
Abstract
Background:
Both late-life depression (LLD) and short sleep duration increase the risk of cognitive impairment. Increased insular resting-state functional connectivity (FC) has been reported in individuals with short sleep duration and dementia.
Objective:
This study aimed to investigate whether short sleep duration is associated with impaired cognition and higher insular FC in patients with LLD.
Methods:
This case– control study recruited 186 patients with LLD and 83 normal controls (NC), and comprehensive psychometric assessments, sleep duration reports and resting-state functional MRI scans (81 LLD patients and 54 NC) were conducted.
Results:
Patients with LLD and short sleep duration (LLD-SS patients) exhibited more severe depressive symptoms and worse cognitive function than those with normal sleep duration (LLD-NS patients) and NC. LLD-SS patients exhibited higher FC between the bilateral insula and inferior frontal gyrus (IFG) pars triangularis than LLD-NS patients and NC, while LLD-NS patients exhibited lower FC than NC. Increased insular FC was correlated with short sleep duration, severe depressive symptoms, and slower information processing speeds. Furthermore, an additive effect was found between sleep duration and LLD on global cognition and insular FC.
Conclusion:
LLD-SS patients exhibited impaired cognition and increased insular FC. Abnormal FC in LLD-SS patients may be a therapeutic target for neuromodulation to improve sleep and cognitive performance and thus decrease the risk of dementia.
Keywords
INTRODUCTION
Late-life depression (LLD) is defined as major depressive disorder in the geriatric population and affects 1.8% to 7.2% of geriatric adults [1, 2]. LLD is associated with impaired cognition [3] and a high risk of dementia [4]. Specifically, longitudinal studies have shown that the incidence of Alzheimer’s disease (AD) is increased in patients with LLD [5–7]. LLD and AD share some pathophysiological mechanisms, including atrophy of both frontocortical and limbic networks [8–11], glutamatergic excitotoxicity [12, 13], dysregulation of the HPA axis [14, 15], decreased levels of brain-derived neurotrophic factor [16, 17], and neuroinflammation [18]. Therefore, early identification (and intervention) regarding risk factors for dementia in LLD patients may prevent the development of dementia.
Nocturnal sleep is vital across the lifespan, and a sleep duration (SD) of 7 to 8 hours is recommended for older adults [19]. Poor sleep increases the risk of depression [20], cognitive decline [21, 22], and AD [23, 24]. Self-reported short SD (≤6 h/night) is significantly associated with worse cognitive performance [25, 26] and a higher burden of amyloid-β (a biomarker of AD) [27]. Additionally, short SD may precede cognitive decline in AD [28]. At any age, inadequate SD is one of the most common symptoms of depression [29]. Self-reported sleep disturbances were observed in 59.9% of LLD patients and associated with depressive symptoms [30]. Furthermore, previous studies have indicated that sleep disturbances, including insomnia, were associated with poor outcomes, poor response to depression treatment [31, 32], and a high recurrence risk [33]. However, whether short SD, as a modifiable risk factor, is associated with impaired cognition remains unclear in the context of LLD.
Although the pathophysiology of short SD remains unclear, accumulating evidence indicates that the insula and salience network (SN) may play a key role [34, 35]. The insula, a core hub of the salience network, evaluates whether a stimulus is emotionally or motivationally salient and links external information with internal motivation [36]. In structural MRI studies, insufficient sleep was associated with changes in gray matter volume and fractional anisotropy of the insula [37, 38] and decreased structural connectivity in a network with the insula as a key node [39]. In a resting-state functional MRI study, increased FC of the insula was observed in individuals with insomnia [35] and in patients suffering from depression with insomnia complaints [40]; this increase in FC was associated with cognitive deficits [41]. According to a systematic review and meta-analysis, AD is associated with hyperconnectivity of the SN, especially in the anterior insula [42]. Increased FC of the insular cortex and SN has been reported in cognitively normal individuals with elevated amyloid levels [43], in carriers of APOE ɛ4 (a risk gene of AD) [44] and in patients with mild cognitive impairment (MCI) [45]. Abnormal insular FC is associated with impaired cognition in MCI [45] and AD [46]. Regarding LLD, reduced insular cortical thickness and gray matter volume were correlated with more severe apathy and anxiety symptoms [47, 48], respectively. Moreover, lower FC between the insula component of the SN and the left executive control network in patients with LLD was reported compared with healthy controls [49]. However, the insular FC of LLD patients with short SD and the relationships among abnormal insular FC, short SD, and impaired cognitive function in LLD patients remain unclear.
