
Abstract
Background:
The Cognitive role of untreated type 2 diabetes mellitus (T2DM) has been less well substantiated.
Objective:
We sought to explore the prospective association of T2DM and untreated T2DM with cognitive function among middle-aged and older Chinese adults.
Methods:
Data of 7,230 participants without baseline brain damage/mental retardation, or memory-related diseases in China Health and Retirement Longitudinal Study (CHARLS) from 2011– 2012 to 2015, were analyzed. Fasting plasma glucose and self-reported information on T2DM diagnosis and treatment were assessed. Participants were categorized into normoglycemia, impaired fasting glucose (IFG), and T2DM (including untreated and treated T2DM) groups. Episodic memory and executive function were assessed by modified Telephone Interview for Cognitive Status every two years. We used generalized estimating equation model to examine the association of baseline T2DM status with cognitive function in succeedingyears.
Results:
Compared to those with normoglycemia, T2DM was associated with worse overall cognitive function after controlling for demographic variables, lifestyles, follow-up time, major clinical factors, and baseline cognitive function, although the associations were statistically non-significant (β= –0.19, 95% CI: –0.39, 0.00). However, a significant association was mainly observed for those with untreated T2DM (β= –0.26, 95% CI: –0.47, –0.04), especially in the domain of executive function (β= –0.19, 95% CI: –0.35, –0.03). In general, IFG and treated T2DM individuals had similar levels of cognitive function with normoglycemia participants.
Conclusion:
Our findings supported a detrimental role of untreated T2DM on cognitive function among middle-aged and older adults. Screening and early treatment for T2DM are warranted for maintaining better cognitive function in later life.
Keywords
INTRODUCTION
With rapid aging of the global population, the number of older adults who suffer from cognitive impairment, Alzheimer’s disease (AD), and other types of dementia are rising dramatically [1]. According to the 2020 World Health Organization Dementia Report, the world population with dementia is projected to be 82 million by 2030, and 152 million by 2050 [2]. These situations lead to direct increases in medical expenses, as well as indirect financial, physical, and psychological care-related burdens.
Despite tremendous progress in detecting and treating type 2 diabetes mellitus (T2DM) in the past two decades, T2DM is still expected to become an expanding global epidemic due to the alarming growth rate of both diagnosed and undiagnosed T2DM [3, 4]. Especially in China, there is a high proportion of undetected prediabetes and T2DM cases due to the lack of population-wide screening programs [5, 6]. Furthermore, suboptimal glucose control in adults with T2DM is a growing challenge in diabetes care [7]. A recent nationally representative survey in China reported that only 32.9% of diabetes participants were being treated, and 50.1% of them were controlled adequately [8].
Several biological and epidemiological studies have suggested that T2DM is a significant risk factor for cognitive impairment and dementia in late-life due to the direct effect of hyperglycemia or its associated comorbidities [9–13]. A meta-analysis of previous prospective studies showed that T2DM conferred a 25–91% higher risk of cognitive disorders (cognitive impairment and dementia) [14]. Most previous epidemiological studies mainly focused on defining the increased risk of cognitive disorders associated with the diagnosis or presence of T2DM among older adults [15]. To date, the potential cognitive role of untreated T2DM, in middle-aged and older adults is less well understood.
To address this research gap, we investigated the association of T2DM and untreated T2DM with cognitive function in the China Health and Retirement Longitudinal Study (CHARLS), a prospective cohort study among Chinese middle-aged and older adults.
MATERIALS AND METHODS
Study design
We utilized the CHARLS data, a nationally representative longitudinal survey of Chinese adults aged 45 years and older. Briefly, between June 2011 and March 2012, 17,708 respondents were recruited at baseline. Standard study follow-ups were conducted every two years up to 2015, using a face-to-face computer-assisted personal interview (CAPI) for updated information on cognitive function, social, economic, lifestyle, and health circumstances [16, 17]. Ethics approval for CHARLS was obtained from the Biomedical Ethics Review Committee of Peking University (IRB00001052-11015). All participants provided signed informed consent. For this study, we first included 11,368 participants with information on plasma glucose and self-reported T2DM at the study baseline. Participants without baseline data on cognitive function (n = 2,199), aged <45 years (n = 198), and with brain damage/mental retardation, or memory-related disorders (n = 313) were excluded. Participants were also excluded if they were without any data on cognitive function during follow-ups (n = 1,428). A total of 7,230 participants were included in the final analysis, of whom 6,423 and 6,164 participants had cognitive assessments at two and four years of follow-up, respectively (Fig. 1).
