
Abstract
Background:
There is a high incidence of cognitive impairment among World Trade Center (WTC) responders, comorbid with post-traumatic stress disorder (PTSD). Yet, it remains unknown whether genetic liability for Alzheimer’s disease, PTSD, educational attainment, or for a combination of these phenotypes, is associated with cognitive impairment in this high-risk population. Similarly, whether the effects of genetic liability are comparable to PTSD and indicators of exposure severity remains unknown.
Objective:
In a study of 3,997 WTC responders, polygenic scores for Alzheimer’s disease, PTSD, and educational attainment were used to test whether genome-wide risk for one or more of these phenotypes is associated with cognitive impairment, controlling for population stratification, while simultaneously estimating the effects of demographic factors and indicators of 9/11 exposure severity, including symptoms of PTSD.
Results:
Polygenic scores for Alzheimer’s disease and educational attainment were significantly associated with an increase and decrease, respectively, in the hazard rate of mild cognitive impairment. The polygenic score for Alzheimer’s disease was marginally associated with an increase in the hazard rate of severe cognitive impairment, but only age, exposure severity, and symptoms of PTSD were statistically significant predictors.
Conclusion:
These results add to the emerging evidence that many WTC responders are suffering from mild cognitive impairments that resemble symptoms of Alzheimer’s disease, as genetic liability for Alzheimer’s disease predicted incidence of mild cognitive impairment. However, compared to polygenic scores, effect sizes were larger for PTSD and the type of work that responders completed during rescue and recovery efforts.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) and related dementias (ADRD) are fatal and costly age-related neurodegenerative disorders [1]. The prodromal phase in ADRD begins with the gradual decline of cognitive ability [2], often characterized clinically by the presence of mild cognitive impairment (MCI) [3]. There is evidence that risk of mortality increases when cognitive impairments affect basic activities of daily living [4]. Consequently, a better understanding of the factors that predict MCI before the emergence of functional limitations is critical to understanding the etiology and pathogenesis of ADRD and crucial for the identification of individuals at heightened risk. Genetic liability is one risk factor for ADRD that can be measured reliably and remains stable across an individual’s life course.
Extant research has uncovered some of the genetic underpinnings for ADRD [5–7]. The identification of risk alleles for ADRD in genome-wide association studies is broadly consistent with findings from biometric studies of cognitive function at midlife [8] and late adulthood [9], having reported heritability estimates ranging from 26% –54% [8, 9]. However, the extent to which genetic liabilities for AD, post-traumatic stress disorder (PTSD), educational attainment, or a combination of these phenotypes are risk factors for cognitive impairment in trauma-exposed populations remains unclear. An ongoing study of World Trade Center (WTC) responders has documented a high incidence of MCI [10], but less is known about the causes of incident MCI and to what degree it is a result of severe trauma exposure versus normal aging. Previous work in the WTC population has reported that MCI is characterized by changes to biomarkers consistent with ADRD [11, 12]. Yet, it has also been found that MCI is precipitated by symptoms of PTSD in WTC responders, consistent with chronically re-experiencing the stressful memories of a traumatic event [10, 14], suggesting that MCI might sometimes be a sequela of PTSD. Moreover, one recent report highlighted educational attainment as a protective correlate of confusion and memory loss in WTC responders, irrespective of PTSD status [15].
It remains unknown whether genome-wide liability for AD, educational attainment, PTSD, or some combination of these pathological and non-pathological phenotypes predict incidence of cognitive impairment among WTC responders. The present study utilized data from WTC responders to conduct a polygenic risk score analysis of mild and severe cognitive impairment to determine whether additive genetic liability for these phenotypes contributes to increased liability for cognitive impairment, after controlling for demographic factors, population structure, and risk and protective factors specific to the WTC rescue and recovery efforts. Results have the potential to underscore underlying genetic risk for cognitive impairment and to help identify individuals at heightened risk in this unique cohort.
