
Abstract
Background:
The Maintain Your Brain (MYB) trial aims to prevent cognitive decline and dementia through multidomain, web-based risk-reduction. To facilitate translation, it is important to understand drivers of participation.
Objective:
To describe characteristics associated with participation in MYB.
Methods:
This was an observational ancillary study of MYB, a randomized controlled trial nested within the 45 and Up Study in New South Wales, Australia. We linked 45 and Up Study survey and MYB participation data. The study cohort comprised 45 and Up Study participants, aged 55–77 years at 1 January 2018, who were invited to participate in MYB. 45 and Up Study participant characteristics and subsequent MYB consent and participation were examined.
Results:
Of 98,836 invited, 13,882 (14%) consented to participate and 6,190 participated (6%). Adjusting for age and sex, a wide range of factors were related to participation. Higher educational attainment had the strongest relationship with increased MYB participation (university versus school non-completion; AdjOR = 5.15; 95% CI:4.70–5.64) and lower self-rated quality of life with reduced participation (Poor versus Excellent: AdjOR = 0.19; 95% CI:0.11–0.32). A family history of Alzheimer’s disease was related to increased participation but most other dementia risk factors such as diabetes, obesity, stroke, high blood pressure, and current smoking were associated with reduced participation.
Conclusion:
Higher socio-economic status, particularly educational attainment, is strongly associated with engagement in online dementia prevention research. Increasing population awareness of dementia risk factors, and better understanding the participation barriers in at-risk groups, is necessary to ensure online interventions are optimally designed to promote maximum participation.
Keywords
INTRODUCTION
Up to 40% of dementia cases globally may be attributable to modifiable risk factors [1]. There is potential to prevent or delay cognitive decline and dementia through behavior modification interventions that reduce dementia risk. Trials such as the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) have shown some efficacy in improving cognition and dementia risk through multi-modal behavioral interventions [2]. However, participants who choose to participate in such intensive trials may be a select group who are highly motivated to embrace change and not representative of the underlying target population [3, 4]. Coley et al. [4] noted that “those most at risk of dementia may not participate in or adhere to preventive interventions” potentially diluting the effect of such interventions.
Maintain Your Brain (MYB) [5] is a randomized controlled trial of multiple interventions designed to target modifiable risk factors for dementia. The four main modules target physical inactivity, poor diet, depression and anxiety, and low cognitive activity. A unique aspect of MYB is that all interventions were delivered online, making it potentially accessible to a wide range of participants, resilient to the wide-scale social impacts from COVID-19, and of high scalability. As internet-based interventions are not reliant on travel to study centers, they can reduce barriers to participation such as poor mobility or lack of access to transport and allow greater participation from non-metropolitan areas [6]. However, they also have certain minimum technological requirements, both in terms of access and skill level, which can create a digital divide—appealing more to younger people and those in higher socio-economic groups [7].
MYB is nested within the Sax Institute’s 45 and Up Study, an observational cohort of 267,357 voluntary participants aged 45 years or older in New South Wales, Australia [8]. This study design provides a unique opportunity to examine in detail the characteristics of both participants and non-participants across a wide range of socio-demographic and health-related factors. This will provide the most in-depth analysis to date of the extent of participation bias within a dementia prevention trial.
Participant characteristics were considered against a version of the Anderson behavioral model of health service use [9], adapted to incorporate aspects of the health behavior model [10] (Fig. 1). These two models have frequently been used to understand the drivers of engagement with health services [11] and preventive health behaviors [12] respectively, with the latter also used as a framework for designing preventive interventions [13]. Factors that may potentially influence participation were categorized as predisposing, enabling, and need-related. Need was considered in terms of measured need for the intervention (based on presence of dementia risk factors). In the context of dementia, it is uncertain whether measured need will be a driver of preventive health behaviors. Lack of knowledge of dementia risk factors has been identified as a barrier for behavioral change [14, 15] and many older Australians do not believe that dementia risk can be reduced [16] although knowledge in this area may be increasing over time [17].
