
Abstract
Background:
Neuroinflammation has been postulated to play an important role in cognitive impairment, cognitive decline, and dementia. Inflammatory biomarkers such as interleukin-6 (IL-6) and IL-8 are found to be associated with the neuro-inflammatory process and worse cognitive function. However, it is unknown whether these interleukins are associated with long-term cognitive function.
Objective:
To investigate the association of baseline IL-6 and IL-8 with cognitive function at baseline as well as its association with cognitive decline over five-year follow-up.
Methods:
387 patients were recruited from an ongoing memory clinic-based study who underwent comprehensive physical, medical, neuropsychological and blood assessments together with brain MRI. IL-6 and IL-8 were measured using LUMINEX assays. The National Institute of Neurological Disorders and Stroke-Canadian Stroke Network neuropsychological battery was used to assess cognitive decline across multiple domains.
Results:
Among the 387 (mean age = 72.9 years and 53.7% males) participants, 322 had at least two follow-up assessments and were included in the longitudinal analysis. Negative linear trend associations were found between tertiles of IL-8 with baseline global cognition (p-trend< 0.001), attention (p-trend = 0.005), executive function (p-trend< 0.001), and visuospatial function (p-trend = 0.002) domains. No association was found between baseline IL-8 and cognitive decline. IL-6 was not associated with both baseline and follow-up cognition.
Conclusion:
IL-8 was associated with worse cognition especially in attention, executive function, and visuospatial function, suggesting the role of neuroinflammation in cognitive impairment. Hence, blood inflammatory biomarkers may be useful indicators in identifying patients at risk of cognitive impairment and warrant consideration for inclusion in treatment trials.
Keywords
INTRODUCTION
Cognitive impairment and dementia are increasingly important public health concerns globally [1]. Several risk factors such as Apolipoprotein E4, diabetes, cerebrovascular disease, and age are found to be associated with cognitive impairment and cognitive decline [2]. Studies have shown that amyloid plaques and neurofibrillary tangles, which are associated with Alzheimer’s disease (AD) pathology, lead to cognitive decline [3]. However, some studies have suggested that there is heterogeneity in cognitive decline, whereby the rate of decline is not significantly associated with factors such as aging [4], suggesting that other factors such as neuroinflammation may play a significant role.
Findings from animal models and clinical studies have shown that chronic neuroinflammation may contribute to cognitive decline [5, 6], where inflammatory mechanisms such as cytokine-mediated interactions with the central nervous system, results in cognitive impairment and eventually cognitive decline and dementia [7]. Interleukin-6 (IL-6), which is a pro-inflammatory cytokine, and interleukin-8 (IL-8), a pro-inflammatory chemokine, are suggested to be involved in this process of neuroinflammation [8, 9].
Several clinical studies suggest that higher levels of blood IL-6 [10] and IL-8 [11] are associated with cognitive impairment in patients with AD. However, these findings have been inconsistent across studies in patients with mild cognitive impairment (MCI) as well as in patients with AD [12], where some studies found that higher levels of these biomarkers were negatively associated with cognitive function in non-demented adults, community-based stroke-free population, and elderly patients with cardiovascular disease [13–15], while others studies in patients with AD [16] and elderly community subjects [17] did not find any association. Moreover, a majority of the studies investigating these two cytokines with cognitive impairment were cross-sectional in design, with a very few longitudinal studies limiting the ability to determine the direction of causality. These previous studies were mainly limited to Caucasian populations with limited data involving Asian populations, which have been known to have higher prevalence of vascular risk factors, cerebral small vessel disease, and cognitive impairment [18].
Thus, in this study, we aim to determine the association of IL-6 and IL-8 with cognitive function at baseline in an Asian memory clinic population in Singapore as well as the longitudinal association of baseline IL-6 and IL-8 with cognitive decline over a follow-up of five years.