MATERIALS AND METHODS
Sample
The present study analyzed data from 3,997 WTC responders. Responders are seen in different health clinics based on their location of residence. The responders included in the present study were seen at one of two responder clinics that are located on Long Island and managed by Stony Brook University. Inclusion criteria included having 1) provided consent for genetic testing, 2) predominately European ancestry as determined by genetic principal components analysis (EUR > 0.80), and 3) had cognitive data, demographic information, and self-reported symptoms of PTSD. The sample was middle-aged at the time of exposure (9/11/2001; mean = 38.20, SD = 8.03) and predominately male (∼93%). See Table 1 for descriptive statistics and sample characteristics.
Descriptive Statistics and Sample Characteristics
n, sample size; M, mean; SD, standard deviation; Min., minimum observed value; Max., maximum observed value. Frequencies and percentages in parentheses are reported for categorical variables. Time-to-event variables represent the number of years after 9/11 when responders exhibit cognitive testing scores indicative of MCI or dementia.
Measures
Demographics and WTC factors
Age in years at 9/11/2001, biological sex as determined by genotype, and self-reported educational attainment were included in inferential analyses as potential demographic correlates of cognitive impairment. Individual differences in WTC exposure were measured using two variables. On average, the more time spent working at Ground Zero, the greater the potential exposure to dust and fine particulate matter, as well as psychological and emotional trauma. Consequently, the number of weeks responders spent working at the WTC was used as an indicator of exposure duration. Exposure severity was also measured using a variable that was based on the type of work responders engaged in during rescue and recovery efforts and the likelihood of exposure to airborne toxins based on that work. Examples of low-risk work are escorting pedestrians around the site, perimeter security, morgue work, and hazard material removal (due to the use of PPE). Examples of high-risk work include truck loading and unloading, sanitation work, bucket barrage, and mechanic work. Whether responders held a supervisory (1 = Yes, 0 = No) or volunteer role (1 = Yes, 0 = No) during the rescue and recovery efforts was also noted, as these features are putatively protective (supervisory role) and risk (volunteer role) factors for exposure severity.
Post-traumatic stress disorder
Symptoms of PTSD were measured using the trauma-specific version of the PTSD checklist (PCL-17) [16] adapted for the 9/11 WTC attacks, which is based on diagnostic criteria from the DSM-IV. In the current study, this scale exhibited high internal consistency evaluated using classical (Cronbach’s α= 0.95) and contemporary (ωt = 0.96, ω= 0.84) psychometric approaches [17]. By study design, symptoms of PTSD were measured before WTC responders completed the cognitive assessment. Of the 3997 responders who met the inclusion criteria for the present study, the baseline cognitive assessment was completed approximately eight years (mean = 7.98 years, range of dates for the baseline assessment = January 2014 to June 2019) after having first completed the trauma-specific, WTC-adapted version of the PCL-17 (range of dates = July 2002 to September 2017).
Cognitive diagnosis
The presence of MCI and probable dementia were made algorithmically following diagnostic guidelines [3, 18]. The Montreal Cognitive Assessment (MoCA) [19], a validated clinical assessment of executive function, memory, and spatiovisual capability that is highly sensitive to detection of mild and severe deficits related to cognitive decline [20, 21], was used to determine the severity of cognitive impairment. At follow-up, among those who were deemed to be unimpaired at baseline, MCI and dementia were determined as the presence of mild (20 < MoCA≤23) to severe (MoCA≤20) cognitive impairment.
Polygenic scores
Blood draws were conducted from January 2012 to January 2019. DNA was extracted from peripheral blood mononuclear cells (PBMCs) and then genotyped using the Infinium Global Screening Array (Illumina, San Diego, CA, USA). Single nucleotide polymorphisms (SNPs) were then processed via established protocols for genotype calling, imputation, ancestry measurement, and the calculation of polygenic scores. Genotypes were imputed to 25,514,638 SNPs using the Haplotype Reference Consortium reference panel on the Michigan Imputation Server pipeline v1.2.4. The analysis utilized a full list of SNPs after clumping (p-value threshold = 1).
