
Abstract
Background:
Coronary atherosclerosis assessed in vivo was associated with cognitive impairment; however, conflicting findings have been reported in autopsy samples.
Objective:
Our aims were to assess the association between atherosclerotic stenosis in the coronary arteries and cognitive impairment and to investigate the possibility of selection bias in an autopsy study.
Methods:
Coronary arteries were collected, and the largest luminal stenosis was measured. Sociodemographic, clinical, and cognitive information were reported by a reliable next-of-kin. The association was tested using logistic and linear regressions adjusted for sociodemographic and clinical variables. We restricted the sample to individuals that were born in 1935 or earlier and stratified the analysis by cause of death to investigate the role of selection bias.
Results:
In 253 participants (mean age = 78.0±8.5 years old, 48% male), stenosis was not associated with cognitive impairment (OR = 0.85, 95% CI = 0.69; 1.06, p = 0.15). In individuals who were born before 1936 in the absence of cardiovascular disease as the cause of death, greater stenosis was associated with cognitive impairment (OR = 4.02, 95% CI = 1.39; 11.6, p = 0.01). On the other hand, this association was not present among those born in 1935 or earlier who died of cardiovascular diseases (OR = 0.83, 95% CI = 0.60; 1.16, p = 0.28).
Conclusion:
We found that higher coronary stenosis was associated with cognitive impairment only in individuals born in 1935 or earlier and who had not died from cardiovascular diseases. Selection bias may be an important issue when investigating risk factors for chronic degenerative diseases in older individuals using autopsy samples.
INTRODUCTION
Coronary heart disease (CHD) is the leading cause of mortality worldwide [1], and it is most commonly due to coronary artery atherosclerosis [2]. At the same time, around 50 million people are living with dementia, and we anticipate about 10 million new cases every year [3]. Dementia is also among the ten most common causes of mortality [4], and it is one of the main causes of disability in older people [5]. Atherosclerosis and dementia share common risk factors, as hypertension [6], dyslipidemia [7], smoking, and diabetes mellitus [8].
Most previous studies have suggested a link between CHD and cognitive impairment. A meta-analysis of cross-sectional, case-control, and cohort studies showed an association of CHD with mild cognitive impairment and dementia only in prospective cohort studies. In these studies, CHD was defined by a combination of a previous diagnosis of myocardial infarction and/or angina pectoris and alterations of laboratory tests and electrocardiogram [9]. On the other hand, coronary artery calcium (CAC) measured by computerized tomography is a quantitative method to evaluate indirectly the subclinical atherosclerosis. CAC was associated with an increased risk of incident dementia, cognitive impairment, and poor performance in cognitive tests [10–12]. However, CAC captures the presence of calcium in the atherosclerotic plaque, which is related to stable and advanced atherosclerotic plaque, and does not necessarily evaluate the artery narrowing [10, 14].
A previous autopsy study with 99 participants showed an association between CHD with AD pathology, mainly in apolipoprotein allele E4 (APOE4) genotype carriers that was independent of other risk factors, such as age and sex [15]. On the other hand, another study found no association between systemic atherosclerosis in the aorta, coronary artery, and intracranial artery with AD pathology. Only cerebral atherosclerosis was associated with an increased dementia risk [16]. Autopsy studies could provide a reliable and less subjective assessment of atherosclerosis due to the possibility of direct arterial measurements when compared to clinical studies. However, previous autopsy studies did not measure coronary atherosclerosis by morphometric methods. One study performed a visual inspection of the artery with the categorization of atherosclerotic plaques into three grades [16] and the stenosis of the coronary artery was not measured in another study [15].
The discrepancy between studies in living persons with autopsy samples could be attributed to issues of measurement or selection biases. Autopsy studies are, by their nature, selected samples. Selection bias could be caused by oversampling of persons with premature mortality due to other mortality causes that compete with the cognitive impairment outcome [17]. Premature deaths due to cardiovascular diseases are a potential selection confounding factor could lead to a false protective effect or absence of association between cardiovascular exposures and cognitive impairment [18]. Analytical strategies are needed to decrease bias. Although some strategies have already been implemented in previous cohort studies, additional strategies should be conducted in cross-sectional studies [12]. Therefore, we aimed to assess the association between morphometric measures of atherosclerosis in coronary arteries and cognitive impairment in an autopsy study and explore the potential impact of selection bias acting on this association.
