
Abstract
Background:
Diabetes is a risk factor for cognitive impairment, and disease duration is associated with geriatric decline and functional disabilities.
Objective:
This study aimed to examine the association of diabetes duration with domain-specific cognitive impairment in elderly.
Methods:
A total of 3,142 participants from the National Health and Nutrition Examination Survey (NHANES) from the period between 2011 and 2014 were included. We assessed cognitive function using the Digit Symbol Substitution Test (DSST), the CERAD Word Learning (CERAD-WL) test, the CERAD Delayed Recall (CERAD-DR) test and animal fluency (AF) test.
Results:
After adjusting for age, sex, race/ethnicity, education level, and annual household income, we found that diabetes with a duration longer than 20 years were at 3.32-fold increased risk of DSST impairment (OR = 3.32, 95% CI: 1.95 to 5.67), 1.72-fold increased risk of CERAD-WL impairment (OR = 1.72, 95% CI: 1.13 to 2.62), and 1.76-fold increased risk of AF impairment (OR = 1.76, 95% CI: 1.23 to 2.53), compared with those with no diabetes. Associations were generally stronger in women than in men. Participants with diabetes, who were diagnosed at 50–59 years old were at increased risk of DSST impairment, CERAD-WL impairment, CERAD-DR impairment, and AF impairment per 5 years longer duration of diabetes.
Conclusion:
Longer diabetes duration was associated with the increased risk of cognitive impairment, especially in processing speed and attention. The presence of chronic kidney disease was associated with the increased risk of DSST impairment.
INTRODUCTION
Diabetes is a major health challenge worldwide, especially in the current aging society, and its prevalence is expected to increase to 10.4% by 2040 [1]. Diabetes can accelerate aging pathologies, and the disease duration is associated with geriatric decline and functional disabilities [2–4]. Evidence has shown that diabetes is a risk factor for brain health decline, including structural brain abnormalities [5–7], cognitive decline, and dementia [8, 9], which can be prevented at an early stage [10]. People with diabetes are shown to have deficits in cognitive function, particularly in memory [11, 12].
Many studies have focused not only on the impact of diabetes [13–15], but also on the impact of disease duration [16–18], antidiabetics use [19, 20], glucose fluctuation [21, 22], glucose control [3, 24], and disease management [25] on brain health, and have found controversial results. Among these factors, disease duration is increasingly recognized as an important risk factor for decline in health and for disease conditions, such as cardiovascular disease [26–28], cognitive impairment [29], and mortality [30, 31]. Moreover, Li et. al. found that the adverse effects of diabetes duration on health are more pronounced in women than in men [30]. Former studies have found that mid-life onset of diabetes, which means a longer duration of disease, has a higher risk of cognitive decline than that of late-life onset of diabetes [14, 32]. However, few studies have focused on the relationship between diabetes duration and domain-specific cognitive impairments. Cognitive impairment and dementia are diseases that emerge to be significant in old age. Thus, we aimed to examine the association between diabetes duration and domain-specific cognitive impairment in individuals aged >60 years using data from the 2011 to 2014 National Health and Nutrition Examination Survey (NHANES), a US national cohort.
METHODS
Data source and participants
The NHANES is a 2-year-cycle cross-sectional survey aimed at evaluating the health and nutritional status of the American population. The data analyzed in this study were obtained from the NHANES database from 2011 to 2014 because of the consistent cognitive testing used among participants aged >60 years during this period. The NHANES, as previously described [33] is a multistage probability sample of the non-institutionalized US population and allows estimates that represent the US population. A total of 19,931 participants were included in NHANES from 2011 to 2014. In the current study, we included people if they 1) were aged ≥60 years; 2) had undergone at least one cognitive test, including the Digit Symbol Substitution Test (DSST), Consortium to Establish a Registry for Alzheimer’s Disease Word Learning (CERAD-WL) test, Consortium to Establish a Registry for Alzheimer’s Disease Delayed Recall (CERAD-DR) test, or animal fluency (AF) test; and 3) had information on the duration of diabetes. Finally, 3,142 participants met the inclusion criteria and were enrolled in the current study. Furthermore, participants for whom information on the age of disease onset was available were included in the subgroup analysis.