METHODS
Study sample
This study was conducted as part of an ongoing prospective study where participants were recruited from memory clinics at the National University Hospital, Singapore. Participants had one of the following diagnoses during baseline evaluation [19]: No Cognitive Impairment (NCI), defined as having no functional or impairment in cognition as assessed through neuropsychological tests; Cognitive Impairment No Dementia (CIND), defined by having impairment in one or more cognitive domains based on neuropsychological tests but were not diagnosed with dementia based on the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition (DSM-IV) criteria; and dementia was diagnosed based on DMS-IV criteria. The etiological diagnoses of dementia were based on internationally accepted criteria: Alzheimer’s disease (AD) was diagnosed using the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) and VaD was defined using the National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherche et l’ Enseignement en Neurosciences (NINDS-AIREN) criteria.
For this study, a total of 537 consecutive patients were recruited between August 2010 to September 2016. Participants underwent clinical examinations, laboratory investigations, and neuropsychological assessments at the National University of Singapore annually, except for brain MRI which was offered biennially. Of these participants, 159 patients were excluded from the analysis as 130 patients had missing blood tests and 29 patients had incomplete or no baseline MRI (Fig. 1). 378 patients were thus included in the cross-sectional analysis. To assess for cognitive decline, participants with baseline and at least two follow-up neuropsychological assessments were included in the analysis. This resulted in the exclusion of 56 patients, leaving 322 patients for the longitudinal study.
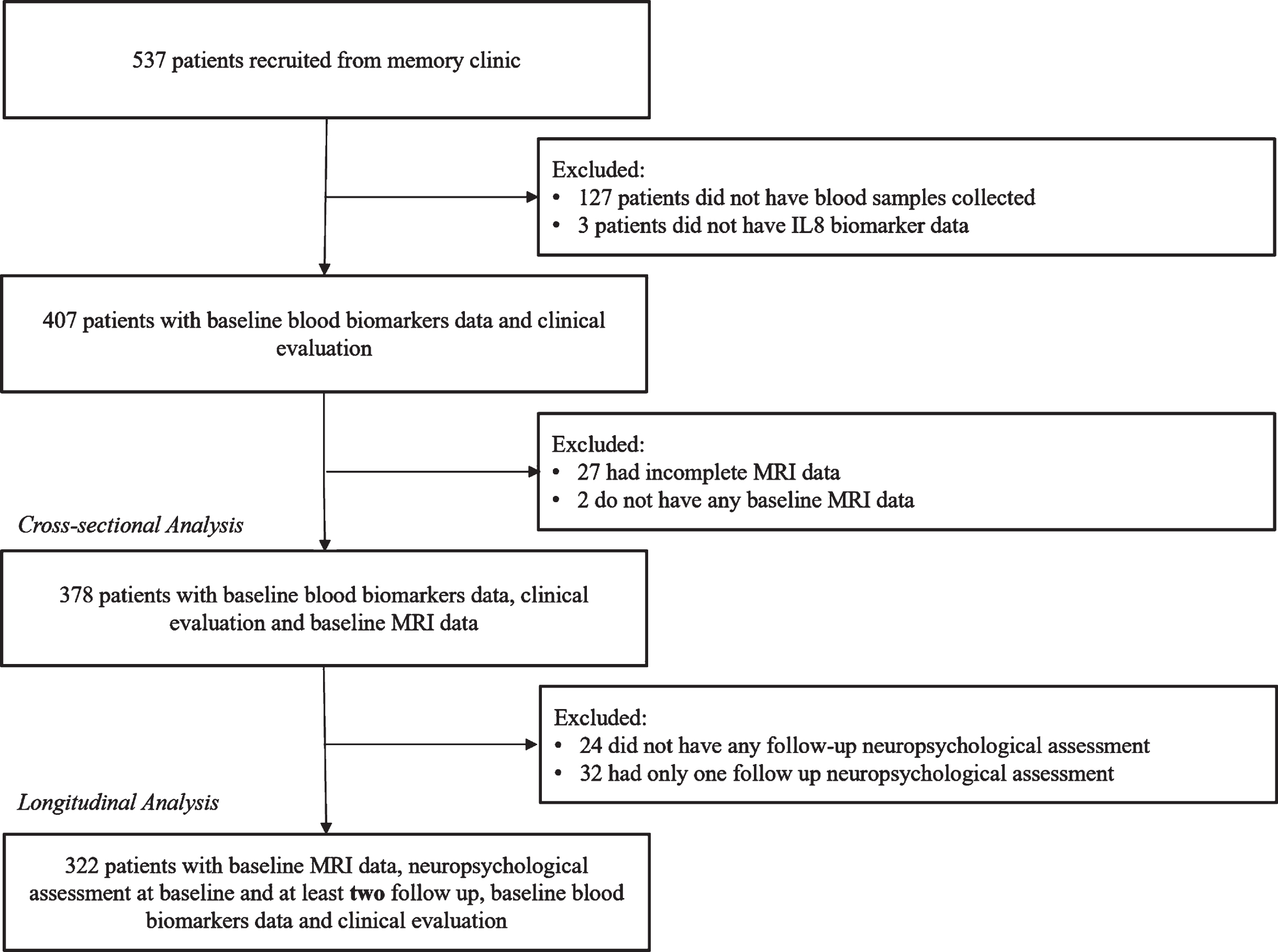
Selection of participants IL-6, Interleukin-6; IL8, Interleukin-6; MRI, magnetic resonance imaging.
Institutional ethics approval was obtained from the National Healthcare Group Domain-Specific Review Board. The study was conducted according to the Declaration of Helsinki. Written informed consent was obtained from all patients in their preferred language before recruitment.
Covariate assessment