METHODS
Participants
This study was conducted at the Laboratory of Cardiovascular Pathology and is part of the Biobank for Aging Studies (BAS) collection [19]. Data were collected from 2011 to 2015 at the Sao Paulo Autopsy Service (SPAS), which performs the autopsy on participants who died in Sao Paulo city from non-traumatic and undefined causes of death [20]. The next-of-kin (NOK) signed an informed consent form before the sample collection and the refusal rate in our sample was 14%. The inclusion criteria for this study were individuals aged 65 years or older, postmortem interval less than 24 hours, availability of a NOK who had at least weekly contact with the deceased in the last six months before death, complete cognitive assessment completed by the next-of-kin, and the collection of heart. Exclusion criteria were participants with injuries that occurred close to death that could influence cognitive function (e.g., anoxic encephalopathy) and inconsistent data provided by the NOK during the clinical interview (e.g., inability to answer appropriately) [19]. This study was approved by the local ethics committee and followed the ethical guidelines of the Declaration of Helsinki.
Clinical evaluation
Trained gerontologists administered a semi-structured interview to the NOK. This interview obtained data on the deceased, including sociodemographic information, such as date of birth collected from official governmental document, sex, and race, which was categorized as White and No-White. Education was measured as the number of years of formal education. The clinical information was investigated through previous diagnoses of hypertension, diabetes mellitus, CHD, heart failure, stroke, and dyslipidemia. We investigated the lifestyle factors as binary variables: physical activity was defined as performing domestic, occupational activities, or formal physical exercises at least 3 times per week; current alcohol consumption (yes or no); and smoking (current or previous/never smokers). Body mass index (BMI) was calculated using the direct measures from weight in kilograms and height in meters measured in a supine position, while the deceased have no clothes or shoes before the autopsy exam [21].
Cognitive evaluation
The NOK completed semi-structured questionnaires previously validated for postmortem application [22] to assess cognitive impairment in the deceased, including the Clinical Dementia Rating Scale (CDR) [23, 24] and the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) [25], validated for the Brazilian population [26].
The CDR is a scale used to obtain information on six domains: memory, orientation, judgment and problem-solving, community affairs, home and hobbies, and personal care. The CDR assesses the presence and the stage of dementia, using a point scale distributed as follows: CDR 0 - cognitively normal individuals, CDR 0.5 - questionable dementia, CDR 1, 2, and 3 - mild, moderate, and severe cognitive impairment, respectively [23, 24]. NOK was instructed to answer the CDR and IQCODE questionnaires based on the deceased’s cognitive abilities three months before death to avoid the cognitive impact of the disease that led the individual to death.
In this study, just the informant section of CDR was applied, and cognitive impairment was used as a categorical variable determined by the presence of CDR≥0.5. We also used the CDR scale sum of the boxes (CDR-SB). The CDR-SB score is obtained by summing the score in each of the CDR domains, with the total score ranging from 0 to 18 with higher scores meaning poorer cognitive function [27].
We used the informant-based version of the IQCODE to retrospectively ascertain the change in cognitive and functional performance over a 10-year time period [25, 28]. The full version consists of 26 questions. The questions were answered based on the Likert scale, with five options: 1 –much improved; 2 –a bit improved; 3 –not much change; 4 –a bit worse, 5 –much worse). The IQCODE has 26 questions that have five possible answers on a Likert scale ranging from 1.00 to 5.00. The final IQCODE score was calculated by summing the points for each question and dividing them by the total number of questions that were answered. Higher scores corresponded to greater cognitive impairment.
Coronary artery atherosclerosis evaluation
The heart was collected and washed to remove clots, and then the right coronary artery, left main coronary or left anterior descending artery, and left circumflex arteries were dissected, filled with gelatin solution to prevent arterial collapse, and then fixed in formalin [29, 30]. The arteries were cut transversally at 5 mm-thickness sections, and each segment was evaluated for the presence of atherosclerotic plaques. The segment with the largest obstruction in each coronary was photographed using a camera (Nikon® SMZ 1000) attached to a stereomicroscope (Leica® DMR). The contour of the lumen area and the outer area was determined using the software Image J®. The stenosis of the coronary arteries was calculated by dividing the difference between the outer area and the lumen area by the outer area and multiplied by 100 to obtain the percentage (Fig. 1) [31].
