
Abstract
Background:
Evidence from predominately non-Hispanic White populations indicates that emergency room (ER) admissions and hospitalizations by older adults with and without dementia are associated with caregiver stress and depressive symptoms. These results may not generalize to Hispanic populations because of cultural differences in caregiving roles, responsibilities, and perspectives about care burden.
Objective:
Investigate the association between ER admissions and hospitalizations by Mexican American older adults with and without dementia and symptoms of depression and stress among family caregivers.
Methods:
Data came from the 2010/11 wave of the Hispanic Established Populations for the Epidemiologic Study of the Elderly and Medicare claims files. The final sample included 326 older adults and their caregivers. Negative binomial regression was used to model the association between hospitalizations and ER admissions by older adults in the previous two years and caregivers’ depressive symptoms and stress in 2010/11.
Results:
The number of older adult ER admissions and hospitalizations was not associated with caregiver depressive symptoms. Two or more ER admissions (incident rate ratio [IRR] = 1.26, 95% CI = 1.05–1.51) and two or more hospitalizations (IRR = 1.32, 95% CI = 1.07–1.61) were associated with significantly higher caregiver stress. Additionally, ER admissions and hospitalizations for a circulatory disease or injury and poisoning were associated with significantly higher caregiver stress. These associations were not modified by the care recipient’s dementia status.
Conclusion:
Hospitalizations and ER admissions by older Mexican Americans were associated with greater caregiver stress but not depressive symptoms. These associations were similar for caregivers to older adults with and without dementia.
INTRODUCTION
The growing older adult population in the US has increased the demand for long-term care. Inadequate government funding [1], a strained workforce [2], and concerns about the quality of care [3] have made the long-term care system in the US poorly equipped to meet the needs of the growing older adult population. Most families cannot afford the high out-of-pocket costs of professional long-term care [4]. Consequently, older adults often rely on a spouse or adult child to assist with daily needs. Each year, nearly 42 million people in the US provide family care to someone aged 50 or older [5]. Over 60% of family caregivers are women, and most care for a parent or parent-in-law [5].
Family caregivers frequently report feeling stressed and are at an increased risk for depression [6]. Family caregivers of older adults with dementia are at especially high risk of experiencing stress because of feeling overwhelmed with managing the care recipient’s complex healthcare needs [7] and the potentially distressing behavioral and psychiatric symptoms of dementia [8]. The high stress of providing care to an older adult with dementia can also lead to a greater risk of depression for caregivers [9].
Older adults with dementia are more likely to be admitted to the emergency room and hospitalized than older adults without dementia [10, 11]. Evidence from predominately non-Hispanic White populations indicates an ER admission or hospitalization can be burdensome for an older adult and their caregiver, especially if the older adult has dementia [12–14]. ER admissions and hospitalizations for older adults with dementia are also more costly [15], and dementia contributes to increased out-of-pocket spending on healthcare [16]. Consequently, family caregivers of older adults with dementia may feel stress about potential financial strain from an ER admission or hospitalization.
Hispanics are the largest minority population in the US [17]. Mexican Americans are the largest subpopulation and account for 62% of all Hispanics in the US [18]. Additionally, 30% of all Mexican Americans were born outside the US [18]. The number of older Hispanic adults living with dementia will increase as the population ages. Projections estimate that the number of Hispanics aged 65 and older living with dementia will increase from 500,000 in 2010 to 3.5 million in 2060 [19].
Approximately seven million Hispanics in the US provide unpaid care to an adult aged 50 or older [5]. Like many cultures [20], Hispanic culture emphasizes that the needs of the family come before a person’s own needs [21] and that a female family member will be the primary caregiver [22]. There are also aspects of being a family caregiver that are unique to Hispanics in the US. Hispanic family caregivers are younger than non-Hispanic White caregivers [23]. Sixty-two percent of Hispanic older adults receive care from an adult child compared to 44% of non-Hispanic White older adults [23]. Thus, Hispanic caregivers often need to balance their role as a caregiver with other responsibilities, such as raising children [24]. Hispanic caregivers are also more likely to live with the care recipient than non-Hispanic White and non-Hispanic Black caregivers [23]. Consequently, Hispanic caregivers provide more intense and demanding care for longer than other racial and ethnic groups [25]. Finally, Hispanic family caregivers may experience more financial strain than non-Hispanic Whites because of limited financial resources [26].
