
Abstract
Background:
The SARS-CoV2 global pandemic impacted participants in the Alzheimer’s Prevention Initiative (API) Autosomal Dominant Alzheimer’s Disease (ADAD) clinical trial, who faced three stressors: 1) fear of developing dementia; 2) concerns about missing treatment; and 3) risk of SARS-CoV2 infection.
Objective:
To describe the frequency of psychological disorders among the participants of the API ADAD Colombia clinical study, treated by a holistic mental health team during the COVID-19 pandemic. The extent of use of mental health team services was explored considering different risk factors, and users and non-users of these services were compared.
Methods:
Participants had free and optional access to psychology and psychiatry services, outside of the study protocol. Descriptive statistics was used to analyze the frequency of the mental health difficulties. A multivariable logistic regression model has been used to assess associations with using this program.
Results:
66 participants were treated by the Mental Health Team from March 1, 2020, to December 31, 2020. Before and after the start of the pandemic, the most common psychological problems were anxiety (36.4% before, 63.6% after) and depression (34.8% before, 37.9% after). 70% of users assisted by psychology and 81.6% of those assisted by psychiatry felt that the services were useful for them. Female sex, depression, and anxiety before the pandemic were positively associated with being assisted by either psychology or psychiatry, while the association with hyperlipidemia was negative.
Conclusions:
A holistic mental health program, carried out in the context of a study, could mitigate psychopathology during pandemics such as COVID-19.
INTRODUCTION
In 2019, the outbreak of the illness caused by SARS-CoV-2, termed COVID-19 by the World Health Organization, the acronym derived from “coronavirus disease 2019”, occurred and quickly became a pandemic [1, 2]. The impact of the pandemic on public health caused psychological and psychiatric difficulties globally. These have arisen both from the direct effects of the infection on the survival of affected people (mortality and post-COVID effects) [3, 4], as well as indirectly through the measures adopted to control the propagation of the virus (e.g., social isolation, curfews, working and studying from home, economic consequences of the restrictions) [3–5].
Some of the mental health problems described over the course of the pandemic include: stress, moderate to severe anxiety [2, 6], depression, insomnia, obsessive symptoms, pathological grief, substance abuse and addiction, psychosomatic disorders [3, 8], acute pandemic stress (stress related to a pandemic that is perceived as an unstoppable and deadly catastrophe without any chance of escaping it) [3], and family conflict, sometimes involving domestic abuse [9]. Emotional wellness has been negatively affected both in people with and without prior history of anxiety, depression, or obsessive-compulsive disorder, particularly in people with severe illness, who perceived a greater impact on mental health [10].
Vindegaard and Benros identified various factors related to high levels of psychiatric symptoms or low levels of psychological wellbeing, specifically, female sex, frontline workers, and self-classification as poor. Psychological wellbeing self-classification as poor could be frequent in participants in clinical trials for catastrophic or highly incapacitating diseases such as cancer, chronic pain, or various psychiatric and neurological disorders [8]. Unfortunately, these studies, which aim to improve life expectancy and wellbeing of patients, were also significantly affected by the pandemic.
Unger et al. reviewed 62,252 interventional and observational oncological, cardiovascular, and mental health studies between 2015 and September 2020, finding that during the initial outbreak of the pandemic (February to May 2020), the rate of monthly trial activations were 57% (201.5/month) of the value expected, that was 355.6/month (RR = 0.57, CI95% 0.52-0.61, p < 0.001) [11]. Moreover, the pandemic led to the suspension of or adjustment to several clinical studies related to Alzheimer’s disease (AD), affecting recruitment, administration of medicines, and monitoring visits, and resulting in protocol amendments being required to deal with missing data, deviations, loss of participants, and to allow the use of telemedicine [4, 12]. This disruption of clinical studies particularly affected patients and their families in drug trials, leading to considerable uncertainty and even desperation [4].
