
Abstract
Background:
Hearing loss is common in people with dementia (PwD) and a modifiable risk factor for cognitive decline. Recent studies revealed that hearing loss could cause social isolation and depression, which is associated with health-related quality of life (HRQoL). However, there is a lack of knowledge about the impact of the utilization of hearing aids on these outcomes.
Objective:
To assess whether hearing aids use might be positively associated with the progression of cognitive function, depression, and HRQoL among PwD.
Methods:
We analyzed two-year follow-up data from 258 PwD (≥70 years, living at home). Cognitive decline was measured with Mini-Mental Status Examination (MMSE), depression using Geriatric Depression Scale (GDS), and HRQoL with Quality of Life in Alzheimer’s Disease Scale (QoL-AD). The impact of hearing aid utilization on the progression of outcomes was assessed using multivariate regression models.
Results:
123 patients had hearing loss (47.7%), from which n = 54 (43.9%) used hearing aids. Patients with hearing loss were older and had a lower HRQoL than those without hearing loss. Use of hearing aids in patients with hearing loss was associated with a lower increase in depressive symptoms (b = –0.74, CI95 –1.48 ––0.01, p = 0.047) over time as compared to those not using hearing aids. There was no effect on PwD’s cognition, and the association with higher HRQoL was significant after one, but not consistently over two years.
Conclusion:
Early detection and intervention of presbycusis using hearing aids might improve mental health and HRQoL in dementia.
INTRODUCTION
With the increase in global life expectancy, age-related chronic diseases such as hearing loss and cognitive decline became more prevalent among older populations, presenting urgent public health issues [1]. Hearing loss is ranked as one of the top three chronic diseases and the number one communication disorder among the aged [2]. Despite the high prevalence of hearing loss and its adverse effect, only a small percentage of older adults use their hearing aids [3, 4]. Dementia is a chronic neurodegenerative condition, which causes persistent impairment in several mental cognitive tasks that interfere with daily life [5]. There is an estimated number of around 55 million people worldwide living with dementia and around 10 million new cases yearly [6]. If unmodifiable risk factors that contribute to the progression of dementia, e.g., genetic predisposition, gender, and age, as well as modifiable factors such as hypertension, diabetes, obesity, lack of physical exercise, depression, social isolation, and hearing loss would be identified early and targeted effectively by specific interventions, the deterioration of dementia could be prevented or decelerated [7, 8].
The link between hearing loss and dementia in the auditory brain is poorly understood. However, it is reported that a hearing deficit of ∼25 dB affects cognitive deterioration equivalent to 6.8 years of aging, and it concluded that hearing impairment is independently associated with lower scores on memory tests [9]. Other studies found a significant association of hearing loss with more rapid cognitive decline [10], as well as with mild cognitive decline and Alzheimer’s disease dementia where the authors concluded that auditory tests in a cognitive screening might play an important role in the early diagnosis of cognitive decline [11]. Due to the lack of curative treatment for cognitive impairment and dementia [12] and the large number of studies that revealed an association between presbycusis and dementia, more attention is needed to identify and treat modifiable risk factors such as hearing loss [13, 14]. Literature suggests a theory where auditory deterioration either has a direct effect on cognitive function due to poor input or indirectly through the impact of hearing impairment on social isolation and depression [15]. Under this assumption, it could be hypothesized that hearing devices could positively affect cognitive abilities [16]. Current literature underlines the necessity for a deeper insight into the link between hearing aids and the progression of dementia. A large cross-sectional study of adults aged 40–69 years indicated a positive association between hearing aid use and better cognition; yet a lack of association between hearing aids and depression [17]. However, evidence is still lacking in an older population, where cognitive dysfunction, usage of hearing devices and depression are prevalent.
Given the mentioned associations and outcome parameters, health-related quality of life (HRQoL) among dementia patients must be taken into consideration as it might change throughout their condition [18] and is regarded accordingly as a relevant outcome to assess interventions in dementia care [19]. For instance, a randomized controlled trial (RCT) evaluated the alteration in HRQoL of patients with dementia living in care homes and observed an association between life quality and changes in mood and cognition [20]. It was also indicated that quality of life does not automatically decrease as dementia progresses [21] but is rather highly affected by the patient’s mood and interaction with their surroundings [20]. Taking this into account, as well as the negative impact of hearing loss on social function [22], we included potential benefits of hearing aids on HRQoL among people with dementia (PwD) in our longitudinal study design. Therefore, the aim of this study is to evaluate whether the utilization of hearing aids is associated with better cognitive performance and mental health and has a positive effect on life quality among people with cognitive impairment and dementia.