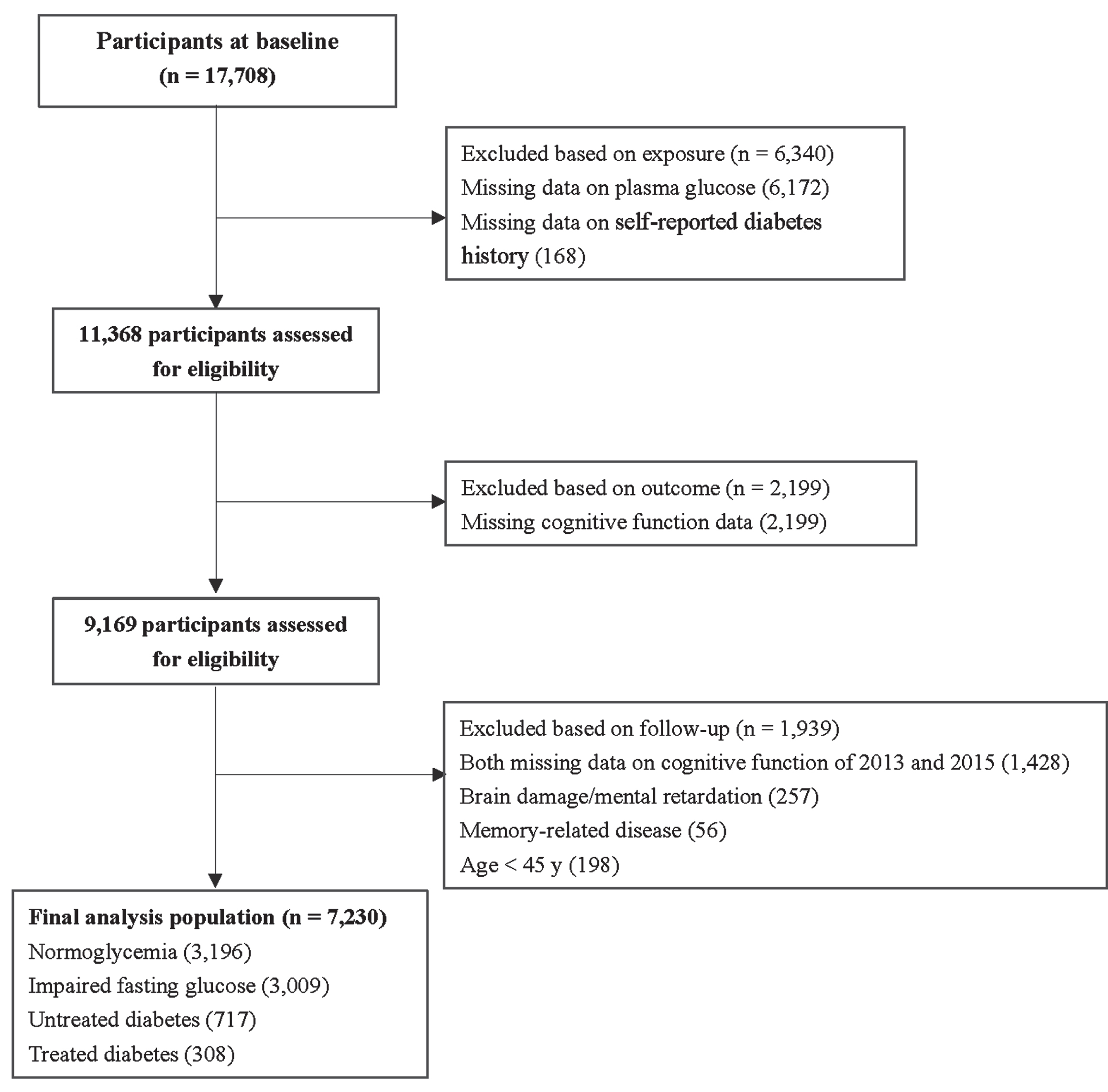
Flow chart of the study population.