In recent years the use of technology has taken on special importance in the healthcare of people without easy access to in-person specialized services [13]. The use of technology can help to reduce the negative emotional, cognitive, and behavioral effects of the pandemic in clinical studies for the prevention and treatment of catastrophic diseases such as dementia, thereby strengthening the ability or willingness of individuals to continue participating in research studies subsequently and during and potential future pandemics [8, 14]. The objective of this report is to describe the frequency of new psychological disorders and the exacerbation of pre-existing disorders among the participants in the Alzheimer’s Prevention Initiative (API) Autosomal Dominant Alzheimer’s Disease (ADAD) Colombia clinical trial, who were treated by a holistic mental health team via telecare over the course of the COVID-19 pandemic. Additionally, the extent of use of mental health team services was explored taking into account different risk factors, and users and non-users of these services were compared.
METHODS
Participants
The participants in this study come from a group of 252 people belonging to the API ADAD clinical trial. This was a double-blind, placebo-controlled parallel-group study in preclinical PSEN1 E280A mutation carriers randomized to crenezumab or placebo, and in non-randomized, placebo-treated non carriers, that evaluated the efficacy and safety of the drug crenezumab in modifying the evolution of cognitive functioning.
Recruitment for the study began in December 2013 and finished in February 2017 [15, 16]. The sample for this analysis are aged 30 and above, including both carriers and non-carriers—subjects with or without a mutated copy of a gene, respectively—of the genetic variant PSEN1 E280A, which is associated with the onset of mild cognitive impairment (MCI) around the age of 44 (CI 95% 43-45) and subsequently dementia around 49 (CI 95% 49-50) [15, 17].
Crenezumab was provided in one of the research centers every two weeks (if delivered subcutaneously) or every four weeks (if delivered intravenously) [15]. Participants who developed MCI or dementia due to AD could continue with treatment in the study [15]. Those who decided to suspend treatment could continue to be followed per protocol without receiving drug or placebo [15].
Procedures
Participants in the API ADAD clinical trial could access a program outside the protocol called the Social and Mental Health Plan, which offered psychoeducation as well as evaluation and monitoring by the psychology, family therapy, and psychiatry services for all the members of the PSEN1 E280A families. This program was created in 1992 with the first Neuroscience Group of Antioquia (Grupo de Neurociencias de Antioquia, GNA) research projects, and got stronger in 2000 thanks to the “Forget me not” initiative, a program to raise funds through private donations and social and academic activities, to provide assistance to Colombian families and individuals with limited financial resources affected by AD or other dementias. In 2015, the GNA included psychiatry and clinical psychology services to the Social Plan, starting the Social and Mental Health Plan as is currently known.
Patient recruitment
The Social and Mental Health Program was promoted by the Principal Investigator and Sub-investigators when the Informed Consent WAS explained is explained. The participants were evaluated by the sub-investigators every fifteen days or every month, according to the API-Colombia trial protocol. The medical sub-investigator offered evaluation by the mental health team of the GNA to those clinical trial participants, or their caregivers in the case of patients with dementia, who showed neuropsychiatric symptoms suggestive of anxiety, depression, psychomotor restlessness or agitation, psychosis, apathy, verbal or physical aggressiveness, problems initiating or maintaining sleep, and other disorders. Likewise, the participants could ask to their subinvestigator for a psychological or psychiatric evaluation.
If the participant, or both the participant and their caregiver in cases where the patient had dementia, accepted this offer, the referral process was carried out in an electronic medical record system specific to the research group for the registration of medical records. When entering the medical history of each participant, orders could be entered to create a request for assessment by the psychology, family therapy or psychiatry service, according to what the sub-investigator deemed pertinent for the patient. Psychology could also refer patients to psychiatry and vice versa.
Care protocol
Once the psychology or psychiatry teams received the referral via email, the representative professionals proceeded to communicate with the patient in order to arrange the date and time of the assessments, which were originally conducted in-person. However, after the onset of the COVID-19 pandemic and given the immediate need for mental health care for clinical trial participants and caregivers, assessments were carried out remotely, in order to minimize the risk of contagion. This was done either on the telephone or via an online videocall platform. All the participants agreed to be evaluated by phone or a videocall during pandemics.
