
Abstract
Background:
Previous in vitro and in vivo studies on Alzheimer’s disease (AD) models have reported that rosmarinic acid (RA) can inhibit the formation of amyloid-β fibrils as well as the oligomerization and deposition of amyloid-β protein. Melissa officinalis (M. officinalis) extract containing 500 mg of RA is tolerable and safe in healthy individuals and patients with mild AD dementia.
Objective:
This randomized placebo-controlled double-blind trial aimed to assess the effects of M. officinalis extract on cognition in older adults without dementia.
Methods:
This study included individuals who were diagnosed with subjective or mild cognitive impairment (n = 323). The trial involved M. officinalis extract supplementation (500 mg of RA per day) period of 96 weeks followed by a washout period of 24 weeks. The primary endpoint was the Alzheimer’s Disease Assessment Scale-cognitive subscale score, and the secondary endpoints were other cognitive measure results as well as safety and tolerability.
Results:
There were no significant differences in cognitive measures between the placebo and M. officinalis groups from baseline to 96 weeks. However, based on the analysis of Clinical Dementia Rating Sum of Boxes scores in participants without hypertension, the score was found to be increased by 0.006 and decreased by 0.085 in the M. officinalis and placebo groups, respectively; this difference was statistically significant (p = 0.036). Furthermore, there were no differences in vital signs, physical and neurological measures, or hippocampal volume between the two groups.
Conclusion:
These results indicate that M. officinalis extract may help prevent cognitive decline in older adults without hypertension.
INTRODUCTION
The number of patients with dementia is increasing worldwide and, of these, more than 50% patients have Alzheimer’s disease (AD). Two characteristic features of AD include amyloid-β protein (Aβ) deposition in the parenchyma and neurofibrillary tangle formation by microtubule-associated protein tau [1–3]. During the progression of AD, Aβ aggregation is followed by neurofibrillary tangle formation and neuronal degeneration, which further leads to brain atrophy [1]. Treatments targeted at Aβ aggregation, including neurotoxic Aβ oligomer formation, should thus be performed early in the disease process [4, 5]. Currently, there are no established disease-modifying therapies for AD, although Aducanumab and Lecanemab are getting attention as promising therapeutic agents for AD [6, 7]. However, dietary modifications and/or nutraceutical supplementation may help prevent or treat AD. Notably, rosmarinic acid (RA) has antioxidant, anti-inflammatory, antimutagenic, antibacterial, and antiviral properties [8]. In our previous study, we found that RA inhibits the formation of Aβ fibrils and destabilizes preformed Aβ fibrils in vitro [9]. It also inhibits the Aβ oligomerization, thereby reducing Aβ oligomer-induced synaptic toxicities [10]. Moreover, it has been reported that RA inhibits both oligomerization and Aβ deposition in AD transgenic mice (Tg2576) [11].
Previously, we prepared Melissa officinalis (M. officinalis) extract that richly contained RA and revealed that a single dose of M. officinalis extract containing 500 mg of RA is safe and tolerable for healthy people [12]. Notably, a randomized double-blind placebo-controlled 24-week study with an open-label extension to 48 weeks involving patients with mild AD dementia reported that M. officinalis extract containing 500 mg of RA is safe, well-tolerated, and helps prevent worsening of AD-related neuropsychiatric symptoms [13].
To further explore the beneficial effects of M. officinalis extract on cognition, we conducted a randomized double-blind placebo-controlled trial involving older adults without dementia. The primary endpoint was M. officinalis extract’s effect on cognitive measures, and the secondary endpoints were the efficacy, safety, and tolerability of the extract. Additionally, hypertension, dyslipidemia, and diabetes mellitus are all well-known risk factors for dementia [14]. Therefore, we performed the sub-analysis stratified by these diseases because of the possibility that the anti-dementia effect of M. officinalis extract may differ depending on the presence or absence of these diseases.