METHODS
Study design
This study was based on data from the ongoing general practitioner (GP) based study DelpHi-MV (Dementia: life- and person-centered help in Mecklenburg-Western Pomerania), a longitudinal, cluster-randomized controlled trial (cRCT) with two arms and yearly follow-ups. A detailed description of the design, the sample and the intervention of this trial is given in more detail elsewhere [23, 24]. The study sample consists of people positively screened for dementia by their treating general practitioner. Inclusion criteria were being older than 70 years, living at home, and having been positively screened for cognitive impairment using the DemTect instrument [25]. Exclusion criteria are medical conditions that would complicate further testing as well as language barrier [26]. Written informed consent was obtained by the participant or a legal representative. The study procedure was approved by the Ethical Committee of the Chamber of Physicians of Mecklenburg-Western Pomerania, registry number BB20/11) and the study is registered with clinicaltrials.gov (Identifier: NCT01401582). The enrollment into the main study started on January 1, 2012, and ended on December 31, 2014, yearly follow-ups were conducted since then.
Participants received identical, standardized, computer-assisted baseline assessments conducted as face-to-face interviews at the participants’ homes. After that, the control group received “care as usual”, while the intervention group received the multi-disciplinary and multimodal-based “DelpHi-Intervention” [23], which intends to provide an individualized “optimum care” in dementia within the established health care and social service system [26].
Study population
A total of 6,838 patients were screened for dementia in 125 participating GP practices. 1,167 patients (17.1%) of these qualified for the DelpHi-MV trial, and 634 patients (54.4%) of these provided informed consent to participate in the study. One hundred eighteen dropped out of the study before the baseline assessment due to withdrawal of informed consent (n = 85); death (n = 19); relocation (n = 5); or other reasons (n = 9). Figure 1 shows the study participants through each stage of the DelpHi-study. Out of the 516 participants, 258 completed the 2nd year follow-up, providing a complete data set with all variables needed for this analysis. The present analyses are based on the data of these 258 patients. A comparison of included and excluded patients revealed no differences in patients’ sociodemographic variables between included and excluded patients. However, patients included in this analysis were less cognitively impaired and had lower depressive symptoms than excluded patients (see Supplementary Table 1).
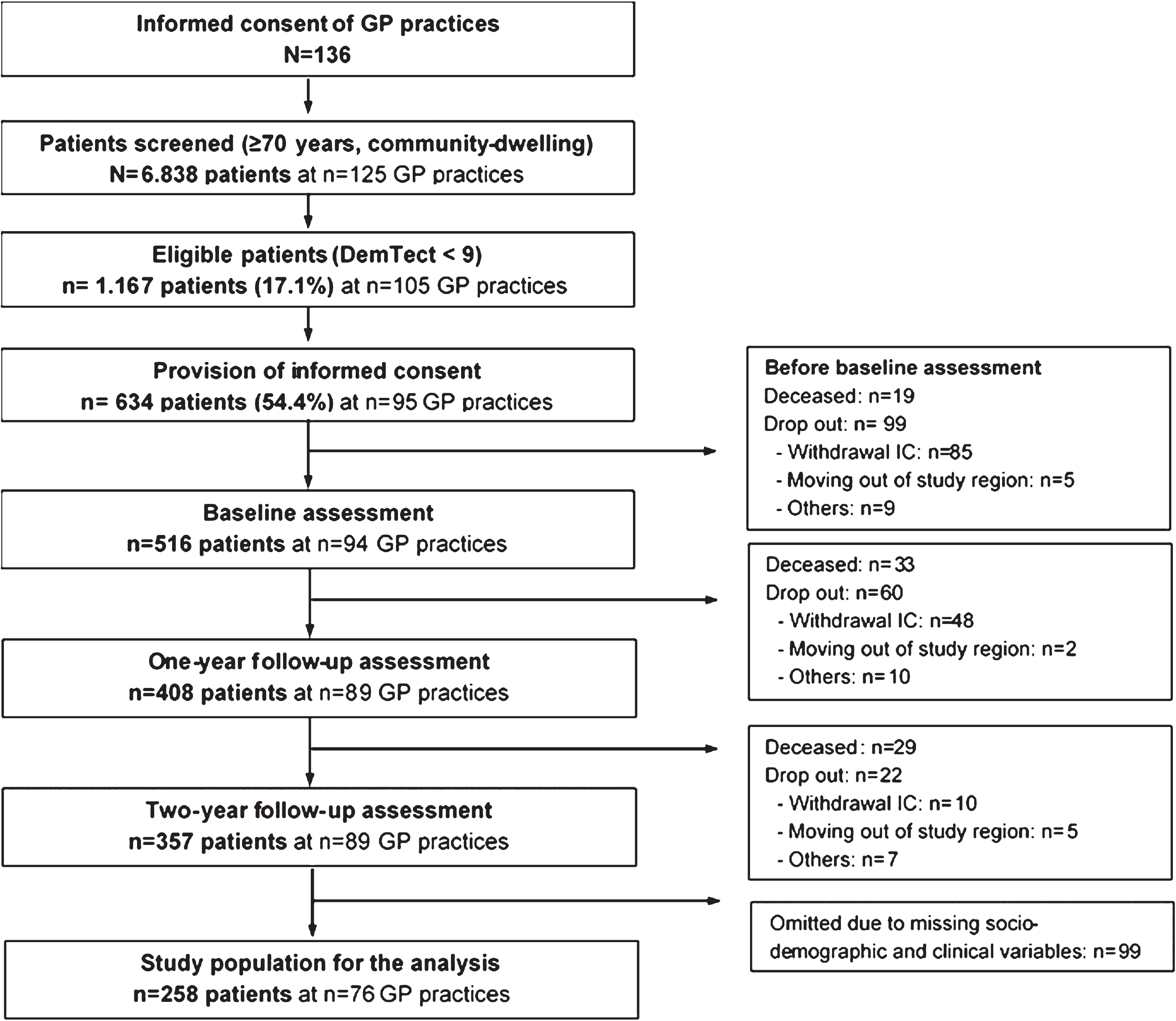
Flow of the study participants through each stage of the DelpHi-study.
Procedures and instruments