T2DM assessment
We categorized the study participants as T2DM (including treated T2DM or untreated T2DM), impaired fasting glucose (IFG), and normoglycemia using a combined criterion of fasting plasma glucose (FPG) concentrations, self-reported diagnosis of T2DM, and treatment history. Participants’ baseline FPG was measured by an enzymatic colorimetric test method. Participants with self-reported diabetes and who received diabetes treatment were defined as the treated T2DM. For diabetes treatment, participants were asked, ‘Are you now taking any of the following treatments to treat or control your diabetes? (Check all that apply)’ with multiple choices including ‘taking Chinese traditional medicine’, ‘taking Western modern medicine’, ‘taking insulin injections’, and ‘none of the above’ [18]. Those without self-reported diabetes but meeting the American Diabetes Association (ADA) diabetes criteria (FPG ≥126 mg/dL [7.0 mmol/L]) or participants with a diabetes history but without corresponding treatment were classified as the untreated T2DM. And those without self-reported diabetes were classified as IFG if their FPG was between 100 mg/dL (5.6 mmol/L) and 125 mg/dL (6.9 mmol/L), otherwise as normoglycemia [19]. A high level of specificity (98.6%) and a relatively moderate sensitivity (41.5%) were reported in a previous validation study for self-reported diabetes in the CHARLS participants [20].
Assessment of cognitive function
Cognitive function was assessed by the modified Telephone Interview for Cognitive Status (TICS) approach, which has been reported as a validated and utilizable cognitive function assessment tool for Chinese adults with different educational levels [21]. Briefly, at baseline and each visit, two dimensions, including executive function and episodic memory, were evaluated [21]. Executive function was adopted to assess numerical ability (serial subtraction of seven from 100 for five times), time orientation (week, month, day, season, and year), and picture drawing (intersecting pentagon copying test). The answers to these questions were accumulated into a score ranging from zero to 11 points [17]. Episodic memory was measured by the average number of immediate and delayed word recall ranging from zero to 10. Immediate recall referred to asking the participants to immediately recall as many words as they could after interviewers read a list of 10 Chinese nouns. Delayed recall referred to asking the participants to recall the same five minutes later [17]. The overall cognitive function score was the sum of these two dimensions, ranging from zero (worst cognitive function) to 21 (best cognitive function) [22].
Assessment of other covariates
We included the following baseline characteristics as covariates based: sociodemographic factors, i.e., age, sex, educational levels, marital status; and depressive symptoms, lifestyle factors, i.e., physical activity, smoking status, alcohol consumption, and sleep duration during the night; and health conditions, i.e., body mass index (BMI) and history of major chronic diseases (hypertension, dyslipidemia, stroke, heart disease, and cancer).
Baseline BMI (kg/m2) was calculated as weight in kilograms divided by height in meters squared. According to World Health Organization (WHO) recommendation for Chinese people, BMI was classified into four categories: underweight (<18.5 kg/m2), normal weight (18.5–23.9 kg/m2), overweight (24.0–27.9 kg/m2), and obesity (≥28.0 kg/m2) [23]. Depressive symptoms were measured using the 10-item version of the Center for Epidemiology Studies Depression Scale (CEDS-10) [24], and CEDS-10 score ≥12 was used to identify the respondents with depressive symptoms [25].
Statistical analysis
We described and compared baseline characteristics by T2DM status using means and standard deviations (SD) for continuous measures and numbers (proportions) for categorical measures. Significant differences across different T2DM statuses were compared using chi-square test for categorical variables. For continuous variables, statistical analysis of different parameters in four groups was carried out by one-way analysis of variance (ANOVA) followed by Tukey-Kramer multiple comparison post hoc test. We used the Generalized Estimating Equation (GEE) model to estimate the association between baseline T2DM status and cognitive function in the following four years. Three multivariable-adjusted models were constructed to account for potential confounding. Model 1 adjusted for follow-up time, age (years), age2, sex (women or men), educational level (illiterate, primary school, middle school, or high school or above), and marital status (married or other). Model 2 further adjusted for BMI (<18.5, 18.5–23.9, 24–27.9, or ≥28.0 kg/m2), depressive symptoms (yes or no), smoking status (non-smokers, ex-smokers, or current smokers), drinking status (never drank, abstainers, or current drinkers), physical activity (none, mild, moderate, or vigorous), sleep duration (≤5, 5.1–6, 6.1–7, 7.1–8, and >8 h), hypertension (yes or no), dyslipidemia (yes or no), stroke (yes or no), heart disease (yes or no), and cancer (yes or no). Model 3 (fully adjusted model) added adjustment for baseline cognitive function.
