
Abstract
Background:
Neuropsychological assessments are essential to define the cognitive profile and contribute to the diagnosis of Alzheimer’s disease (AD). The progress in knowledge about the pathophysiological process of the disease has allowed conceptualizing AD through biomarkers as a biological continuum that encompasses different clinical stages.
Objective:
To explore the association between cerebrospinal fluid (CSF) biomarkers of AD and cognition using the NEURONORMA battery, in a sample of cognitively unimpaired (CU), mild cognitive impaired (MCI), and mild dementia of the Alzheimer type (DAT) subjects, and to characterize the cognitive profiles in MCI subjects classified by A/T/N system.
Methods:
42 CU, 35 MCI, and 35 mild DAT were assessed using the NEURONORMA battery. Core AD biomarkers [amyloid-β42 (Aβ42) peptide, total tau (t-tau), and phosphorylated tau 181 (p-tau181)] proteins were measured in CSF. Correlation coefficients, multivariate regression, and effect sizes were calculated. We explored the age- and education-adjusted cognitive profiles by A/T/N variants within the MCI group.
Results:
Cognitive outcomes were directly associated with CSF Aβ42 and inversely with CSF tau measures. We found differences in both biomarkers and cognitive outcomes comparing all pairs except for CSF measures between cognitively impaired groups. The highest effect size was in memory tasks and biomarkers ratios. Lower performances were in memory and executive domains in MCI subjects with AD pathology (A+T+N±) compared to those with normal levels of AD biomarkers (A– T– N).
Conclusion:
This study provides further evidence of the validity of Spanish NEURONORMA cognitive battery to characterize cognitive impairment in the AD pathological continuum.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the main cause of dementia [1, 2] accounting for 50– 70% of cases of patients with cognitive impairment [3]. Episodic memory impairment and also of other cognitive domains such as language, executive functions, praxis, and visuospatial abilities typically characterize AD [4–8]. Mild cognitive impairment (MCI) is defined by objective cognitive impairment in at least one cognitive domain but without meeting the dementia criteria [9]. It might be caused by different etiologies [10]. Amnestic MCI has been typically considered as a pre-dementia stage of AD although there are other types of onset such as logopenic aphasia or dysexecutive syndrome that can be observed in atypical variants of AD [11, 12]. Nowadays it is possible to detect in vivo the pathophysiological changes in proteins related to the hallmarks of AD proteinopathies (amyloid-β and tau tangles). This possibility to detect and to track pathophysiological changes, using fluid biomarkers or molecular neuroimaging techniques, contributes to a more accurate diagnosis and to a better knowledge of AD.
Regarding AD core biomarkers in CSF, decreased concentrations of amyloid-β42 (Aβ42) peptide and increased concentrations of total tau (t-tau) and phosphorylated tau (p-tau) proteins in CSF are consistent with AD pathology [13, 14]. A recent criterion from [15] in research framework proposes a definition of AD categories according to biological profiles. The A/T/N classification system [16] which biomarkers are grouped into “aggregated Aβ or associated pathologic state (A)”, “aggregated tau (neurofibrillary tangles) or associated pathologic state CSF phosphorylated tau (T)”, and “neurodegeneration or neuronal injury (N)”. From combinations of these profiles the following categories are derived: Normal AD biomarkers (A– T– N–). Non-AD pathologic change (A– T+N–, A– T– N+, A– T+N+) and AD continuum (A+ independently of T and N) which includes 3 subcategories: AD pathologic change (A+T– N–), AD (A+T+N–, A+T+N+), and AD and concomitant suspected non-AD pathologic change (A+T– N+). Moreover, these criteria include a “numeric clinical staging scheme” for those individuals in the AD continuum that shows the sequential evolution of AD.
Association between cognition and AD biomarkers
During the last decade, several studies have suggested an association between AD biomarkers and cognition, as assessed by different neuropsychological measures.
Cross-sectional studies have reported a clear correlation between abnormal Aβ measures and low performance in different memory tasks in MCI and AD patients [17–22]. Abnormal levels of t-tau and p-tau protein and CSF Aβ42/t-tau ratio are associated with low performance in memory [19–28], attentional and executive functions in MCI and AD subjects [19, 24]. Aβ levels and cognition also show an association in CU individuals with and without subjective cognitive decline in memory [17, 29– 31] and in other cognitive domains such as executive functions, working memory, and language [21, 32– 35]. Two meta-analyses concluded that there is a significant association, with a small effect size, between memory and Aβ in CU subjects [29, 36].
Several longitudinal studies showed that baseline abnormal AD biomarkers levels are associated with cognitive decline over time. MCI subjects with abnormal Aβ, tau, or both concentrations at baseline showed a higher decline in episodic memory [37–40], working memory and executive functions tasks [38, 41] and in Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog) [42]. Similarly, in CU subjects, baseline abnormal biomarkers have also been found to predict a steeper decline over time in episodic memory [43–49], executive tasks [44, 48], and on the Preclinical Alzheimer Cognitive Composite (PACC) [50]. In addition, some studies have found an association between a subsequent memory decline in CU population and CSF Aβ42/t-tau and Aβ42/p-tau ratios [51–53].
It is mandatory to extend the study of individual cognitive capacities to improve the knowledge of how these are affected during the disease and their association with biomarkers [3]. Considering this, the present study aims to show the associations between a comprehensive and validated cognitive battery in Spanish population (NEURONORMA battery) [54–61] and specific CSF AD biomarkers across the entire AD continuum. A previous work has shown the characteristic cognitive profiles of NEURONORMA battery in MCI and DAT subjects and the differences of these neuropsychological variables and neuroimaging outcomes comparing with control subjects [62]. The present study is a further development to validate the battery with a sample of individuals with AD biomarker measures available. The study of associations between specific cognitive tests and biomarkers will enable us to refine diagnostic protocols by selecting those measures that show highest accuracy to detect patients with a clinical and biological diagnosis across the AD continuum.