Both LLD and self-reported short SD are modifiable risk factors for developing dementia. Increased insular FC has been reported in individuals with short SD and is associated with cognitive decline along the AD continuum. Therefore, it is necessary to clarify whether LLD patients with self-reported short SD exhibit impaired cognition and higher insular FC than those with adequate SD. The present study compared the cognitive performance and insular FC patterns between LLD patients with short or adequate SD and explored the relationships among insular FC, short SD, and cognitive function. The present study may provide new insights into the pathophysiological substrate by which short SD increases the risk of dementia in patients with LLD.
METHODS
Participants
A total of 186 patients with LLD were recruited from the Affiliated Brain Hospital of Guangzhou Medical University and 83 normal controls (NC) matched according to age and sex distributions were recruited from the community between June 2016 and October 2020. Informed consent was obtained from all participants before participation in the study. The study was approved by the Ethics Committee of the Affiliated Brain Hospital of Guangzhou Medical University (2015, 013). The inclusion criteria for patients with LLD were as follows: 1) age≥55 years, 2) at least one episode of depression after 55 years, and 3) a diagnosis of major depressive disorder according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV). The inclusion criteria for NC were as follows: 1) no history of psychiatric disorders and 2) normal cognition.
The diagnoses and assessments of all participants were confirmed by at least two trained psychiatrists. Participants were excluded if they met the following criteria: 1) history of other major psychiatric illnesses, such as bipolar disorder or schizophrenia; 2) physical diseases that can cause emotional abnormalities, such as anemia or hypothyroidism; and 3) neurological diseases, such as Parkinson’s disease or stroke. All participants who underwent MRI were right-handed and had no contraindication that precluded MRI scans. The question “During the past month, how many hours of sleep did you get each night?” was used to measure sleep duration. According to self-reported SD in the past month, LLD patients were divided into two subgroups: the LLD-SS group (LLD patients with short SD:≤6 h) and the LLD-NS group (LLD patients with normal SD: 7-8 h) [27]. Patients with other values of self-reported SD were not included in the study.
Psychometric assessments
The participants underwent a comprehensive battery of psychometric assessments by a trained psychologist and a psychiatrist in a specific room. The battery assessed 1) global cognitive performance with the Mini-Mental State Examination (MMSE), 2) activities of daily living with the Activities of Daily Living Scale (ADL), 3) memory function with the Auditory Verbal Learning Test (N5, the recognition item), 4) visuospatial skills with the Rey-Osterrieth Complex Figure test, 5) working memory with the Digit Span Test, 6) language function with the Verbal Fluency Test, 7) executive function with Stroop Color and Word Test C, and 8) information processing speed (IPS) with the Symbolic Digit Transformation Test (SDMT).
Depressive symptoms were assessed with the Geriatric Depression Scale (GDS), a battery that lacks items assessing sleep disturbance, and the adjusted 17-item Hamilton Depression Rating Scale (HAMD), in which the scores on sleep-related items (items 4, 5 and 6) were excluded to minimize any effects of sleep disturbance on the severity of depression (below, HAMD scores refer to adjusted HAMD scores) [40, 50].