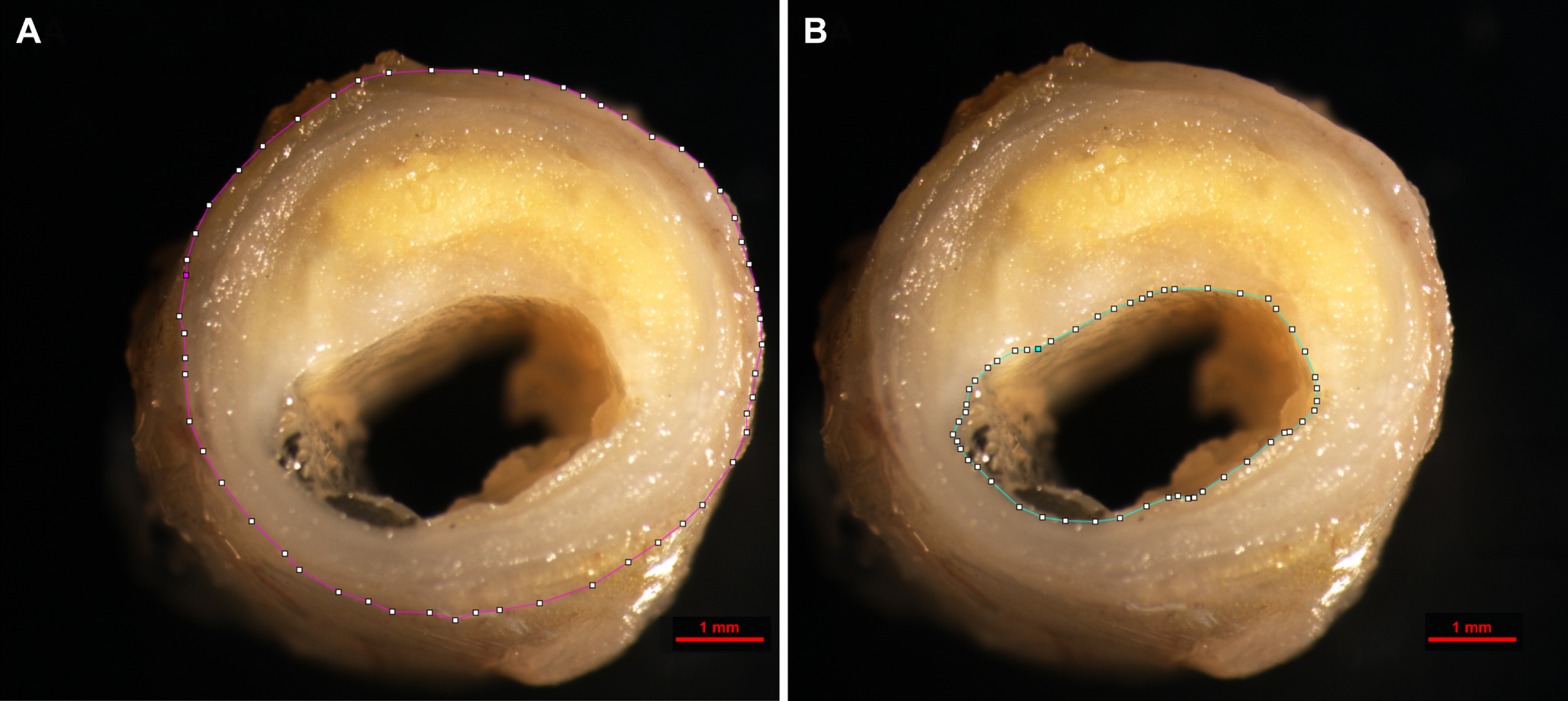
Cross-sectional view of the anterior descending artery. A) Delimitation of the outer border of the artery. B) Delimitation of the lumen of the artery. Source: Laboratory of Cardiovascular Pathology.
Statistical analysis
The characteristics of study participants were described using the mean and standard deviation (SD) or the median and interquartile range (IQR) for continuous variables, and absolute and relative frequencies for categorical variables. The sociodemographic and cardiovascular risk factors were compared across individuals with (CDR≥0.5) and without (CDR = 0) cognitive impairment using unpaired t-test for continuous variables with normal distribution and non-parametric Mann-Whitney test when we had a non-normal distribution. The categorical variables were compared using chi-squared test.