MATERIALS AND METHODS
Participants and study design
Older adults (65–79 years old) without dementia were recruited in this study through local advertisements in Kanazawa City and Nanao City, Ishikawa Prefecture, Japan. All participants provided written informed consent for participation in this study. The study was approved by the Ethics Committee of the Kanazawa University Medical Ethics Review Board (approval number: 2018-014 (8013)) and was conducted in accordance with to the Declaration of Helsinki. The study trial was registered, and the protocol was uploaded to the Japan Registry of Clinical Trials and UMIN-CTR with the identifiers jRCTs041180064 and UMIN000021596, respectively.
The inclusion criteria were as follows: patients with an age of 65–79 years at the time of providing informed consent; those with a diagnosis of subjective or mild cognitive impairment: a Mini-Mental State Examination (MMSE) score of >24 at screening; those willing to provide a blood or urine sample for laboratory testing and apolipoprotein E (APOE) genotyping; and those with a stable lifestyle, e.g., those with stable exercise and eating habits. Patients with any other mental illness, such as schizophrenia, bipolar disorder, and depression; a Geriatric Depression Scale 15 score of >6 at screening; uncontrolled health problems within 3 months of screening, such as heart failure, angina pectoris, renal dysfunction, etc.; malignancy within 5 years; and allergies to polyphenols, drugs, or foods were excluded from the study. We also excluded subjects who have untreated hypertension, dyslipidemia, and diabetes mellitus and subjects if whose physician in charge did not approve subject to join our clinical trial because of unstable condition of the disease.
Diagnosis of subjective and mild cognitive impairment
Subjective cognitive impairment was defined as follows: (i) a Clinical Dementia Rating (CDR) score of 0; (ii) a response of “Yes” to the question “Do you have forgetfulness?”; and (iii) failure to meet the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), criteria for major neurocognitive disorder. Mild cognitive impairment was defined as follows: (i) a CDR score of 0.5 and (ii) failure to meet the DSM-V criteria for major neurocognitive disorder [15].
Intervention
This study comprised two phases: phase 1, a randomized, double-blind, placebo-controlled, parallel-group 96-week trial; phase 2, a washout period of 24 weeks. Figure 1 illustrates the trial’s time course. Placebo and M. officinalis extract capsules (M. officinalis extract containing RA) were provided by Maruzen Pharmaceuticals Co., Ltd., Japan. Lemon balm leaves (M. officinalis) were extracted with hot water and were purified with ethanol to obtain rosmarinic acid-rich extract. Each M. officinalis extract capsule contained 185 mg M. officinalis extract along with 50 mg RA, 60 mg lactose, and 5 mg calcium sterate. Each placebo capsule contained 210 mg lactose, 35 mg caramel, and 5 mg calcium stearate. There was no detectable RA content in the placebo capsule. Placebo capsules were made of the same size and color as the M. officinalis extract capsules [12]. All participants discontinued taking M. officinalis extract or placebo capsules during phase 2. Notably, participants were assessed at screening, baseline, and 24-, 48-, 72-, 96-, and 120-week follow-ups. The assessment items at each visit are shown in Supplementary Table 1. A 1:1 ratio was used to dynamically assign participants to the intervention (M. officinalis extract) or placebo group according to age, gender, length of education, APOE E4 carrier or noncarrier status, CDR score, and MMSE score at screening.