MRI acquisition and preprocessing
The participants underwent MRI scans on Philips 3.0T MR systems. A single-shot gradient echo-planar imaging (EPI) pulse sequence in 8 min was used to obtain a sagittal resting-state fMRI dataset. The parameters of the EPI pulse sequence were as follows: TE = 30 ms, TR = 2000 ms, volume = 240, flip angle (FA) = 90 degrees, number of slices = 33, slice thickness = 4 mm, matrix size = 64×64, and field of view (FOV) = 220×220 mm. Statistical Parametric Mapping (SPM12) and Data Processing Assistant for Resting-State 5.1 (DPASF 5.1) were used for data preprocessing [51]. After the first 10 images were discarded, the remaining 230 volumes were corrected for slice timing and head motion. Head motion data were provided after realignment correction. Participants were excluded if they had > 2° of angular motion, 2 mm of displacement in any plane, or 0.2 mm of mean framewise displacement (FD) (no participants were excluded). The standard Montreal Neurological Institute (MNI) EPI template was applied for spatial normalization, and the images were resampled to 3×3×3 mm3 and smoothed using a 6-mm full-width at half-maximum (FWHM) Gaussian kernel. After removing the linear trend, signals of white matter, cerebrospinal fluid, and the Friston-24 parameters of head motion were regressed out as nuisance covariates [52]. To minimize the influence of head motion, the mean FD of each participant was regressed out in group-level analysis. A bandpass filter of 0.01–0.1 Hz was applied [53].
Seed-based FC analysis
Regions of interest (ROI) in the seed-based FC analysis were the left and right insula, anatomically derived from the automated anatomical labeling atlas [54, 55]. The time-series data in each ROI were extracted and averaged for reference as the seed point. FC maps of each individual were acquired from the Pearson correlation coefficient between the averaged time series of each ROI and the time series of each voxel of the whole brain. Fisher’s r-to-z transformation was used to improve the normality of FC maps. Group-level statistical analyses of FC were based on z-score maps.
Statistical analyses
Statistical analyses were carried out using The Statistical Package for the Social Sciences (IBM SPSS 25.0). Demographic variables were analyzed by univariate ANOVA with general linear model and the χ2 test. Psychometric variables were analyzed by ANCOVA with general linear model, and sex, age, and years of education were included as covariates. The least significant difference (LSD) method was used to determine significant differences between pairwise comparisons. All statistical tests were two-tailed, and the significance level was defined as p < 0.05.
For FC analyses, significant differences among the three groups were tested using one-way ANCOVA on z-score maps for each ROI. The FC maps were corrected using a false discovery rate (FDR) correction at q < 0.05. The significantly different regions among the three groups in ANCOVA were extracted and averaged for post hoc analysis with LSD correction. Control variables included mean FD, sex, age, and years of education.
Partial correlation analyses were applied to detect the relationships among SD, psychometric variables, and FC, controlling sex, age, and years of education. Multiple linear regression analyses were used to further explore the factors that determine SD-related cognitive performance and insular FC. Dependent variables included neuropsychological scores and FC respectively that significantly correlated with SD in correlation analyses, independent variables included SD, LLD, an interaction term between SD and LLD, and other variables that correlated with dependent variables. Specifically, the regression model was first constructed with covariates including age, sex, year of education and FD (FD was included when FC was a dependent variable). Then a stepwise analysis method was used for independent variables, with p(entry) 0.05 and p(removal) 0.10. Each potential independent variables was tested as it was added to the model, retaining those deemed most statistically significant. This process is repeated until the results are optimal.
Validation analysis
Depressive symptoms (HAMD scores) and insomnia symptoms (sleep items of the HAMD) were controlled to validate the comparison of cognitive performance and insular FC among the three groups.
RESULTS
Demographic and psychometric characteristics
Demographic and psychometric data are listed in Table 1. There was no significant difference in age or sex distribution among the three groups. The LLD-SS group had significantly fewer years of education and lower scores on the ADL, MMSE, and SMDT as well as higher HAMD scores than the other two groups (p < 0.05, LSD correction). The NC group exhibited significantly lower GDS and HAMD scores and higher scores on the MMSE, Auditory-Verbal Learning Test, Rey– Osterrieth Complex Figure test, Digit Span Test, Verbal Fluency Test, and SDMT than the other two groups (p < 0.05, LSD correction). No significant difference was found in scores on the Stroop Color and Word Test C among the three groups. Functional MRI data were collected and analyzed from 56 LLD-SS patients, 25 LLD-NS patients and 54 NC. There was no significant difference in FD among the three groups (LLD-SS patients: 0.051±0.021, LLD-NS patients: 0.053±0.029, NC: 0.047±0.023, F = 0.794, p = 0.454).