Existing evidence on the association between hospitalizations and ER admissions among older adults and caregiver mental health is primarily based on caregiver-older adult dyads who are non-Hispanic White. These results may not generalize to Hispanic populations because of unique Hispanic cultural values that influence caregiving roles, responsibilities, and perspectives about care burden [23, 28]. Hispanic caregivers provide more intense care for a longer period than non-Hispanic White caregivers [23] but report fewer depressive symptoms and lower levels of stress [29]. The findings of lower stress, depression, and burden among Hispanic family caregivers have been attributed to the positive perceptions of caring for a family member [30].
Our primary objectives were to investigate the association between hospitalizations and ER admissions of Mexican American older adults and caregivers’ self-reported symptoms of depression and stress. We also sought to determine if the older adult’s dementia status modifies these associations. We hypothesize that hospitalizations and ER admissions will be associated with greater depressive symptoms and stress among caregivers, especially among those caring for older adults with dementia.
MATERIALS AND METHODS
Data source and sample population
Data came from the 2010/11 wave of the Hispanic Established Populations for the Epidemiologic Studies of the Elderly (H-EPESE). The H-EPESE is a population-based cohort study of Mexican Americans aged 65 years and older living in Texas, Colorado, New Mexico, Arizona, and California [31]. The baseline observation wave was completed in 1993/94 and included 3,050 participants aged 65 and older. Participants were interviewed every two to three years. During the 2010/11 observation wave (Wave 7), participants provided the name and contact information of the person they were closest to or most dependent on for help. A total of 1,078 participants were interviewed in 2010/11, of which 925 provided an informant’s name and contact information (i.e., caregiver). Each caregiver was asked questions about the participant’s health, function, living arrangement, and socioeconomic characteristics. Caregivers were also asked questions about their own socioeconomic and health characteristics.
Survey data for H-EPESE participants interviewed between 1999/2000 (Wave 4) and 2012/13 (Wave 8) have been linked with the following Medicare claims files for 1999 to 2012: (1) Master Beneficiary Summary Files (MBSF), Medicare Provider Analysis and Review (MedPAR) files, Outpatient Standard Analytic files (OUTSAF), and Carrier files [32]. These files were used to identify care recipients who had ever been diagnosed with dementia and hospitalizations and ER admissions in the two years before the 2010/11 interview.
Figure 1 presents the selection of the final sample. Of the 925 caregiver-care recipient dyads, 625 included a care recipient linked with Medicare claims files. We excluded an additional 247 dyads with a care recipient who did not have continuous fee-for-service enrollment for two years before their 2010/11 interview. Finally, we excluded 52 dyads because the caregiver or participant was missing one or more variables. The final sample included 326 dyads.

Selection of the final sample. Note: FFS (fee for service).
Supplementary Table 1 shows the characteristics of the 326 dyads included in the final sample compared to those we excluded from the analysis. Caregivers excluded from the sample were older (56.5 years versus 54.7 years), less likely to be a child of the participant (64.8% versus 74.8%), and had a higher average score on the Center for Epidemiologic Studies Depression (CES-D) Scale (5.73 points versus 3.87 points) than caregivers included in the sample. Excluded care recipients were significantly younger than those included in the analysis (85.6 years versus 86.2 years). Exploratory analyses indicated a large difference in the average number of depressive symptoms among caregivers according to if the care recipient had continuous fee-for-service enrollment (CES-D 3.81 points) or not (CES-D score 6.59 points).
Measures
Caregiver depressive symptoms and stress
Depressive symptoms were measured using the CES-D [33]. The CES-D includes twenty questions about depressive symptoms experienced during the past week. Respondents can reply with rarely or none of the time, some or a little of the time (1–2 days), occasionally or a moderate amount of time (3–4 days), and most or all of the time (5–7 days). The CES-D has a total score that ranges from 0 to 60 points.