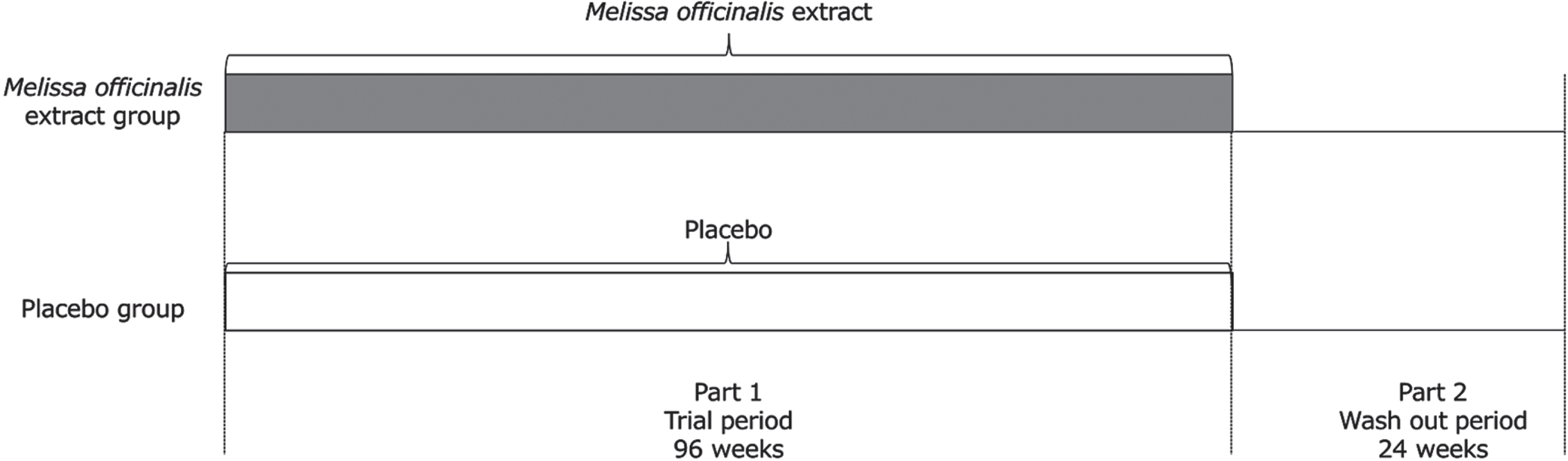
Trial time course. Part 1 of the trial was designed as a randomized double-blind placebo-controlled parallel-group 96-week trial. Individuals were randomly allocated in a 1:1 ratio to either the Melissa officinalis group (receiving M. officinalis extract containing 500 mg of rosmarinic acid [RA] daily) or the placebo group. Part 2 (24 weeks) of the trial was a wash out period for all individuals.
Primary outcome
The primary outcome was change in cognitive performance from baseline to 48- or 96-week follow-up examinations. Cognition was assessed using the Alzheimer’s Disease Assessment Scale-cognitive subscale (ADAS-cog score). Scores on the scale ranged from 0 to 70, and higher scores indicated greater cognitive decline.
Secondary outcomes
Changes in clinical assessments, hippocampal volume (HV) measured by head magnetic resonance imaging (MRI), and the safety and tolerability of M. officinalis extract were secondary outcomes. Various cognitive and neuropsychiatric measures were performed at baseline and at 48-, 96-, and 120-week follow-ups. These measures were: the MMSE and Clinical Dementia Rating Sum of Boxes (CDR-SB), which involve the assessment of six domains of functioning, including memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care. Safety was assessed using vital sign and adverse event (AE) evaluations, urine analysis, and routine laboratory tests. Participants were instructed to store unused M. officinalis extract or placebo capsules and to return them to the investigating physician at each follow-up visit. The number of these capsules was counted to assess adherence.
Isoelectric electrophoresis was used to determine the genotype of APOE, as reported by Kamboh et al. [16]. Changes in HV-to-estimated total intracranial volume (eTIV) from baseline to 96-week follow-up examination were assessed according to volumetric MRI.
Sample size determination
The number of participants needed for this study was determined using an a priori power calculation performed G*Power software (version 3.1.9.2). With an effect-size (d) of 0.10, a significance level of α= 0.05, and a power of 0.8, the power analysis revealed a sample size of 264 participants. Nevertheless, we aimed to recruit 330 participants, assuming a dropout rate of 25%.
Attrition
Overall, 376 older adults were assessed in this study; of these, 42 did not meet the inclusion criteria (22 had a Geriatric Depression Scale 15 score of >5, 4 had a MMSE score of <24, 10 had health problems, 3 had medication contraindications for coadministration, and 3 had drug and/or food allergies), and 11 patients were not interested in participating (Fig. 2).