To assess patient’s hearing loss and their utilization of hearing aids, patients responded to related screening dichotomous (yes/no) questions, “Do you have hearing problems?” and “Do you use a hearing aid?”, where interviewers were instructed to ask the questions as clearly as possible. For data accuracy and quality purposes, caregivers (if available) were invited to join the interview.
To describe the socio-demographic and clinical characteristics of the study sample, we assessed variables including sex, age, living situation (alone/not alone), cognitive function, depression, and quality of life. Cognitive function was evaluated using the German version of the Mini-Mental State Examination (MMSE) [27]. Any score between 27–30 (out of 30 points) indicates “no cognitive impairment”. Below this, scores can indicate “mild” (points 20–26), “moderate” (points 10–19), and “severe cognitive impairment” (points 0–9). Geriatric Depression Scale (GDS) was used to measure depression (a score of 0–5 indicates “no depression"; Score 6–15: “depression") [28]. Patient’s HRQoL was assessed using the mean score of the Quality of Life in Alzheimer’s Disease Scale (Qol-AD), a questionnaire comprising 13 items designed to obtain both a patient and a caregiver report for the patient’s HRQoL. Answers range between 1 (poor) to 4 (excellent), and total scores are obtained by the sum of all items, ranging from 13 to 52 [26, 29].
Statistical analyses
Descriptive statistics were calculated to describe the socio-demographic and clinical characteristics of the population. For univariate subgroup analyses, the patients were categorized into the following groups: 1) Patients without hearing loss, and 2) patients with hearing loss. We tested for statistically significant differences between the subgroups with Welch’s t-test for continuous and Fisher’s exact test for categorized variables. Multivariate regression analyses were applied to analyze the impact of hearing loss as well as of the utilization of hearing aids (predictor variables) on the progression of cognitive impairment, depressive symptoms, and HRQoL (variables of interest). To identify differences in these outcomes over the years, we used the delta (difference between baseline and two years after) of these outcome variables. All models were adjusted for socio-demographic (age, sex, living situation), PwDs comorbidity and the baseline value of the outcome variable. All multivariate models also included dummy variables indicating the belonging of the PwD to the intervention or the control group, adjusting for the impact of the intervention on outcomes. Also, the DelpHi-trial is a cluster-randomized trial, where it is important to consider the dependency of data from participants who are part of the same cluster (i.e., the same GP). Accordingly, we used generalized least square (GLS) regression with random effects for GP practices, which can give consistent estimates in cases of clustered data. The statistical analyses were carried out using Stata version 15.1 (StataCorp) [30].