Symptoms of stress were measured using a four-item version of the Perceived Stress Scale (PSS-4) [34, 35]. The PSS-4 includes questions about how often during the past month a person felt that they were unable to control important things in their life, handle personal problems, things were going their way, and unable to overcome difficulties. Respondents can reply with never, almost never, sometimes, fairly often, and very often. Each question is scored as 0 (never) to 4 points (very often), and the total score ranges from 0 to 16. The items for being able to handle personal problems and that things were going their way were reverse-coded.
Dementia diagnosis
We used the Chronic Conditions Segment of the Medicare Beneficiary Summary File to identify participants diagnosed with dementia before their 2010/11 interview [11]. The Chronic Conditions Segment of the Summary file includes a variable for dementia that indicates if at least one out of 24 ICD-9 codes are present on one or more inpatient, skilled nursing, home health, Part B institutional, or carrier file claims over a three year period [36, 37]. We used the date of dementia diagnosis in the Chronic Conditions Segment fill to identify participants diagnosed with dementia before their Wave 7 interview. We used the diagnosis date also to determine the age of dementia diagnosis and the number of years before the date of the participant’s 2010/11 interview that dementia was diagnosed.
Emergency room admissions and hospitalizations
We used the Medicare claims files to identify the number of ER admissions and hospitalizations during the two years before the participants’ 2010/11 interview [11, 32]. The MedPAR and OUTSAF files were used to identify ER admissions according to an ER charge of more than zero dollars or ER revenue code, respectively. We used the MedPAR file to identify acute and critical access hospital stays. ER admissions and hospitalizations were each categorized as zero, one, or two or more.
We also investigated if the association between participants’ ER admissions and hospitalizations and caregivers’ mental health differed according to the reason for an ER admission or hospitalization. Because participants could have multiple ER admissions and hospitalizations during the two years before their 2010/11 interview, we selected the ER admission or hospitalization closest to the 2010/11 interview date. The average time between the ER admission or hospitalization and subsequent 2010/11 interview was 8.5 months (median = 7.2, 1st quartile = 2.8, 3rd quartile = 12.7) and 9.6 months (median = 8.4, 1st quartile = 3.5, 3rd quartile = 14.5), respectively. We used the primary ICD diagnosis code for the ER admission or hospitalization to group participants into one of nineteen categories (Supplementary Table 2). The three most common primary ICD diagnosis code categories were circulatory system diseases, digestive system diseases, and injury and poisoning. The remaining categories were combined for sample size reasons and labeled as other.
Covariates
Information for caregivers’ demographics, health characteristics, and mental health symptoms came from the 2010/11 interview. Demographic characteristics included age, gender, marital status, and a dichotomous variable indicating if the caregiver was a child of the participant. Caregivers self-rated their health as excellent, good, and fair-poor. The demographic characteristics of the participants included age, gender, and years of education. We used the Neuropsychological Inventory (NPI) to determine the number of psychiatric symptoms the participant expressed over the last 30-days as reported by the caregiver [38]. The NPI includes 12 symptoms. We categorized the number of symptoms as 0, 1-2, and 3 or more. Finally, we included a dichotomous variable indicating if the caregiver reported being the primary person responsible for assisting the care recipient with household tasks (e.g., cooking, cleaning) or personal care tasks (e.g., bathing, toileting).
Statistical analysis
We used chi-square tests and independent sample t-tests to describe the caregiver and participant characteristics according to the participant’s dementia status. Negative binomial regression was used to model the association between ER admissions and hospitalizations among participants and the number of depressive symptoms and stress symptoms reported by caregivers. Negative binomial regression was used to account for the overdispersion of the scores for depression and stress. The estimated beta coefficients were exponentiated to present the results as incidence rate ratios (IRR). The IRR is the predicted number of depressive or stress symptoms of caregivers to participants with one or two or more ER admissions or hospitalizations compared to caregivers of participants with no ER admissions or hospitalizations.