A detailed questionnaire was administered at baseline to all patients to collect information on age, sex, race, years of education and past medical history of hypertension, hyperlipidemia, and diabetes mellitus. Patients’ medical history was also thereafter verified through the reviewing of their medical records.
Peripheral inflammatory markers
Non-fasting blood samples were drawn from patients into serum-separating tubes. The samples were centrifuged at 2,000 RCF at 4°C for 10 min and the serum samples were stored at –80°C until being used for analysis. Multiplex xMAP-based Luminex assays (Millipore Corp., Billerica, MA, USA) were utilized to measure the concentrations of several assays part of 9-plex Human Adipokine Panel such as Nerve Growth Factor, IL-6, IL-8, Insulin, Leptin, Hepatocyte Growth Factor, MCP-1, IL-1β, and TNFα. However, for this study, only the data of IL-6 and IL-8 were analyzed. The range of concentrations detectable were 0.2 to 15,000 pg/mL for IL-6 and 0.3 to 10,000 pg/mL for IL-8. For 101 cases whose IL-6 concentration fell below detectable range, the lowest detectable value (0.2 pg/mL) was used in statistical analyses. No cases were detected lower than the detectable range for IL-8. Quality controls included in both were within lot-specific target ranges and were established from 12 independent assays. Luminex based multiplexing platform is now well-established, with multiple papers across different disciplines using them. In terms of reliability, while batch to batch differences may exist, their intra- and inter-assay % CV for both IL6 and IL8 are below 10 and 15% respectively. For the analyses, the biomarkers concentration values were categorized into tertiles as determined by the respective biomarker levels in the study.
Neuroimaging
All participants underwent a brain MRI, performed on a 3T Siemens Magnetom Trio Tim scanner utilizing a 32-channel head coil, at baseline at the Clinical Imaging Research Centre of National University of Singapore. Patients who were unable to undergo MRI scans due to reasons such as claustrophobia and contraindications for MRI were excluded from this study. The standardized neuroimaging protocol used for this study included 3-dimensional T1-weighted, T2-weighted, fluid-attenuated inversion recovery (FLAIR), and susceptibility weighted imaging sequences.