During the consultation, the mental health professional interviews the patient, makes a diagnosis, makes decisions regarding treatment (i.e., therapy sessions, medication), suggests any tests they consider necessary, and arranges a follow-up consultation with the patient.
Specifically, in the initial consultation, the psychologist interviewed the patient, made a diagnosis, and recommended a treatment based on the most suitable options and in accordance with institutional protocols for managing the identified clinical condition. They also determined the need to refer to other services such as social work, family therapy, or psychiatry, and finally scheduled a follow-up appointment. The psychiatrist, in addition to what was done by psychology during the first consultation, could request diagnostic aids, and ultimately recommended a pharmacological and/or non-pharmacological treatment, depending on the patient’s health condition. This initial consultation lasted for one (1)hour.
Both the psychological and psychiatric evaluations aimed to identify symptoms and signs of mental impairment that manifested as alterations in affect, cognition, and behavior, as well as the implications these had on basic activities of daily living.
Follow-up appointments, which were scheduled immediately after the initial consultation and subsequent ones, had a duration of 30 min or 45 min, depending on the patient’s situation. During these appointments, the patient’s medical history was reviewed, they were questioned about their current physical and mental health status, conversations could take place with their companion, and psychotherapy was applied, or the pharmacological treatment was adjusted if necessary.
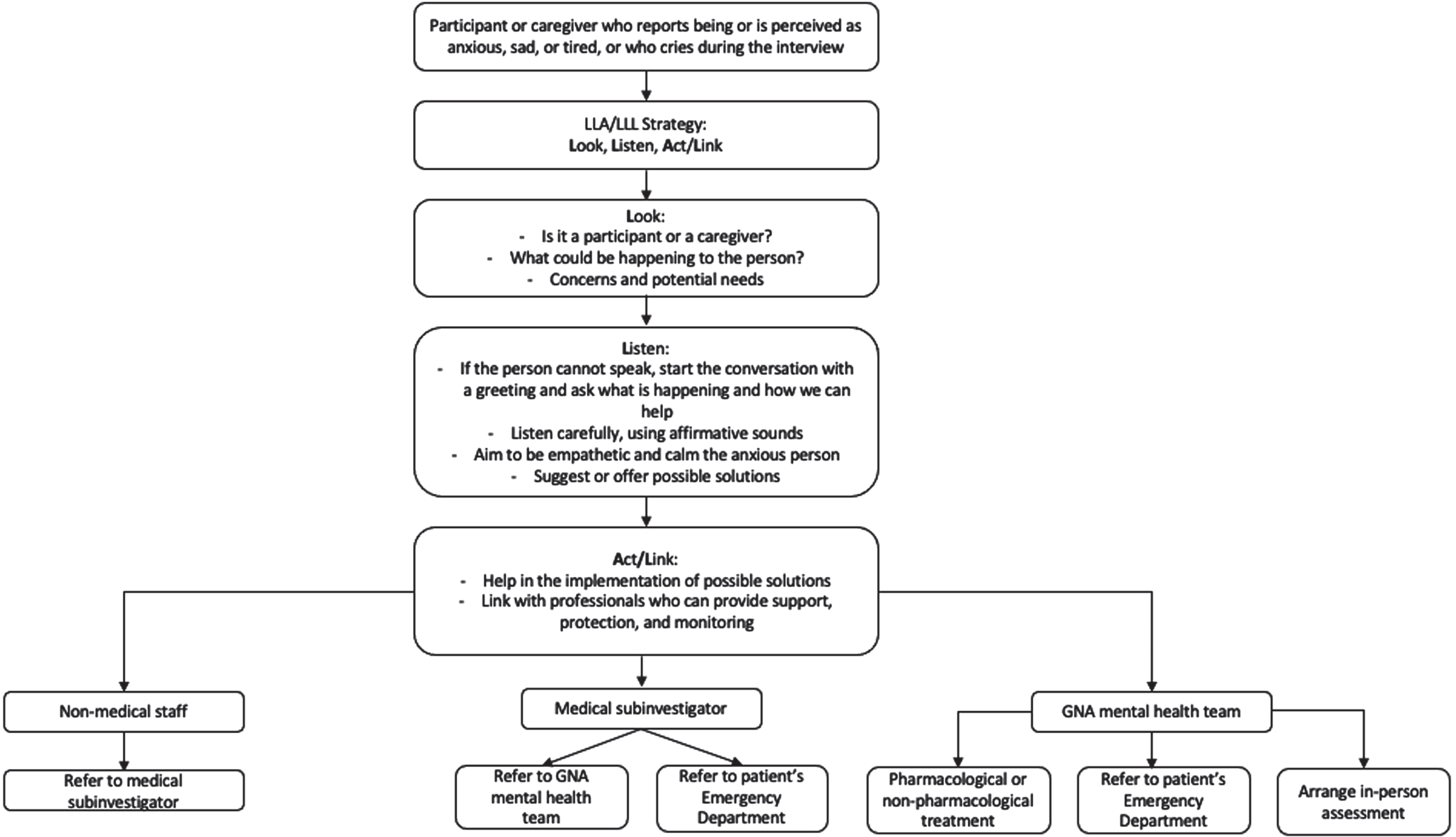
In some situations, a family member or caregiver of the patient was also interviewed, when the patient was unable to answer the questions or had neuropsychiatric symptoms that constituted the main reason for the referral (Fig. 1).

Individual care of the patient with complaints or difficulties in their mental health: care flowchart.
The standard number of sessions offered by psychology and psychiatry was five, but the participants could access to more than five sessions if the psychologist or the psychiatrist considered it necessary, and the participants agreed. Every participant and their relatives (parents, siblings, and children) could access to the Mental Health services.
Considering the effects that the pandemic situation could have at any time on clinical trial participants and caregivers, both medical and non-medical GNA staff received training in the application of psychological first aid for the initial care of people in crisis, in order to: a) reduce the initial stress caused by the traumatic event; b) teach coping strategies in the short, medium and long term, and c) enhance coping strategies previously learned [18–20] (Fig. 2).