We modeled the number of hospitalizations and ER admissions separately. All analyses controlled for caregivers’ demographic characteristics, self-rated health, caregiving responsibilities (i.e., household and personal care tasks), and participants’ demographic characteristics and NPI symptoms. We used interaction terms for ER admission by dementia status and hospitalizations by dementia status to test if the associations between ER admissions, hospitalizations, and caregivers’ mental health differed according to participants’ dementia status.
RESULTS
Caregiver and participant characteristics
Table 1 shows the caregiver and participant characteristics according to the dementia status of the care recipient. The average age of caregivers was 54.7 years. Most caregivers were female (73.9%), married (56.4%), and a child of the care recipient (74.8%). Approximately 44% of caregivers reported being in good health. The average scores for depressive symptoms and stress were 3.87 points and 3.72 points, respectively. The average age of care recipients was 86.2 years, 63.2% were female, and the average years of education were 4.6 years (Table 1).
Descriptive characteristics of caregivers and care recipients according to the dementia status of the care recipient
We identified 187 (42.6%) participants diagnosed with dementia before their 2010/11 interview. The average age at first dementia diagnosis was 82.8 years. The average time between the age of dementia diagnosis and the 2010/11 interview was 4.6 years (median = 4.2, 1st quartile = 1.8 years, 3rd quartile = 6.8 years).
The average stress score of caregivers to care recipients with dementia was 4.05 points and 3.47 points for caregivers to care recipients without dementia (p < 0.05). There were also statistically significant differences in the number of NPI symptoms, ER admissions, and hospitalizations by dementia status. The majority (53.2%) of care recipients with dementia had three or more NPI symptoms compared to 31.0% of care recipients without dementia. Forty-six percent of participants with dementia had no hospitalizations compared to 63.1% of care recipients without dementia. Approximately 27% of care recipients with dementia had no ER admissions compared to 40.6% without dementia. We did not detect statistically significant differences in the primary diagnosis code for ER admissions and hospitalizations by dementia status.
Caregiver depressive symptoms