Polygenic scores are a summation of the SNPs associated with a target phenotype, weighted by their effect size from a genome-wide association study. The effects of all SNPs were coded so higher polygenic scores are associated with higher values or greater incidence of the respective phenotype. The current study included polygenic scores for educational attainment [22], AD [23], and PTSD [24], and also for re-experiencing symptoms of PTSD [24], as previous research on chronic PTSD supports the view that merely re-experiencing a significant trauma, absent other symptoms, can result in increased risk of ADRD [25]. To avoid the potential inflation of standard errors due to multicollinearity, polygenic risk scores for PTSD and re-experiencing symptoms were included in separate models. Only findings from models that included the polygenic score for PTSD are reported in the results because conclusions remain unchanged when the polygenic score for reexperiencing symptoms was substituted for the polygenic score for PTSD.
Data analytic procedures
Data was imported into R Studio version 1.3.1056, and inferential analyses were conducted using the “survival” package [26] and “survminer” package [27]. To begin, descriptive statistics were calculated for study variables. Next, Kaplan-Meier non-parametric survival analyses were used to examine the cumulative incidence of mild and severe cognitive impairment, before estimating Cox proportional hazard models to provide insight into the effects of demographic factors, polygenic scores, and features of the WTC rescue and recovery efforts, including measures of exposure duration, symptoms of PTSD, and probable exposure to airborne toxins (low-risk or high-risk) based on the type of work responders completed at the WTC sites. Tied survival times were handled using the Breslow approximation [28]. A test of proportionality was conducted using the Schoenfeld residuals test [29]; Stratified Cox models were estimated to allow for different baseline hazards for any variable that violated the proportionality assumption. To assess the explanatory power of study variables in predicting cognitive impairment, generalized coefficients of determination (R2) were calculated for Cox models [30].
To adjust for population structure, the first twenty genetic principal components were included as covariates in all models. To help ease the computational burden on estimation algorithms and to facilitate the interpretation of parameter estimates, all continuous variables were standardized (M = 0, SD = 1) prior to estimating models. Finally, a sensitivity analysis was performed to evaluate the consistency of estimated effects across different analytic routines. Specifically, robust Poisson regressions [31] were estimated using the “lmtest” package [32] and “sandwich” package [33] to predict the occurrence of cognitive impairment irrespective of the amount of time that lapsed between the WTC exposure and the onset of impairment. The effects of all predictors were estimated simultaneously so hazard ratios and relative risk ratios are adjusted for the effects of the other variables in model.
RESULTS
Mild cognitive impairment
Results are reported in Table 2 and depicted in Fig. 1, including Kaplan-Meier non-parametric survival functions for MCI. Older age was significantly associated with MCI, such that a standard deviation increase in age (∼8 years) was associated with a 44% increase in the hazard rate of MCI. Compared to not finishing high school, having a college degree was associated with a 44% decrease in the hazard rate of MCI, although this effect was not statistically significant in the robust Poisson regression (p = 0.179). Compared to males, females exhibited a 46% decrease in the hazard rate of MCI. Exposure severity due to engagement in high-risk work and symptoms of PTSD were also associated with a significant increase in the hazard rate of MCI, with an especially pronounced effect observed for the measure of exposure severity that sorted responders into low-risk and high-risk groups based on the type of work they completed at the WTC sites and probable exposure to airborne toxins due to that work. Finally, the polygenic scores for educational attainment and Alzheimer’s disease were significantly associated with a 14% decrease and 10% increase in the hazard rate of MCI, respectively. Statistically significant (p < 0.05) effects are depicted in Fig. 1.
Results of Cox and Poisson Models Predicting Mild Cognitive Impairment
Effects were estimated simultaneously and additionally adjusted for the first twenty genetic principal components. aHR, adjusted hazard ratio; aRR, adjusted relative risk ratio. Lower and upper 95% denote confidence intervals for adjusted hazard ratios and relative risk ratios.
