fig. 1 C) suggests that MEM effects were most robust at the 60 ms prepulse interval (d = 0.62), as previously reported in other healthy and patient populations [2,4, 2,4]. ANOVA of % latency facilitation revealed significant main effects of pill (F = 5.90, df 1,13, p = 0.03; d = 0.41) and prepulse interval (F = 5.88, df 4,52, p < 0.001), no significant effect of sex or eye side and no significant 2- or 3-way interactions (all ps > 0.25) (Fig. 1D). For 60 ms intervals, MEM-induced increases in latency facilitation reached a large effect size (d = 0.69).
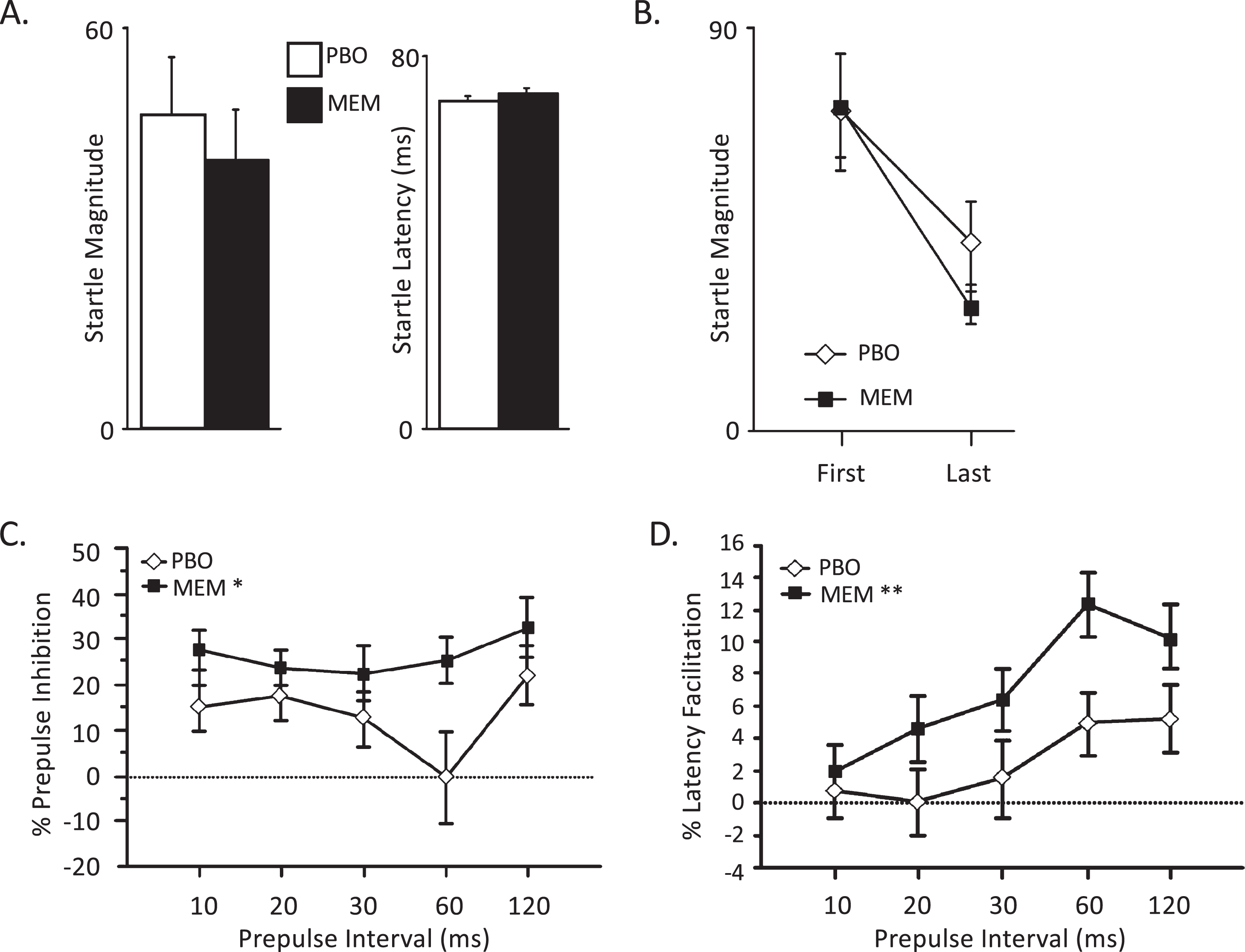
Effects of MEM on startle measures (mean, SEM). A) MEM did not modify startle magnitude or peak startle latency on pulse alone trials. B) There was no significant effect of MEM on startle habituation, based on the decrement of startle magnitude between the first and last blocks of pulse alone trials. C) MEM significantly enhanced PPI across all prepulse intervals (main effect of pill (*p < 0.04)) and no significant pill x interval interaction. D) Similarly, MEM significantly enhanced prepulse effects on peak startle latency (**p = 0.03), with no significant pill x interval interaction.