Demographic and clinical data of all participants
SD, self-report sleep duration; LLD-SS, late-life depression with short SD; LLD-NS, late-life depression with normal SD; NC, normal control; HAMDa, adjusted Hamilton Depression Scale (sleep items were removed); GDS, Geriatric Depression Scale; ADL, activities of daily living; MMSE, Mini-Mental State Examination; DST, Digit Span Test; SDMT, Symbolic Digit Transformation Test. *Age, sex, and years of education were included as control variables. #A, LLD-SS; B, LLD-NS; C, NC.
Differences in insular FC among the LLD-SS, LLD-NS, and NC groups
The ANCOVA on insular FC revealed differences in FC among the LLD-SS, LLD-NS and NC groups (shown in Table 2 and Fig. 1A, B), including the FC (1) between the left insula and right inferior frontal gyrus (IFG) pars triangularis, and (2) between the right insula and right IFG pars triangularis. In the post hoc analysis (Fig. 1C), the LLD-SS group exhibited increased FC between the left insula and right IFG pars triangularis compared with the LLD-NS (p < 0.001) and NC group (p < 0.001) and increased FC between the right insula and right IFG pars triangularis compared with the LLD-NS (p < 0.001) and NC group (p < 0.001). The LLD-NS group exhibited decreased FC between the left insula and right IFG pars triangularis compared with NC group (p = 0.047) and between the right insula and right IFG pars triangularis compared with the HC group (p = 0.011).
Differences of FC among LLD-SS, LLD-NS, and NC group
False discovery rate (FDR) at q < 0.05. FC, functional connectivity; ROI, regions of interest. LLD-SS, late-life depression with short sleep duration; LLD-NS, late-life depression with normal sleep duration; NC, normal control; MNI, Montreal Neurological Institute; IFG, inferior frontal gyrus.
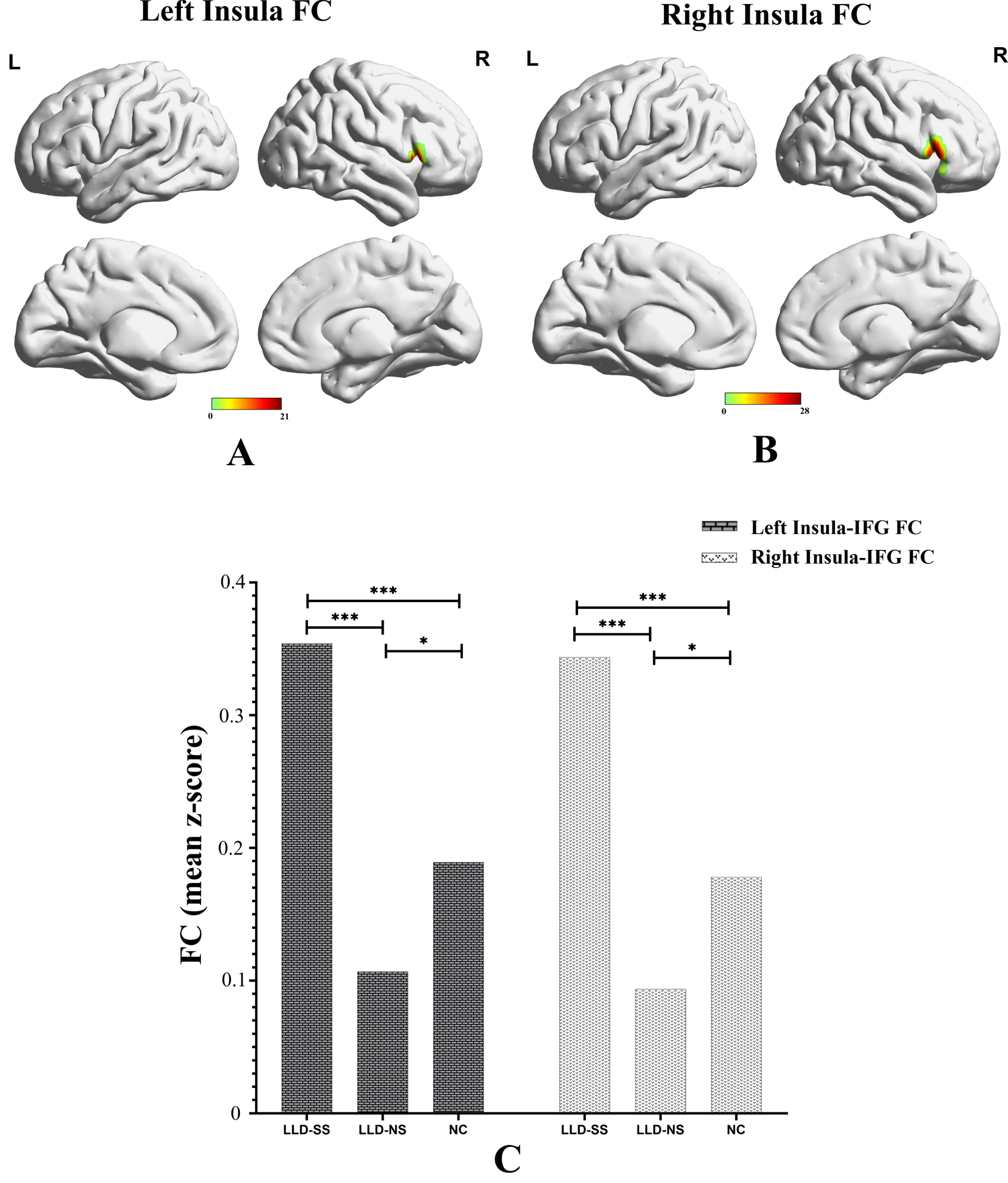