Telephone psychological first aid. Adapted from “Remote Psychological First Aid during COVID-19”, with permission [20].
Diagnosis and treatment
The diagnosis of participants in this study was made through an unstructured interview by a psychologist (CM) and a psychiatrist (CR), both with experience in the diagnosis and management of the clinical changes described in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, DSM-5 [21].
Treatment was also provided in accordance with the recommendations of the health care guidelines for Colombia [22].
Both the initial psychological and psychiatric assessments, as well as the follow-up process and psychotherapy treatments, were in line with the recommendations made by Muir et al. [23], who propose a seven-phase model for the implementation of this therapeutic modality [23, 24]: 1) review of the status quo (i.e., the human and technological resources that were available when the offer of telecare by the mental health team was considered); 2) recruitment of the work team (psychology, psychiatry, principal investigator, medical director, members of the clinical trial coordination area, area in charge of the GNA quality processes, professional neuropsychology teams, systems engineers, members of the pharmacy and nursing area); 3) training and development of communication strategies (a psychological first aid training was given to all medical and non-medical staff in contact with clinical trial participants and caregivers, and staff made aware of the mental health care flowchart for these patients); 4) plans for implementing the strategy and for evaluating both the process and the outcomes; 5) implementation preparation (Google Meets was selected as an interim platform for clinical care, while the systems area continued to develop its own platform for patient care in the future); 6) implementation of a pilot test (after attempting the assessment and follow-up processes through video call alone, it was necessary to offer these services by conventional telephone call to people who did not have a data plan or access to a stable Internet connection); and 7) implementation of the program with the adjustments made after the completion of the first assessments. During the sessions, the clinicians paid special attention to their tone of voice, speech patterns and, where video call was used, body language, in order to show interest and empathy, key elements in the psychotherapeutic process [25].