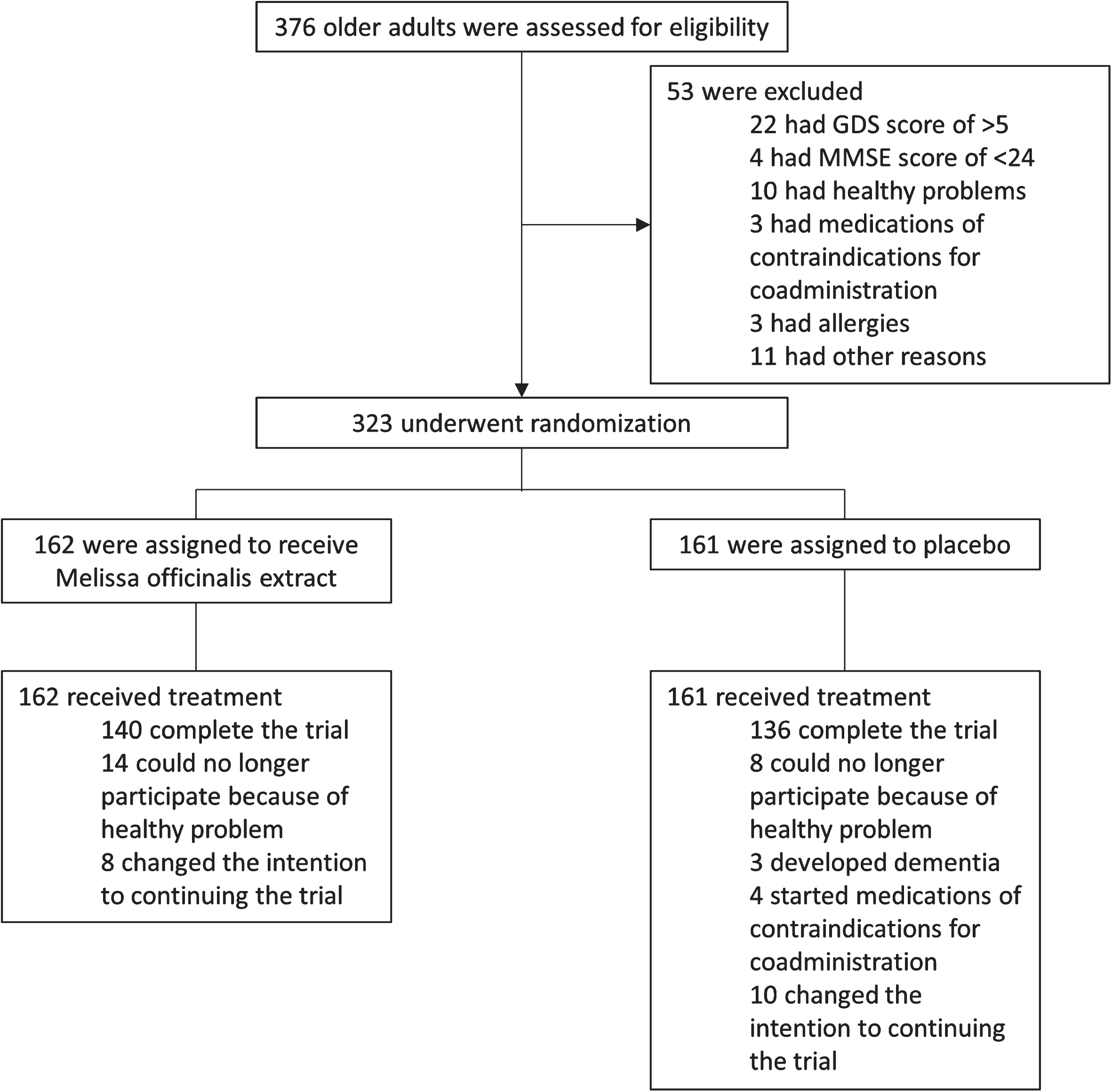
Trial randomization, trial-group assignment, and follow-up. GDS, Geriatric Depression Scale 15; MMSE, Mini-Mental State Examination.
Statistical analysis
The efficacy and safety of M. officinalis extract were evaluated using available data from available subjects, i.e., full-analysis set. We used generalized linear mixed effects repeated measure analysis to evaluate the effect of treatment on changes in all measures from baseline to 48- and 96-week follow-ups and baseline to 48-, 96-, and 120-week follow-ups. Unless otherwise specified, data were presented as mean±standard deviation. A p-value <0.05 was considered statistically significant. Statistical analyses were performed using Statistical Package for the Social Sciences software (version 28; SPSS Inc., Chicago, IL, USA).