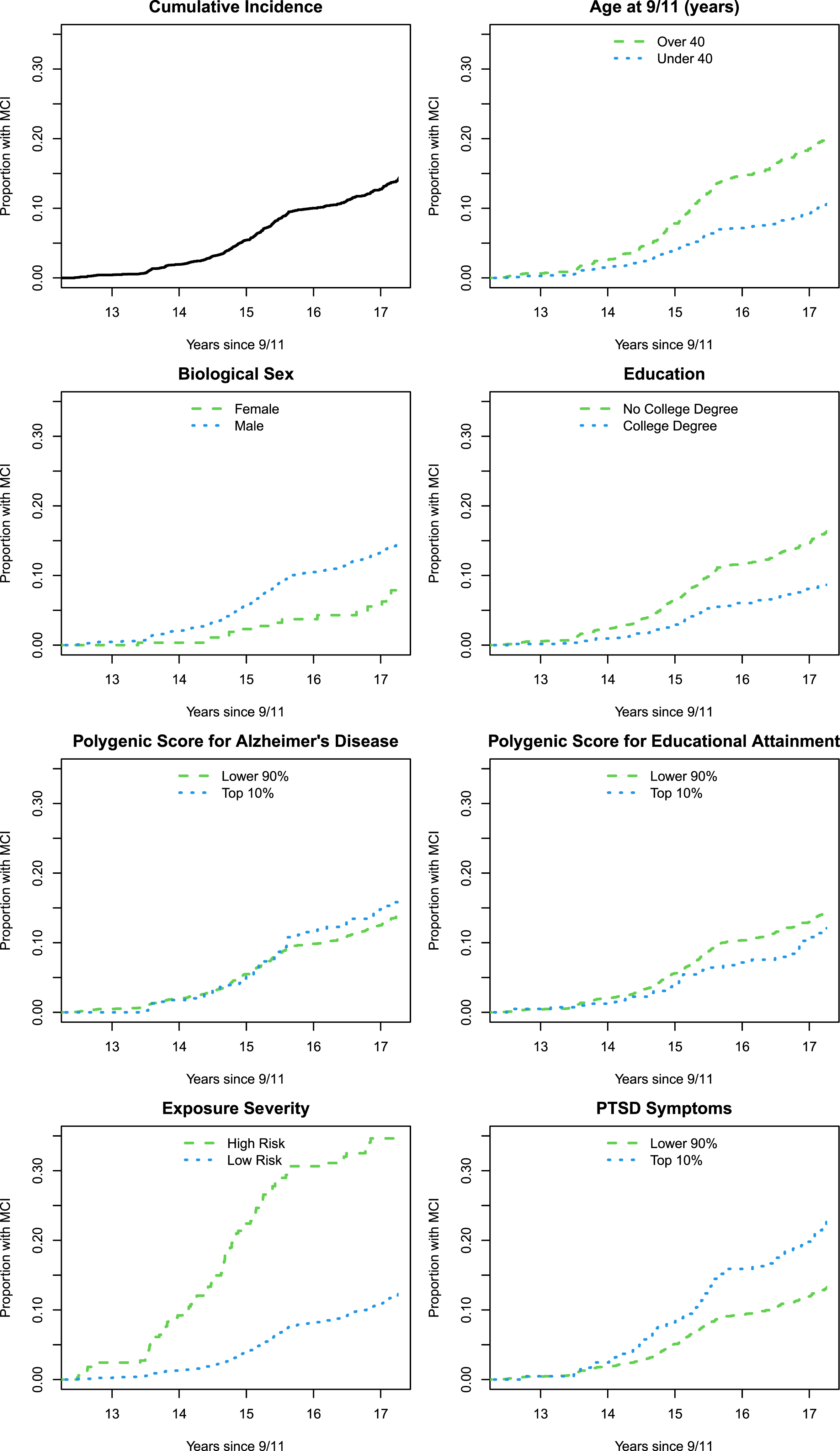
Cumulative Hazards of Mild Cognitive Impairment. Kaplan-Meier non-parametric survival functions are plotted.
The global proportional odds assumption was not upheld for the Cox model of MCI (χ2 = 51.66, df = 35, p = 0.035) because the measure of exposure severity violated the proportionality assumption (χ2 = 19.17, df = 1, p < 0.001). Therefore, a stratified Cox model was estimated that allowed for separate baseline hazards for high-risk and low-risk groups. A likelihood-ratio test indicated that stratification significantly improved model fit (χ2 = 505.95, df = 1, p < 0.001), and the global proportionality assumption was upheld for the stratified Cox model (χ2 = 29.37, df = 34, p = 0.694). Next, a stratified interaction model was estimated that also allowed the effects of study variables to differ for high-risk and low-risk groups, but the fit of the stratified interaction model did not differ significantly from the stratified model with no interaction (χ2 = 42.14, df = 34, p = 0.159). Moreover, the same pattern of results emerged from the stratified Cox model (see Supplementary Material), including the direction, size, and precision of estimates.