Table 2 presents the adjusted IRRs for the association between care recipients’ ER admissions and hospitalizations and caregivers’ depressive symptoms. The number of ER admissions and hospitalizations was not significantly associated with caregiver depressive symptoms. Dementia status was also not associated with caregiver depressive symptoms. Older caregiver age and three or more NPI symptoms were associated with significantly more depressive symptoms, whereas married caregivers had significantly fewer depressive symptoms (Table 2).
Adjusted association between care recipient emergency room admissions and hospitalizations and caregiver depressive symptoms.
We did not detect statistically significant interactions between ER admissions and dementia status (p = 0.37) or between hospitalizations and dementia status (p = 0.13). Finally, there were no statistically significant differences in caregiver depressive symptoms according to the primary diagnosis code for ER admissions or hospitalizations (Fig. 2).
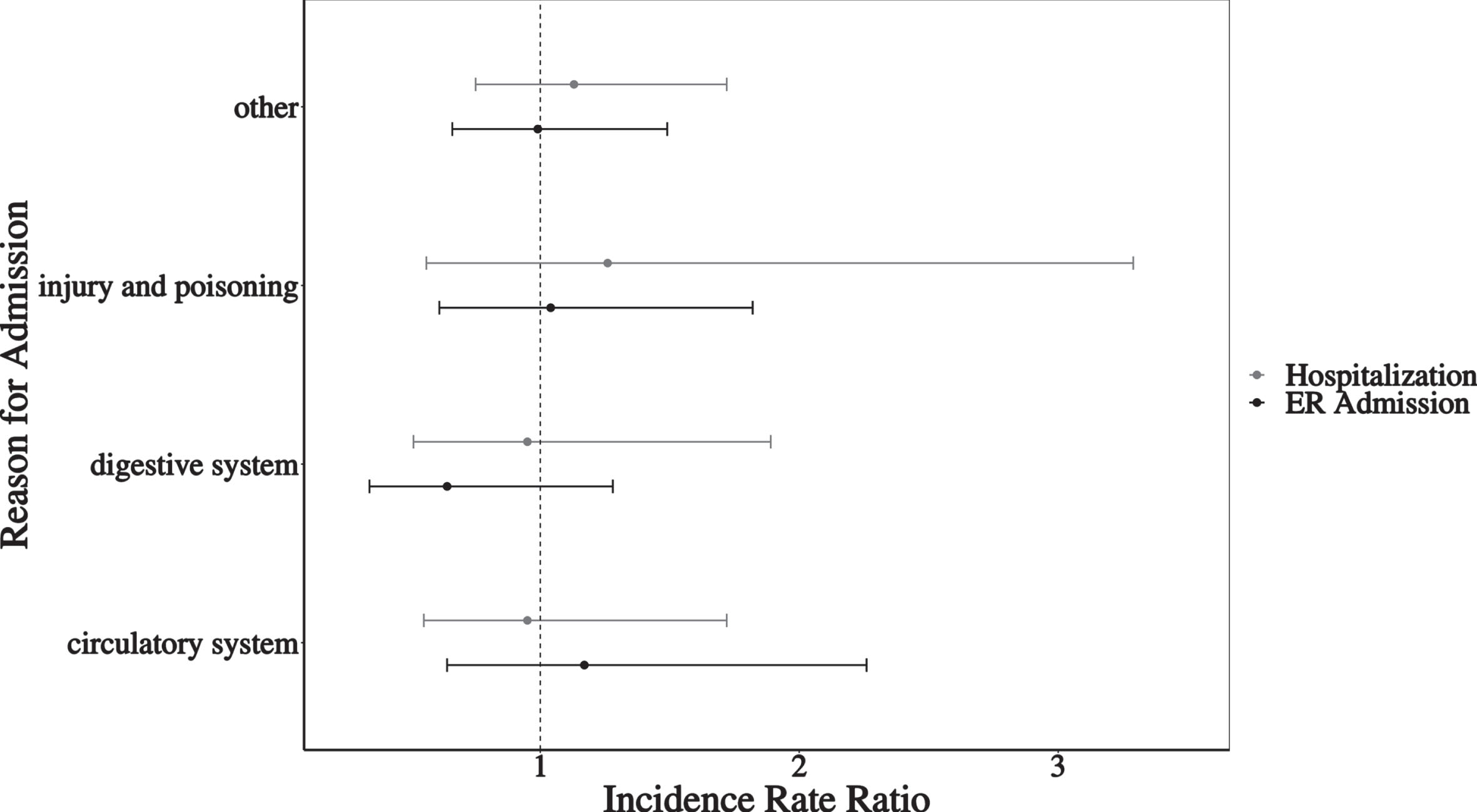
Adjusted association between primary diagnosis code for emergency room admission and hospitalization and caregiver depressive symptoms.
Caregiver stress
The number of care recipients’ ER admissions and hospitalizations was associated with significantly higher caregiver stress scores (Table 3). Compared to caregivers of care recipients with no ER admissions, two or more ER admissions were associated with 1.26 (95% CI = 1.05–1.51) times higher stress. Caregivers of care recipients with two or more hospitalizations had significantly higher stress compared to caregivers of participants with no hospitalizations (IRR = 1.35, 95% = 1.10–1.64). We did not detect statistically significant interactions between care recipients’ dementia status and the number of ER admissions (p = 0.75) or hospitalizations (p = 0.69) and caregiver stress.
Adjusted association between care recipient emergency room admissions, hospitalizations, and caregiver stress
There were statistically significant differences in caregiver stress according to the primary diagnosis code for ER admissions (p < 0.001) and hospitalizations (p = 0.01) (Fig. 3). An ER admission for a circulatory disease (IRR = 1.50, 95% CI = 1.15–1.94) or injury and poisoning (IRR = 1.45, 95% CI = 1.15–1.82) were associated with significantly higher caregiver stress compared to caregivers of participants with no ER admissions. Similarly, hospitalization for a circulatory disease or injury and poisoning was associated with 1.37 (95% CI = 1.08–1.74) and 1.45 (95% CI = 1.01–2.08) times higher caregiver stress, respectively. ER admissions or hospitalizations for a circulatory disease or injury and poisoning were not associated with significantly higher stress compared to admissions for a digestive system condition or other reasons.