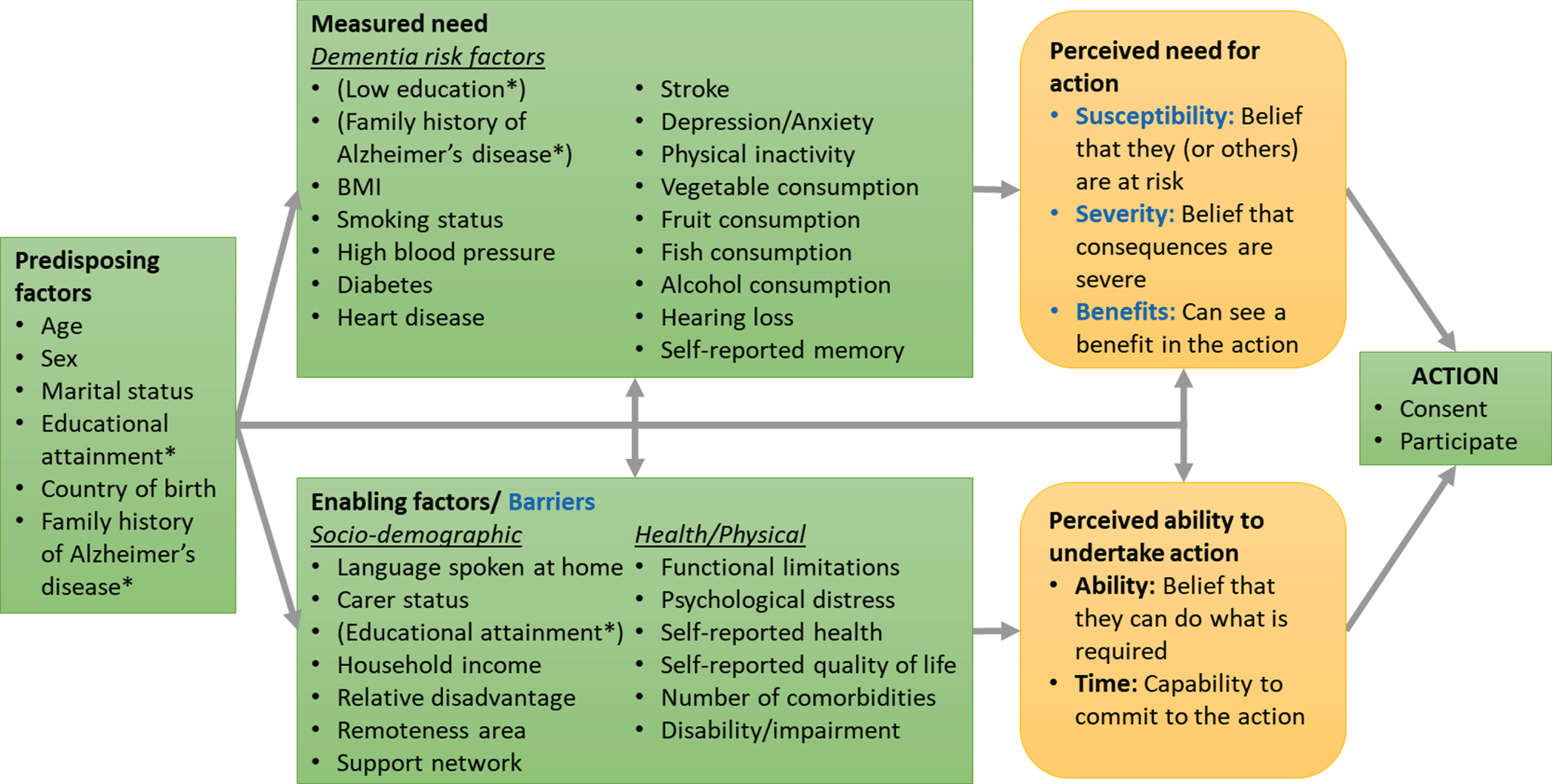
Factors that may influence participation in a dementia prevention study. Darker colored boxes in green denote factors that are measured in the current study aligned with the Anderson model of health service utilization [9]; Lighter colored boxes in yellow propose unmeasured mediating factors; Barriers, Susceptibility, Severity and Benefits are highlighted to denote key categories of the Health Belief Model [10]; *Educational attainment and a family history of Alzheimer’s disease are included as both predisposing and need factors as they are likely to influence attitudes and opinions regarding dementia as well as elevate risk of dementia for an individual. Educational attainment may also be an enabler of action in terms of increasing overall health literacy.
The current study aims to 1) systematically explore the characteristics associated with participation in the MYB trial and 2) identify the extent to which participation bias exists. It is postulated that participation within the MYB trial will be influenced by predisposing and enabling factors. It is anticipated that this will bias the MYB participant group towards those who have higher education and economic resources and fewer physical limitations and comorbidities.
METHODS
Setting and design
MYB is a randomized controlled trial nested within the Sax Institute’s 45 and Up Study, a prospective cohort study in New South Wales (NSW), Australia. Recruitment to the 45 and Up Study was through selection from the Services Australia Medicare enrolment database using stratified random sampling based on age and geography. This database provides near complete coverage of the population [8]. People aged 80 years and over and residents of non-metropolitan areas were oversampled. A total of 267,357 participants joined the 45 and Up Study by completing a baseline questionnaire between 2005 and 2009 and providing written informed consent for future follow-up surveys and linkage of their information to routine health databases [18]. Baseline questionnaires were only provided in English, requiring a reasonable level of English proficiency. About 19% of those invited participated, and participants included about 11% of the NSW population aged 45 years and over. The 45 and Up baseline cohort was slightly healthier and more educated than the broader NSW population [8, 19].
Data linkage
MYB participation data was linked back to the 45 and Up Study Wave 1 (baseline: 2005–2009) and Wave 3 (2018–2020) surveys by the Sax Institute using uniquely assigned identifiers. During this process, names were cross-checked to ensure consistency of linkage before the Sax provided de-identified linked data.
The study cohort
Participants of the 45 and Up Study were invited to MYB if they were alive and aged between 55 and 77 years at 1 Jan 2018, had agreed to be contacted about further studies, did not have dementia, Parkinson’s disease, or multiple sclerosis (based on available 45 and Up Study records) and did not participate in any previous MYB validation or pilot studies.