The following MRI markers of cerebrovascular disease (CeVD) were graded based on STRIVE criteria [20]: Lacunes were defined as round or ovoid lesions involving the subcortical regions, 3 to 15 mm in diameter, with a low signal on T1-weighted images and fluid-attenuated inversion recovery, a high signal on T2-weighted images, and a hyperintense rim with a center following the cerebrospinal fluid intensity [20]. White matter hyperintensity (WMH) was graded based on the Age-Related White Matter Changes (ARWMC) scale [21]. Cortical infarcts were defined as focal lesions interrupting the cortex gray/white junction, signal following cerebrospinal fluid intensity, hyperintense rim on FLAIR images, and tissue loss of variable magnitude, with prominent adjacent sulci and ipsilateral ventricular enlargement [20]. Patients were determined to have significant CeVD when there was presence of cortical infarct, at least two lacunes or confluent WMH where ARWMC score≥8 [11].
Neuropsychological assessment
All patients completed the National Institute of Neurological Disorders and Stroke– Canadian Stroke Network battery [19] neuropsychological test battery to assess their cognition at baseline and at follow up visits. The 60 min protocol covers the following cognitive domains: Attention: Digit span forward and backward Executive function: Verbal fluency, Color Trial Test A and B Memory: Rey Complex Figure Test – immediate/delayed recall and recognition and Hopkins Verbal Learning Test – immediate/delayed recall and recognition Language: 15-item modified Boston Naming Test Visuomotor speed: Symbol Digit Modalities Test Visuospatial function: Rey Complex Figure Test-copy
All raw scores for the individual tests were transformed to standardized z-scores using the means and standard deviation of the control group, patients with NCI. The score for each cognitive domain was calculated by taking the average of the z-scores for the respective tests for that domain and then standardized based on the composite mean and SD of the control group. The global score was computed by averaging the z-scores across the domains and standardized based on the mean and SD of the control group. For the follow-up visits, the global score and z-scores for each domain were computed based on the means and SDs of the control group at baseline [19].
Statistical analysis
Descriptive statistics consisted of counts and percentages for categorical variables (sex, hypertension, hyperlipidemia, diabetes, and significant CeVD), means and standard deviations for normally-distributed continuous variable (age) and median along with first quartile and third quartile were reported for continuous variables with skewed distribution (education, IL-6, IL-8). To compare baseline characteristics of participants who were included and excluded in the analyses, Chi-square tests was used for categorical variables, Student t-test was used for normally-distributed continuous variable and Wilcoxon rank-sum test was used for continuous variables with skewed distribution.
To assess the cross-sectional association between blood inflammatory biomarkers and baseline cognitive scores, multiple linear regression models were utilized. For the longitudinal analyses between baseline inflammatory biomarkers and cognitive decline, linear regression models with generalized estimating equations (GEE) were constructed to account for within-subject correlation between repeated measures taken across the period of follow-up. A first-order autoregressive correlation structure was specified along with the Huber-White Sandwich Estimator to obtain a robust standard error for the regression estimates. An interaction term between the biomarker and follow-up time was also included to investigate the heterogeneity of the biomarker effect on cognition over time. Biomarkers were included as categorical variables based on the tertiles in the models and test for linear trends (p-trend) were assessed by modelling tertiles as numeric variables (first tertile assigned numerical value of 1, second tertile assigned the value of 2 and the third tertile with the numerical value of 3). Log transformation (natural logarithm) was performed for skewed distributed inflammatory biomarkers data, which was used as continuous data in the supplementary analysis.
For both the cross-sectional and longitudinal analyses, regression models were adjusted for age, sex, education, and baseline diagnosis (no dementia versus dementia), hypertension, hyperlipidemia, diabetes, and significant CeVD. Baseline diagnosis of dementia was also adjusted across all models to account for differences in baseline cognitive impairment. For longitudinal analysis, time was included as a predictor in all models. Wald test was utilized to assess for any interaction between tertiles and baseline cognitive scores. In our secondary analysis, we divided our dementia participants into two groups, i.e., AD and VaD. All the analyses were performed for global cognition and domain-specific cognitive tests as outcomes in all patients and separately for patients with AD and VaD.