Stratified analyses were conducted across subgroups of sex (women or men), age (45–59 or ≥60 years), educational level (primary school/below or junior high school/above), smoking status (never or former/current), drinking status (never or former/current), BMI (<24 or ≥24 kg/m2), depressive symptoms (yes or no), and history of major chronic diseases (yes or no). To further address potential reverse causation, we conducted sensitivity analyses by excluding participants with extremely low overall cognitive function scores at baseline (<mean - 2sd). Given that the educational level, especially illiteracy, may influence the accuracy of cognitive assessment, we also performed additional sensitivity analysis after excluding participants who were illiterate. To further assess the associations of diabetes treatment on cognition, we conducted another sensitivity analysis by using HbA1c to categorize glycemic control status among participants with treated T2DM. Controlled T2DM was defined as treated T2DM individuals with an HbA1c concentration of less than 7.0% [8, 12]. Additionally, to further control for the potential confounding of restrictions on activities of daily living (ADL), we performed sensitivity analyses with additional adjustment for ADL (zero or≥one). All analyses were conducted using Stata version 15 (Stata Corp, College Station, TX). All reported p values were two-tailed, with a significance level of 0.05.
RESULTS
The baseline characteristics of the overall study population and T2DM status were shown in Table 1. Among 7,230 participants (mean age of 58.06±8.21 years), 48.85% were men, and over half of them only accepted primary school or lower education (64.89%). On average, compared with normoglycemia, participants with T2DM were slightly older, more likely to be overweight and obese. They were more likely to have hypertension, heart disease, stroke, and dyslipidemia. The mean (SD) duration of T2DM in treated T2DM participants and untreated T2DM participants were 5.41 (4.67) and 2.90 (4.71) years, respectively. Compared to participants with treated T2DM, those with untreated T2DM were less likely to be overweight and obese, and more likely to be current smokers and current drinkers.
Baseline characteristics of participants overall and by T2DM status (n = 7,230)
Participants with diabetes history and who received diabetes treatment were defined as treated diabetes. Those without diabetes history, who met the American Diabetes Association (ADA) criteria for diabetes (FPG ≥126 mg/dL [7.0 mmol/L]) or who had diabetes history but not received treatment were classified as untreated diabetes. No diabetes history participants were classified as IFG if their FPG was between 100 mg/dL (5.6 mmol/L) and 125 mg/dL (6.9 mmol/L), otherwise were classified as normoglycemia. aPost-hoc comparisons were performed to examine characteristics among four T2DM groups. Significant differences between normoglycemia and impaired fasting glucose: ***P < 0.001, **P < 0.01, *P < 0.05; normoglycemia and untreated T2DM: +++P < 0.001, ++P < 0.01, +P < 0.05; normoglycemia and treated T2DM: AAAP < 0.001, AAP < 0.01; AP < 0.05.
In the multivariable models adjusted for follow-up time, sociodemographic factors, health conditions, and lifestyle factors, participants with T2DM had a lower cognitive function score during four years’ follow-up (β= –0.23, 95% CI: –0.44, –0.03). These associations were slightly attenuated and became non-significant after further adjustment for baseline cognitive function (β= –0.19, 95% CI: –0.39, 0.00) (Table 2). After dividing T2DM participants into treated and untreated T2DM groups, a stronger association was mainly observed for participants with untreated T2DM (β= –0.26, 95% CI: –0.47, –0.04). In contrast, individuals with IFG (β= –0.04, 95% CI: –0.17, 0.09) and treated T2DM (β= –0.03, 95% CI: –0.36, 0.30) had similar cognitive performance with normoglycemia participants.
Association between T2DM status and overall cognitive function (n = 7,230)
The mean differences (β) and 95% confidence intervals (CIs) of overall cognitive function according to T2DM status were listed. Model 1: Adjusted for follow-up time, age, age2, sex, educational level, and marital status; Model 2: Adjusted for covariates in Model 1 + body mass index, depression symptom, smoking status, drinking status, physical activity, sleep duration, hypertension, dyslipidemia, stroke, heart disease, and cancer; Model 3: Adjusted for covariates in Model 2+ baseline cognitive function (binary). Data with P-value below 0.05 are presented in bold type.
In the fully adjusted models for the cognitive subdomain, compared with the normoglycemia group, the corresponding level of difference in executive function were –0.11 (95% CI: –0.25, 0.04) for T2DM and –0.19 (95% CI: –0.35, –0.03) for untreated T2DM, respectively (Table 3). In contrast, non-significant associations were found for episodic memory between treated T2DM and cognitive performance (β= –0.14, 95% CI: –0.30, 0.01) (Table 3).