Exposures and outcomes
Type 2 diabetes was diagnosed according to the following standards: 1) fasting blood glucose ≥126 mg/dL or glycated hemoglobin (HbA1c) ≥6.5%; 2) diagnosis by a physician; 3) use of antidiabetic medication; or 4) hospital record of type 2 diabetes. Diabetes duration and age at diagnosis were collected using the question, “How old were you when a doctor or other health professional first told you that you had diabetes or sugar diabetes?”. Diabetes duration was measured by the number of years. We defined the duration of new-diagnosed diabetes as 1 year and non-diabetes as 0. In the current analysis, the diabetes duration was divided into six groups: 0 year, 1–4 years, 5–9 years, 10–14 years, 15–19 years, and ≥20 years. We also collected the information of age at diabetes diagnosis from questionnaire.
In the survey, four cognitive tests were conducted (DSST, CERAD-WL, CERAD-DR, and AF), which have been widely used in largescale screening, epidemiological, and clinical studies [34–37]. All cognitive tests were assessed in a household interview or a Mobile Examination Center (MEC), which are parts of the NHANES.
The DSST relies on processing speed, sustained attention, and working memory and is regarded as a high-sensitivity cognitive test to detect cognitive dysfunction [38, 39]. The CERAD-WL and CERAD-DR were used to assess immediate and delayed memory, respectively [40]. The AF test examines categorical verbal fluency, which is a component of executive function [41]. In these four cognitive tests, a higher score indicates better cognitive performance.
Because no gold standard cut-off score exists for the CERAD, DSST, and AF tests to identify cognitive impairment, we used the lowest quartile of the score as the threshold point, according to previous studies [42, 43]. Thus, the cut-off points of the DSST, CERAD-WL, CERAD-WL, and AF tests were 30, 14, 5, and 17, respectively.
Covariables
Potential confounding factors included age (continuous variable), sex (male and female), race (black and others), smoking status (current smokers and others), fasting glucose level (continuous variable), hypertension, chronic kidney disease, cardiovascular disease, annual household income (whether more or equal to 65,000 US Dollars or not), education level (whether college graduate or above), and body mass index (BMI). Chronic kidney disease (CKD) and cardiovascular disease (CVD) were determined using a combination of self-reported physician diagnoses and standardized medical status questionnaires completed during individual interviews. All these data were selected from the NHANES database directly and were included in the analysis model to eliminate potential bias as much as possible.
Statistical analysis
Diabetes duration is an ordinal categorical variable; therefore, Spearman correlation analysis was used to determine between-group differences in cross-sectional characteristics for continuous data, and the Mantel – Haenszel chi-square test was used for dichotomous and categorical data. Linear regression was used to assess the relationship between two continuous variables. Logistic regression was used to examine the association between two categorical variables. Model 1 was adjusted for age, sex, race, educational level, and annual household income. Model 2 was further adjusted for log albuminuria, BMI, HbA1c, smoking status, hypertension, chronic kidney disease, and cardiovascular disease. We performed further analyses in men and women. Statistical significance was defined as a two-sided p-value of <0.05. All analyses were performed using STATA (version 15.0) (STATA Corporation, College Station, TX, USA).
RESULTS
Characteristics of the participants
Overall, 3,632 individuals from the total 19,931 participants of the NHANES (2011–2014) were aged ≥60 years. Of these, 451 and 39 participants were excluded because of the absence of data on cognitive test scores and diabetes duration, respectively. Finally, 3,142 participants, including those with and without diabetes, were included in the analysis of the relationship between diabetes duration and domain-specific cognitive impairment (Fig. 1). However, because of missing data only 894 participants were included in the analysis of the relationship between the age at diabetes onset and domain-specific cognitive impairment.