The generalized coefficient of determination indicated modest explanatory power for predicting incidence of MCI (R2 = 0.51), with genetic principal components and polygenic scores accounting for only a moderate proportion of the total variance (5.48%). Notably, relative risk ratios from Poisson regressions indicated that substantive conclusions remained largely unchanged irrespective of whether the time to onset of MCI or MCI itself was specified as the outcome of interest. For example, the relative risk ratio for the polygenic score for AD indicated that a standard deviation increase in genetic liability for AD was associated with an 10% increase in the risk of MCI (p = 0.018).
Severe cognitive impairment
Compared to MCI, fewer variables were significantly associated with the hazard rate of severe cognitive impairment indicative of probable dementia. Results are reported comprehensively in supplemental material (Supplementary Figure 1, Supplementary Tables 2 and 3). Older age was a significant predictor, such that a standard deviation increase in age (∼8 years) was associated with a 63% increase in the hazard rate of severe cognitive impairment (p < 0.001). Similar to MCI, the type of work responders completed at the WTC sites (low-risk or high-risk), and symptoms of PTSD were also associated with increases in the hazard rate of severe cognitive impairment (p-values < 0.001). The polygenic score for Alzheimer’s disease was marginally associated with a 14% increase in the hazard rate of severe cognitive impairment (p = 0.095) and having a college education was marginally associated with a 51% decrease in the hazard rate (p = 0.096). No other variables were significant predictors of severe cognitive impairment (p-values > 0.10). The proportional odds assumption was upheld for the Cox model (χ2 = 36.20, df = 35, p = 0.413), and the generalized coefficient of determination indicated appreciable explanatory power (R2 = 0.58), with genetic principal components and polygenic scores accounting for 4.42% of the total variance. Finally, the effects of age, high-risk work, and PTSD remained largely unchanged in Poisson models (see Supplementary Material).
Mild and severe cognitive impairment
Two additional analyses were conducted at the request of reviewers. First, to increase the power to detect predictors of cognitive impairment, Cox and Poisson models were estimated after combining mild and severe cognitive impairments into a single outcome (MoCA < 23). Second, to provide an estimate of a psychologically traumatic or emotionally salient exposure, whether responders saw blood or bodily fluids (Yes ∼ 41%, No ∼ 59%) during rescue and recovery efforts was included as an additional predictor of cognitive impairment, before and after combing mild and severe impairments into a single outcome.
Results are reported in Table 3 and also in supplemental material (Supplementary Tables 4–8). Briefly, with few exceptions, the predictors of mild and severe cognitive impairments were similar after adjusting for whether responders saw blood or bodily fluids during rescue and recovery efforts, which was itself not a significant predictor of mild or severe cognitive impairment, regardless of whether mild and severe impairments were tested individually or combined into a single outcome (p-values > 0.10). In fact, the effect size of the polygenic score for Alzheimer’s disease was larger after combing mild and severe impairments into a single outcome, such that a standard deviation increase in the polygenic score for AD was associated with a 17% (p = 0.007) and 18% (p = 0.004) increase in the hazard rate and relative risk of cognitive impairment, respectively. On the other hand, the effect size of the polygenic score for educational attainment remained unchanged in the Cox model but was only marginally significant in the robust Poisson regression (RR = 0.90, p = 0.060).
Results of Cox and Poisson Models Predicting Mild & Severe Cognitive Impairment Including an Estimate of Exposure to Blood and Bodily Fluids
Effects were estimated simultaneously and additionally adjusted for the first twenty genetic principal components. aHR, adjusted hazard ratio; aRR, adjusted relative risk ratio. Lower and upper 95% denote confidence intervals for adjusted hazard ratios and relative risk ratios. Multiple imputation was used for missing data. Details on the multivariate imputation model and the results of a complete cases analysis are reported in supplemental material.