A p-value of < 0.05 was considered statistically significant for the interaction term between the baseline biomarker and time. Due to multiple testing when assessing cognitive scores of the specific domains, the Bonferroni correction was used such that the p-value of < 0.05/6≈0.0083 was considered statistically significant. All statistical analyses were performed using STATA Version 17.
RESULTS
Baseline characteristics
A total of 378 participants were included in the cross-sectional analysis. The baseline characteristics of study participants included and excluded from this analysis is shown in Table 1. Generally, those included and excluded in the analysis had similar profile for age, gender, education, hypertension, diabetes, and significant CeVD with those included in the analysis having a significantly lower proportion of participants with dementia at baseline than those excluded. The median concentrations of IL-6 and IL-8 among included participants were 1.28 pg/mL and 5.02 pg/mL respectively (Table 2). Of 378 participants, 90 were NCI, 156 CIND, 99 AD, and 33 VaD. The characteristics of NCI, CIND, AD, and VaD is shown in (Supplementary Table 1). NCI participants were youngest (mean age = 69.89 years) and with higher median number of years of education (10 years). They also have lowest burden of cardiovascular risk factors (hypertension 55%, hyperlipidemia 20%, and diabetes 25%) and cerebrovascular disease compared to CIND, AD, and VaD.
Baseline Characteristics of Study Participants
ap-value from Student t-test bp-value from Chi-square test cp-value from Wilcoxon rank-sum test d1 missing data (n = 158) e39 missing (n = 120) n, number; Q1, first quartile; Q3, third quartile; SD, standard deviation.
Baseline Biomarker Levels of Study Participants
IL-6, Interleukin-6; IL8: Interleukin-6; Q1, first quartile; Q3, third quartile.
Among the 378 participants, the 322 participants included in the longitudinal analysis were younger, had more years of education, but are less likely to have hypertension and significant CeVD compared to the 56 excluded participants (Supplementary Table 2).
Baseline inflammatory biomarkers and cognitive impairment
Table 3 shows the cross-sectional analyses of the association between the blood inflammatory biomarkers and cognitive scores at baseline. The highest tertile of IL-6 was significantly associated with lower global cognitive scores, executive function, memory, language, and visuospatial function in the unadjusted model (data not shown). However, these associations were no longer statistically significant after adjustment for demographics, cardiovascular risk factors and MRI markers, and there was no significant linear trend (i.e., p-trend > 0.05) (Table 3). Similar observations were seen, when IL-6 was treated as a continuous variable (Supplementary Table 3).
Association of Baseline Blood Inflammatory Biomarkers with Cognitive Scores
Multiple linear regression models used in this analysis (values represent regression coefficient [estimate] and 95% confidence interval [CI], and the degrees of freedom [df] of the numerator is 1 for all models and the dfs of the denominator for the t-test = 367) Reference group = tertile 1 All values adjusted for age, sex, education, and baseline diagnosis (No dementia versus dementia), hypertension, hyperlipidemia, diabetes, and significant CeVD aβ represents mean difference in cognitive scores per increase in natural log of IL-6 bβ represents mean difference in cognitive scores per increase in natural log of IL-8 95% CI, 95% confidence interval; IL-6, Interleukin-6; IL8, Interleukin-6.