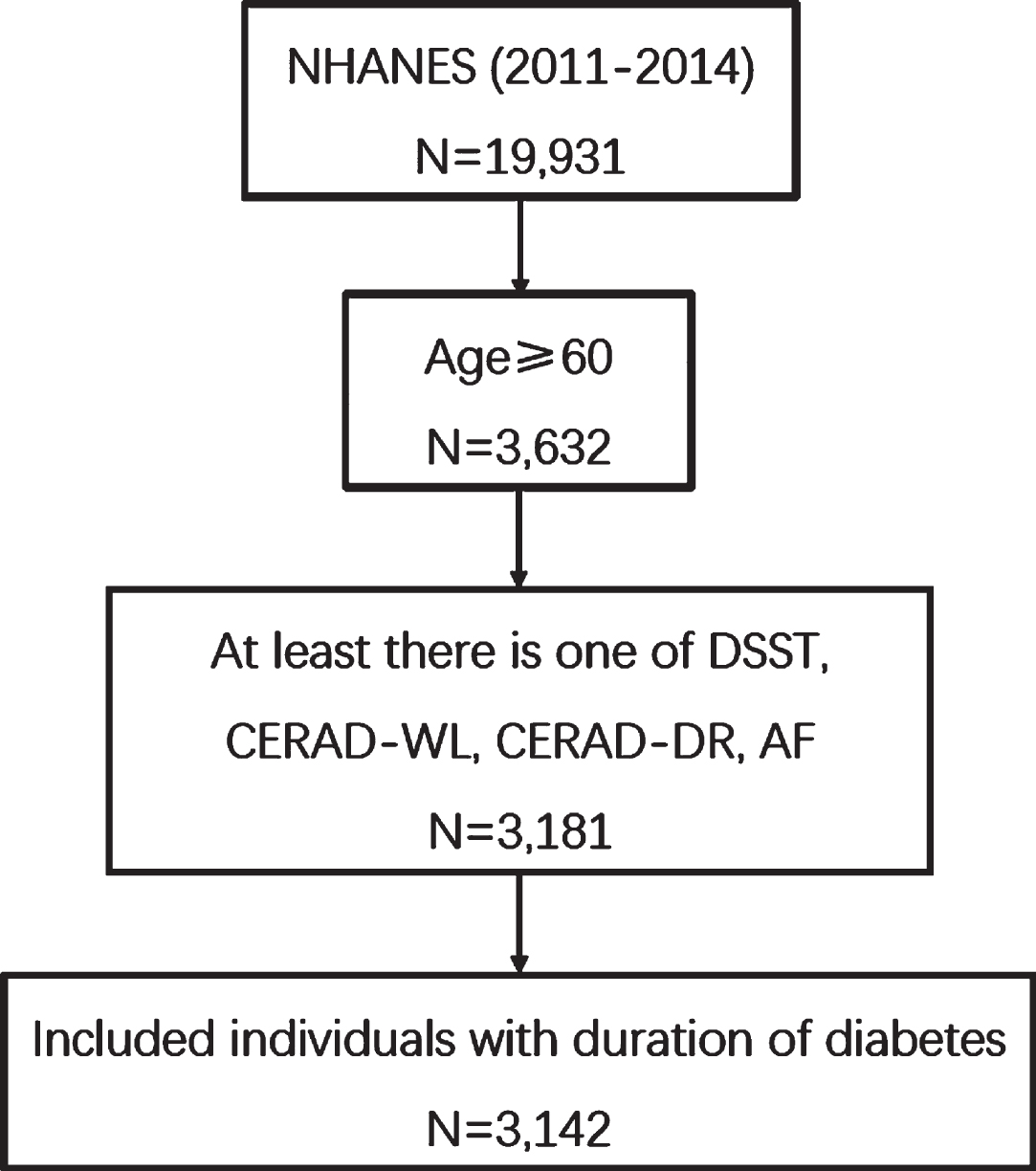
Participants selection for analysis between diabetes duration and cognitive impairment at survey (N = 3,142). DSST, Digit Symbol Substitution Test; CERAD-WL, Consortium to Establish a Registry for Alzheimer’s Disease Word Learning test; CERAD-DR, Consortium to Establish a Registry for Alzheimer’s Disease Delayed Recall test; AF, animal fluency test. NHANES, National Health and Nutrition Examination Survey.
The characteristics of the enrolled 3,142 participants are shown in Table 1. No statistically significant trends in participant number, sex, and smoking status were observed among the different diabetes duration groups (all p > 0.05). People with diabetes, especially those with a longer disease duration, had significant trend regarding age and color (p = 0.03, p < 0.001, respectively), and were found to have comorbid conditions. Participants without diabetes were more likely to have a higher annual household income (p < 0.001) and an advanced education level (p < 0.001). The different cognitive test scores decreased with longer disease duration across the diabetes groups (p < 0.001).