The independent variable was the percentage of stenosis categorized in 10 groups: category 1 = 0 | 10%; category 2=10 | 20%; category 3 = 20 | 30%; category 4 = 30 | 40%; category 5 = 40 | 50%; category 6 = 50 | 60%; category 7 = 60 | 70%; category 8 = 70 | 80%; category 9 = 80 | 90%; and category 10 = 90 | 100%. The dependent variables were cognitive impairment as a binary variable (CDR) and cognitive function as a continuous variable (CDR-SB and IQCODE). We used logistic (cognitive impairment outcome) and linear regression (CDR-SB and IQCODE outcomes) models with robust standard error to account for repeated measures in the same individual (i.e., three coronary artery measurements per person). Regression models were adjusted for age at death, sex, race, education, alcohol use, smoking, physical activity, hypertension, diabetes mellitus, and BMI.
To explore the role of selection factors, we restricted the sample to individuals that were born in 1935 or earlier and stratified all analyses by whether the deceased had a cardiovascular cause of death. Restriction to those born in 1935 or earlier allowed us to consider a sample that was not enriched in those with premature death (and associated risk factors), and which was composed of older adults who experienced similar environmental risk factors in a similar time period [32]. Stratified analysis by cardiovascular disease as the cause of death allowed us to consider whether selection into the autopsy sample based on cardiovascular death could have biased study results [33]. We considered a 5% level of significance in two-tailed tests. All analyses were performed using STATA 13 (StataCorp., College Station, TX, USA).
RESULTS
The final sample consisted of 253 participants with a mean age was 78.0 (SD 8.5) years old; 48% were male, 65% were white, and 77% had 0 to 4 years of education. Cognitive impairment, defined as CDR≥0.5 was present in 31%. Compared to participants without cognitive impairment, participants with cognitive impairment were older and more likely to be women, were more physically inactive, and had lower values of BMI. Individuals without cognitive impairment presented more hypertension, previous history of CAD, and current smoking (Table 1). Among 128 participants who were born in 1935 or earlier, the mean age was 85 (SD 5.2) years old, 46% presented cognitive impairment, hypertension was less prevalent, BMI was lower, and physical inactivity was more frequent among participants with cognitive impairment (Supplementary Table 1).
Description of the clinical variables of the study participants (n = 253 participants)
CDR, Clinical Dementia Rating scale; IQCODE, Informant Questionnaire on Cognitive Decline in the Elderly; CVD, cardiovascular disease; CAD, coronary artery disease; SD, standard deviation; IQR, interquartile range; BMI, body mass index. *Comparison of social and clinical variables between groups: CDR = 0 and CDR≥0.5; at-test; bchi-squared; cMann-Whitney test.
In adjusted models, stenosis was not associated with cognitive impairment in either the total sample (OR = 0.85 per 10% increase in stenosis, 95% CI = 0.69; 1.06, p = 0.15) or in individuals who were born in 1935 or earlier (OR = 0.95, 95% CI = 0.73; 1.24, p = 0.73). Coronary stenosis was not associated with CDR-SB in the total sample (β=–0.39, 95% CI=–0.89; 0.09, p = 0.11) and among individuals born in 1935 or earlier (β=–0.26, 95% CI = –1.01; 0.48, p = 0.48). Similarly, there was no association between stenosis and IQCODE in the total sample (β=–0.04, 95% CI = –0.09; 0.01, p = 0.11) and among individuals born in 1935 or earlier (β=–0.03, 95% CI = –0.11; 0.04, p = 0.38) (Table 2).
Association between dementia, CDR Box Sum, IQCODE, and stenosis in coronary arteries
CDR, Clinical Dementia Rating scale; IQCODE, Informant Questionnaire on Cognitive Decline in the Elderly; OR, odds ratio; CI, confidence interval. *Logistic regression with robust SEs to account for repeated measures in the same individual through cluster adjustment. **Linear regression with robust SEs to account for repeated measures in the same individual through cluster adjustment. a Adjusted for age, sex, race, education in years, alcohol use, smoking, physical inactivity, hypertension, diabetes mellitus, and body mass index.