Intervention
Participants were sent either an email (if email address was available) or physical mail invitation between June 2018 and October 2018 describing the MYB trial and inviting them to participate. Participants were given a unique registration link to log on to a secure website and provide informed consent for the MYB trial including data linkage. Participants with mailed invitations needed to enter an email address and their identifying code to receive the registration link. Registration links expired on October 9, 2018, when enrolment closed. Participants who consented were invited to complete baseline screening questions and computer-based cognitive performance testing comprising validated modules from CogState [20, 21] and Cambridge Brain Sciences [22]. At least one reminder email was sent for those who consented. Those who completed all baseline data collection and satisfied eligibility requirements were randomized for participation in the trial. People with acute health issues or who lacked access to the internet and a computer were excluded. The information provided to invitees advised that the MYB trial aimed to evaluate the impact of a tailored online health program on memory and thinking skills. The information brochure also outlined that they would be randomised to either an information or coaching group and that in the first year they would be asked to complete up to 4 online information-based or coaching modules of 3 months each based on their health profile. Participants would then receive less frequent activities in years 2 and 3 of the study and be asked to complete yearly follow-up surveys. See the Supplementary Material 1 for further information on the invitation and eligibility criteria.
Outcome measures
Two binary outcome measures were assessed in this study: Consent to participate; and participation in the MYB trial (indicated by randomization after completion of a baseline assessment).
Predictor variables
Participant characteristics were examined using self-reported data from the baseline survey collected at enrolment to the 45 and Up Study. Factors investigated were mapped to the modified Anderson model as indicated in Fig. 1. More detailed variable descriptions are provided in Supplementary Material 2.
Statistical analyses
The main analysis examined the relationship between predictor variables and MYB participation among all invited. As participation required two steps, secondary analyses examined each step separately: consent to participate among all invited and participation (i.e., completing baseline assessment and being randomized) among all who consented. Descriptive analyses firstly examined means and proportions by outcome group for continuous and categorical variables respectively. Age- and sex-adjusted logistic regression models were used to estimate adjusted odds ratios (ORs) to assess the relationship between each covariate and the outcomes.
Three sensitivity tests were also conducted. The first examined the independence of the relationships between predictors and outcomes using fully adjusted logistic models. MYB participation among the invited group was run as a backwards stepwise logistic model removing covariates based on change in the Akaike Information Criterion. Categorical variables were also removed if the “not available” category was the only category remaining which had a significant relationship with the outcome. The secondary models, (consent among all invited, and participation among all who consented) included the same reduced set of predictors.
The second sensitivity test restricted the analysis to only those participants who completed the 45 and Up Study 2018–2020 Wave 3 follow-up survey. This ensured focus on a group who were demonstrably still contactable, and amenable to research participation in general, within the time-period relevant to MYB participation.
The third test restricted this Wave 3 cohort further to include only those people who completed a follow-up survey in 2018 and used the more recent Wave 3 survey data for participant characteristics to ensure these variables were measured in the same time period as MYB recruitment. 2018 data were available for all predictor variables except age, sex, educational attainment, country of birth and language spoken at home which were only collected in the baseline survey. All variable definitions were the same as for the baseline survey (see Supplementary Material 2).
Finally, to assess the extent of participation bias in the MYB sample, we benchmarked selected characteristics of the sample against the Australian National Health Survey (NHS) weighted to be representative of the Australian population. Selected key characteristics that were collected using comparable questions across the NHS and 45 and Up Study were identified. Participants aged 45–69 years in the 2007/8 NHS survey were selected to provide the closest match to the timeframe and age range of the MYB participants when they answered the 45 and Up Study baseline survey. Proportions of participants with the selected characteristics were compared for 1) the final MYB sample, 2) the invited MYB cohort, 3) 45–69-year-old respondents to the 2007/08 NHS. NHS estimates were produced from the Australian Bureau of Statistics NHS 2007/8 Basic Confidentialized Unit Record File [23]. Differences were compared using chi-square tests and ANOVA as appropriate.
Data management used SAS version 9.4 (Cary Institute, NY) and data analysis used R version 4.03.
Ethical approval
This study was conducted in accordance with the Australian National Health and Medical Research Council’s National Statement on Ethical Conduct in Human Research [24]. Sub-studies of the 45 and Up Study such as MYB require additional ethical approval and consent and invitations are coordinated by the Sax Institute. Approval for the 45 and Up Study was granted by the University of New South Wales Human Research Ethics committee (HC 15408) and for the MYB trial by the University of New South Wales Human Research (HC 16252) and NSW Population and Health Services research ethics committees (2016/03/636).