The main objective of this work is to explore the association between NEURONORMA cognitive battery and CSF biomarkers in the AD continuum. Secondary objectives are: 1) to explore the differences and their effect sizes in cognition and CSF outcomes levels between subjects with a clinical diagnosis of cognitive impairment (MCI and mild DAT) compared with CU subjects, and 2) to describe the cognitive profile of MCI subjects classified by A/T/N system.
MATERIALS AND METHODS
Participants
We included 112 participants with a diagnosis of CU (n = 42), MCI (n = 35), and mild DAT (n = 35) from the “Estudio de Correlación de Instrumentos Cognitivos y Biomarcadores en la Enfermedad de Alzheimer (CORCOBIA Project)”, a multicenter study lead by Hospital del Mar and the Laboratori de Referència de Catalunya whose main objective was to obtain the cut-off values for AD CSF biomarkers for reference population of the participating centers. The CSF data from CU and mild DAT subjects from the study were used to calculate the CSF cut-offs [63]. This project was approved by the Research Ethics Committee of the Hospital del Mar Research Institute (Barcelona, Spain) (Ref. 2014/5638) and was conducted according to the Declaration of Helsinki and its subsequent amendments, and the European Union regulations concerning medical research. All participants gave informed consent to participate in the project and in case of subjects with a diagnosis of mild DAT, a caregiver or relative signed the informed consent.
The selection criteria for all participants were as follows: Inclusion criteria: a) age between 60 and 85 years, b) hearing, vision and physical conditions adequate to perform neuropsychological assessments, c) minimum education years to perform neuropsychological assessments (at least reading and writing skills), d) medical condition and stable pharmacological treatment for 3 months before the beginning of the study; Exclusion criteria: a) unwillingness or inability of the subject to collaborate adequately in the study, b) any pathology of the central nervous system other than those studied that may affect cognition, c) history of psychiatric disorders that, in the opinion of the investigator, may affect the cognitive abilities of the participants, major depressive episode, bipolar disorder, decompensated dysthymic disorder, schizophrenia or psychotic episode, according to DSM-V criteria), d) hypothyroidism and/or vitamin deficiencies (B12, folic acid) or any other medical condition that, in the judgment of the investigator, interferes with the cognitive performance of the participants, e) any medical condition that implies contraindication for the performance of a lumbar puncture (e.g., active treatment with anticoagulants, hematological disorders that affect coagulation such as significant thrombocytopenia or coagulopathies, severe hepatic insufficiency or lumbar pathology that implies a high risk for the performance of the lumbar puncture), f) alcohol consumption in a pattern of abuse or consumption of toxic substances that, in the investigator’s judgment, could interfere with the participants’ cognitive performance, g) any medical condition that, in the investigator’s judgment, could interfere with cognitive assessment, existence of any situation that could make the subject, in the opinion of the principal investigator, unsuitable for the study.
Participants were assigned to the different groups according to the following criteria: I) ‘DAT’: patients with moderate cognitive impairment and dementia according to the Global Deterioration Scale (GDS)-4 [64] who also meet diagnostic criteria for ‘probable’ DAT according to 2011 NIA-AA criteria [65]. Atypical onsets (logophenic aphasia, dysexecutive variant, and posterior cortical atrophy) were not included. II) ‘MCI’: patients with mild cognitive impairment with objective impairment in at least episodic memory and activities of daily living relatively preserved (GDS-3) [11]; ‘CU’": subjects presenting a normal neuropsychological study adjusted for age and education. CU sample was composed, on the one hand, by patients who consulted for subjective cognitive decline and an MCI clinical diagnosis was ruled out (61.9%) and, on the other hand, by relatives of participants (75% were spouses).
Neuropsychological measures
NEURONORMA battery includes the following cognitive tests: Digit Span forward and backward [66], Corsi’s test [67], Trail Making Test (TMT) [68] - both parts A and B were assessed, Symbol Digit Modalities Test (SDMT) [69], Boston Naming Test [70], Token Test [71], Judgment of Line Orientation [72], Rey-Osterrieth Complex Figure (ROCF) [73, 74], Free and Cued Selecting Reminding Test (FCSRT) [75], Verbal fluency, including a semantic task (animals) and a phonemic task (words beginning with p) [66], Stroop Color-Word Interference Test [76], Tower of London Drexel University version (TOL-Dx) [77], and four selected test (Object decision, progressive silhouettes, position discrimination, and number location) of the Visual Object and Space Perception Battery (VOSP) [78]. All tests were administered by trained neuropsychologists and scored according to standardized procedures published in each test manual. In this study, it has also been included Dual Task (DT) test, an experimental measure of divided attention included in NEURONORMA-Plus, an ulterior extension of the original NEURONORMA project [79, 80] which is composed by a concurrent verbal span and a cancelation task. DT was only administrated in CU and MCI groups. The Goldberg scale [81] was used for assessing anxiety and depression symptoms and Blessed Dementia Rating Scale (BDRS) [82] for assessing daily living activities.
CSF acquisition and analysis and APOE genotyping
Lumbar puncture (LP) was performed in all participants, as well as blood sampling for APOE genotyping. The CSF AD core biomarkers measurements were performed at the Laboratori de Referència de Catalunya (LRC) using ’Lumipulse G 600 II’ system and its IVD reagents (Fujirebio). APOE-ɛ genotyping was performed at LRC with ‘APOE Real Type’, IVD reagents from Progenie Molecular SLU. Further details about CSF acquisition and measurements and APOE genotyping are detailed in our recent published work [63].
NEURONORMA cognitive profiles
Cognitive profiles are formed by the selected cognitive variables and the set of scaled scores resulting from published normative data of NEURONORMA project (Peña-Casanova. 2009a). In summary, subject’s raw scores were transformed to age-adjusted scaled scores based on percentile ranges and a further education adjustment based on linear regressions. Scaled scores (from 2 to 18) have a mean of 10 and standard deviation (SD) of±3. Scaled scores from ≤5 are considered as an impaired performance, scaled scores of 6 and 7 as borderline and low average performances respectively, and scaled scores ≥8 are considered within the normality range. Average cognitive profiles subjects were created by calculating the medians of scaled scores.