RESULTS
The socio-demographic and clinical characteristics of the study population are displayed in Table 1. In this sample, PwD were on average 79.9 years old, 60.5% were female, and about 52% indicated living alone. Based on the MMSE, people under examination were on average mildly cognitively impaired (mean MMSE score = 23.5). In the GDS test, 13.6% scored more than 6 points, which indicates mild depression. The HRQoL was ‘average’ or ‘rather good’ (mean = 2.8 on a scale from 1–4). Nearly half of all observed patients suffered from hearing loss (47.7%), and only 43.9% of those stated the use of hearing aids. Patients with hearing loss had a significantly lower HRQoL (2.7 versus 2.8, p = 0.021) and a higher age (80.8 versus 79.0, p = 0.005) compared to patients without hearing loss. Otherwise, according to all other socio-demographic and clinical variables, there were no statistically significant differences between patients with and without hearing loss.
Sociodemographic and clinical variables of the study sample at baseline
MMSE, Mini-Mental State Examination; range 0–30; higher score indicates better cognitive functioning; GDS, Geriatric Depression Scale, sum score 0–15; score ≥6 indicates depression; QOL-AD, Quality of life in Alzheimer’s disease; mean sum score 1–4, higher score indicates better quality of life; *Fisher’s exact test; †Welch’s t-test. Bold p-values indicate p < 0.05.
Patients’ change in clinical characteristics and quality of life over time from baseline to the two-year follow-up is demonstrated in Table 2. Comparing patients with and without hearing loss and patients utilizing and non-utilizing hearing aids, cognitive impairment and quality of life did not change significantly over time. However, depressive symptoms, according to the GDS increased more intensively over time in patients with hearing loss compared to patients without hearing loss (+0.02 versus +0.6, p = 0.047). Patients with hearing loss utilizing hearing aids also had a lower increase in depressive symptoms over time compared to patients with hearing loss not using hearing aids (+0.09 versus +1.0, p = 0.042).
Change in clinical characteristics and quality of life over time
MMSE, Mini-Mental State Examination; range 0–30; higher score indicates better cognitive functioning; GDS, Geriatric Depression Scale, sum score 0–15; score ≥6 indicates depression; QOL-AD, Quality of life in Alzheimer’s disease; mean sum score 1–4, higher score indicates better quality of life. Bold p-values indicate p < 0.05.
The multivariate analyses could confirm these results. Whereas we could not find any significant association between hearing loss on patients’ change in depression, quality of life and cognition over time (see Supplementary Table 2), hearing devices use was significantly associated with a reduction of depressive symptoms measured by the GDS, after one (b = –0.85, CI95 –1.46 ––0.24, p = 0.006) and two years (b = –0.74, CI95 –1.46 ––0.01, p = 0.047). Among patients with hearing loss, we could also not identify a statistically relevant association between the utilization of hearing aids and the change in cognitive impairment. Furthermore, there was a significant association between the utilization of hearing aids and patients’ quality of life (Qol-AD) after one year (b = 0.12, CI95 0.04 –0.21, p = 0.047) but not after two years, indicating an inconsistent finding. The results of the multivariate analyses are summarized in Table 3.
Multivariate analysis of the impact of hearing aid utilization on clinical and patient-reported outcomes in n = 116 patients with hearing loss
MMSE, Mini-Mental State Examination; range 0–30; higher score indicates better cognitive functioning; GDS, Geriatric Depression Scale, sum score 0–15; score ≥6 indicates depression; QOL-AD, Quality of life in Alzheimer’s disease; mean sum score 1–4, higher score indicates better quality of life; HA, hearing aid; *Bold p-values indicate p < 0.05.
DISCUSSION
Utilizing hearing aids in PwD with hearing loss was not significantly associated with cognitive function. However, a slower progression of depressive symptoms after one year (b = –0.85, CI95 –1.46 ––0.24, p = 0.006) and after two years (b = –0.74, CI95 –1.48 ––0.01, p = 0.047) was observed in those utilizing hearing aids compared to those who did not. Whereas we found an improvement in quality of life after one year (b = 0.12, CI95 0.04 –0.21, p = 0.005), this association was mitigated by the second year, demonstrating an inconsistent finding.
Hearing ability and utilization of hearing aid in our study sample were measured subjectively using single dichotomous questions (Yes/No). Subjective assessment of hearing ability could be less reliable, valid, and biased. However, objective assessment such as having a hearing loss diagnosis in GP file could also lack completeness because hearing loss is underdiagnosed and often unaddressed in primary care [31]. Taking into account, GPs in Germany play an important role in care coordination with other specialists, which implies that GP patient’s records would include diagnoses given by any specialist including audiologists the patient has previously visited [32, 33].