RESULTS
A total of 99,018 participants from the 45 and Up Study aged between 55–77 years on 1 January 2018 were invited to participate in the MYB trial. Twenty people withdrew from the 45 and Up Study after being invited to participate in MYB (June-October 2018) but prior to linkage of 45 and Up Study and MYB data collection (December 2021). A further 162 MYB participants who could not be matched to 45 and Up Study participants based on provided details were excluded from the current analysis to ensure accurate linkage with the 45 and Up Study, leaving 98,836 in scope for this ancillary study—and referred in this paper as the invited group. Among the invited group, 13,882 (14%) consented to participate in MYB and 6,190 people (6%) were randomized. Figure 2 shows the participant flow from invitation to participation. Of those who consented, 5,990 were excluded because they did not complete screening or baseline data collection, 1,239 were ineligible because they met at least one exclusion criterion (see Supplementary Material 1 for further details), and 442 withdrew their consent prior to randomization (they were not asked for reasons for withdrawal). A further 21 participants completed all screening and baseline data collection but were not eligible for any of the modules due to an absence of investigated risk factors and so were also excluded.
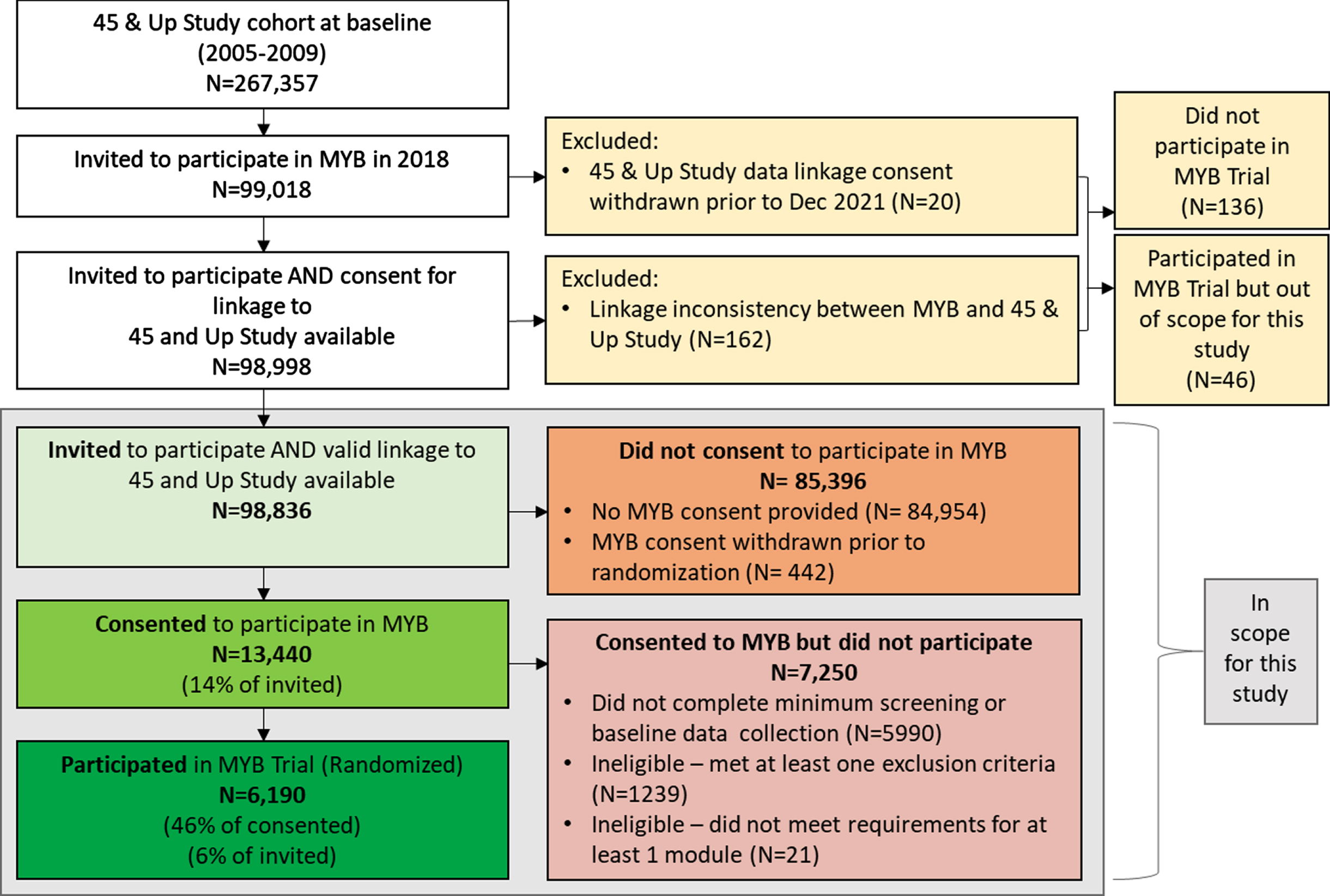
MYB Participant flow-chart. The final MYB participant group in the current study was 6,190 compared to 6236 randomized in the MYB trial - a difference of 46 people due to the extra exclusions highlighted in yellow that were required for linking back to the 45 and Up Study.
MYB participants had a mean age of 64.9 years and 63.6% were female, making them younger and more likely to be female compared to people who consented but did not participate (65.2 years, 57.6% female) and people who did not consent (66.1 years, 57.3% female) (Table 1).