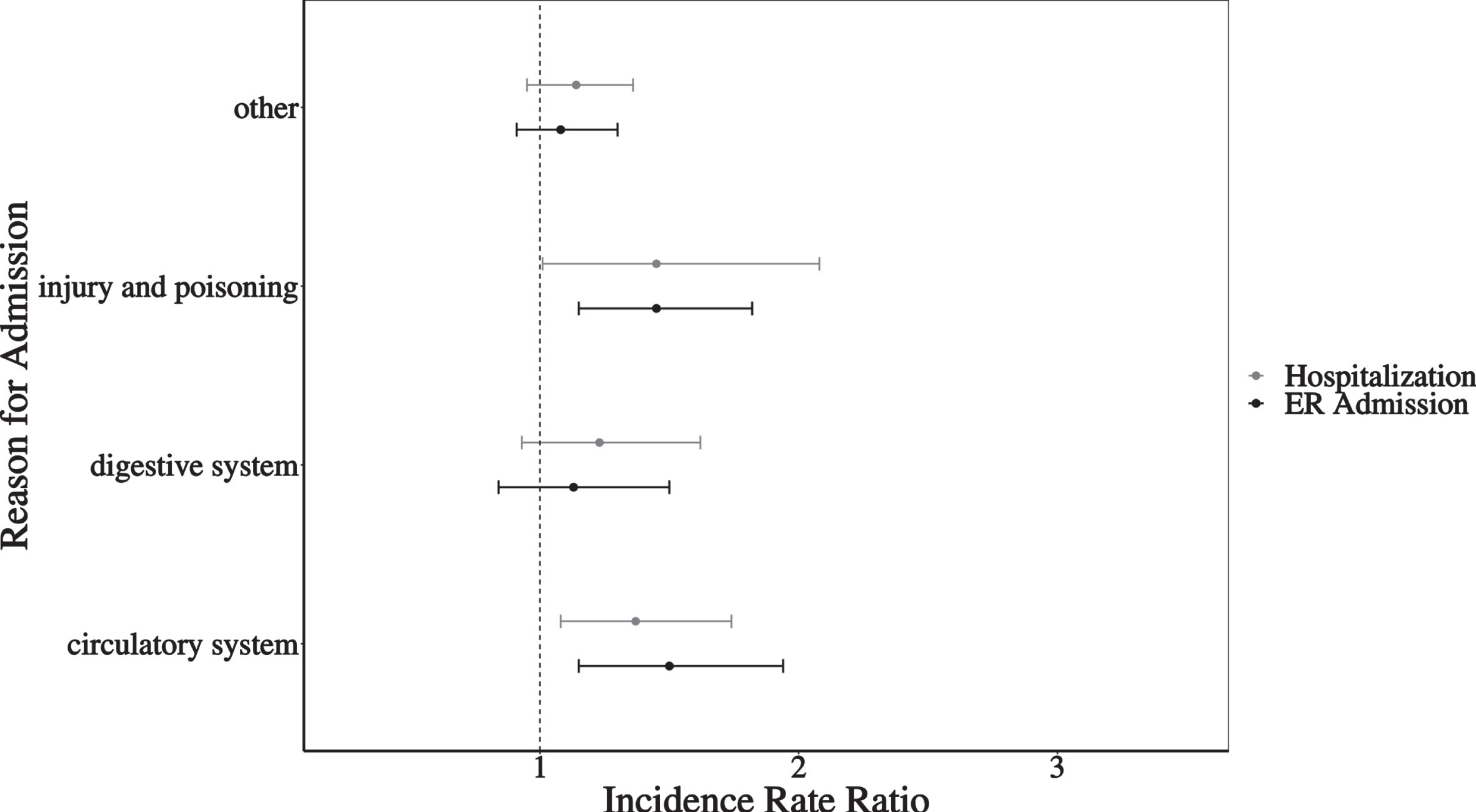
Adjusted association between primary diagnosis code for emergency room admission and hospitalization and caregiver stress.
DISCUSSION
We investigated the association between ER admissions and hospitalizations over two years by Mexican American older adults and caregivers’ depressive symptoms and stress. We found that a greater number of hospitalizations and ER admissions were associated with greater caregiver stress but not depressive symptoms. Older adults’ dementia status did not modify these associations.