RESULTS
Study population and baseline characteristics
Overall, 323 participants were randomly allocated to the M. officinalis (n = 162) and placebo groups (n = 161). The demographic and clinical characteristics of the participants from the full-analysis set are presented in Table 1. In total, from baseline to the 120-week follow-up visit, 47 participants withdrew from the study. Of these, 22 participants, including 14 and 8 from the M. officinalis and placebo groups, respectively, withdrew because of health problems, such as malignancy or stroke, and 18 participants, including 8 and 10 from the M. officinalis and placebo groups, respectively, withdrew because of changes in their intention to continue participation in the trial (Fig. 2). In addition, three and four participants from the placebo group discontinued placebo capsule intake because they developed AD dementia and started medications with contraindications for coadministration, respectively. Finally, 276 participants (84.4% –86.4% of the participants originally assigned to each group) completed the trial up to the 120-week follow-up visit (Fig. 2).
Demographic and baseline characteristics of the study participants
ADAS-cog score, Alzheimer’s Disease Assessment Scale-cognitive subscale; APOE, apolipoprotein E; CDR-SB, Clinical Dementia Rating Sum of Boxes; eTIV, estimated total intracranial volume; HV, hippocampal volume; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination‘.
Primary outcome
There were no significant differences in changes in ADAS-cog scores between the two groups from baseline to the 48-, 96-, and 120-week follow-up visits (Table 2).
Mean and estimated mean change in cognitive assessments from baseline to the 96-week follow-up visit
ADAS-cog, Alzheimer’s Disease Assessment Scale-cognitive subscale; CDR-SB, Clinical Dementia Rating Sum of Boxes; MMSE, Mini-Mental State Examination.
Secondary outcomes
Changes in MMSE and CDR-SB scores from baseline to the 48-, 96-, and 120-week follow-up visits did not differ significantly between the two groups (Table 2).
Participants who were stratified by co-occurring diseases, such as hypertension, dyslipidemia, and diabetes mellitus, underwent additional analyses. The clinical characteristics of study participants based on hypertension status and treatment group are summarized in Supplementary Table 2. The number of males among participants with hypertension was significantly higher than that among those without hypertension (Supplementary Table 2). There were no significant differences about the demographic and clinical characteristics between the treatment and placebo groups among participants without hypertension (Supplementary Table 3). The analysis of data stratified for hypertension, dyslipidemia, and diabetes mellitus revealed a significant time×treatment interaction, time, and treatment effects on CDR-SB score from baseline to the 48-, 96-, and 120-week follow-up visits (F = 3.004, p = 0.030; F = 2.772, p = 0.041; F = 4.712, p = 0.031, respectively). Post-hoc analysis of time revealed a significant difference from baseline to the 48-week follow-up visit (p = 0.026). The analysis of CDR-SB score change in participants without hypertension from baseline to the 48- and 96-week follow-up visits revealed a significant time×treatment interaction and time effects (F = 3.403, p = 0.034; F = 3.632, p = 0.027, respectively), and the treatment effect was positively but insignificantly different between the M. officinalis and placebo groups (F = 3.76, p = 0.054; Fig. 3). The mean CDR-SB score increased by 0.006 in the M. officinalis group and decreased by 0.085 in the placebo group among participants without hypertension from baseline to the 96-week follow-up visit (Table 3). Post-hoc analyses of time revealed a significant difference from baseline to the 48-week follow-up visit (p = 0.024). Further analysis of the change in each CDR domain score from baseline to the 48-, 96-, and 120-week follow-up visits revealed no significant time×treatment interaction effects. However, the mean score of the CDR-SB memory subscale increased by 0.005 in the M. officinalis group and decreased by 0.03 points in the placebo group (p = 0.034), whereas the mean score of the judgment and problem-solving subscale decreased by 0.005 and 0.04 in the treatment and placebo groups, respectively (p = 0.047), between the baseline and the 96-week follow-up visit (Supplementary Table 4).