Criteria of participants according to duration of diabetes in 5-year increments of the NHANES study populations (N = 3,142)
CKD, chronic kidney disease; CVD, cardiovascular disease; DSST, Digit Symbol Substitution Test; CERAD-WL, CERAD Word Learning; CERAD-DR, CERAD Delayed Recall; AF, animal fluency.
Association between diabetes duration and cognitive performance
First, we examined domain-specific cognitive test scores with continuous variables expressed using mean values and standard error (SE). After adjusting for related variables, each 1-year increase in diabetes duration was associated with lower DSST scores (–0.17 score, 95% confidence interval [CI]: –0.28, –0.05), but no statistically significant association was found between CERAD-WL, CERAD-DR, and AF scores and diabetes duration (–0.03 score, 95% CI: –0.06 to 0.01; –0.01 score, 95% CI: –0.03, 0.001; and –0.03 score, 95% CI: –0.07 to 0.01, respectively) (Table 2).
Continuous cognitive scores according to duration of diabetes in all participants (N = 3,142)
Model 1 sequentially adjusted for SES (age, sex, race/ethnicity, education level, and annual household income). Model 2 sequentially adjusted for SES plus log albuminuria, body mass index, glycohemoglobin (%), conditions (smoking status, hypertension, chronic kidney disease or cardiovascular diseases). DSST, Digit Symbol Substitution Test; CERAD-WL, CERAD Word Learning; CERAD-DR, CERAD Delayed Recall; AF, animal fluency.
We then defined four types of cognitive impairment based on the four cognitive tests; scores below cut-offs for DSST, CERAD-WL test, CERAD-DR test, and AF test indicated information processing impairment, immediate recall impairment, delayed recall impairment, and executive function impairment, respectively. After adjusting for age, sex, race/ethnicity, education level, and annual household income in Model 1, the results showed that participants with diabetes duration ≥20 years had a 3.32-fold increased risk of information processing impairment (odds ratio [OR] = 3.32, 95% CI:1.95 to 5.67), a 1.72-fold increased risk of immediate recall impairment (OR = 1.72, 95% CI: 1.13 to 2.62), and 1.76-fold increased risk of executive function impairment (OR = 1.76, 95% CI: 1.23 to 2.53) compared to those without diabetes. Notably, these results were statistically significant. A longer diabetes duration was associated with a higher risk of information processing impairment (p value for trend = 0.0001), not immediate (p value for trend = 0.09) and delayed recall impairment (p value for trend = 0.94), and executive function (p value for trend = 0.12). Further adjustment for log albuminuria, BMI, glycohemoglobin (%), smoking status, hypertension, CKDs, or CVDs in Model 2 revealed a 2.07-fold increased risk of information processing impairment that was significant in people with diabetes ≥20 years (OR = 2.07, 95% CI: 1.34 to 3.20), compared to that in those without diabetes. Further analysis of continuous data in Model 1 showed that each 1-year increase in diabetes duration increased the risk of impaired information processing by 1.03- fold (95% CI: 1.00 to 1.06), impaired immediate recall by 1.02-fold (95% CI: 1.00 to 1.04), and impaired executive function by 1.02-fold (95% CI: 1.00 to 1.04). In all analyses, no significant relationship was found between longer diabetes duration and delayed recall impairment (Table 3). Thereafter, we performed the analyses exclusively in patients with diabetes. Compared to patients with diabetes duration of 1–4 years, those with diabetes duration ≥20 years had a 1.89-fold increased risk of impaired information processing (95% CI: 1.00 to 3.60) and 2.01-fold increased risk of impaired immediate recall (95% CI: 1.03 to 3.93) after adjusting for all covariables. Analysis of p value for trend showed that a longer diabetes duration was associated with a higher risk of information processing impairment (p value for trend = 0.01), not immediate (p value for trend = 0.24) and delayed recall impairment (p value for trend = 0.88), and executive function (p value for trend = 0.25) after adjusting full factors (Supplementary Table 1). The proportion of participants with cognitive impairment according to different diabetes duration groups is shown in Fig. 2.