There were significant negative linear trend found for the association between highest tertile of IL-8 with global score (p-trend< 0.001), attention (p-trend = 0.005), executive function (p-trend< 0.001), language (p-trend = 0.036), visuomotor speed (p-trend = 0.031), and visuospatial function (p-trend = 0.002) after adjusting for demographic variables, cardiovascular risk factors and the presence of significant CeVD (Table 3). In particular, participants in the highest tertile of IL-8 had poorer global cognition (β = –0.80, 95% CI = –1.23, –0.37), attention (β = –0.41, 95% CI = –0.70, –0.12), executive function (β = –0.85, 95% CI = –1.22, –0.47), language (β = –1.02, 95% CI = –1.96, –0.08), visuomotor speed (β = –0.22, 95% CI = –0.43, –0.02), and visuospatial function (β=–0.64, 95% CI = –1.04, –0.24) compared to the participants in the lowest tertile in Model 3. The association of IL-8 with attention, executive function and visuospatial function remained statistically significant after Bonferroni correction for multiple testing. Similarly, IL-8 was significantly associated with global score and executive function when analyzed as a continuous variable (Supplementary Table 3).
Baseline inflammatory biomarker and cognitive decline
There was a negative linear trend found for baseline IL-8 and executive function (p-trend = 0.022) at each time-point during the 5-year follow-up after adjusting for demographic factors, cardiovascular risk factors and presence of significant CeVD (Table 4). Participants in the highest tertile of IL-8 were more likely to have poorer executive function (β= –0.46, 95% CI = –0.86, –0.06) compared to participants in the lowest tertile at each time-point over the 5-year. This association was however no longer statistically significant after applying the Bonferroni correction. No other association was found between tertiles of IL-8 and global cognition or any other cognitive domains. In addition, there was no significant interaction found between IL-8 and time. For IL-6, similar to the cross-sectional analysis, there was no association seen between tertiles of IL-6 and global cognition or any of the cognitive domains. There were also no significant associations found when both biomarkers were analyzed as continuous variables (Supplementary Table 4).
Effect of Baseline Blood Inflammatory Biomarkers with Cognitive Scores over Time
Linear regression model with generalized estimating equations used in this analysis (values represent regression coefficient [estimate] and 95% confidence interval [CI], and degrees of freedom = 1 for all Wald chi-square tests, except for two-way interaction that have degrees of freedom = 10). Reference group = tertile 1 All values adjusted for age, sex, education and baseline diagnosis (no dementia versus dementia), hypertension, hyperlipidemia, diabetes, and significant CeVD p-trend based on regression models without the interaction term between biomarker and follow-up time aβ represents mean difference in cognitive scores per increase in natural log of IL-6 bβ represents mean difference in cognitive scores per increase in natural log of IL-8 95% CI, 95% confidence interval; IL-6, Interleukin-6; IL8, Interleukin-6.
Stratified analysis among participants with AD and VaD
Supplementary Tables 5 and 6 show the stratified analysis among participants with AD and VaD on the association between baseline inflammatory biomarkers with global and domain-specific cognitive scores across time respectively. On stratified analysis, there was no significant association between IL-6 and IL8 with cognitive decline in patients with AD (p-trend> 0.005). The analysis with patients with VaD showed similar results (p-trend> 0.005). There were no differences in cognitive decline in patients with AD and VaD.
DISCUSSION
In this study, we found that there were negative linear associations between IL-8 and global cognition, attention, executive function, language, visuomotor speed, and visuospatial function at baseline, of which the association with attention, executive function and Visuospatial function remained statistically significant after Bonferroni correction. Moreover, patients in the highest tertile of IL-8 had poorer cognitive performance compared to patients in the lowest tertile of IL-8, after adjusting for demographic, cardiovascular risk factors and presence of significant CeVD. No significant interaction between IL-8 and time was found suggesting no association between baseline IL-8 levels with cognitive decline over the five-year. In addition, there was no association between baseline IL-6 levels and cognitive impairment at baseline or cognitive decline over the 5-year follow-up.