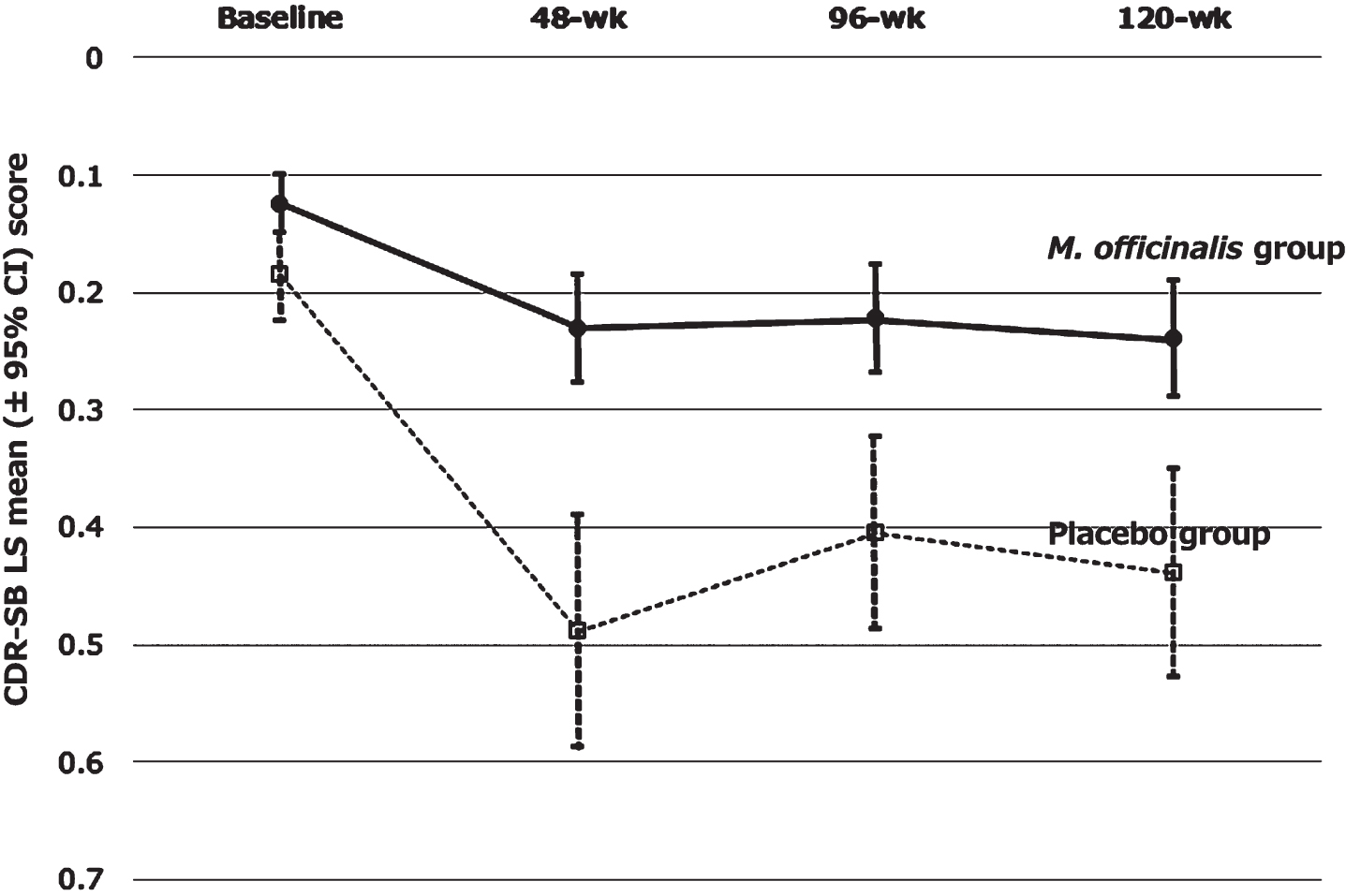
Least squares mean (±95% CI) change from baseline in CDR-SB in without hypertension group. Solid line represents the Melissa officinalis group (M. officinalis) and dotted line represent the placebo group. CDR-SB, Clinical Dementia Rating Sum of Boxes; LS, Least squares; M. officinalis, Melissa officinalis.