MCI groups were created according to A/T/N system [15, 16] and the frequency of profiles were the following: A– T– N– (n = 9), A– T+N+ (n = 1), A+T– N– (n = 5), A+T+N– (n = 2) and A+T+N+ (n = 18). We used “±” symbol to encompass both variants (A+T+N– and A+T+N+). This classification was done by applying cut-offs values of CSF biomarkers published in our recent work [63], A+ was considered when: Aβ42 ≤750 or Aβ42/ Aβ40 ≤0.062 or both, T+ was considered when p-taup-tau181 ≥69.85 and N+ was considered when t-tau ≥522. Moreover, these criteria [15] include a ‘numeric clinical staging scheme’ (C) for those individuals in the Alzheimer’s continuum that shows the sequential evolution of AD.
Statistical analysis
Sample sociodemographic and clinical data included mean and standard deviation for continuous variables, and frequency and percentage for categorical variables. The normality assumption for continuous variables was tested using the Shapiro-Wilk test. Pearson’s Chi-Squared test was applied to analyze group differences in categorical variables, while Kruskal-Wallis and Mann– Whitney U tests (adjusted by Bonferroni’s correction) were applied to continuous variables. Spearman’s correlation (rho) was used to test the correlation between CSF and cognitive measures in global sample. In this study a correlations <0.4 was considered as small, 0.40– 0.70 as moderate and >0.7 as strong. Medians and interquartile range for study variables (CSF measures and raw cognitive scores) are presented. Differences between clinical groups for CSF and cognitive measures were checked through multiple linear regression using a robust M-estimator for the target variables to control for the presence of outliers. Multivariate model was performed adjusting for potential confounders (co-variables: age, education, and sex). Coefficients, confidence intervals (CI) 95% and adjusted p-values were obtained. For the effect size study, Cohen’s d values of both CSF and cognitive measures (a total of 42 variables) were obtained to analyze the differences of all pairs: mild DAT versus CU, MCI versus CU, and mild DAT versus MCI. Significance threshold was set at p < 0.05. The statistical analysis was performed with the Statistical Package for the Social Sciences 22.0 program, STATA 15.1 and the corrplot package in R statistical software (v 4.1.2).
RESULTS
Demographics and clinical characteristics
The mean age was 73.25 (5.57) years, 57.1% of the sample were women. All participants were Caucasian, with a mean of 9.62 (4.15) years of education. The characteristics of the three sample groups (CU n = 42, MCI n = 35 and mild DAT n = 35) are shown in Table 1. No significant differences were found regarding sex and years of education among groups. CU participants were younger than MCI participants (p < 0.05). A worse performance in Mini-mental State Examination (MMSE) and a greater impairment in IADL, measured by Blessed Dementia Rating Scale (BDRS) (instrumental activities part) and an increased percentage of APOEɛ4 carriers was found in mild DAT participants (p≤0.001). No differences were found in anxiety and depression symptoms among groups.
Characteristics of the study sample
CU, cognitively unimpaired subjects; MCI, mild cognitive impairment; DAT, dementia of the Alzheimer type; APOE, Apolipoprotein E; MMSE, Mini-Mental Status Examination. BDRS, Blessed Dementia Rating Scale. Data are expressed as Mean (M) and Standard Deviation (SD) [age, education, MMSE, BDRS, and Goldberg scale] or number of participants (n) and percentage (%) [sex, APOE ɛ4 carrier status]. 1Kruskall Wallis Test (age, education, MMSE, BDRS and Goldberg scale) and Chi square (sex, APOE ɛ4 carrier status). P-values Mann-Whitney U test (Bonferroni’s correction): astatistically significant for CU versus mild DAT; bstatistically significant for CU versus MCI; cstatistically significant for MCI versus mild DAT. APOE ɛ4 genotype was not available in 3 (2.68%) individuals. BDRS scale was not available in 23 (20.5%) individuals. Goldberg scale was not available in 8 (7.14%) individuals.
Cognitive and CSF variables in the global sample
Figure 1 shows the correlation matrix between cognitive measures and biomarkers in the overall sample (n = 112). Spearman rho values and associated p-values are shown in Supplementary Table 1. The correlations between CSF Aβ measures (Aβ42, Aβ42/Aβ40) or the combination ratios (CSF Aβ42/t-tau, CSF Aβ42/p-181) and cognitive variables positive, except for timed scores. The opposite effect was observed regarding CSF tau measures (t-tau and p-tau181). Only the variable P-Dual did not show this association. Overall, correlations were statistically significant (p < 0.05) between cognitive variables and CSF measures, except some variables from VOSP and the P-Dual. The strongest association was observed between CSF Aβ42/p-Tau181 and memory tests (FCSRT and ROCF), showing moderate positive correlations (FCSRT Free recall trial 1: rho = 0.53, p≤0.001, CI = 0.36– 0.66; FCSRT Total free recall: rho = 0.54, p≤0.001, CI = 0.37– 0.67; FCSRT Total recall: rho = 0.58, p≤0.001, CI = 0.42– 0.69; FCSRT Free delayed recall: rho = 0.54, p≤0.001, CI = 0.38– 0.66; FCSRT Total delayed recall: rho = 0.61, p≤0.001, CI = 0.46– 0.72; FCSRT ISC: rho = 0.57, p≤0.001, CI = 0.42– 0.68; ROCF 3 min recall: rho = 0.53, p≤0.001, CI = 0.37– 0.66; ROCF 30 min recall: rho = 0.55 p≤0.001, CI = 0.38– 0.66; ROCF Recognition task: rho = 0.50, p≤0.001, CI = 0.33– 0.64). However, these associations are mainly driven by symptomatic patients and were weaker, but still mainly significant for the FCSRT, when CU participants were excluded (data not shown).