Different population-based studies from the U.S. assessed the association between the use of hearing aids and the development of the cognitive function. An 8-year longitudinal survey, including adults aged ≥66 (mean = 75.8) years reported the utilization of hearing aids was linked with a delayed diagnosis of Alzheimer’s disease dementia among older adults with hearing loss [34]. Another longitudinal 20 years study assessed adults aged ≥50 (mean age of first-time hearing aid use = 63 years) and revealed that early use of hearing aids in the course of hearing impairment may have an impact on cognitive decline trajectory, potentially causing a reduction of rising prevalence of dementia globally [35]. In contrast to our findings, both papers indicated a positive association between hearing aids utilization and cognitive performance. A potential reason for the divergence of findings could be the younger age of their study samples, which drew our attention to possible benefit of early interventions on the progression of dementia. Intervention in our study subjects was provided at an age of 70 or older (mean = 79.9), which may reduce chances of cognitive function stabilization. Additionally, the duration of two years in our sample might have been insufficient to examine longer-term impact of aided hearing on trajectory of cognitive performance, depression, and patient-reported outcomes. According to Alzheimer’s Association, patients with AD live an average of four to eight years after diagnosis [36]. Considering this time frame and the older age of our sample already diagnosed with AD, a study duration of two years is deemed reasonable.
A small percentage of our participants with hearing loss (43.9%) used their hearing devices. This confirms previous findings showing a very low rate of patients in need of hearing aids [37, 38], where hearing aids effectiveness (e.g., type, suitability of the device) as well as patient adherence play an important role [39]. Previous studies discussed potential factors that may contribute to a low rate of hearing intervention compliance such as problems with commitment to technology among aged adults, health status, lower socioeconomic status and self-reported hearing performance, and expectations about hearing aids and support from relatives [40, 41]. More attention on influencing contributors is needed to facilitate an early intervention using hearing devices, shortening the delay in device acquisition after prescription of hearing aids, as well as motivating owners of hearing devices to maintain their daily usage [40, 42].
Prior research has emphasized the association between depression and hearing loss [43]. Our results showed that the utilization of hearing aid is associated with an improvement in depression within two years, similar to findings in other observational studies revealing that hearing aids not only to be associated with improved depressive symptoms but also have a protective effective on depression [44, 45]. Furthermore, previous small single-arm studies documented that the short-term (3–6 months) usage of hearing aid is associated with improved depression symptoms and psychosocial well-being [46, 47]. We did, however, see a tendency towards the reduced impact of hearing aid use on depressive symptoms in the second year in our findings (b = –0.74, CI95 –1.46 ––0.01, p = 0.047) compared to the first year (b = –0.85, CI95 –1.46 ––0.24, p = 0.006). This could indicate that the effect of hearing aids support is transient. Previous literature has reported the benefits of enhancing hearing on mitigating social isolation and depression accordingly [48]. Nevertheless, we must consider that depressive symptoms in our data may rather be related to other (multiple) factors and are not causally related to hearing loss. Further psychological interventions may be required. Future research may conduct additional longitudinal studies to examine longer-term influence of hearing aids utilization and the duration of their positive impact on depressive symptoms, as well as the possibility of prolonging their benefit on mental health through earlier intervention. On the other hand, other studies showed no association between hearing aids use and depression [17, 49], either explained by inadequate sensitivity of their assessment based on responses to a single screening question “Over the past two weeks, how often have you felt down, depressed or hopeless?” [17], or a possible lack of differentiation between hearing aid ownership and hearing aid use in numerous studies, which in turn may lead to uncertain findings [43]. Also, our results may have been affected by exclusion of patients who did not complete the 2-year follow-up visit, who had higher rates of cognitive impairment and depression at baseline. Therefore, further research is needed to replicate findings of this study.
For HRQoL, our results showed a positive association with hearing aids in the first year (b = 0.12, CI95 0.04 –0.21, p = 0.047), yet no association after the second year. Sarant et al. presented similar findings, where participants aged 62–82 years with hearing problems were fitted hearing aids for 18 months and reported an overall enhancement in quality of life. However, the MMSE score of their participants was m = 28.7, while ours was m = 23.5, which indicates a relevant disparity in study samples in terms of cognitive performance [50]. Another double-blind randomized placebo-controlled trial evaluated the impact of hearing aids on HRQoL of 51 patients with hearing impairment and Alzheimer’s disease over a period of 12 months and, conversely, revealed no proof of life quality improvement [51]. Despite the high value of randomized trials, a further study with a larger number of participants may be required to confirm these results. As we did not control other factors that may affect quality of life in PwD such as pain management, communication, and physical and behavioral symptoms communication [52], mood and cognition, etc. [53], we cannot exclude the possibility that this improvement was influenced by other factors and not only due to hearing aids utilization. Hence, we recommend future research focusing on lifestyle and social interaction factors when assessing the impact of hearing loss and aids on cognitive decline, depression, and HRQoL. This applies likewise to cognitive function and depression.