Mean and estimated mean change in cognitive assessments from baseline to the 96-week follow-up visit and baseline to the 120-week follow-up visit among with and without hypertension groups
ADAS-cog, Alzheimer’s Disease Assessment Scale-cognitive subscale; CDR-SB, Clinical Dementia Rating Sum of Boxes; MMSE, Mini-Mental State Examination.
Regarding disease-related biomarkers, there were no significant differences between the M. officinalis and placebo groups in terms of HV-to-eTIV. Similarly, there were no differences in vital signs or physical and neurological examination results between the two groups. AEs occurred in 46.9% and 45.3% of participants from the M. officinalis and placebo groups, respectively (p = 0.824). Table 4 shows the number of each type of AE according to the allocation group. AEs led to study discontinuation in 22 participants, including 14 and 8 in the M. officinalis and placebo groups, respectively (p = 0.269, Fig. 2). Serious AEs were reported in 62 participants (34 and 28 in the M. officinalis and placebo groups, respectively) in addition to 80 hospitalizations (45 and 35 in the M. officinalis and placebo groups, respectively), although none of these were related to M. officinalis. The two groups did not differ in the number of participants who had at least one serious AE (30 in the M. officinalis group and 27 in the placebo group, p = 0.771) and at least one hospitalization (30 in the M. officinalis group and 26 in the placebo group, p = 0.660). There were no significant differences in the serum levels of the indicators of liver function—aspartate aminotransferase, alanine aminotransferase, lactate dehydrogenase, and total bilirubin—and kidney function—blood urea nitrogen and creatinine—as well as in hematology findings between the M. officinalis and placebo groups. Finally, treatment adherence among participants the M. officinalis and placebo groups was 81.7% and 78.2%, respectively.
Number of participants reporting adverse events
DISCUSSION
In this 96-week double-blind placebo-controlled study with a 24-week washout period, we evaluated the effects of M. officinalis extract containing RA (500 mg daily dose) on cognitive ability among older adults without dementia. The results of this study revealed no significant differences between the treatment and placebo groups in terms of ADAS-cog score changes from baseline to 48- or 96-week follow-up visits.
Moreover, we assessed the safety, tolerability, and clinical effect of M. officinalis extract as secondary endpoints. Notably, we found no differences between the treatment and placebo groups in terms of HV-to-eTIV. Supplementation was tolerable for 96 weeks, and it did not cause any safety concerns that could be clinically manifested; moreover, no routine blood tests were required. There were no differences between the two groups in terms of MMSE and CDR-SB score changes from baseline to the 48- or 96-week follow-up visits. In contrast, a significant time×treatment group interaction effect was observed for the CDR-SB score in participants without hypertension. Post-hoc tests revealed that the memory and judgment and problem-solving subscale scores were significantly different between the treatment and placebo groups, suggesting that the benefits of treatment are limited to memory, judgment, and problem-solving functions. Finally, although limited, our study provides statistically significant evidence regarding the clinical efficacy of M. officinalis extract for participants without hypertension.
A recent study found that supplementation of spearmint extract containing 130 mg RA for 90 days improved work-related memory among healthy older adults [17]; this finding partially conforms to our findings. Moreover, spearmint extract supplementation has been shown to improve cognitive performance in young population [18]. Notably, plants of Lamiaceae family, such as spearmint, rosemary, sage, and lemon balm, have been reported to be beneficial for memory after acute dose regimen [19]. To the best of our knowledge, the present study is the first to provide evidence on the benefit of M. officinalis extract for long-term cognition in older adults.