Baseline characteristics in the 45 and Up Study and subsequent MYB participation
SD, standard deviation; k10, Kessler10 scale of psychological distress; SF36, Short Form 36 –physical functioning scale; BMI, body mass index; DSSI, Duke Social Support Index; Bold text indicate significant at p < 0.05. Due to rounding error, summing percentages across categories may not exactly equal 100.
Table 2 shows age and sex adjusted ORs for: (A) participation among the invited group; (B) consent among the invited group; and (C) participation among all who consented. Participation within the invited group was positively associated with: being married or having a partner (compared to being single) (AdjOR = 1.27, 95% CI:1.13–1.43), higher education (university degree versus <year 12, AdjOR = 5.15, 95% CI:4.70–5.64) and being born in English-speaking countries other than Australia (UK/USA/NZ/Canada versus Australia, AdjOR = 1.41, 95% CI:1.32–1.52). Higher household income ($70,000+ versus < $20,000, AdjOR = 4.61, 95% CI:4.02–5.28) and living in areas of lower disadvantage (quintile of least disadvantage versus most, AdjOR = 2.26, 95% CI:2.06–2.47) or major cities (major cities versus outer regional/remote/very remote, AdjOR = 1.51, 95% CI:1.37–1.66) were all associated with higher participation. The only dementia risk factors positively associated with participation were having a family history of Alzheimer’s disease (AdjOR = 1.23, 95% CI:1.15–1.31) and having low vegetable consumption (AdjOR = 1.19, 95% CI:1.12–1.26). Alcohol consumption also had a positive curvilinear relationship with participation. Compared to non-drinkers, relative participation peaked among moderately high drinkers (8–13 drinks per week compared to zero: AdjOR = 1.71, 95% CI:1.58–1.86) and dropped slightly for very high drinkers (>14 drinks per week compared to zero: AdjOR = 1.54, 95% CI:1.41–1.69).
The relationship between baseline characteristics in the 45 and Up Study and (A) MYB participation among all MYB invitees, (B) MYB consent among all MYB invitees and (C) MYB participation among all MYB consenters
AdjOR, Adjusted Odds Ratio; Age was adjusted for sex and sex was adjusted for age, all other variables adjusted for both age and sex; SD, standard deviation; k10, Kessler10 scale of psychological distress; SF36, Short Form 36 –physical functioning scale; BMI, body mass index; DSSI, Duke Social Support Index; Bold text indicate significant at p < 0.05. Not available or missing data categories were included in the models, but Adj ORs are not presented for these categories.
Potential barriers associated with reduced participation included: regularly caring for a sick or disabled family member or friend (AdjOR = 0.77, 95% CI:0.71–0.84); speaking a language other than English at home (AdjOR = 0.67, 95% CI:0.60–0.75); having physical limitations (severe versus no limitations, Adj OR = 0.32, 95% CI:0.27–0.38); higher psychological distress (very high distress versus low, AdjOR = 0.41, 95% CI:0.31–0.55); poorer self-reported general health (poor versus excellent, AdjOR = 0.24, 95% CI:0.15–0.37); and poorer self-reported quality of life (poor versus excellent, AdjOR = 0.19, 95% CI:0.11–0.32). Higher social interaction was related to slightly increased participation when adjusting for age and sex (high interaction versus low interaction: AdjOR = 1.06 (1.00–1.13).
The following dementia risk factors were also associated with reduced likelihood of participation: underweight (AdjOR = 0.53, 95% CI:0.47–0.60), overweight (AdjOR = 0.76, 95% CI:0.72–0.81), or obese (AdjOR = 0.81, 95% CI:0.77–0.86) (compared with healthy weight), history of diabetes (AdjOR = 0.43; 95% CI:0.36–0.51), stroke (AdjOR = 0.52; 95% CI:0.37–0.73), heart disease (AdjOR = 0.85; 95% CI:0.75–0.95), high blood pressure (AdjOR = 0.75; 95% CI:0.70–0.79), depression or anxiety (AdjOR = 0.91; 95% CI:0.85–0.98), poorer self-rated memory (poor versus excellent, AdjOR = 0.50; 95% CI:0.37–0.66), insufficient physical activity (AdjOR = 0.76; 95% CI:0.72–0.81), current smoking (AdjOR = 0.43; 95% CI:0.37–0.50), and low fruit consumption (AdjOR = 0.86; 95% CI:0.81–0.90).
Table 2 shows that the covariates with significant relationships with participation (column A) in most instances had a relationship with both the decision to consent (column B) and subsequent participation once consent had been given (column C). In general, the relationships between predictors with consent were slightly stronger than with participation once consent was given, indicated by ORs further from 1. Exceptions to this pattern included sex and marital status where the effect size was larger for participation compared to consent.
After additionally controlling for all other factors, 19 factors remained as independently predictive of participation (Supplementary Material 3, Supplementary Table 3.1). These included lower age, being female, being born overseas in an English-speaking country, higher educational attainment, higher income, speaking a language other than English at home, living in an area of lower disadvantage or metropolitan location, reporting fewer physical limitations and better quality of life, having fewer social interactions, not reporting caring responsibilities, having a family history of Alzheimer’s disease, being a healthy weight, non-smoker (compared to current smoker), not having high blood pressure or diabetes. In addition, when controlling for all other factors, being an ex-smoker was associated with increased participation compared to non-smokers and self-reported hearing loss was associated with higher participation compared to those not reporting hearing loss. Self-reported memory had a non-linear relationship with participation with those with good and fair memory being most likely to participate (compared to both excellent and poor).