Other limitations should be considered when interpreting our results. The inadequate sensitivity of hearing ability measurement and hearing aids utilization measurement via response to the screening questions restricts the generalizability of our results even though objective assessments such as having a hearing loss diagnosis in GP file could possibly lack completeness due to underdiagnosed and often neglected hearing loss in primary care. Further extended longitudinal interventional studies with a focus on hearing are needed for more precision, where an initial objective hearing assessment and a subsequent obtainment of hearing aids take place, and the measured effects are solely related to the hearing intervention. This would reduce measurement and misclassification concerns.
Furthermore, although answering the single question “Do you use a hearing aid?” shows treatment adherence, there is no data available on number of hours per day or other frequency measures of patient’s devices use, nor on the appropriateness of their fitting, auditory/speech perception, and communication. It is challenging to identify an appropriate compliance measurement tool for hearing aids usage [39]. A recent study analyzed remote data logging using smartphone-connected hearing aids which was found to be more accurate in providing information about hearing aids usage patterns and the environmental factors in which they were used [54]. This kind of tool was, however, not available during the Delphi-MV trial. Therefore, the generalizability of the demonstrated results is limited. Uncertainty is given about whether or not the impact of aided hearing on outcomes is caused by poorly fitted hearing devices or inadequate compliance. Thus, the identification of appropriate measurement tools for monitoring hearing aids treatment compliance and effectiveness in aged and cognitively impaired adults is of great importance for the future. Moreover, despite MMSE being one of the most frequently used cognitive assessment tools in clinical trials and research among the aged [55, 56], it has been criticized to be insensitive concerning the detection of subtle changes during mild cognitive impairment (MCI) stages [57]. Thus, the use of MMSE with our sample (mean = 23.5) could be a reason for the lack of association between hearing aid use and cognitive function. We, therefore, recommend using other adequately sensitive tests such as MoCA when investigating a sample with MCI [58]. Moreover, MMSE is less sensitive in detecting executive functions such as the ability to plan, focus, working memory and self-control [59]. Considering that hearing aids have a positive effect on the cognitive domain of executive function [60], MMSE would most likely be limited in detecting executive function improvements caused by hearing aids in our study sample. Finally, having a small sample size (n = 54 using hearing aids) is a result of hearing aids prevalence in our study that could restrict the generalizability of results presented in the regression models although the models showed a significant association.
This study did not observe that the use of aided hearing is associated with enhanced cognitive performance among people with cognitive impairment and dementia; however, finding that the use of hearing devices is associated with improved depressive symptoms within two years supports previous findings in the literature, which may encourage early identification of hearing difficulties and provision of appropriate interventions in order to improve mental health among the aged. Additionally, our analysis revealed a transient benefit of hearing aids on life quality for one year, which requires further research to consider lifestyle and social interaction factors that might affect HRQoL and hearing aid use. Other extended longitudinal studies and RCTs might also be valuable to confirm our research findings.
Footnotes
ACKNOWLEDGMENTS
The authors acknowledge Aniela Angelow, Grit Aßmann, Georgia Böwing, Adina Dreier-Wofgramm, Thomas Fiß, Daniel Fredrich, and Leonore Köhler. An experienced field study team provided support with data collection and data management: Ines Abraham, Kerstin Albuerne, Vaska Böhmann, Kathleen Dittmer, Sarah Gardzella, Jana Hubert, Ulrike Kempe, Viktoriya Kim, Julius Krause, Andrea Pooch, Saskia Moll, Melanie Reimann, Sabine Schmidt, and Christine Winckler. They thank all participating patients and their caregivers as well as the participating general practitioners for their most valued collaboration.
FUNDING
The authors would like to acknowledge that the DelpHi-MV-trial (Dementia: Life- and person-centered help in Mecklenburg Western Pomerania) and was funded by the German Center for Neurodegenerative Diseases (DZNE) and the University Medicine of Greifswald.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author.