Although the average age at death was similar between cardiovascular and other causes of death in the whole sample (p = 0.19) and both birth cohorts (1935 or earlier: p = 0.54 and before 1935: p = 0.41) (Supplementary Table 2), there was an excess of deaths by CVD, which is three times more frequent (75%) than death by other causes (25%). Deaths by CVD were also highly correlated with coronary stenosis (Supplementary Table 3) and with cognitive impairment, especially in those born after 1935 (p = 0.03). After selecting only participants who were born in 1935 or earlier because they survived premature deaths due to cardiovascular diseases, we observed the loss of significance between death from cardiovascular disease and the cognitive impairment (p = 0.46, Supplementary Table 4). Therefore, the excess of death by CVD is a potential source of selection bias. After stratifying the sample by cause of death, we found that among participants that died from cardiovascular causes, a higher stenosis was related to a better cognitive function defined by lower scores in the CDR-SB (β=–0.67, 95% CI = –1.28; –0.06, p = 0.03) and IQCODE (β=–0.07, 95% CI = –0.13; –0.005, p = 0.03), while we did not find any association among those who did not die from cardiovascular disease and in stratified analysis by the presence of cognitive impairment (Table 3). After restricting to individuals born in 1935 or earlier that died from cardiovascular disease, we found a borderline protective association between stenosis and CDR-SB (β=–0.83, 95% CI = –1.76; 0.09, p = 0.07) and IQCODE (β=–0.09, 95% CI = –0.19; 0.01, p = 0.07). On the other hand, in individuals who were born in 1935 or earlier in the absence of cardiovascular disease as the cause of death, higher stenosis was associated with 4-fold increased risk of cognitive impairment (OR = 4.02, 95% CI = 1.39; 11.6, p = 0.01), and poorer cognitive function defined by higher CDR-SB scores (β=1.19, 95% CI = 0.09; 2.29, p = 0.03) while no association was observed with IQCODE scores (β= 0.09, 95% CI=–0.02; 0.21, p = 0.12) (Table 3).
Association between dementia, CDR Box Sum, IQCODE, and stenosis in coronary arteries stratified by cardiovascular disease as the cause of death
CDR, Clinical Dementia Rating Scale; IQCODE, Informant Questionnaire on Cognitive Decline in the Elderly; OR, odds ratio; CI, confidence interval; CVD (+), presence of cardiovascular disease; CVD (-), absence of cardiovascular disease. *Logistic regression with robust SEs to account for repeated measures in the same individual through cluster adjustment. **Linear regression with robust SEs to account for repeated measures in the same individual through cluster adjustment. aAdjusted for age, sex, race, education in years, alcohol use, smoking, physical inactivity, hypertension, diabetes mellitus, and body mass index.
DISCUSSION
In this autopsy study, coronary atherosclerotic stenosis was not associated with cognitive impairment and related daily functioning in the whole sample. However, in individuals who were born in 1935 or earlier, in the absence of cardiovascular disease as the cause of death, higher stenosis was associated with higher odds of cognitive impairment and poorer cognitive function. On the other hand, in individuals who died from cardiovascular causes, higher stenosis was related to better cognitive function in both the total sample and when restricted to those born in 1935 or earlier.
We hypothesized that a higher coronary atherosclerotic stenosis would be associated with cognitive impairment as shown in a previous meta-analysis from cohort studies [9, 34] and in an autopsy-based study that showed an association between with AD-associated neuropathology, mostly in APOE4 genotype carriers [15]. However, our findings were in line with Dolan et al. [16] that found no association of the degree of atherosclerosis in coronary, carotid, and cerebral arteries with the degree of Alzheimer’s type pathology.
However, the results of autopsy analyses are dependent on the autopsy sample. Autopsied participants may not be representative of the target population and can yield biased results. Beeri et al. [15] found an association between CAD with Alzheimer’s disease pathology; however, the studied sample had only 99 brains. Of those 42 were APOE4 carriers and the majority were institutionalized women (82%) that are known risk factors for cognitive impairment. APOE4 carriers probably had more chances to develop cognitive impairment before death, counteracting the effect of selection bias in this study [35]. On other hand, Dolan et al. [16] did not find associations between atherosclerosis with Alzheimer’s disease in a well-educated sample (mean education of 17.1±3.9 years), which is considered a protective factor [3]. Our sample was more balanced concerning sex and education distribution, avoiding these possible biases. The lack of association in our first result, even after careful statistical analysis and accurate direct morphometric measurements of atherosclerosis could be explained by selection bias, which was frequent in investigations about the association between cardiovascular and neurodegenerative diseases [17, 18]. The excess of CVD deaths in younger participants led to selection bias in our study. However, stratifying the sample by cardiovascular and non-cardiovascular cause of death without the birth cohort restriction would lead to a spurious protective association. We found that higher coronary stenoses were associated with a better cognitive function in those that died from cardiovascular disease. This finding could be related to the fact that participants who died from cardiovascular causes died at a younger age than those who die from other causes is lower than other death causes and they were too young for having a high risk to have cognitive impairment. The arbitrary cutoff of age at 80 years old at 2015, which was the last year of our sample collection, was done to restrict the sample to older adults that survived premature death by cardiovascular disease. In the group that was born in 1935 or earlier and did not die from cardiovascular disease, an increase in coronary stenosis was related to cognitive impairment and worse cognitive function, as expected. These findings are probably related to survival bias since participants with high atherosclerotic stenosis are more likely to die before they can develop cognitive impairment, as shown previously in studies related to cancer and dementia [36, 37]. Death from cardiovascular disease may be acting as a collider since dementia [38] and higher coronary stenosis may both lead to death [33, 39]. The association between coronary stenosis with poor cognitive function was found for CDR-SB, but not for the IQCODE. Differences in the pattern of associations may be due to the differences in range and scale in the two questionnaires, the CDR-SB ranges from 0 to 18, while the IQCODE ranges from 1.00 to 5.00, which gives more power to analyses that have the CDR-SB as the outcome. Moreover, the two questionnaires measure different constructs related to cognitive impairment. The CDR is used to determine the presence and severity of dementia, while IQCODE evaluates cognitive decline when comparing current cognitive abilities related to 10 years ago [40, 41]. The linear regression coefficients represent the average increase or decrease in the CDR-SB or IQCODE scores for each 10% increase of stenosis.