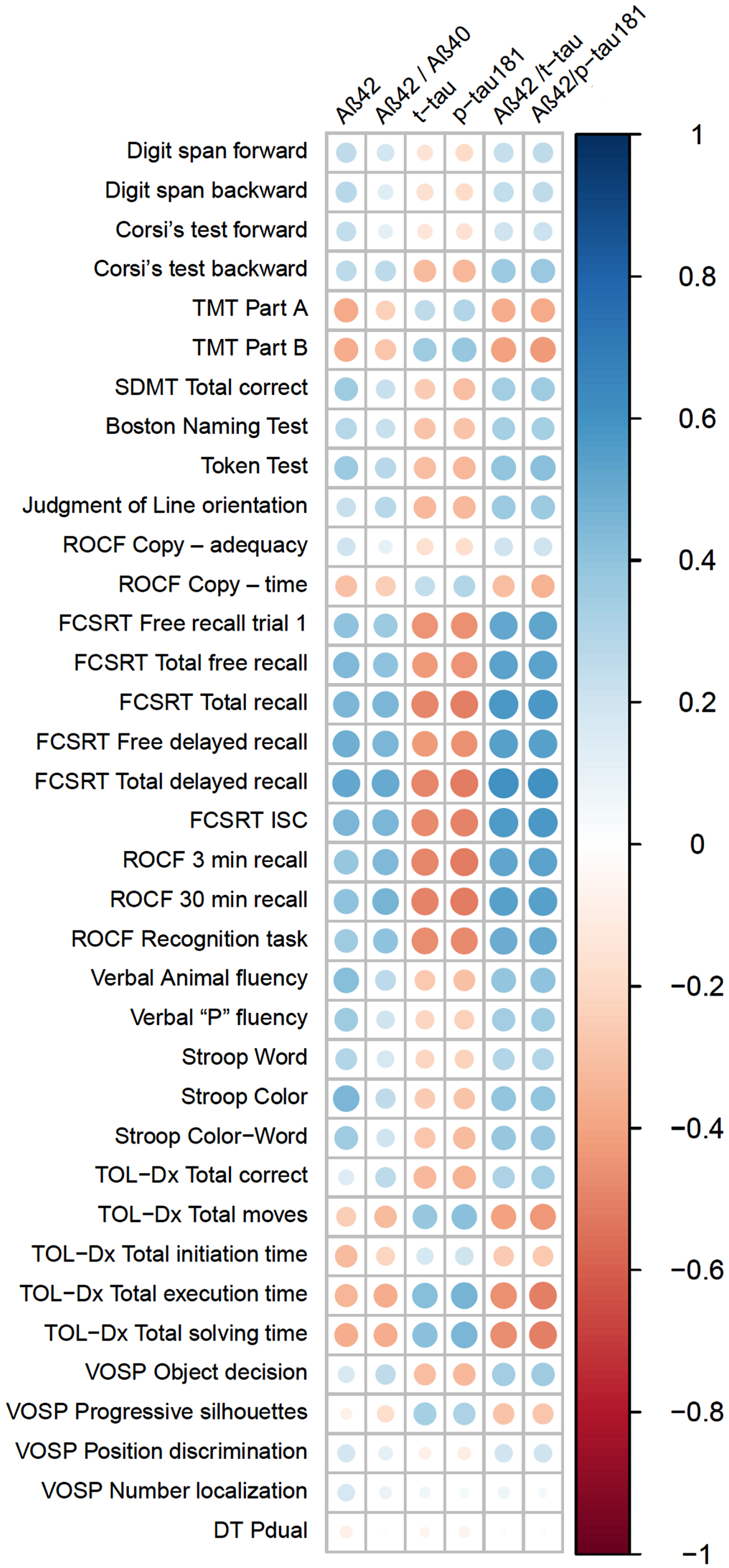
Spearman’s (rho) correlation matrix of CSF measures and NEURONORMA battery on the global sample (r and p-values in Supplementary Table 1).
Comparisons among clinical groups
The whole analyzed CSF measures and raw NEURONORMA scores and the results of the adjusted comparison of each group are summarized in Table 2 (except for VOSP-Position discrimination since many subjects obtained the maximum test score, and no differences could be detected). Coefficients and CI 95% values are shown in Supplementary Table 2. Significant lower CSF Aβ42 and Aβ42/Aβ40 (p < 0.05), CSF Aβ42/t-tau and Aβ42/p-tau181 values (p≤0.001) and significant higher t-tau and p-tau181 (p < 0.05) values were found in cognitively impaired groups, compared with CU participants. Conversely, our results did not show differences between MCI and mild DAT subjects in any CSF measures (p = 0.068– 0.203). Mild DAT subjects scored significantly lower than CU subjects in all the cognitive measures, except for VOSP-Number localization (p = 0.797), with values of p≤0.001 (except from Digit span forward, p = 0.003 and Digit Span backward p = 0.002). Also, compared with CU, MCI participants showed lower scores in all tests (p < 0.05), except for Digit span forward (p = 0.268), ROCF Copy-Adequacy (p = 0.753), Stroop-Word (p = 0.109), TOL-Total initiation time (p = 0.097), VOSP-Number localization (p = 0.542), and Pdual (p = 0.450).
Medians and interquartile ranks from the CSF measures and raw scores of NEURONORMA battery and adjusted p values from multivariate robust regression of all pairs comparisons
CU, cognitively unimpaired subjects; MCI, mild cognitive impairment; DAT, dementia of the Alzheimer type; CSF, cerebrospinal fluid; Aβ, amyloid-β protein; t-tau, total tau protein; p-tau181, phosphorylated tau protein 181; TMT, Trail Making Test; SDMT, Symbol Digit Modalities Test; ROCF, Rey-Osterrieth complex figure; FCSRT Free and Cued Selective Reminding Test; ISC, Index of sensitivity of cueing; TOL-Dx, Tower of London Drexel version; VOSP, Visual Object and Spatial Perception Battery; DT, Dual Task; NA, not applicable. ap values: adjusted p values (covariates: age, education, and sex). *significant at level p < 0.05. **significant at level p < 0.001.