Adjusted odd ratios (ORs) for presence of cognitive impairment according to duration of diabetes in all participants (N = 3,142)
The reference group is people with no diabetes. DSST, Digit Symbol Substitution Test; CERAD-WL, CERAD Word Learning; CERAD-DR, CERAD Delayed Recall; AF, animal fluency.
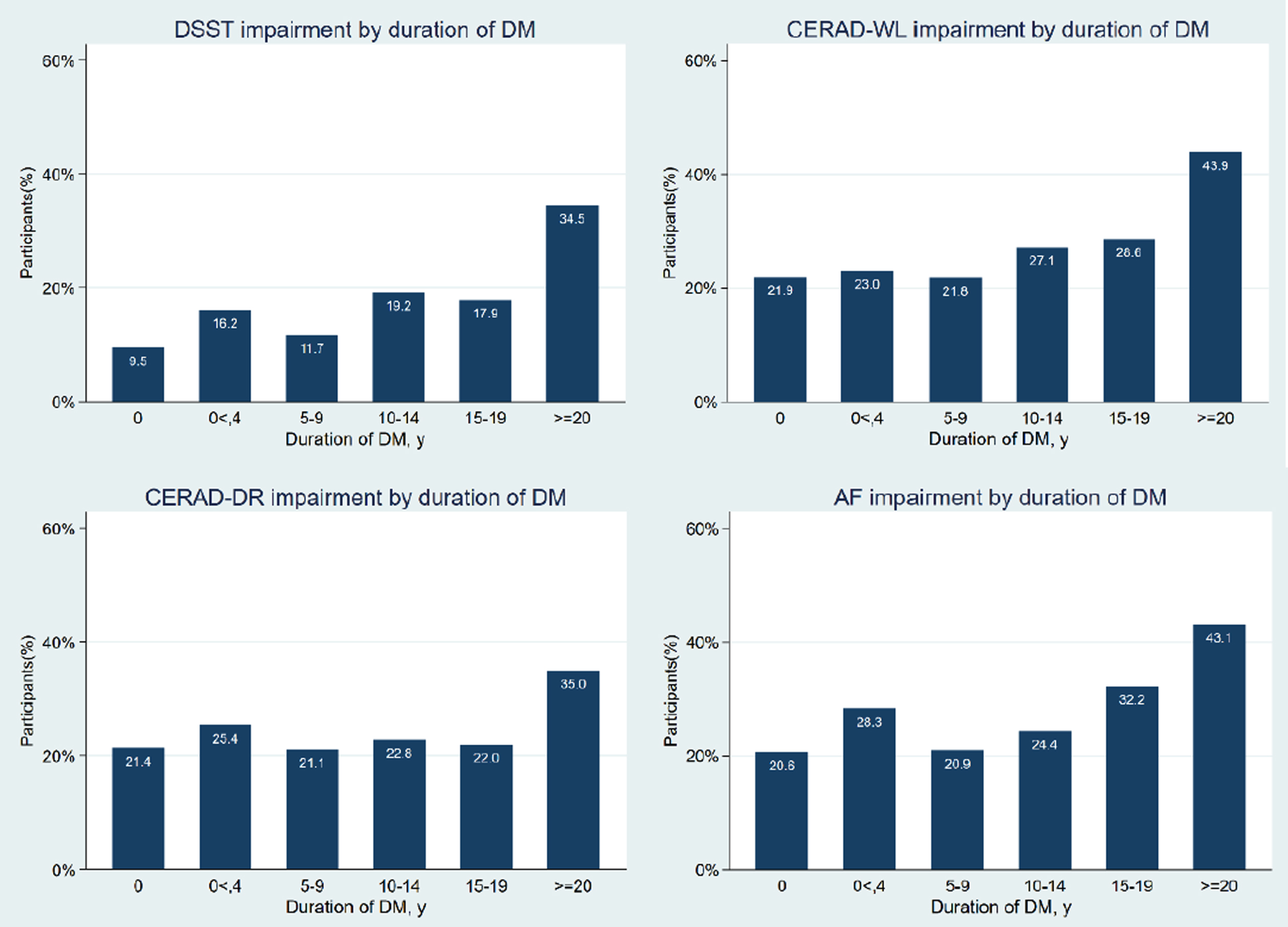
Cognitive impairment distribution according to duration of diabetes (N = 3,142).