When restricting the cohort to people who responded to the 45 and Up Study Wave 3 follow-up survey (conducted between 2018–2020, which was 0–2 years after MYB baseline), all relationships between predictors and participation followed the patterns in Table 2 and remained significant, although with a slight reduction in strength of relationships (Supplementary Material 3, Supplementary Table 3.2). The only exception was anxiety/depression which became non-significant (AdjOR = 0.96; 95% CI:0.89–1.03).
The third sensitivity test used 45 and Up Study Wave 3 data for participant characteristics in place of baseline data (2006–2009) for 12,863 participants who responded to the Wave 3 survey in 2018. The pattern of relationships between participant characteristics and MYB participation remained consistent with the primary results in Table 2, with some small differences in size of effect and some relationships, while similar in effect, were non-significant in this smaller sample (see Supplementary Table 3.3).
Figure 3 shows that compared to the Australian population, the proportion with a university degree was higher within the MYB invited group and higher again within the MYB participant group (18.9% versus 31.8% and 54.6% respectively). A similar pattern was observed for proportion with a spouse/partner (71.2%, 79.6%, 81.9%), and English spoken at home (90.7%, 93.1%, 95.1%). Conversely the pattern was opposite for the proportion with obesity (Australia: 24.0%, MYB invited: 21.1%, MYB participants: 14.6%), fair or poor self-reported health (18.7%, 8.5%, 3.9%), and high or very high psychological distress (12.6%, 6.4%, 4.5%). While MYB participants were more likely to live in major cities than the invited MYB group, both groups had lower proportions living in major cities compared to the Australian population (Australia: 65.1%, MYB invited: 51.2%, MYB participants: 58.0%).
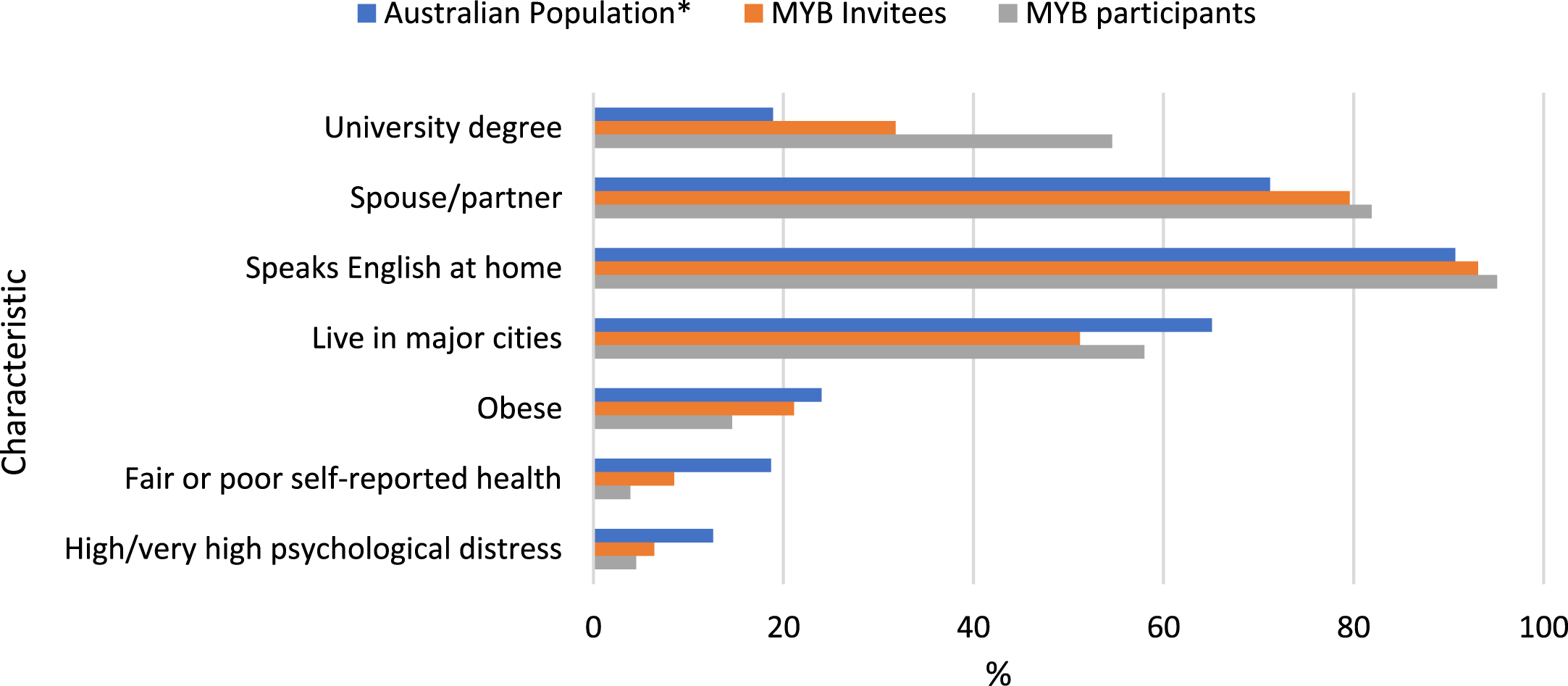
Comparison of MYB participants to the invited cohort and Australian population, by selected characteristics. To be comparable with the information available from the 45 and Up Study baseline survey collected in 2006–2008, estimates are taken from the 2007/8 National Health Survey for the 45–69-year age group as this group provides the closest match to the target MYB age group in 2018.