ER admissions and hospitalizations for circulatory system conditions, injury, and poisoning were associated with significantly higher caregiver stress. Heart failure is a circulatory system condition that is highly prevalent among older Hispanic adults [39] and is a common hospital discharge diagnosis among older Mexican American adults [32]. Family caregivers to older adults with heart disease must manage increasingly complex and demanding needs as the care recipient’s disease progresses [40]. Family caregivers are often not trained on how to manage complications from circulatory diseases such as heart failure [41], types of home modifications that can prevent falls [42], and ways to reduce the likelihood of adverse events from medication administration errors [43]. In some cases, it may be helpful for a clinician to reassure the family caregiver that some health events that lead to an ER admission or hospitalization cannot be prevented [44].
Physicians, nurses, and other clinicians have a critical role in identifying family caregivers experiencing stress or at high risk for stress [45]. A care recipient’s hospitalization or ER admission may be an opportune time for a physician to ask the caregiver about their health and well-being. Clinicians must be mindful of Hispanic cultural values (e.g., familismo, marianismo) and social characteristics (e.g., gender, nativity, acculturation) that shape caregiving circumstances and influence a caregiver’s willingness to share feelings of stress or burden [46, 47]. The clinical team should also teach caregivers about the care recipient’s health condition, provide training on important caregiving tasks, and give information on how to access supportive services [48, 49].
Our study has limitations. First, we did not have information about caregivers’ depression or stress before their 2010/11 interview. Wave 7 was the first time the Hispanic EPESE interviewed informants (i.e., caregivers). The survey did not ask if the caregiver had previously experienced symptoms of stress or depression. This limitation means our findings do not give evidence for a causal association between a care recipient’s ER admissions and hospitalizations and caregiver stress. There is also the possibility of reverse causality. High depressive symptoms and stress among caregivers are associated with increased hospitalizations and ER admissions for older adults [50]. Second, while other caregiving studies have used the CES-D and PSS-4 [51, 52], these are general measures that do not reflect depressive symptoms or stress from caregiving. Third, unlike prior studies [12–14], caregiver depressive symptoms and stress were not assessed at the time of the older adult’s ER admission or hospitalization.
Another limitation is that we used Medicare claims files to identify older adults with dementia. Medicare claims files have low sensitivity to detect older adults with dementia [53, 54]. Hispanic older adults more often experience a delayed or missed dementia diagnosis than non-Hispanic White older adults [55]. Consequently, we may have misclassified the dementia status of some older adults. Finally, the H-EPESE only includes Hispanics who are of Mexican origin. The Hispanic population in the US is highly diverse, with differences in sociodemographic, behavioral, and health characteristics by country of origin and nativity status [56–58]. This heterogeneity means our results may not be generalizable to Hispanics who are not Mexican American.
Conclusions
Our analysis showed that hospitalizations and ER admissions among Mexican American older adults were associated with greater stress but not greater depressive symptoms for caregivers. Caregiver stress was greatest for those providing care to an older adult with an ER admission or hospitalization for a circulatory condition, injury, or poisoning. We did not find evidence that these associations significantly varied according to the older adults’ dementia status. Future research needs to replicate our findings using measures designed to assess symptoms of depression and stress among caregivers. Future research should also carefully examine the role that health complications and behavioral symptoms that lead to an ER admission or hospitalization have on caregiver depressive symptoms and stress.
Footnotes
ACKNOWLEDGMENTS
We thank Ms. Lin-Na Chou MS of the University of Texas Medical Branch for creating the data file for this analysis.
FUNDING
This research was supported by the National Institutes of Health, National Institute on Aging (K01AG0589, RF1AG068988, R01AG010939, P30AG059301, P30AG024832), National Institute for Minority Health and Health Disparities (R01MD010355), and Eunice Kennedy Shriver National Institute of Child Health and Human Development (K01HD101589).
CONFLICT OF INTEREST
The authors have no conflicts of interest to disclose.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article and/or its supplementary material.