Finally, we repeated the analysis by considering sex. After adjusting for covariables in model 1, in male participants, diabetes duration ≥20 years was associated with a 4.15-fold increased risk of information processing impairment (OR = 4.15, 95% CI: 1.66 to 10.38) but no significant increase in the risk of impaired immediate recall (OR = 1.63, 95% CI: 0.95 to 2.78), delayed recall (OR = 0.99, 95% CI: 0.54 to 1.79), or executive function (OR = 1.43, 95% CI: 0.78 to 2.60). In contrast, in female patients with diabetes duration ≥20 years, we found a 2.70-fold increase in risk of impaired information processing (OR = 2.70, 95% CI: 1.29 to 5.65), a 1.89-fold increase in risk of impaired immediate recall (OR = 1.89, 95% CI: 1.11 to 3.23), and a 2.16-fold increase in the risk of impaired executive function (OR = 2.16, 95% CI: 1.25 to 3.73), but no significant increase in the risk of impaired delayed recall (OR = 1.87, 95% CI: 0.99 to 3.52) (Supplementary Table 2).
Role of CVD and CKD in the association between diabetes and different cognitive impairment scores
CVD and CKD were also associated with an increased risk of cognitive impairment in the study participants. In Model 1, diabetics with CVD and CKD were at a significantly greater risk of impaired processing speed (OR = 4.73, 95% CI: 2.38 to 9.42) and executive function (OR = 2.09, 95% CI: 1.27 to 3.46) but not of impaired immediate recall (OR = 1.25, 95% CI: 0.69 to 2.25) or delayed recall (OR = 0.85, 95% CI: 0.45 to 1.63), compared with people with no diabetes. In the fully adjusted model, diabetics with CKD and those with CKD and CVD were at a higher risk of impaired information processing (diabetics with CKD: OR = 3.45, 95% CI: 1.34 to 8.89; diabetics with CVD and CKD: OR = 3.37, 95% CI: 1.52 to 7.48) than that of non-diabetics. No statistically significant results were found in the relationship between diabetes with CVD or CKD alone and immediate recall, delayed recall, and executive function impairment in any of the models (Table 4). Further, we conducted an analysis exclusively among diabetics, comparing those with CVD and/or CKD to those without these comorbidities, and obtained similar results (Supplementary Table 3)
Role of cardiovascular diseases and chronic kidney diseases in the association between diabetes and cognitive impairment in all participants (N = 3,142)
The reference group is people with no diabetes. CKD, chronic kidney disease; CVD, cardiovascular disease; DSST, Digit Symbol Substitution Test; CERAD-WL, CERAD Word Learning; CERAD-DR, CERAD Delayed Recall; AF, animal fluency.
Role of age at onset of diabetes in the association between diabetes duration and different cognitive impairment scores
To further understand the association between diabetes duration and cognitive impairment, we repeated the analysis among those with information on the age at onset of diabetes. We divided the participants (n = 894) into four groups according to their age at diabetes onset: 40–49, 50–59, 60–69, and ≥70 years. Participants with diabetes diagnosed at 40–49 years of age showed a statistically significant increase in the risk of impaired immediate recall (OR = 2.74, 95% CI: 1.09 to 6.87) and delayed recall (OR = 4.00, 95% CI: 1.29 to 12.39) per 5-year increase in diabetes duration, but not in the risk of information processing impairment (OR = 3.61, 95% CI: 0.77 to 16.91) or executive function impairment (OR = 2.74, 95% CI: 0.91 to 8.27). For those diagnosed with diabetes at 50–59 years of age, every 5-year increase in diabetes duration was associated with a significant increase in the risk of information processing (OR = 2.28, 95% CI: 1.38 to 3.77), immediate recall (OR = 1.81, 95% CI: 1.10 to 2.99), delayed recall (OR = 1.72, 95% CI: 1.01 to 2.94), and executive function (OR = 1.74, 95% CI: 1.09 to 2.77) impairment. Participants with diabetes diagnosed at 60–69 years of age had a 2.09-fold increased risk of impaired information processing (OR = 2.09, 95% CI: 1.46 to 3.00), 2.31-fold increased risk of impaired immediate recall (OR = 2.31, 95% CI: 1.72 to 3.10), and 1.48-fold increased risk of impaired delayed recall (OR = 1.48, 95% CI: 1.03 to 2.13) with every 5-year increase in diabetes duration. However, this trend was not observed in the association with executive function impairment (OR = 1.20, 95% CI: 0.91 to 1.60). Patients diagnosed with diabetes at ≥70 years of age had a 3.69-fold increased risk of information processing impairment (OR = 3.69, 95% CI: 1.11 to 12.25) with every 5-year increase in diabetes duration but showed no significant increase in the risk of immediate recall, delayed recall, and executive function impairment (Table 5).