Association between T2DM status and executive function and episodic memory (n = 7,230)
The mean differences (β) and 95% confidence intervals (CIs) of executive function and episodic memory according to T2DM status were listed. Model 1: Adjusted for follow-up time, age, age2, sex, educational level, and marital status; Model 2: Adjusted for covariates in Model 1 + body mass index, depression symptom, smoking status, drinking status, physical activity, sleep duration, hypertension, dyslipidemia, stroke, heart disease, and cancer; Model 3: Adjusted for covariates in Model 2+ baseline cognitive function (binary). Data with P-value below 0.05 are presented in bold type.
In the stratified analyses, we found no statistical evidence that the longitudinal association between untreated T2DM and cognitive function was modified by sex, age, educational level, smoking status, drinking status, BMI, depressive symptoms, and history of major chronic diseases (Fig. 2, Supplementary Table 1). In general, although we did not observe statistically significant effect modification by educational levels in the stratified analyses (p-interaction = 0.735), a lower level of cognitive function associated with untreated T2DM was observed among participants with low education level (primary school education or below, β= –0.31, 95% CI: –0.60, –0.04). Additional sensitivity analyses were overall consistent with the primary analysis. In an attempt to adjust for ADL, we observed similar associations between T2DM and overall cognitive performance (Supplementary Table 2). After eliminating 213 participants with extremely low scores in overall cognitive function at baseline (<mean - 2sd), the association was nonsignificant for general cognitive function scores (βuntreatedT2DMvs . normoglycemia = –0.20, 95% CI: –0.42, 0.02) (Supplementary Table 3). The results of sensitivity analysis were similar to the main analysis when excluding 1,648 participants who were illiterate (Supplementary Table 4). For glycemic control status, non-significant associations were observed (Supplementary Table 5).
DISCUSSION
In this prospective cohort of 7,230 Chinese middle-aged and older adults followed up to four years, we observed that participants with untreated T2DM had worse overall cognitive performance than the normoglycemic group. Furthermore, significant inverse associations were mainly observed in the domain of executive function. Individuals with IFG and treated T2DM had similar levels of cognitive function with normoglycemia participants.
Several epidemiological studies across different world regions have studied the association between T2DM and cognitive function. A meta-analysis pooling 144 prospective studies with almost one million participants summarized a positive association between T2DM and cognitive decline; they reported about a 25% higher risk of global cognitive decline (RR = 1.25, 95% CI: 1.12, 1.39), a 44% elevated risk of executive function decline (RR = 1.44, 95% CI: 1.23, 1.69), and a 27% increased risk for memory function impairment (RR = 1.27, 95% CI: 1.16, 1.39) among T2DM populations [14]. Consistent with the findings from these studies, we observed marginal significant lower global cognitive function among T2DM participants compared with normoglycemia participants. Furthermore, our study divided T2DM participants into untreated and treated T2DM with consideration of the role of T2DM treatment. Compared with the normoglycemia group, the worse overall cognitive function in untreated T2DM patients was observed. Our observations were in line with previous studies suggesting that T2DM patients with poorer glycemic control had faster cognitive decline (n = 5,653 with ten years of follow-up) [26]. Another study of 457,902 UK adults aged ≥50 years and followed for a median of six years, also showed that poorly controlled diabetes (hemoglobin A1c,HbA1c, >7%) was associated with increased dementia risk [27]. Our results extended and refined evidence of the detrimental role of T2DM and untreated T2DM in cognitive performance in a nationally representative cohort in China, a country with the most T2DM patients worldwide.

Difference in cognitive function for untreated diabetes compared with the normoglycemia in fully adjusted models. The mean differences (β) and 95% confidence intervals (CIs) of overall cognitive function for untreated diabetes and normoglycemia were listed. All models were adjusted for follow-up time, age, age2, sex, educational level, and marital status, body mass index, depression symptom, smoking status, drinking status, physical activity, sleep duration, hypertension, dyslipidemia, stroke, heart disease, and cancer, and baseline cognitive function (binary).
When investigating the associations in different domains of cognitive function, we observed significant inverse associations between untreated T2DM and executive function. These findings were in general consistent with previous evidence [28, 29]. The detrimental associations with executive function could be partially explained by the higher risk of small-vessel disease among T2DM individuals, which has been shown to impair prefrontal cortex processing tasks such as executive function [30, 31]. In addition, untreated T2DM participants may have poorer levels of glycemic control and therefore more likely to have worse executive function. In terms of episodic memory, a non-significant association was observed in untreated T2DM. To date, limited studies have investigated the potential associations between glycemic control levels and cognitive domains. Taken together, these findings heightened the need for further studies on glucose control status and different domains of cognitive function.