MEM effects on PPI and latency facilitation were not significantly impacted by pill order, or by use of an AChE-I or other psychotropic agents (Table 2A). No significant correlations were detected between either MEM-enhanced PPI or latency facilitation at the 60 ms interval (MEM minus placebo) and age, anticholinergic burden, or clinical variables (MoCA, ADAS-cog total score, NPI-Q, or GDS) (Table 2B). MEM-enhanced PPI and latency facilitation were also not significantly correlated with each other (r = 0.12, ns).
MEM-enhanced prepulse modification of startle: Potential moderating variables
Correlations (R): Variable versus MEM sensitivity of startle measures at 60 ms intervals
*Spearman Rank Correlation. MEM, memantine; PPI, prepulse inhibition; AChE-I, acetylcholinesterase inhibitor; ACB, anticholinergic burden; ADAS-cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; GDS, Geriatric Depression Scale; NPI-Q, Neuropsychiatric Inventory Questionnaire.
In the full sample (n = 18), MEM did not impact either the RBANS total index score (mean (SEM): placebo = 70.0 (3.8); MEM = 69.3 (4.0); F < 1) or scores across the 5 RBANS domains (main effect of pill: F < 1; pill x domain interaction: F = 1.41, df 4,68, ns).
DISCUSSION
This is a planned preliminary analysis of specific measures of acute MEM sensitivity in AD patients, designed to confirm active dose effects on measures that may ultimately be used to predict clinical sensitivity to MEM [13]. As such, the study design cannot answer questions regarding AD-specific deficits in these measures, or AD-specific effects of MEM on these measures (as there is no direct comparison group of age-matched healthy individuals). The modest preliminary sample size is suboptimal for pursuing subgroup analyses and inter-measure or clinical correlations. The use of only a single active dose of MEM is also a limitation, despite previous studies suggesting that 20 mg is the optimal dose for MEM effects on PPI in HP and SZ patients [2,4, 2,4]. APOE status and other genetic information, which will be available at completion of the clinical trial, might reveal that specific patient subgroups are sensitive to MEM effects on startle modification. Given these limitations, this study identified two effects of MEM on startle-related measures that are worth describing as a basis for confirmatory analyses in a larger cohort.
First, MEM was associated with significant increases in PPI, reaching a large effect size at the 60 ms prepulse interval. This finding extends evidence that MEM enhances auditory sensorimotor gating independent of diagnosis (HP versus SZ versus AD) [2,4, 2,4]; it also suggests that MEM enhances sensorimotor gating not by targeting a source of pathology per se, but instead by acting on healthy circuitry, perhaps relatively early in the auditory system. While 5 years separated our PPI studies in HP and SZ participants [4] versus AD participants (present study), these studies were both conducted in the same facility using the same equipment models, stimulus parameters, session design, MEM dose, test schedule, etc. To the degree that data from these studies can be compared, the magnitude of the PPI-enhancing effects of MEM were evident across all prepulse intervals in patient (SZ or AD) groups versus limited to 60 ms intervals in HP. This temporal pattern and large magnitude of MEM effects on PPI in AD and SZ populations may not entirely reflect features of these disorders per se, but rather may, in part, be a function of lower baseline levels of PPI that allowed more “room” to detect increases; indeed, we reported more robust and interval-independent MEM effects on PPI in HP with lower versus higher baseline levels of PPI [2,4, 2,4]. These patterns are also more consistent with MEM effects on intact neural substrates of PPI, rather than on circuitry that is dysfunctional per se.
Second, MEM significantly enhanced latency facilitation in AD participants. The effects of prepulses on reflex latency are less studied, compared to prepulse effects on reflex magnitude (PPI). The two phenomena are often reported to be independent of one another: many drugs (e.g., dopamine agonists [23]) or disorders (e.g., SZ [24]) that impact PPI are reported to lack effects on latency facilitation. In the present study, MEM effects on PPI and latency facilitation were not correlated within participants, suggesting that these two effects may provide non-redundant information regarding an individual’s neural sensitivity to MEM. Pulse alone reflex latency is reported to be impacted by both disease state and age, with slowed reflex latency reported in patients with SZ [24], Huntington’s disease [25], and AD [26]; reflex slowing also occurs as a function of normal aging [27].