DISCUSSION
The final MYB sample size of over 6,000 is one of the largest globally recruited to a dementia prevention trial. However, MYB consent (14%) and participation (6%) rates were lower than the 48% of FINGER invitees who attended screening and 23% of invitees who participated [25]. Other studies such as the Multidomain Alzheimer Preventive Trial (MAPT) and the Prevention of Dementia by Intensive Vascular Care (pre-DIVA) trial also had higher participation rates [26, 27]. These studies all had very different recruitment strategies, including in-person contact with participants. The lower participation rate of 6% within MYB was the same as that found in the Healthy Ageing Through Internet Counselling in the Elderly (HATICE) trial [28]. HATICE and MYB were both internet-based pragmatic trials with broad eligibility and reasonably passive contact strategy, relying on communication by either email or mail to invite participants to the study. MYB consent and participation rates also appear comparable to studies such as the Australian Study for the Prevention through Immunization of Cardiovascular Events which used a similar contact strategy [29].
Nearly all hypothesized predisposing and enabling factors were significantly related to the likelihood of participating in the MYB trial. Socio-economic factors appeared to have a particularly strong link: university graduates had more than five times the odds of participating compared to early school leavers and participation increased linearly with increasing income. The initial invitation sent to participants regarding MYB provided very little information explaining the lifestyle risks for dementia as this would become part of the trial intervention. Higher education can pre-dispose a person to have an overall higher level of health literacy [30], and so university graduates may have seen greater value in a preventive trial both personally and in general [31].
Measured need was not a clear driver of participation. Except for having a family history of Alzheimer’s disease, low vegetable intake, and alcohol consumption which were positively associated with participation, nearly all dementia risk factors investigated were inversely related to participation—that is, those who were potentially at highest risk of dementia (and most in need of the intervention) were less likely to take part in the trial.
While we were able to assess measured need in terms of dementia risk factors, we could not assess a person’s perception of need which is likely to be the more influential driver of action and requires further study. From other research we know that population level knowledge of dementia risk is poor [16, 31]. However, it is likely that people with a first-hand knowledge of dementia such as those with a family history of Alzheimer’s disease will be more aware of dementia risk which, as we found, may make them more motivated to participate in a trial like MYB [32]. Low vegetable intake was very common in the 45 and Up Study cohort and it is possible participants with high health literacy and low vegetable intake were aware that an improved diet could assist healthy ageing, motivating their participation. However, vegetable intake did not remain a significant predictor when controlling for all other factors, suggesting this relationship is complex. Non-drinking or reduced drinking can be associated with the onset of health issues that could interfere with participation [33].
When controlling for all other factors, there were some indications that risk factors such as self-rated hearing loss and poorer memory may have been a positive motivator for participation, but these require further investigation. Being an ex-smoker was also associated with increased participation in the fully adjusted models and may signal an intention to adopt a healthier lifestyle. In the fully adjusted models, lower social interaction score was also associated with higher participation, possibly demonstrating the appeal of online interventions among people without existing networks [34].
Other risk factors may pose more of a barrier to participation rather than any incentive. For example, obesity has been found to be a barrier to cancer screening [35] and has been associated with avoidance of preventive health care in general [36]. Obese people can feel stigmatized about their weight and avoid situations where weight may be a focus [37]. Stigma has also been associated as a barrier to accessing healthcare for other risk factors such as current smoking [38] and depression or anxiety [39].
Reporting a lower health-related quality of life due to physical limitations (as measured within the 45 and Up Study using the SF-36 physical function sub-scale [40]) was associated with a much lower likelihood of participating in MYB and highlights the difficulty of engaging people with perceived physical limitations in health promotion activities. The Groningen Intervention Study on Successful Aging (GISSA) similarly found participants reported fewer perceived physical limitations compared to non-participants [41] and de Souto Barreto et al. observed that participants in their exercise study had less physical function decline and reported higher volumes of physical activity than non-participants [42].
Participation in the MYB trial also decreased with age, aligning with findings from other dementia prevention studies [4, 25] as well as internet-based interventions in general [43]. Older people may experience more barriers in using the necessary technology such as an increase in visual impairment and low computer literacy [7]. Some studies have also found that some older people tend to think dementia is a more normal part of aging, potentially lowering their perception of benefit from a trial such as MYB [44].