Finally, overall scores were lower in mild DAT individuals comparing with MCI. Memory (eg. FCSRT), executive (eg. TMT part B, Verbal Animal Fluency), or language (Boston Naming Test) domains remained significantly different (p < 0.05). However, we found similar performances in Digit span backward, Corsi’s test forward, ROCF Recognition task, TOL-Dx Total correct and subtests of VOSP (Object decision and Progressive silhouettes) and in those already observed in the MCI versus CU comparison.
Effect size study
Highest Cohen’s d values were observed when comparing mild DAT versus CU. All results of the effect size study are available in Supplementary Table 3, where the variables of the mild DAT versus CU comparison are sorted from highest to lowest. All cognitive variables from FCSRT, ROCF, most variables from TOL-Dx and Stroop Test, SDMT total correct, animal verbal fluency and Boston Naming Test showed higher effect size (d = 4.41– 1.73) than CSF Aβ42/p-tau181, the CSF measure with the highest effect size observed (d = 1.56). Figure 2a shows the Cohen’s d values of all CSF measures from all groups. Combination of CSF Aβ and tau measures (Aβ42/p-tau181 and Aβ42/t-tau ratios) obtained higher effect sizes. Figure 2b shows cognitive variables whose effect size were d≥2 in the mild DAT versus CU comparison, and values of these variables in the MCI versus CU, and MCI versus mild DAT comparisons. All FCSRT scores showed the largest differences between both groups of cognitively impaired subjects and CU (MCI d > 2 and mild DAT d > 3), and FCSRT total recall was the measure with a greater effect size when differentiating between MCI and mild DAT (FCSRT delayed total recall d = 1.15 and FCSRT total recall d = 1.03).
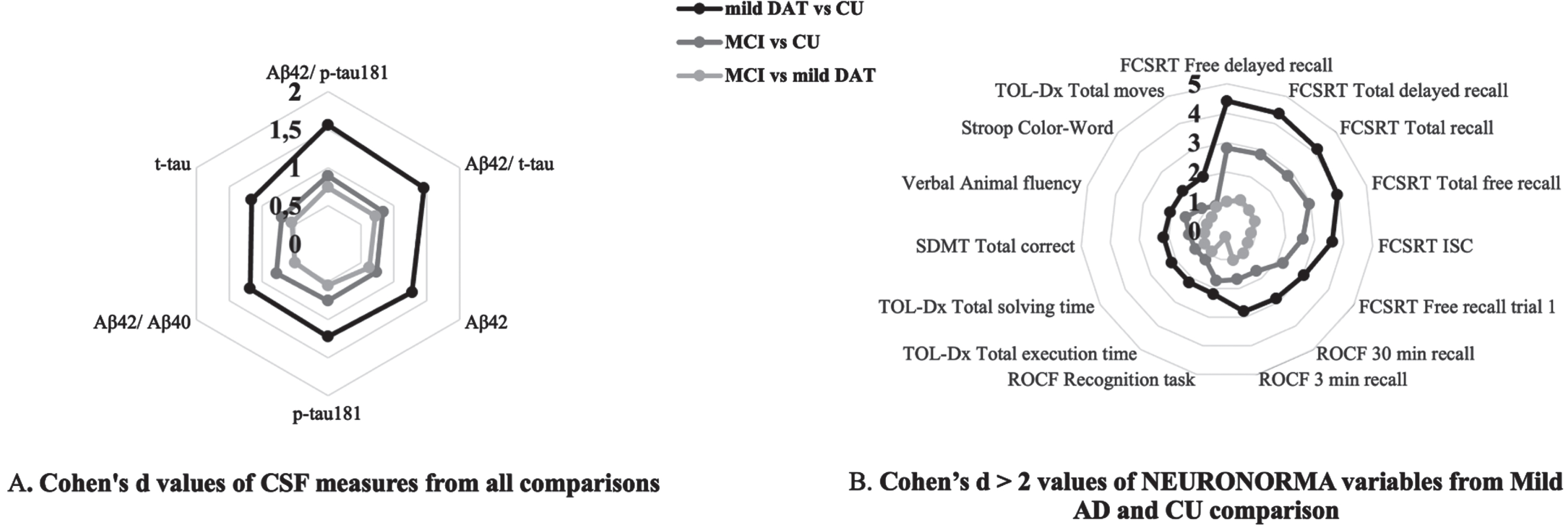
Effect size of CSF and cognitive measures between groups.
A/T/N cognitive profiles in MCI subjects
MCI individuals (n = 35) were subcategorized into A/T/N profiles and categories according to CSF cut-offs previously established [63]. We found that 71.4% (n = 25) of MCI group were positive for AD biomarkers and classified into AD continuum. Of these subjects, A+T+N+ variant was the most common (n = 18) followed by A+T– N– (n = 5) and A+T+N– (n = 2), resulting in a 57.1% (n = 20) of MCI individuals categorized as ‘AD stage 3’ according to NIA-AA (2018) criteria. On the other hand, 25.7% (n = 9) of MCI group showed normal levels of core AD biomarkers in CSF (A– T– N–) and 1 subject was categorized with A– T+N+ profile. NEURONORMA cognitive profiles expressed as the medians of scaled scores (adjusted for age and education) of ‘AD stage 3 (A+T+N±)’ and ‘MCI (A– T– N–)’are presented in Fig. 3. Comparing with normative data, FCSRT showed the lowest performances in both groups, with the most impaired subjects from ‘AD stage 3’ obtaining scaled scores within a range of 3– 5. TMT-B, TOL- Dx Total Moves and Execution time performances were also impaired (scaled score 5) in ‘AD stage 3’ group.