Differences of FC among LLD-SS, LLD-NS, and NC group. A) Differences of FC between left insula and right IFG pars triangularis; B) Differences of FC between right insula and right IFG pars triangularis; C) Comparison of FC among LLD-SS, LLD-NS, and NC group: LLD-SS group exhibited increased FC between left insula and right IFG pars triangularis, and between right insula and right IFG pars triangularis compared with LLD-NS (p < 0.001, p < 0.001) and NC group (p < 0.001, p < 0.001). LLD-NS group exhibited decreased FC between left insula and right IFG pars triangularis, and between right insula and right IFG pars triangularis compared with NC group (p = 0.047, p = 0.011). *p < 0.05; **p < 0.01; ***p < 0.001. FC, functional connectivity; LLD-SS, late-life depression with short sleep duration; LLD-NS, late-life depression with normal sleep duration; NC, normal control; IFG, inferior frontal gyrus.
Correlation and regression analyses
In all participants, SD was correlated with HAMD (r = –0.26, p < 0.001), GDS (r = –0.21, p = 0.006), ADL (r = 0.20, p = 0.001), MMSE (r = 0.39, p < 0.001) and SDMT scores (r = 0.28, p < 0.001). No significant correlation was found between SD and other psychometric characteristics. Furthermore, regression analyses of the psychometric variables exhibited that 1) MMSE was associated with SD (β= 0.23, p < 0.001), LLD (β=–0.29, p < 0.001), interaction between SD and LLD (β= 0.09, p = 0.049), and HAMD (β=–0.25, p < 0.001); and that 2) SDMT was associated with SD (β= 0.14, p = 0.007), LLD (β=–0.26, p < 0.001), and HAMD (β=–0.22, p < 0.001) (Table 3).
Regression analyses of the psychometric variables and insular FC
#a categorical variable representing whether the participants suffered LLD or not. *an interaction term between SD and LLD. LLD, late-life depression; FC, functional connectivity; SD, sleep duration; MMSE, Mini-Mental State Examination; SDMT, Symbol-Digit Modality Test.