IL-8 plays a regulatory role in the acute inflammatory process by attracting and activating acute neutrophils to the site of inflammation [22]. This is hypothesized to be associated with neurodegeneration and thus leading to cognitive decline [23]. It has been shown that higher levels of IL-8 were associated with AD. 11 but there have been inconsistent findings between IL-8 and cognitive function. Some studies did not find any association with global cognition [24] and other cognitive domains [25] while others have reported that IL-8 was associated with lower cognitive speed and memory domains [26]. Studies have postulated that IL-8 may lead to cognitive impairment via microglia in response to proinflammatory stimuli [27]. These stimuli may further initiate neurodegeneration as a result of excitotoxicity due to the production of glutamate, damaging neurons and oligodendrocytes [28]. The upregulation of IL-8 levels due to activated microglia may also lead to increased proinflammatory and pro-oxidant nitric oxide, which leads to vascular brain anomalies such as white matter hyperintensities, lacunes, and cortical infarcts and thereby affecting cognitive function [11, 29]. Conversely, it has also been reported that higher IL-8 levels were associated with better cognitive performance in memory, proposing that IL-8 may have a role in enabling the survival of hippocampal neurons in vitro. Our study is in concordance with the studies which suggest that higher levels of IL-8 was associated with cognitive impairment. However, we were unable to find any association between baseline IL-8 and cognitive decline in this study, this may be because cognitive decline is gradual process, as such 5-year of follow-up in this study may not be sufficient to detect cognitive decline. It may also be possible that along the different stages of cognitive decline different risk factors may have more prominent effects hence, the effect of inflammation especially IL-8 may be attenuated by other risk factors such as amyloid, tau, or cerebrovascular disease [18]. Moreover, the inflammatory reaction induced by increased level IL-8 in the brain may be counter-balanced by the production of other anti-inflammatory components, which may have different effect cognitive performance [30]. In this study IL-8 was a static exposure in the longitudinal analysis. Hence, future studies examining IL-8 as a time-varying exposure would increase our understanding on the association between IL-8 and cognitive decline.
IL-6 is secreted by glial cells and has been found to be upregulated adjacent to amyloid-β to form plaques indirectly via neuroinflammation [32] hence, many studies have been undertaken to better understand its role in the neurodegenerative process [10]. Increased levels of IL-6 have been found in AD [10, 12] but findings from previous studies to investigate IL-6 and its association with cognitive function and decline have been mixed. Despite some studies finding an association between IL-6 levels and global cognition [15, 33], memory [25], and executive function [34], our findings is in concordance with other studies which found that there were no associations between the biomarkers and cognitive function [16, 25] and decline [36]. Although IL-6 is found to be associated with amyloid-β, the lack of association between IL-6 levels and cognitive function as per our findings along with other studies could be due to peripheral IL-6 being differently regulated across various groups of individuals [37], hence, it may be less accurate in predicting the brain pathophysiology compared to CSF IL-6 concentrations. Also, the conflicting findings across studies could be due to IL-6 being found to not only contribute to the inflammatory response but also observed to have anti-inflammatory or regenerative effects [11, 38]. Moreover, cognitive decline is gradual and slow process, thus the association between IL-6 levels and cognitive decline may only be evident in later stages of the disease. For instance, there was no association observed for a longitudinal study between IL-6 and cognitive decline over a follow-up of 3-years [35], while other studies that spanned across seven to eight years follow-up periods found negative associations between cognitive decline and IL-6 levels [33, 39]. Additionally, the differences in findings may be, at least in part, due to low sensitivity of assay or selective non-responses and loss to follow-up by the frailer elderly in the memory clinic cohort.