The intervention in MYB did not include medical monitoring and optimization of metabolic and vascular disorders associated with dementia risk as included in other studies [2, 45]. The absence of this aspect is likely to facilitate the study scalability, but also may make the intervention less appealing for older adults with prevalent chronic conditions, which are often not well managed from pharmacological and non-pharmacological points of view.
MYB participants were more likely to be female, contrasting with findings from MAPT [4] but in line with other studies [46, 47]. There are some quite distinct differences between this MYB participation study and the ancillary study assessing participation in MAPT. MAPT was more focused on vascular risk which may be skewed towards males, and for the MAPT ancillary study, participants and non-participants were surveyed following in-person screening for eligibility, whereas a much broader cohort of invitees was considered within MYB.
Overall, when examining key characteristics of the MYB participant group, the MYB trial is biased towards a more highly educated and healthier cohort compared to the Australian population in general. This appears to be due to processes that have occurred at several points: self-selection into the 45 and Up Study has likely resulted in a slightly healthier and more educated sample [8] from which the invitations to MYB were issued; the propensity to consent to the MYB trial then also narrowed this cohort; and finally, the process of meeting inclusion criteria and completing all baseline assessments appears to have narrowed the final MYB sample further.
The baseline cognitive testing required a reasonably large time investment over two separate sessions 24 h apart (20–30 min per session), and some participants could potentially have encountered fatigue or technical issues at this point. While remote technical support was available, there were some observed issues such as incompatibility of the MYB system with mobile devices that may have provided insurmountable barriers for some participants. Further qualitative research is underway to better understand other issues encountered and improve the online delivery system.
Because the initial 45 and Up Study over-sampled people from non-metropolitan areas [8], the MYB sample is slightly over-representative of non-metropolitan areas compared to national population distributions despite this group having a lower participation rate.
As the MYB trial was testing a randomized intervention, these selection biases are not likely to lead to biased results for the main trial outcomes but are important to understand for several reasons related to external validity or generalization. Firstly, they provide context for examining the magnitude of any trial effect; testing an intervention in a cohort with lower dementia risk could potentially lessen the impact of the intervention. Secondly, they will inform any wider-scale translation of the intervention should it be effective. Given there are clear sub-groups under-represented in the MYB trial compared to national estimates, such as people with lower education or increased physical limitations, there are challenges ahead in developing better engagement strategies for these groups. Finally, the lack of representativeness also affects the generalisability of the findings to the whole population. Sub-group analysis of MYB trial results may be useful to understand whether any differential effects exist and aid in evaluating the generalisability of findings.
One of the main strengths of this study is that a very wide range of socio-demographic and health-related information was available for a large cohort of people invited to participate in MYB. This is the only dementia prevention trial that we are aware of that has such detailed information on all non-participants. While the 45 and Up Study baseline survey preceded recruitment to MYB by a period of approximately 10 years, we were able to repeat the analyses on a subset of the cohort using 2018 survey data for participant characteristics and the pattern of relationships remained.
As this study relied on data collected separately and prior to MYB, it was not possible to explore new concepts such as perceived need for dementia risk reduction, or motivation/intention to change, that would have added additional depth to the current analysis. There were also no questions within the 45 and Up Study baseline survey or 2018 Wave 3 survey that captured confidence in technology use that was likely have been a relevant enabler or barrier to MYB participation given it was an online trial.
Conclusions
Higher socio-economic status, particularly educational attainment, is a major factor predisposing or enabling people to engage in online dementia prevention. Increasing awareness of dementia risk factors and benefits of risk reduction in the population is necessary to promote uptake of dementia prevention interventions among sub-groups most at risk. Further research is required to better understand participation among these groups and ensure online interventions are designed in ways to encourage maximum access and participation.
FUNDING
The Maintain Your Brain Trial was supported by a NHMRC program grant (Grant#1095097)
KJA is funded by ARC Laureate Fellowship FL190100011.
CONFLICT OF INTEREST
MV is co-founder and has a financial interest in Skin2Neuron Pty Ltd, with no relevance to this work. HB is or has been an advisory board member or consultant to Biogen, Eisai, Nutricia, Roche and Skin2Neuron. He is a Medical/Clinical Advisory Board member for Montefiore Homes and Cranbrook Care. NL received support from Lundbeck for investigator-initiated research. She is a board member for the Melbourne Academic Centre for Health.
DATA AVAILABILITY
45 and Up Study data for approved projects are available through application to the Sax Institute. Details are available at https://www.saxinstitute.org.au/our-work/45-up-study/ or through contacting 45andUp.research@saxinstitute.org.au.
Footnotes
ACKNOWLEDGMENTS
This research was completed using data collected through the 45 and Up Study (![]() ). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW; and partners: the Heart Foundation; NSW Ministry of Health; and Australian Red Cross Lifeblood. We thank the many thousands of people participating in the 45 and Up Study. The linked data was managed and accessed through the Sax Institute’s Secure Unified Research Environment (SURE).
). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW; and partners: the Heart Foundation; NSW Ministry of Health; and Australian Red Cross Lifeblood. We thank the many thousands of people participating in the 45 and Up Study. The linked data was managed and accessed through the Sax Institute’s Secure Unified Research Environment (SURE).