Importantly, in this preliminary sample, MEM’s effects were limited to modifying the impact of prestimuli on startle; it did not significantly impact startle magnitude and latency on pulse alone trials. This suggests that, under the experimental conditions used here, MEM acts within circuitry related to the modulatory effects of the weak prepulse on startle characteristics, rather than circuitry underlying the reflex response to the intense startling pulse. Furthermore, it would be difficult to explain MEM’s effects on prepulse modification of startle, based on a generalized interference with startle behavior per se.
It is worth considering how MEM might increase prepulse effects on reflex amplitude (PPI) and latency (latency facilitation). The degree of magnitude suppression produced by a prepulse is increased by making the prepulse more salient, either by increasing the prepulse intensity (over background), or by directing attention to the prepulse; this latter effect (attentional enhancement) is not evident with discrete prepulses at short prepulse intervals (e.g.,<60 ms). While this has been less studied, prepulse effects on reflex latency also may be increased by making prepulses more salient [28, 29]. Thus, it is conceivable that MEM-enhanced PPI and latency facilitation may reflect drug-induced increases in prepulse salience or detectability. We previously reported that MEM increases electrophysiological measures of early auditory information processing [19] and behavioral measures of auditory discrimination in both SZ patients and HP [7]; in SZ patients, MEM also enhanced auditory discrimination-based learning [7]. There are reports that MEM has either protective or restorative effects on auditory system mechanisms, in structures as distant as cochlea [5] and auditory cortex [6], suggesting that MEM is at least active within brain circuitry associated with early auditory processing. Thus, there is loosely knit but converging evidence that MEM acts within auditory circuitries to produce both neuronal and behavioral evidence of increased auditory stimulus salience and detectability. Whether such effects contribute to its therapeutic impact in AD is not clear, but there are reports that MEM enhances verbal communication in AD and augments the therapeutic impact of auditory-based therapies in AD patients [30–34]; both of these effects might reasonably be ascribed in part to MEM-induced increases in auditory discrimination.
Consistent with our past findings, acute MEM-induced changes in auditory processing after a single dose of MEM are not accompanied by acute gains in neurocognitive performance, as assessed here by the RBANS. This pattern previously led us to propose that changes in early auditory processing must be sustained over time, and perhaps paired with auditory-based learning, in order to effect gains in neurocognition [4, 7]; alternative explanations, including the possibility that specific patient subgroups might show more rapid neurocognitive gains after acute MEM, will be tested when the full study sample has been acquired.
While MEM is active at NMDA receptors, its distinctive preclinical and clinical profile compared to other NMDA antagonists such as ketamine have raised speculation that its primary mechanisms may involve non-NMDA substrates. Interestingly, ketamine also enhances PPI in HP [35, 36], suggesting an area of converging mechanisms for these drugs within PPI-regulatory circuitry. By contrast, ketamine does not appear to alter prepulse latency facilitation [35, 36], though full dose-range effects have not been explored.
A minority (3/18) of participants in this study had “mild” AD (MoCA > 20). Some [9, 10] but not all [11] meta-analyses support the clinical benefits of MEM in cohorts with mild-to-moderate AD, though conceivably, sensitive patients at all levels of illness severity might be identified using “personalized” biomarker strategies. In a large observational study, treatment of mild AD with AChE-Is, with or without MEM, was associated with earlier clinical decline, and patients receiving combined therapy declined even sooner [37]. Despite the interpretative challenges inherent to observational studies, it is important to consider the potential risks associated with the off-label use of MEM in patients with mild AD.
The main scientific limitations of this study are noted above: the lack of a healthy comparison group, a modest study sample, lack of genetic markers and a single active dose of MEM. Despite these limitations, the acute changes identified in PPI and startle latency facilitation after MEM ingestion suggest that these measures can be used to detect an AD patient’s central nervous system sensitivity to acute MEM challenge, and thereby might help predict the patient’s sensitivity to MEM’s therapeutic effects. We will test this hypothesis, as these (and additional) participants complete a 24-week open-label trial of MEM (10 mg bid).
Footnotes
ACKNOWLEDGMENTS
Research was supported by the National Institute on Aging (AG059640) and facilitated by the Shiley-Marcos Alzheimer’s Disease Research Center (National Institute on Aging, P30AG062429). Authors (NRS, YBJ, JS, JLM, GAL) were supported by the VISN-22 Mental Illness Research, Education, and Clinical Center (MIRECC) and the Department of Veterans Affairs Rehabilitation Research and Development Service (IK1 RX003683 (JLM), IK2 RX003395 (YBJ)). Excellent manuscript assistance was provided by Ms. Maria Bongiovanni.