ORs and 95% CI for cognitive impairment associated with 5-year increase in diabetes duration in people with prevalent diabetes stratified by age at diabetes diagnosis in all participants (N = 894)
Model sequentially adjusted for SES (sex, race/ethnicity, education level, and annual household income), log albuminuria, body mass index, glycohemoglobin (%), conditions (smoking status, hypertension, chronic kidney disease, or cardiovascular diseases). DSST, Digit Symbol Substitution Test; CERAD-WL, CERAD Word Learning; CERAD-DR, CERAD Delayed Recall; AF, animal fluency.
DISCUSSION
This study showed that people with a longer duration of diabetes were at a higher risk of cognitive decline, especially in terms of processing speed and attention, and the phenomenon was more obvious in women. The presence of CVD and/or CKD increased the risk of cognitive decline in patients with diabetes, with the effect being more statistically significant in patients with CKD. Further findings showed that the relationship between a longer diabetes duration and worse cognitive performance was more pronounced in participants with mid-life onset of diabetes than in those with late-life onset of diabetes.
Diabetes can increase the risk of pre-dementia states, including prodromal states of dementia such as mild cognitive impairment [44–48]. A prospective analysis of the Atherosclerosis Risk in Communities (ARIC) Study (2011–2013) showed that participants with a longer diabetes duration had a 1.59-fold increased risk of incident cognitive impairment (≥5 versus <5 years; HR 1.59 [95% CI 1.23, 2.07]) [32]. However, all these studies have assessed overall cognitive impairment and have not examined domain-specific cognitive performance [12]. In the present study, diabetes duration was significantly and adversely associated with processing speed and attention, thus indicating that diabetes duration may have a domain-specific impact. Similar to our findings, a meta-analysis of 26,137 participants with diabetes suggested that cognitive impairment relies on executive function, attention/concentration, visual memory, and verbal memory [49]. Altogether these findings suggest that the duration of diabetes could variably affect the brain domains involved in memory and cognitive impairment.
When the analysis was performed considering sex, we found that the association between diabetes duration and cognitive impairment was more pronounced in women than in men, which was consistent with a previous study’s findings [30]. Nevertheless, this result was not statistically significant after adjusting for comorbidities, such as CVD or CKD. Endocrine and behavioral factors could be involved in this finding; however, the underlying mechanisms remain to be elucidated.
Age at diagnosis and the duration of diabetes are closely interlinked. We further explored the impact of age at onset/diagnoses of diabetes on the association between diabetes duration and cognitive decline and found that diagnosis at mid-life showed more significant results than diagnosis later in life. Earlier studies have found a higher risk of dementia in mid-life onset diabetes than in late-life onset diabetes [14, 50]. Mid-life onset diabetes results in a longer disease duration. Interestingly, previous studies found that some risk factors change to beneficial ones from middle-age to older age [51]. In samples of older adults, some risk factors were rarely associated with poor cognition [52, 53] and were sometimes significantly associated with good cognition [54–57]. A possible explanation for this is that people with more risk factors at an early age have shorter survival times. Thus, genes of older individuals with long survival durations may be different from those of others, and this may be the direction for future exploration.