In participants who underwent functional MRI scans, SD was correlated with FC between the left insula and right IFG pars triangularis (r = –0.27, p = 0.001) and FC between the right insula and right IFG pars triangularis (r = –0.38 p < 0.001); FC between the right insula and right IFG pars triangularis correlated with HAMD (r = 0.19, p = 0.030) and SDMT scores (r = –0.27, p = 0.002). Furthermore, regression analyses of the insular FC exhibited that 1) FC between the left insula and right IFG pars triangularis was associated with SD (β=–0.20, p = 0.019), LLD (β= 0.22, p = 0.011), interaction between SD and LLD (β=–0.21, p = 0.011), and that 2) FC between the right insula and right IFG pars triangularis was associated with SD (β=–0.28, p < 0.001), LLD (β= 0.20, p = 0.019), interaction between SD and LLD (β=–0.22, p = 0.006) and SDMT (β=–0.19, p = 0.034) (Table 3).
Validation results
The main results validated the comparison of cognitive performance and insular FC among the three groups (Supplementary Tables 1 and 2).
DISCUSSION
The present study investigated the insular FC of LLD patients with short SD and explored the influence of insular FC on the relationship between SD and cognition. The main results are as follows. First, LLD-SS patients exhibited more severe depressive symptoms and worse cognitive function (especially in global cognition, ADL, and IPS) than LLD-NS patients and NC. SD significantly correlated with global cognition and IPS after adjusting potential confounders. Second, LLD-SS patients exhibited higher FC between the bilateral insula and IFG pars triangularis than the LLD-NS and NC group, while LLD-NS patients showed lower FC between the bilateral insula and IFG pars triangularis than the NC group. And this increase in insular FC was correlated with shorter SD, more severe depressive symptoms and slower IPS. Third, an additive effect was found between SD and LLD on global cognition and insular FC.
Accumulating evidence has indicated a crucial role of amyloid-β clearance in the relationship between short SD and the risk of AD, as short SD reduces clearance [56, 57]. Consistent with these experimental findings, an epidemiological study found an association between self-reported short SD and a greater amyloid-β burden in community-dwelling older adults [58]. Another study with a sample size of 4,000 individuals also found that self-reported short SD correlated with a high amyloid-β burden, which was associated with cognitive decline [27]. It is well acknowledged that short SD and cognitive impairment are common manifestations of LLD and may be influenced by the severity of depression [29, 59], which may lead to an underestimation of the effects of short SD on impaired cognition caused by potential AD-related pathology. In the present study, LLD patients with self-reported short SD exhibited impaired cognition relative to LLD patients with adequate SD and NC, and SD correlated with cognitive performance after adjustment for potential confounders. Furthermore, an additive effect was found between SD and LLD on global cognition. The results suggest that LLD patients with self-reported short SD may be more vulnerable to cognitive decline caused by AD-related pathology. Therefore, intervention for short SD in patients with LLD should be emphasized. Furthermore, longitudinal studies are necessary to verify the risk of AD in LLD patients with short SD and whether interventions for short SD decrease the risk of AD.
We found that LLD patients with short SD exhibited increased FC between the bilateral insula and right IFG pars triangularis compared with the LLD-NS and NC group. In addition, these increased FC values were associated with short SD, severe depressive symptoms and poor cognitive performance. Similarly, increased activation of the insula and IFG were detected by assessing the amplitude of low-frequency fluctuations (ALFF) in major depressive disorder patients with insomnia complaints [40]. Studies have shown that the IFG is correlated with deliberative processing, response inhibition, emotion regulation and memory maintenance [60–63]. In an fMRI study using a modular graph theoretic analysis, the largest homotopic module (defined as the insular module, containing the IFG pars triangularis) was disrupted in AD, and the corresponding gray matter concentration was decreased in AD patients compared with NC [64]. NC carrying APOE ɛ4 showed higher fractional ALFF in the insula and IFG compared with those not carrying APOE ɛ4, indicating that greater activation may act as a compensatory mechanism against the neural challenges arising from AD pathology [65]. Additionally, according to a meta-analysis, the anterior insula and IFG were the only regions with overlapping activation for both physiological and psychosocial stressors, and this activation was considered to be a global neural stress reaction [66]. And there was found an additive effect between SD and LLD on FC between the bilateral insula and right IFG pars triangularis in the present study. Given the above findings and, it could be inferred that the increased FC between the insula and IFG in the present study may be a neural stress reaction due to short SD, more severe depressive symptoms and potential AD-related pathology. Similar to previous studies [47–49], the LLD-NS group showed lower FC between the bilateral insula and IFG pars triangularis than the NC group, but only the difference in FC between the left insula and right IFG pars triangularis was significantly lower than that in the NC group (p = 0.047) and therefore should be interpreted cautiously. The decreased FC may be a manifestation of lower insular function in LLD. In the present study, the sign of changes in insular FC was associated with SD, and the underlying neural mechanism should be further explored in future studies.