Compared with untreated patients, treated T2DM were less likely to be smokers and drinkers. The possible explanation could be that treated T2DM patients were more likely to receive medical advice to adopt healthier behaviors for disease management after diagnosis [32, 33]. In addition, treated T2DM participants were more likely to be older thus may be prone to be overweight and obese and have other types of comorbidities. Notably, underdiagnosis and suboptimal practice of diabetes treatment are potential issues among adults in China. At the baseline of the current study, 14.18% of the participants had diabetes. Among them, only 39.90% of T2DM patients had been previously diagnosed, and only 30.05% of those diagnosed ones were being treated, which was similar to those reported in previous nationally representative cross-sectional studies [8, 12]. For treated T2DM, we did not observe significant differences in the overall performances of cognitive function compared with normoglycemia, potentially due to the relatively small sample size of treated T2DM. Taken together, our findings reinforce the need for regular screening, early diagnosis, and effective management and treatment to reduce the risk of cognitive impairment among T2DM individuals.
Suggested potential pathophysiological mechanisms involved in this association are accelerated cerebrovascular disease, accumulation of advanced glycation endproducts (AGEs), and reduced amyloid-β clearance through disturbing the role of the insulin-degrading enzyme [33–35]. Hyperglycemia is associated with cerebral microvascular and macrovascular damage, indirectly affecting cognition [36]. Chronic hyperglycemia could also cause cognitive impairment by direct neuronal damage, possibly by AGEs. A previous study reported that patients with AD had higher brain concentrations of AGEs, such as pyraline and pentosidine, compared to normal controls [37]. Finally, the discovery of insulin-degrading enzyme amyloid-β clearance from previous research suggested that the hypofunction of this enzyme could be linked to the development of AD directly [38].
The present study has several strengths. CHARLS provides nationally representative longitudinal data of the Chinese population [16]. Moreover, strict quality control and quality-assured measures had been implemented at each stage of the CHARLS research, providing a high-standard database with a wide range of information. In addition, our findings extended and refined additional evidence from preceding research because only a limited number of studies have focused on T2DM treatment and cognitive function. However, several limitations need to be addressed. First of all, given that the T2DM diagnosis information was based on self-reports, there may be an underestimation of people with T2DM [39]. However, the combined criterion of FPG, self-reported diabetes, and treatment history were used to categorize the T2DM status. Secondly, the level of plasma glucose was measured only once during the study period. Thus, measurement error was inevitable. However, since all blood glucose measurements in our study were conducted at Capital Medical University laboratory, protocols for quality control were the same. Moreover, plasma glucose was measured before cognitive assessments, any non-differential measurement error on blood glucose level may bias the association towards the null. Thirdly, the current study did not measure plasma level of insulin, we, thus, could not fully evaluate the level of glycemic control status. Nevertheless, we used a combined criterion of FPG concentrations, self-reported diagnosis of T2DM, and treatment history to categorize the T2DM status. We additionally utilized HbA1c to further categorize glycemic control status among treated T2DM in the sensitivity analysis. In this analysis, non-significant associations of controlled and uncontrolled T2DM with cognitive function were observed possibly due to limited sample size, although a potential detrimental association may exist for uncontrolled T2DM. Overall, future studies with high-quality glycemic control data are needed to elucidate the relationship between T2DM and cognitive function. Furthermore, the cognitive function test used in the current study was a modified TICS approach, and more than half (65.28%) of the study participants had a primary school education or below. Nevertheless, previous studies demonstrated its moderate-to-high validity with cognitive function measured by Mini-Mental State Examination and Clinical Dementia Rating Scale in similar participants, indicating its ability to distinguish individuals based on the relative level of cognitive function [40, 41]. In addition, although a wide range of confounding factors for cognitive impairment has been adjusted, residual and unmeasured confounding cannot be fully controlled. Finally, generalizability could be limited because the study populations were mainly rural individuals (80%) [42].
In summary, our prospective cohort study provided evidence that untreated T2DM in middle-aged and older adults was associated with worse cognitive function. Screening and treatment for T2DM are warranted for maintaining better cognitive function in later life.
Footnotes
ACKNOWLEDGMENTS
The authors acknowledge the support from the Key Laboratory of Intelligent Preventive Medicine of Zhejiang Province (2020E10004).
FUNDING
This study was supported by National Key R&D Program of China (number 2022YFC2010106) and Zhejiang University Global Partnership Fund.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.