Finally, the effects of the last tertile to the first tertile from the cross-sectional analysis were attenuated in the longitudinal analysis; these estimates are more or less comparable as they are estimating the effects of IL-6 and IL-8 on cognition score at each time point, and for cross-sectional analysis, the timepoint is specifically at baseline while longitudinal analysis have multiple time points. This could suggest the weakening of the IL-8 effect observed in the cross-sectional analysis resulting in non-significant findings in the longitudinal analysis. The attenuation of the effect could be heterogeneity in the IL-8 effect on score over time, but it was not detected in the interaction analysis. There could potentially be a lack of power in detecting the interaction, the 56 participants that were excluded from the longitudinal analysis but were still in the baseline analysis could be another reason for not detecting the interaction as there were some differences in the two groups of participants. In particular, the people included in the longitudinal analysis had lower median IL-6 and IL-8 levels than those excluded from the longitudinal analysis. Hence, further attenuating the effects. It has been further postulated that in healthy state or in preclinical stage disease, the inflammatory response at certain degree would be beneficial for the clearance of waste and toxins products from the brain and better cognitive performance, however, in later stages of disease, the chronic and severe inflammatory response which is beyond self-repair capacity would exacerbate the neuroinflammation, neurodegeneration and worse cognitive function [30]. Hence, our result with IL-6 and cognitive function may be partially driven by those patients who are at early stage of disease, i.e., patients with NCI and CIND.
Similarly, in secondary analysis among patients with AD and VaD, we were unable to find any association between baseline inflammatory biomarkers and cognitive decline and there were no differences in cognitive decline in those patients. Furthermore, patients with AD and VaD are at the late stage of disease where there is extensive brain damage, loss of synapse and neurodegeneration and further cognitive decline will be difficult to detect due to ceiling effect and may be masked by other comorbidities [19]. In this study, the number of participants with VaD is low (n = 33) which may have resulted in low power on detecting cognitive decline. Moreover, in this study the effect sizes for the associations between IL-6 and IL-8 with cognitive decline were in the negative direction, we cannot deny that baseline level of these biomarkers may have a subtle effect on cognitive decline in patients with AD and VaD. Although no direct conclusion can be drawn with respect to IL-6 and IL-8 and cognitive decline in patients with dementia from the present study, further studies with a larger sample size and longer duration of follow-up are required to confirm thesefindings.
The limitations of this study include, firstly, our population encompassed patients from the memory clinic which may reduce the generalizability of the findings to other populations such as the community. Secondly, even though our analyses accounted for numerous confounders, there may be some residual confounding which were not accounted for in our models. Additionally, given inter- and intra-individual variability of inflammation where the inflammatory blood biomarkers may be acutely influenced by factors such as sleep behavior and exercise [40], measuring the biomarker levels only once may potentially result in exposure misclassification. Lastly, only two inflammatory biomarkers were analyzed in this study for their association with cognitive function and decline. There could be other markers of inflammation that could be stronger predictors of cognition or brain pathology. The strengths of our study include the usage of a comprehensive neuropsychological test battery to better assess cognition for specific domains. Additionally, our study included longitudinal analyses which assisted in providing a better understanding of the possibility of causality compared to most existing studies which were cross-sectional in design. The use of GEE in the analysis enabled correlations between repeated measures taken during the follow-up assessments to be accounted for.
Conclusion
Our study found that IL-8 was associated with poorer global cognition at baseline, which is likely driven by the attention, executive function, and visuospatial function domains, regardless of the baseline diagnosis of dementia. These association was not similarly seen on follow-up and were attenuated. Nevertheless, this suggests that neuroinflammation might aid in the prediction of cognitive function, hence additional studies investigating mechanistic pathways are required to generate further insights into the pathology of cognitive decline and identify the future therapeutic target.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Footnotes
ACKNOWLEDGMENTS
We acknowledge all the Memory Aging & Cognition Centre, National University Hospital coordinators for their contribution to recruitment and data acquisition.
FUNDING
This work was supported by National Medical Research Council, Singapore [NMRC/CG/NUHS/2010, NMRC/CG/013/2013, NMRC/CIRG/1485/2018, NMRC/CSA-SI/007/2016], NUS start-up grant (A-0006088-00-00), National University Health System SEED funding (A-0006090-00-00), Transition Award (A-0006310-00-00) and Ministry of Education, Academic Research Fund Tier 1 (A-0006106-00-00).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.