In addition to the pharmacological recommendations, treatment strategies were recommended including the following: a) interpersonal therapy, a useful method in situations of grief or transition, where there are conflicts regarding roles, and where interpersonal relationships are lacking [26]; b) attachment-based family therapy carried out either individually or with a family group, which is an experiential treatment focused on the way in which emotions affect relationships, histories and the severity of stress experienced by the patient [9], and c) psychoeducation of participants and caregivers, emphasizing the need to build a support network, stay well informed, ensure an adequate supply of food and medical supplies, avoid social isolation and take regular physical and cognitiveexercise [27].
To ensure multidisciplinary treatment of participants with serious mental health difficulties, the diagnosis of these patients was discussed by professionals in psychology, psychiatry, and social work according to the International Classification of Diseases, 10th Revision, ICD-10, with a view to identifying the best therapeutic approach at the individual, family, and community levels. To estimate the frequency of the disorders, different diagnostic codes were grouped by generic clinical syndromes (Table 1).
Clinical syndromes and ICD-10 related codes used to diagnose the participants evaluated in the mental health program of the API ADAD Colombia clinical trial
To identify clinical improvement, the evaluators analyzed if the patients felt that the treatment had been useful or not to reduce severity or frequency of the symptoms they had before the intervention onset.
Ethical considerations
Participants or their caregivers if they lacked consent capacity, consented to receiving care from the mental health team, whose services were part of the Social Plan designed to contribute to the well-being of clinical trial participants and their families, and which had the approval of the local Institutional Review Board, IRB [15]. All the participants with dementia and able to give their assent, accepted to be evaluated by the mental health team.
Statistical analysis
The sociodemographic aspects of the population, as well as the characteristics of the mental health problems of the participants, were described through frequencies and percentages of qualitative variables, as well as measures of central tendency (mean, median) and dispersion (standard deviation, interquartile range) in the case of quantitative variables. To evaluate the association of the different evaluated variables with the possibility of using either of the two services, namely psychology or psychiatry, or with the use of each of these services separately, an exploration of potential predictors was conducted through unadjusted bivariate associations (these calculations can be reviewed in the Supplementary Material, which is also attached as recommended by the Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis, TRIPOD guidelines [28]).
Since this study was not planned for developing a predictive model of services utilization, in order to explore which predictors were important, relevant predictors were selected from the perspective of statistical significance (not recommended) using the p-value adjusted for false positive rate. This was done because the number of events and sample size limited the model to a higher number ofpredictors.
Then, using the Lasso regularization method, predictors from the candidate set selected based on statistical and clinical criteria were chosen for the final model, taking into account prior analysis of the issue of multicollinearity. The carrier status of the PSEN1 E280A variant was also considered. All analyses were performed with the statistical software R version 4.3.0 [29] and RStudio [30].
RESULTS
Among the 252 participants in the clinical trial, 60 received treatment from psychology, 38 received treatment from psychology, 38 received treatment from psychiatry, and 66 individuals received treatment from either psychology or psychiatry as part of the Mental Health Team between March 1, 2020, and December 31, 2020 (Table 2). Although some non-users experienced worsened mental health following the onset of the COVID-19 pandemic, they did not receive any referral to the Mental Health Team. All participants referred to the Mental Health Team agreed to be evaluated by psychiatry or psychology. The majority of those who received treatment were women (psychology service users, 83% ; psychiatry services users, 76% ; and either psychology or psychiatry service users 80.3% ). The average age of both service users and non-users was similar, around 44 years old. Many of the participants, whether users or non-users, were married or living with a partner. Almost one-third of the 66 API participants (28.8% ) had not previously been assessed by the Mental Health Team before the pandemic. There was no difference in the carrier status of the PSEN1 E280A variant between the Mental Health Team users and non-users in this study.
Demographic characteristics, medical comorbidities, and psychological status of participants in the mental health program of the API ADAD Colombia clinical trial compared to those who did not use these services
*Depression includes ICD-10 diagnoses as moderate depressive episode; other depressive episodes; depressive episode, unspecified; recurrent depressive disorder, current episode mild; recurrent depressive disorder, current episode moderate; recurrent depressive disorder, unspecified, dysthymia, mixed anxiety, and depressive disorder. **Anxiety includes ICD-10 diagnoses as specific phobias, panic disorder, generalized anxiety disorder; mixed anxiety and depressive disorder; other mixed anxiety disorders; other specified anxiety disorders; anxiety disorder, unspecified; acute stress reaction; other stressful life events affecting family and household; stress, not elsewhere classified. †Subjective memory complaints mean score is calculated by adding the participant score to the informant score and dividing it by two. ‡A score of 20 or more is considered clinically significant.