The full-body autopsy allows the determination of the accurate cause of death. Furthermore, the autopsy is an important tool to study risk factors for cognitive change since a full-body autopsy exam allows for direct and reliable measurements of tissue damage [42, 43]. For example, the assessment of atherosclerosis in vivo is based on calcification measured by computerized tomography. However, calcification assessed by CAC is useful to detect stable and advanced atherosclerotic plaque and does not necessarily evaluate the arterial narrowing, because other atherosclerotic plaque components were not evaluated by this imaging method [44]. On the other hand, the autopsy exam allows studying other components of the atherosclerotic plaque.
The association between coronary artery atherosclerosis and cognitive impairment could be explained by different mechanisms [10, 12]. Coronary atherosclerosis could be a marker of intracranial cerebral atherosclerosis [45], which could be the cause of vascular dementia and may also be related to amyloid pathology as a result of amyloid-β accumulation and impaired amyloid-β clearance [46]. Another mechanism could be chronic cerebral hypoperfusion due to a narrowing of the coronary arteries, leading to reduced cardiac output, and consequently lower brain blood flow, leading to impaired cognitive function [47].
Our study has some limitations. This cross-sectional study does not allow establishing causal inference. Moreover, the cognitive assessment was based on postmortem information collected from the next-of-kin. Although this approach has been validated [22] and applied in several studies [48, 49], a pre-morbid assessment would be preferable. Furthermore, as neuropathological assessment was not performed at this time, we were not able to analyze the association of coronary atherosclerosis with the neuropathology of Alzheimer’s disease or vascular dementia. Although we included education in our adjusted analyses, other measures of socioeconomic status were not collected in our study and residual confounding may be present in our study. Additionally, we were unable to collect clinical and sociodemographic data from those who refused to participate in the study, which did not allow us to compare excluded individuals with study participants. The main strengths of this study are the direct anatomic measurement of the atherosclerotic plaque, instead of symptoms-based diagnosis, and the determination of causes of death by full-body autopsy.
In conclusion, this study showed no association between coronary stenosis and cognitive impairment. Larger coronary atherosclerosis was associated with cognitive impairment only in individuals born in 1935 or earlier without cardiovascular disease as cause of death. In the presence of cardiovascular disease as cause of death, the association tends to be protective. Autopsy-based studies have a selection pressure about who gets into autopsy sample that can change the results significantly, and the result may be biased concerning the target population of interest. Cardiovascular disease as the cause of death is an important factor related to selection bias since these participants are more likely to die before developing cognitive impairment. Aging research is a challenge, and it is important to be aware of methodological problems in studies about chronic degenerative diseases. Further longitudinal studies with longer follow-up and methodological approaches to control for selection bias will be important to assess whether coronary atherosclerosis is a risk factor for cognitive impairment.
Footnotes
ACKNOWLEDGMENTS
The authors acknowledge the staff of the Sao Paulo Autopsy Service and the Biobank for Aging Studies.
FUNDING
This study received a grant (AARG-20-678884) from Alzheimer’s Association; CKS received a grant (2013/00335-2; 2017/11313-0) and DSF-I received a scholarship (2013/12290-3;2017/24066-1) from Sao Paulo Research Foundation (FAPESP).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data associated with the paper are not publicly available but are available from the corresponding author on reasonable request.