DISCUSSION
The present study tested whether demographic factors, indicators of physical and psychological trauma, and polygenic scores for AD, PTSD, and educational attainment were associated with incidence of mild and severe cognitive impairments among WTC responders. The polygenic score for educational attainment was significantly associated with a decrease in the hazard rate of MCI, while the polygenic score for AD was significantly associated with an increase in the hazard rate of MCI, as well as a marginally significant increase in the hazard rate of dementia. Although genetic factors in aggregate accounted for a moderate degree of variance in MCI (5.48%) and dementia (4.42%), including genetic principal components and polygenic scores, effect sizes were small for individual polygenic scores. For example, the polygenic score for educational attainment accounted for less than 1% of the total explanatory power of study variables predicting MCI. Similarly, the polygenic score for AD accounted for approximately 1% of the total explanatory power of study variables predicting MCI. These small effect sizes indicate that polygenic scores alone provide limited utility in predicting the individuals who will suffer from cognitive impairment in this trauma-exposed cohort, despite highlighting potentially important pathogenic factors that are present at the time of gamete formation.
Critically, results of the current study further underscore the importance of individual differences in trauma exposure and long-term psychiatric sequalae in understanding the precipitously high incidence of cognitive impairment among WTC responders. Exposure severity was strongly associated with increases in the hazard rates of mild and severe cognitive impairments, specifically when measured in terms of high-risk work at the WTC site that increased the likelihood of responders encountering fine particulate matter that can infiltrate the brain to cause neuronal damage, potentially resulting in neurodegenerative disease. Importantly, the strong links between high-risk work and incidence of mild and severe cognitive impairments persisted after accounting for population stratification and genetic liability for AD, PTSD, and educational attainment.
Symptoms of PTSD were also consistently linked with incidence of mild and severe cognitive impairments. These finding are consistent with growing evidence that trauma exposure and PTSD may result in an AD-like disorder by causing early proliferation of tau protein and Aβ [34]. A notable finding has been the identification of the presence of physical functional limitations [35] alongside changes in proteins consistent with inter-neuronal damage in WTC responders with PTSD and MCI [36]. Taken together with the present findings and recent meta-analyses of the link between PTSD and dementia [37–39], these results suggest that symptoms of PTSD are a risk factor for a condition arising independently from AD though having similar symptomatology.
While the polygenic score for AD was significantly associated with a higher incidence of MCI, it was only marginally associated with a higher incidence of severe impairment. This may come as a surprise as genetic liability for a severely debilitating neurodegenerative disease, like AD, might be expected to predict severe impairments more strongly than mild impairments. Indeed, the effect size of the polygenic score for AD was larger for severe impairments than MCI but estimated with less precision due to the lower incidence, in turn, resulting in insufficient power to detect a significant genetic signal. Consistent with this interpretation, the effect of the polygenic score for AD was statistically significant when power was increased by combining mild and severe cognitive impairments into a single outcome. Further, many of the WTC responders with cognitive impairments are currently at midlife, prior to the age at which symptoms of AD typically appear, and MCI has many potential causes and does not necessarily progress to dementia. Therefore, it remains an open question whether genetic signal for AD will increase as WTC responders continue to age chronologically and cognitively.
Crucially, the statistically significant association of the polygenic score for AD with MCI should not be interpreted as definitive evidence that cognitively impaired WTC responders are suffering from early-onset AD. For one, polygenic risk scores are often associated with a target, sometimes called a ‘proxy phenotype’, that is different from the phenotype for which the PRS was developed [40]. In other words, a polygenic risk score based on one phenotype may be predictive of a trait that is similar in clinical presentation or genetically correlated with the phenotype for which the polygenic score was constructed. Moreover, as previously noted, the effect size of the polygenic score for AD was small and overshadowed by the effects of high-risk work and PTSD, indicating that the clinical presentation of cognitive impairments among WTC responders bears a resemblance to AD but with etiology more closely tied to the severity of a traumatic exposure than inherited pathogenic variants.