Before and after the onset of the pandemic, the most common psychological problems were anxiety (before 36.4% , after 63.6% ) and depression (before 34.8% , after 37.9% ). Only two participants (3% ) reported that they had had COVID-19. Of the individuals assisted by the mental health team, 70% of those seen by psychology and 81.6% of those seen by psychiatry felt that the services were helpful for them. The percentage of conditions among those who received psychological or psychiatric assistance and who felt that the services were useful for their conditions were 71.4% and 86.9% respectively (patients with depression); 70.3% and 75% (anxiety); and 60% and 76.2% (adjustment or sleep disorders, relationship or lifestyle problems, borderline personality disorder) (Fig. 3).

Percentage of participants with depression, anxiety, and other disorders, who considered psychological or psychiatric care to be useful.
Regarding the multivariable prediction model, a selection of predictors was made for the final model using the Lasso regularization method for three situations: use of psychology service (Table 3A, B), use of psychiatry service (Table 3C, D), and use of at least one of the two services, psychology, or psychiatry (Table 3E, F).
Predictive multivariable model for using the Mental Health Team services by participants of the API Colombia trial A) Psychology service use (variable PSEN1 E280A variant carrier status has been included)
B) Psychology service use (variable PSEN1 E280A variant carrier status has not been included)
Area under the curve: 0.7866.
C) Psychiatry service use (variable PSEN1 E280A variant carrier status has been included)
D) Psychiatry service use (variable PSEN1 E280A variant carrier status has not been included)
Area under the curve: 0.8397.
E) Either psychology or psychiatry service use (variable PSEN1 E280A variant carrier status has been included)
F) Either psychology or psychiatry service use (variable PSEN1 E280A variant carrier status has not been included)
Area under the curve: 0.803.
In the model for the outcome “use of psychology service” without considering the carrier status of the PSEN1 E280A variant, the variables that obtained statistical significance and therefore could have a significant impact on this outcome were female sex (OR 3.19, 95% CI 1.42–7.89, p = 0.007), history of hyperlipidemia (OR 0.12, 95% CI 0.03–0.33, p < 0.001), history of hyperlipidemia (OR 0.12, 95% CI 0.03–0.33, p < 0.001), history of depression before the pandemic (OR 2.82, 95% CI 1.23–6.51, p = 0.014), and history of anxiety before the pandemic (OR 2.61, 95% CI 1.18–5.79, p = 0.017).
In the model for the outcome “use of psychiatry service” without considering the carrier status, the variables that obtained statistical significance and could have a significant impact on this outcome were history of hyperlipidemia (OR 0.31, 95% CI 0.09-0.87, p = 0.039), history of dementia before the pandemic (OR 6.47, 95% CI 1.74-24.00, p = 0.005), history of depression before the pandemic (OR 7.07, 95% CI 2.91-17.71, p < 0.001), and history of anxiety before the pandemic (OR 3.19, 95% CI 1.30-7.68, p = 0.010).
In the model for the outcome “use of psychology or psychiatry services” without considering the carrier status, the variables that obtained statistical significance and could have a significant impact on this outcome were female sex (OR 2.44, 95% CI 1.13-5.64, p = 0.029), history of hyperlipidemia (OR 0.17, 95% CI 0.06-0.43, p = 0.001), history of depression before the pandemic (OR 3.31, 95% CI 1.46-7.62, p = 0.004), and history of anxiety before the pandemic (OR 3.32, 95% CI 1.50-7.41, p = 0.003).
The carrier status of the PSEN1 E280A variant did not behave as a relevant variable for predicting the use of the different mental health services described here. That is why two models are presented for each outcome: one with the “carrier” variable and another without this type of variable.