Potential mechanisms
The mechanism underlying the association between diabetes duration and cognitive decline is still not fully understood, and may be linked through several potential pathways [58]. This association may represent an aggregate of damage due to the diabetic milieu [59], as well as the concomitant insulin resistance that occurs in type 2 diabetes [60] and hypoglycemia in people using insulin therapy [61]. Longer diabetes duration increases the likelihood of prolonged exposure to hyperglycemia, which may lead to glucose toxicity and damage to both the parenchyma and vasculature of the brain [16, 62]. Long time exposure to chronic hyperglycemia is known to be linked to inflammation, oxidative stress [63], vascular damage [64, 65], and neurovascular dysfunction [66] which may directly impact cognitive performance. In addition, frequent hypoglycemic episodes are well-recognized risk factors for cognitive impairment [61]. It should be noted that hyperglycemia is associated with reduced gray matter density in posterior cingulate, superior temporal gyrus, and parahippocampal gyri, which are important cognitive areas [67]. In the current study, a longer duration of diabetes was associated with a higher risk of processing speed and attention but not memory. One possible explanation is that memory depends on hippocampal function [68], while information processing speed and attention depend on cortical function [69]. Previous studies have found that the pathobiology of hippocampal degeneration may be driven by amyloid-beta and tau accumulation [70] and that cortical dysfunction may be more strongly determined by vascular dysfunction [71]. Diabetes was proven to damage both micro-and macrovessels but had limited evidence of impact on amyloid-beta/tau accumulation [72, 73]. Finally, some other disorders caused by longstanding hyperglycemia, including endothelial dysfunction and abnormalities in fibrinogen and clotting mechanisms [74] may also contribute to the development of cognitive impairment.
Public health
With the increasing prevalence of diabetes in this aging society, prevention and early intervention of other age-related diseases are considered increasingly important, especially in individuals with diabetes as a risk factor [30]. Moreover, because of the obesity epidemic among young adults, the age at diabetes diagnosis has decreased recently [75, 76], and with improvements in diabetes care, individuals with diabetes are living longer and hence present a higher risk of cognitive decline. In this study, we found that a longer diabetes duration was associated with an increased risk of cognitive decline, and this relationship was especially pronounced in women. In addition, diabetes diagnosed at mid-life was associated with a higher risk of cognitive impairment than diabetes diagnosed in late life. Thus, the prevention of diabetes is particularly important in midlife. It should be noted that cognitive decline has a negative impact on the management of diabetes, including medication use, dietary arrangement, and blood glucose monitoring. In addition, patients with diabetes and cognitive decline have a higher risk of hypoglycemia and overall mortality [77, 78] which has a significant economic impact on healthcare systems. Our results suggest that women with longer diabetes duration and mid-life onset of disease should be particularly targeted for cognitive interventions. However, the means to mitigate the cognitive damage associated with diabetes duration remains a challenge, and further research focusing on mid-life onset diabetes and subsequent cognitive decline is needed.
Strengths and limitations
Our study has some strengths, such as the use of a national cohort. To the best of our knowledge, this study is the first to explore the combined effect of diabetes duration and age of disease onset on cognitive decline. However, the association between duration of diabetes and cognitive impairment is complex, and some limitations of this study should be acknowledged. First, owing to the cross-sectional design of this analysis, the findings were observational. A causative association between the duration of diabetes and different cognitive impairments cannot be established, and further longitudinal studies are needed. Second, some variables were self-reported, including age at diabetes diagnosis, thus making it difficult to avoid a related bias. Third, some other factors, such as pharmacotherapy (especially insulin and metformin) [79, 80], diabetic complications (including diabetic retinopathy [81–83] and diabetic nephropathy [84, 85]), long-time glucose fluctuation [79, 86], and the duration of CKD and CVD, may confound the association between diabetes duration and cognitive impairment. Unfortunately, no related data were provided by the NHANES. Finally, in the current analysis, it was difficult to distinguish older adults with preexisting mental health conditions.
Conclusion
In summary, a longer diabetes duration increased the risk of cognitive decline, especially processing speed and attention, but did not affect delayed memory. In addition, this association was more pronounced in female patients with diabetes, those with mid-life onset diabetes, and those with concomitant CKD. However, the cross-sectional design of this study limits the scope of the results, and a longitudinal study is needed to validate our findings.
Footnotes
ACKNOWLEDGMENTS
The authors thank the staff in this study for their indispensable contribution.
FUNDING
This work was supported by the National Natural Science Foundation of China (No. 82070851), Beijing Municipal Administration of Hospital’s Youth Program (QML20170204), and Excellent Talents in Dongcheng District of Beijing.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Data from the National Health and Nutritional Examination Survey are available online through the US Centers for Disease Control and Prevention.