Exposure severity based on probable exposure to air born toxins was strongly associated with cognitive impairment in the present study, both mild and severe impairments, even after controlling for genetic liability for risk and protective phenotypes, including AD, PTSD, and educational attainment. On the other hand, exposure to blood and bodily fluids was neither associated with mild nor severe cognitive impairment. However, exposure to blood and bodily fluids by no means comprehensively captures the myriad of toxic and traumatic exposures endured by the heroes who facilitated rescue and recovery efforts after the 9/11 attacks. For example, many responders saw people fall or jump from the Twin Towers and suffer reliving those horrific memories for the rest of their lives. Others were injured while excavating debris to search for survivors, and others had a relative, friend, or co-worker killed and were (and continue to be) burdened with the emotional and physiological consequences of bereavement. Finally, others witnessed the destruction of their homes, places of work, and community at large. Understanding how these emotional and physical traumas combine and intersect with exposure to airborne toxins, as well as other environmental exposures and psychosocial factors that contribute to cumulative stress [41], will be crucial to better characterizing the exposome of PTSD and AD, i.e., the totality of pathogenic exposures over the life course that lead to the expression of psychiatric symptoms and accelerated cognitive decline [42]. This will include discerning the common and unique features of the exposomes for PTSD and AD.
Limitations
It has been argued that “using the term “causal” is necessary to improve the quality of observational research” [43]. In this vein, the longitudinal design and temporal order of variables in this prospective study strengthens causal inference by excluding the possibility of reverse causation, e.g., inherited genetic factors and the WTC attacks preceded and, therefore, cannot be caused by symptoms of PTSD and cognitive impairment. Nevertheless, effect sizes may be biased estimates of causal effects due to the potential influence of unmeasured variables (a.k.a. third-variable confounding), a limitation that is inherent to all non-experimental studies. For this reason, drawing definitive causal conclusions from the reported findings is not warranted. Moreover, as all WTC responders were exposed to some level of trauma, the current study lacks a proper control group to better understand and contextualize the effect sizes documented in the current study. The residents of the NYC greater metropolitan area, including many WTC responders, differ from the general population in important ways, including greater exposure to airborne pollutants due to high population density. Additionally, the demographic characteristics of WTC responders do not correspond with the demography of the general U.S. population, with most emergency responders being white and male.
As genome-wide association studies have largely been conducted with participants of predominately European ancestry, polygenic risk scores based on those studies lack validity in more diverse populations. Therefore, using European-derived polygenic scores that may have clinical implications in diverse ethnicities has the potential to further exacerbate racial and ethnic health disparities [44]. There is a need to expand genome-wide discovery efforts in non-European populations to improve our understanding of existing racial/ethnic disparities in ADRD [45, 46]. Thus, it remains unclear whether the current study findings generalize to other trauma-exposed populations, particularly those that are more diverse. Nevertheless, the current study adds to the emerging evidence that many WTC responders are suffering from AD-like cognitive impairments by documenting links between genetic liability for AD and incidence of cognitive impairment.
Conclusions
Genetic liability for multiple phenotypes can help us to understand the unique factors through which clinical entities might be emerging in this trauma-exposed population. To date, the extent that WTC responders, who were heavily exposed to traumatic events and to airborne materials expelled from the Twin Towers after the collapse, are suffering from early-onset AD or another unknown condition is unclear. This study found that genetic liability for AD is a statistically significant predictor of MCI. This work also identified genetic liability for educational attainment as an independent predictor of MCI in responders, even after adjusting for the significant effects of polygenic risk for AD and the highest level of education completed by responders. However, compared to the effects of polygenic scores, effects on incident MCI were larger for exposure severity and PTSD. In sum, results of the present study suggest the potential for more than one ongoing process including AD and non-AD pathogenesis linked to exposure severity and symptoms of PTSD in WTC responders.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
Data collection was funded by R01AG049953, awarded to S.A.P.C., CDC 2011-200-39361 awarded to B.J.L., U01OH011864 awarded to M.A.W, and by the SUNY Research Foundation. The analyses were funded by R21AG074705 awarded to F.D.M.
CONFLICT OF INTEREST
The authors have no conflict of interest to disclose.
DATA AVAILABILITY
A limited dataset can be made available to interested researchers upon completion of a data usage agreement and IRB approval.