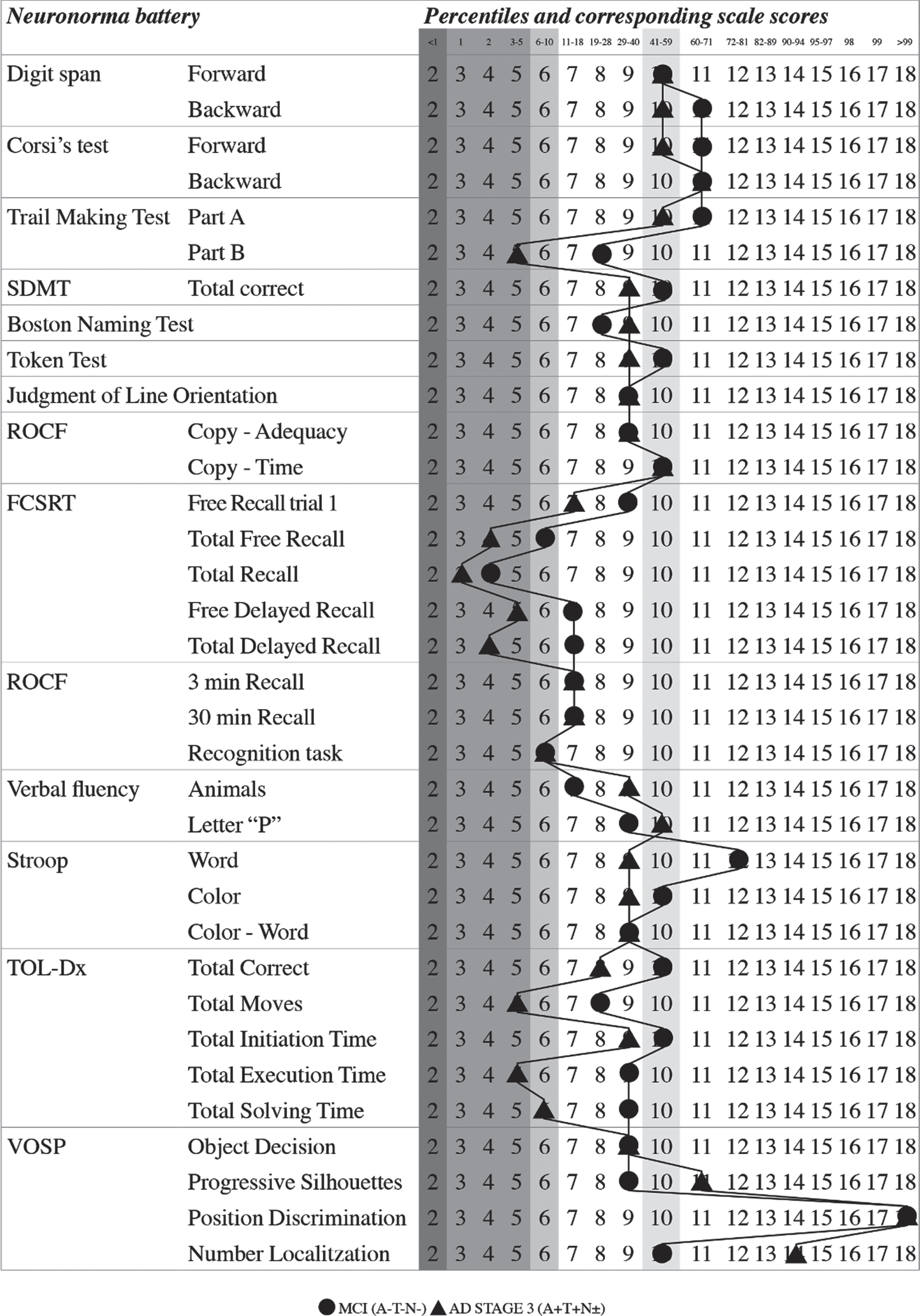
Cognitive profiles of AD stage 3 (A+T+N±) and MCI (A– T– N–) groups in the NEURONORMA battery. Medians of age- and education-adjusted scores are shown. Gray-scaled shading shows the impaired (2-5) and borderline (6) scaled scores (SS) and the mean (SS = 10) according NEURONORMA scoring system.
DISCUSSION
In this study, we explored the associations between the NEURONORMA cognitive battery and CSF biomarkers in a sample of CU, MCI, and mild DAT. As expected, we found differences among clinical groups, being memory, the domain showing the highest size effect values. We also show cognitive profiles in MCI groups classified by A/T/N system.
Association between CSF biomarkers and cognitive outcomes
In the overall sample, we found an association between almost all NEURONORMA variables and CSF biomarkers. CSF Aβ measures (Aβ42, Aβ42/Aβ40) and Aβ42/ t-tau, Aβ42/p-tau181 ratios showed a positive correlation with neuropsychological variables. Conversely, measures of tau protein (t-tau, p-tau181) had negative correlations with cognitive variables. Globally, correlations were significant, and the highest rho values were observed for memory and executive domains. Specifically, the strongest correlations were observed between the set of variables of the FCSRT and the ROCF and the ratios CSF Aβ42/t-tau and Aβ42/p-tau181, showing a clear association between memory and specific measures of AD biomarkers, as reported in previous studies with samples composed of CU, MCI, and AD subjects [21, 83]. However, no association was found between some cognitive and biological variables. These associations did not follow a specific pattern and were isolated cognitive variables as they did not represent a specific cognitive domain.
When comparing clinical groups, the results were consistent with previous studies [84–90]. CSF measures differences were found between cognitively impaired subjects and CU participants in all parameters and no differences were found between MCI and mild DAT subjects. The similarity between the MCI and mild DAT groups has probably been due to the proximity of the clinical stage of those groups. In addition, it may be related to the fact that, especially for amyloid levels, biomarker have already reached a plateau at these clinical stages, as steeper changes occur earlier in the disease [91].