DISCUSSION
Some mental health problems, such as anxiety, began or were exacerbated during the COVID-19 pandemic among participants in a clinical trial aimed at preventing or delaying the onset of symptomatic AD. However, it was possible to mitigate the psychological effects of the COVID-19 pandemic through a comprehensive mental health program, which included the provision of care by psychology and psychiatry services from within the same research group that patients attend.
In 2020, Vindegaard and Benros [8] published the results of a systematic review to describe the psychiatric complications related to COVID-19 infection, and the mental health impact on psychiatric patients and the general population, associated with the pandemic. This work included 43 post-pandemic studies, two of which corresponded to research conducted with people who had a history of mental illness, and another 19 focused on the general population. They found that aggravation of symptoms occurred in 20.9% of participants with chronic psychiatric disorders after the onset of the pandemic. In comparison, in our study, 53% of participants who received mental health services between March 1, 2020, and December 31, 2020, perceived an exacerbation of their baseline clinical condition. In the systematic review of the above-mentioned study, it was reported that living alone was a risk factor for the development or worsening of psychiatric symptoms, and in our study approximately 60% of participants were married or lived with a partner. In our study, 80.3% of participants who received mental health services during the above-mentioned period were women, and the average number of children was 2.03 (SD 1.29); in the above-mentioned systematic review, having two or more children was identified as a risk factor. In our research, sex and civil status were not related to lack of improvement feeling after the psychological or psychiatric intervention. Nevertheless, a mental health worsening after the pandemic onset was positively associated to the improvement feeling with the psychological treatment, and sleep disorders after pandemic onset was negatively associated to it. This report highlights the importance of studying the effects of the pandemic on mental health, in order to identify and promote preventative measures during subsequent pandemics [8].
Unlike depression, the prevalence of which was similar before and after the onset of the pandemic (before 34.8% ; after 37.9% ), the prevalence of anxiety disorders increased by 1.7-fold after the COVID-19 pandemic began. It is possible that the onset or worsening of symptoms was contributed to by the participants’ perception of their own and their loved ones’ risk of COVID-19 infection [31], history of other mood disorders; social distancing measures and lockdowns; social isolation; economic problems; and feelings of uncertainty or hopelessness [32, 33]. Measurement and relationship between the presence of anxiety and other psychiatric symptoms with these possible explanatory factors were not calculated for this study.
With the aim of preventing and controlling significant mental health deterioration in the participants of the API ADAD Colombia clinical trial, a telecare intervention strategy was quickly organized. In order to provide a service appropriate to the needs and expectations of each individual, both psychology and psychiatry teams participated in this as well as social workers and nursing staff. This is in accordance with the recommendation of Jayarajan et al. [34] in their article on basic guidelines for the use of telemedicine in psychiatric telerehabilitation.
More than 70% of participants who received psychological or psychiatric care through telecare felt that these services were useful for the management of two common mental health disorders: anxiety and depression. This result is compatible with previous evidence on the efficacy of clinical intervention using telemedicine that shows comparability with face-to-face care in terms of cost-effectiveness, comfort, usefulness in isolated communities or with participants who do not have access to the internet, and reduction of symptoms, hospitalizations, and unnecessary trips to the public health emergency services [13, 35]. Regarding this mental health program for participants in the API ADAD Colombia trial, other benefits in virtual mental health care are presumed, for example, prevention of exacerbation of cognitive disorders in symptomatic individuals, minimization of psychopathology secondary to stressful or potentially traumatic events and reduction of the impact of the pandemic on participation in the clinical trial.
According to a recent article published by Tambling et al. [36], having high levels of anxiety is associated with a higher likelihood of seeking some form of help to improve mental health, with individuals with higher levels of depression specifically seeking psychological care. A similar finding was also observed in the different predictive models for the use of psychological or psychiatric services described here, where a history of anxiety or depression acted as important risk factors for this outcome. This association was also highlighted by Tambling et al. in their research on factors related to seeking mental health care [36].