Previously, we studied the pharmacokinetics of M. officinalis extract containing RA, and we found that food intake affects the maximum serum concentration, increases the area under the curve, and delays the time of maximum serum concentration [12]. As food intake was expected to affect RA absorption and increase RA exposure, participants in our previous study were asked to take placebo or M. officinalis extract after meals [12]. Moreover, we evaluated the influence of M. officinalis extract on clinical assessment scores and biomarkers in a 24-week double-blind placebo-controlled study involving patients with AD; we found that this extract was beneficial for the management of irritability or lability, implying its therapeutic effects on the brain [13]. However, we could not provide biological evidence regarding the efficacy against AD pathophysiology through changes in amyloid or tau markers in our previous trial. Moreover, RA was undetectable (<0.28×10–2 nmol/L) in the cerebrospinal fluid of the M. officinalis group after the intervention, indicating poor permeation through the blood–brain barrier, although RA and its metabolites were detectable in serum [13]. A recent study on rats reported that intact RA is present in the plasma and brain at the mean concentrations of 1440 and 24.1μM, respectively (plasma:brain = 60:1) [20]; however, to the best of our knowledge, no studies have reported RA in the central nervous system of humans. Regarding the demonstration of the effects of M. officinalis extract on the prevention of brain atrophy and cognitive decline in patients with AD, a 96-week trial may be extremely short because Aβ aggregate deposition in the AD brain occurs before ∼25 years of the appearance of clinical symptoms [4, 5]. Thus, the protective ability of phenolic compounds against dementia can be further evidenced by long-term studies using small molecule compounds exhibiting suitable blood–brain barrier permeation.
In the present study, we found no evidence regarding the clinical efficacy of M. officinalis for participants with hypertension. Notably, hypertension significantly increases the risk of vascular cognitive impairment and AD [21]. Moreover, it induces microvascular rarefaction and cerebromicrovascular endothelial dysfunction as well as impairs cerebral blood supply and the blood–brain barrier; thus, it finally promotes neuroinflammation and amyloid pathology exacerbation [21]. Therefore, M. officinalis extract may not be sufficiently effective in preventing cognitive decline among patients with hypertension and atherosclerosis.
The 0.091-point change between the treatment and placebo groups in CDR-SB scores from baseline to the 96-week follow-up visits in participants without hypertension may be little clinical significance, it is statistically significant although. The small difference in CDR-SB might be due to good cognitive function of participants in this study. We have conducted 3 cognitive batteries: ADAS-cog, MMSE, and CDR-SB. Among those, we found significant differences between treatment and placebo groups only in terms of CDR-SB score changes in participants without hypertension. CDR-SB is assessed by a structured, clinician-rated interview and can estimate comprehensive cognition [22]. On the other hand, ADAS-cog and MMSE are assessed by asking questions to subject and can evaluate cognitive function. We speculate that CDR-SB may be superior to ADAS-cog or MMSE for detecting minimal cognitive impairment.
This study has several limitations. First, amyloid, tau, nor inflammatory biomarkers other than those observed using head MRI were not assessed. Second, potential confounding factors, such as diet and lifestyle, cannot be ruled out, although participants were asked to maintain their usual diet and exercise routine to minimize these factors. A larger study with additional biomarkers is needed to confirm the benefits of M. officinalis containing RA. Nevertheless, the randomized, double-blind, placebo-controlled design of the present study is its strength.
In conclusion, the results of this trial involving older adults without dementia revealed that M. officinalis extract containing RA (500 mg/day) may help prevent cognitive decline among patients without hypertension, however, the primary outcome of this study revealed no significant differences between the treatment and placebo groups in terms of ADAS-cog score changes from baseline to 48- or 96-week follow-up visits.
Footnotes
ACKNOWLEDGMENTS
The authors thank the participants. The authors also thank Dr. Kiyonobu Komai, Dr. Hiroyuki Fujii, Dr. Mitsuhiro Yoshimura, Ms. Yukari Yagi, Ms. Hiroko Notohara, Ms. Chiemi Abe and Ms. Miyuki Nakamura for their excellent support; Maruzen Pharmaceuticals Co., Ltd. for supplying placebo and RA capsules; and Enago (![]() ) for the English language review.
) for the English language review.
This trial was partially supported by the Japan Agency for Medical Research and Development (dk0207025 and 22dk0207053h0001). The sponsor had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.