In the present study, IPS seemed to be the most vulnerable to LLD-induced changes, as IPS scores were significantly lower in LLD-SS patients than in LLD-NS patients and NC, and IPS was correlated with SD and insular FC after adjusting for potential confounders; other cognitive domains did not show the same pattern. Among various cognitive impairments in patients with LLD, slower IPS is considered as the most core domain, and it plays a critical role in downstream processes of other cognitive domains [67, 68]. Moreover, slower processing speed impairs the development of expectancies in antidepressant trials with LLD patients, which may help explain the lower antidepressant response among older adults [69]. Therefore, greater attention should be given to IPS in LLD-SS patients, and early intervention may improve their prognosis. Furthermore, a previous study reported that the activation of the IFG and anterior insula is often discounted as due to motor inhibition or orienting responses, rather than changes in speed– accuracy trade-offs [70], which may affect IPS. Therefore, the FC between the right insula and right IFG pars triangularis may be a therapeutic target for neuromodulation to alleviate cognitive and sleep problems in LLD patients.
There are a few limitations of our study. First, self-reported SD is a subjective measure used as a proxy for poor sleep. The use of this proxy is supported by previous studies that reported a correlation between high amyloid-β burden and indices of poor sleep quality, including subjective sleep quality [71], objective sleep efficiency and fragmentation [72, 73], and nonrapid eye movement slow wave activity [74]. In the present study, the statistical significance of associations decreased when insomnia was controlled as a covariate, which means insomnia may mediate the impacts of short SD on cognition and FC. Therefore, future studies with objective sleep measures should be performed to resolve this discrepancy. Second, variable types and doses of antidepressants may be confounding factors in the relationships among FC, cognitive function, and depressive symptoms. Third, the insula is a heterogeneous brain region that comprises three cytoarchitecturally distinct subregions [75]. Further studies using insula subregions (rather than the entire insula) as ROIs may provide more detailed insights into the role of insular FC in LLD-SS patients. Additionally, other brain areas may be correlated with LLD and short SD, which merit further exploration. Fourth, the results from the present study were based on cross-sectional data, and the causality of associations among short SD, insular FC and risk of dementia could not be established. Well-designed longitudinal studies are needed in the future.
In conclusion, the LLD-SS group exhibited worse global cognition, slower IPS, and increased FC between the bilateral insula and IFG pars triangularis compared with the LLD-NS and NC group, suggesting that LLD patients with short SD may have a higher risk of developing dementia. Moreover, this increased insular FC was associated with short SD and poor cognitive performance. In particular, an additive effect was found between sleep duration and LLD on global cognition and insular FC. Abnormal FC in LLD patients with short SD may be therapeutic targets for neuromodulation to improve sleep and cognitive performance and thus decrease the risk of dementia. Future studies are needed to investigate whether interventions to normalize insular FC in LLD patients with short SD could decrease the risk of developing dementia and clarify its underlying mechanisms.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This study was supported by a grant from the National Natural Science Foundation of China (No. 82171533, No. 82101508), Medical Scientific Technology Research Foundation of Guangdong Province of China (NO.A2020446), the Key Laboratory for Innovation Platform Plan, the Science and Technology Program of Guangzhou, China, the Science and Technology Plan Project of Guangdong Province (No. 2019B030316001), Key Medical Specialty Construction Project of Traditional Chinese Medical Science in the 13th Five-Year Plan of Guangdong Province; Key Medical Specialty Construction Project of Traditional Chinese Medical Science of Guangzhou (2020–2022). Guangzhou Municipal Key Discipline in Medicine (2021-2023), Guangzhou High-level Clinical Key Specialty, Guangzhou Research-oriented Hospital. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available from the corresponding author upon reasonable request.