Regarding the use of psychiatric services, another risk factor related to this outcome, and not associated with the use of psychological services or the use of either service (psychology or psychiatry), was a history of dementia before the pandemic. This may be related to the increased psychological and behavioral symptoms experienced by these patients during the pandemic, as indicated by Wei et al. in their article on the effects of COVID-19 on neuropsychiatric symptoms in individuals with major neurocognitive disorder [37].
An interesting finding that was consistent across all six models was the negative association, with an odds ratio (OR) less than 1 and statistically significant, between a history of dyslipidemia and the use of psychology or psychiatry services. This could be explained by the relationship described between low cholesterol levels and the presence of mood disorders, as reported by some authors [38]. However, other researchers have described non relationship [39], or an opposite relationship, suggesting that low cholesterol levels are associated with a lower risk of depression [40], or that a triglyceride/HDL ratio greater than 1 increases the likelihood of emotional problems such as depression, specifically in men [41]. Our study did not differentiate between hypercholesterolemia and hypertriglyceridemia, nor between previous or current presence of dyslipidemia. Therefore, it is necessary to consider these subcategories and monitor the affective and behavioral symptoms of individuals with and without these metabolic conditions in the future.
The lack of a validated instrument to measure the response of patients to the interventions carried out by the mental health team should be recognized as a limitation; only the perception of usefulness of the care received from the psychology or psychiatry services was considered. In the future, we hope to be able to use tools such as that proposed by Coleman et al. [42], which evaluates the impact of the COVID-19 pandemic on access to health services, social support, finances, the ability to meet basic needs and the physical or emotional health of participants in pragmatic clinical trials. Moreover, our study did not measure satisfaction with the services provided by the mental health team through telecare, or consider the barriers that interfered with the use of virtual care, such as difficulties in communication, an intermittent or non-existing internet connection, living in rural areas with an unstable telephone signal, or lack of a private space where participants could talk freely about thoughts and emotions [24, 43]. Finally, this was a study not designed to establish a predictive model of using the Mental Health Team services, therefore the related results must be interpreted withcaution.
In conclusion, the following statement by Alonso-Lana et al. [4] relates to people with some degree of cognitive impairment but is considered relevant even for asymptomatic participants of clinical trials aimed at changing the natural course of Alzheimer’s disease: “.... it is essential and urgent to minimize the potential negative effects of the pandemic on the cognitive and psychological functioning and quality of life of survivors”. The results of this study suggest that the involvement of a mental health team in the care of individuals and their families helps us in our quest to optimize and maintain the well-being of patients.
Footnotes
ACKNOWLEDGMENTS
We thank the families with the genetic variant PSEN1 E280A for allowing us to learn about Alzheimer’s disease with them, through them and for them.
FUNDING
This work is supported by the NIA (RF1AG041705-01A1, R01AG055444, P30AG19610, P30AG072980); Roche/Genentech, Banner Alzheimer’s Foundation; Anonymous international foundation; Flinn Foundation; No Me Olvides initiative; Nomis Foundation, Colciencias 1115-65741185408-20512, 1115-54531651, CODI 2017 408-20543; and the State of Arizona (Arizona Alzheimer’s Consortium).
CONFLICT OF INTEREST
Claudia Ramos is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review. Silvia Rios-Romenets was supported by Genentech/Roche. Francisco Lopera has grants supported by Roche, Banner, NIH, Enroll-HD, Large PD and DIAN. The rest of the authors from GNA have no financial interest of affiliations relevant to the subject to this manuscript. Jessica B. Langbaum reports grants from NIA (RF1AG041705, P30AG072980, R01AG05544, 1R33AG070604, 1R01AG069453, 1R01AG063954, 1R01AG058468) and received consulting fees from Alector, Biogen, Denovo Biopharma, and Provoc. Pierre Tariot reports receiving research support and consultant fees from Abbvie, AC Immune, Acadia, Athira, Biogen, BioXcel, Cortexyme, Eisai, Genentech, Merck, Novo Nordisk, Otsuka & Astex, Syneos and T3D Therapeutics. Kaycee M. Sink and Eric Reiman do not have any direct conflicts/disclosures to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.