Comparing cognitive measures among groups (Table 2), CU subjects performed significantly better in all cognitive tests as compared to impaired groups, except for P-dual from DT and VOSP - Position discrimination. DT is a new cognitive test and may depend on unknown factors. We hypothesize that the fact of adapting the difficulty of the task (span series length) to the actual capacity of each individual, may mask true differences in dual tasking ability. Besides VOSP subtest, scores showed a “ceiling effect” (maximum score) in all groups suggesting that a low performance on this could be pathognomonic of overt visuospatial alteration which is, in addition, a non-prevalent manifestation in mild stages of the typical variant of DAT.
As expected, all cognitive variables showed significant differences between mild DAT and CU subjects, and most of them also showed differences between CU and MCI subjects. These findings exemplify once more the cognitive deficits observed in neuropsychological tests in AD [92, 93] and in MCI, specifically in memory [94–96] and in executive functions [97–99]. Finally, as previously described deficits in executive functions domain [6] such as semantic fluency [102], planning and solving capacities [103–106], inhibition capacity [107, 108] comparing MCI and mild DAT subjects, we also found significant differences in many cognitive variables although their scores were closer. These results are in line with previous study results comparing these clinical groups with the NEURONORMA battery [62]. Previous work showed that all cognitive variables found significant differences between controls and DAT subjects and found similarities in Digit span forward, TOL-Dx Total initiation time and another visuospatial subtest of VOSP between controls and MCI. In addition, a decrease in cognitive scores was reported observed when the results of cognitive performance of the three clinical groups were plotted in a cognitive profile and run in parallel. These results allow us to expose that NEURONORMA battery is useful for distinguishing cognitive performance among CU, MCI, and mild DAT subjects. In addition, the present study also shows that, when comparing MCI and mild DAT, cognitive capacities decrease, while CSF core AD measures are similar. This leads to support the notion that a formal and extensive neuropsychological assessment is an essential diagnostic tool for accurate staging of cognitive impairment.
The effect size results showed that CU versus mild DAT were the less overlapped groups for all the study variables. Regarding the CSF measures, Aβ42/t-tau and Aβ42/p-tau181 obtained the highest Cohen’s d values with a large effect between CU subjects and both impaired groups and a moderate effect comparing MCI and mild DAT subjects. This finding concurs with previous studies that have shown the better discrimination and increase diagnostic accuracy of biomarkers combination indexes between controls and AD patients [86, 101]. Comparison between cognitively impaired groups showed the smallest effect size. Unexpectedly, Aβ42 showed a larger effect (Cohen’s d value 0. 65) than t-tau and p-tau181 (Cohen’s d values 0. 53 and 0.50 respectively). Although these values are not notably different, it was expected that values of tau proteins to be more discriminative than Aβ42 due to their late alteration according to in vivo AD biomarkers studies [91]. One reason that may explain this fact is a higher prevalence of subjects with non-AD etiology in the MCI group compared to mild AD. Regarding the cognitive outcomes, comparing CU and mild DAT groups, memory tasks showed the largest effect size, with Cohen’s d values were >3 in episodic verbal memory (FCSRT test), and specifically the values of delayed and total recall, that resulted >4, can be considered as having near-absolute discriminative ability [102]. The values from visual memory (ROCF), executive functions (TOL-Dx total moves and execution and solving time, SDMT total corrects, semantic fluency, Stroop Color-Word), and language (BNT total correct) also had a large effect size (Cohen’s d around 2). In the remaining comparisons (CU versus MCI and MCI versus mild DAT) it was found that, again, performances in memory tasks (FCSRT and ROCF) were the most helpful when discriminating between groups, followed by executive functions (semantic fluency and TOL-Dx variables).
These results confirm that impaired episodic memory, and especially those involving semantic encoding, is the main cognitive change in AD [4, 92]. Our results support the recommendation of using the FCSRT as a gold standard test for the detection of memory loss in AD population [103]. Besides, our finding concurs with classical literature which exposes that AD presents with deficits in executive functions domain [6] such as semantic fluency [104], planning and solving capacities [105–108], inhibition capacity [109, 110]. And other cognitive capacities such as working memory [111] and language (i.e., naming) [5]. Our results are also in line with the previous findings published using the NEURONORMA battery in a different sample [62], in which the FCSRT and the ROCF obtained Cohen’s d values were ≥3, followed also by semantic fluency, SDMT and TOL-Dx time performances. Previous literature has shown that, although memory impairment in MCI subjects is the most indicative factor of having AD as underlying pathology and forms the core diagnosis of this entity [112] also executive functions are commonly affected [99].
Our findings showing that cognitive outcomes displayed larger differences than CSF are, once again, in line with previous studies with the NEURONORMA battery that showed a higher size effect of memory performances than common AD neuroimaging biomarkers [62]. Effect size analysis highlights that some cognitive performances, specifically those of memory and executive functions, could be more useful to discriminate between these states than CSF measures. This fact can be explained because a notable number of MCI and mild DAT subjects obtained minimal scores in some memory and executive tasks, and this may cause a greater distance between groups. Also, these cognitive tests are sensitive for detection of clinical symptoms over CSF measures (the recruitment of this study was based on clinical diagnosis). Another potential explanation is the fact that cognitive impairment follows a rather linear decreasing trajectory along AD continuum while CSF biomarkers may show a less linear trajectory (for instance, CSF Aβ reaches a plateau on early stages). In addition, cognitive assessments are used for describing the disease tracking and staging while CSF biomarkers are useful to determine the etiology of clinical symptoms.
NEURONORMA cognitive profile of A/T/N groups in MCI subjects
In the present study, A+/T+/N±were the most frequent biological variants in MCI, considering them as indicative of prodromal AD in agreement with other current A/T/N classification studies [113–118].
The NEURONORMA cognitive profile shows the performance on each cognitive variable after adjusting for age and education. In this case, comparing the mean profiles of the ‘AD stage 3 (A+T+N±)’ and “MCI (A– T– N–)’, we found that both show an almost identical trend. Therefore, there were not remarkable differences of cognitive outcomes between MCI groups regardless the AD CSF biomarkers status. The main feature of both profiles is that verbal episodic memory is the most affected cognitive domain, consistent with the entity’s own definition. Scaled scores of FCSRT outcomes, except for ‘free recall trial 1’, are ≤5, which were in the deficit range (> – 1.5 standard deviation) for ’AD stage 3 (A+T+N±)’ subjects, while ‘MCI (A– T– N–)’ group obtained slightly higher scaled scores in these variables, reaching scale scores of 7 (lower limit of normality, – 1 standard deviation) in delayed recall. On the other hand, we found in both groups a better performance on visual memory, as measured by the ROCF, compared with verbal memory. Although the ROCF is a test usually used to measure visual memory, it is well known that its performance is influenced by executive function and constructional ability. This result states once again that a primary amnesic syndrome is the main cognitive impairment that defines prodromal AD according to the lexicon proposed by Dubois et al. [103], and it is in line with previously mentioned studies about the association of low memory performances and AD biomarkers in MCI samples [17– 19, 37– 39]. Moreover, our results are in line with a previous work from Moscoso et al. [115] which showed a steeper decline in MMSE performance in those MCI subjects with a A+T+N+ profile. Notwithstanding these findings, it is pertinent to state that ‘MCI (A– T– N–)’ group also obtained deficit scores in FCSRT total free recall and total recall.
Regarding executive functions, ‘AD stage 3 (A+T+N±)’ subjects also showed a lower performance resulting in deficient and borderline performances (scaled scores of 5-6) in TMT Part B and TOL-Dx (total moves and execution and solving times) comparing with ‘MCI (A– T– N–)’ whose scores were in range of normality. Previous mentioned studies of association of cognition and MCI subjects according biomarkers outcomes also exposed similar findings [19– 21,38,41, 19– 21,38,41] and current works according to A/T/N profiles [113, 116].
Thus, our results suggest that delayed recall in verbal episodic memory and solving capacities may be sensitive cognitive variables to distinguish between MCI due to AD and non-AD MCI subjects. However, the small sample size of each group prevents from drawing strong conclusions.
Surprisingly, although both scale scores were in normal ranges, semantic fluency outcome was lower in ‘MCI (A– T– N–)’ subjects. It would have been expected a worse performance in ‘AD stage 3 (A+T+N±)’ as other work showed [23, 41].
Finally, we can summarize through NEURONORMA cognitive profile that ‘AD stage 3 (A+T+N±)’ subjects showed an amnestic multi-domain pattern (verbal memory and executive function impairment), thus considering as a population with a higher risk of developing dementia, as previous literature suggests [12, 119]. Although biomarker analysis is highly useful for AD diagnosis and treatment, neuropsychological characterization is still essential for the disease tracking and identification of patient’s deficits and for a better deployment of non-pharmacologic interventions [120].
Limitations
Our study is not free of limitations. The main ones are the limited sample size and the cross-sectional design. The moderate sample size has led to comparative analyses between groups of few subjects, which prevents us from finding differences that may exist at a population level. On the other hand, a longitudinal study would allow us to compare the progression of both cognitive performance and biomarkers. Regarding the inclusion criteria, we acknowledge that our clinically definition of the groups, especially the MCI one, may have decrease the internal validity in terms of neuropsychological characterization, but increases the external validity and the relevance of the results in real world clinical settings. We also acknowledge that we performed a high number of statistical tests, since we studied a comprehensive cognitive battery and a set of fluid biomarkers measures. Although no formal correction for multiple comparisons was applied, we observed low p-values (<0.001) in most of the comparisons between groups. Another limitation is the inclusion of subjects with cognitive complaints (61.9%) in the CU subsample. As the current literature states, subjects with subjective cognitive decline are a population at risk of subsequently developing MCI and dementia [121]. In this sense, this may also have led to a higher prevalence of preclinical AD [122]. Thus, although the results may be partially affected by the inclusion of individuals with complaints, we did not observe any difference between complainers and non-complainers neither in cognitive performance nor in CSF variables (data not shown).
Conclusions
In conclusion, we found that CSF Aβ42 and CSF tau biomarkers were associated to cognitive performance in the continuum of AD. Globally, clinical groups were different with respect to cognitive performances on the NEURONORMA battery showing a greater difference between CU and mild DAT subjects. CSF biomarkers were similar in MCI and mild DAT groups supporting the evidence of AD pathology in early stages of the disease and CSF levels seems to remain stable at the dementia stage. The largest effect size was found for memory outcomes, CSF Aβ42/t-tau and Aβ42/p-tau181 in all comparisons. Cognitive profiles in the MCI sample, using age and education adjusted scores, showed that episodic memory was the most impaired domain, followed by some executive tasks, with lower average scaled scores in individuals with evidence of AD pathology (A+T+N±).
Footnotes
ACKNOWLEDGMENTS
The authors would like to express their sincerest gratitude to the altruism of all the subjects of the present study as well as that of all the professionals from the different centers that have participated in it.
FUNDING
This research has not received specific support from public sector agencies, commercial sector, or non-profit entities.
CONFLICT OF INTEREST
GSB is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review. GSB has worked as a consultant for Roche Farma, S.A. and received funding from the Ministerio de Ciencia e Innovación, Spanish Research Agency, PID2020-119556RA-100.
MSC has worked as a consultant and on advisory boards for Roche Diagnostics International Ltd and has given lectures at symposia sponsored by Roche Diagnostics, S.L.U and Roche Farma, S.A. MSC receives funding from the European Research Council (ERC) in the framework of the European Union’s Horizon 2020 research and innovation program (European Union’s Horizon, Grant agreement No. 948677) and Marie Skłstrokodowska-Curie fellowship (No 847648 (LCF/BQ/PR21/11840004), as well as from the Instituto de Salud Carlos III (PI19/00155), and from Fundació la Caixa (ID 100010434).
ING receive funding from the Instituto de Salud Carlos III (ISCIII-FEDER, PI21/00194).
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding authors. Requests will be reviewed, and access will be granted if approved.