
Abstract
Background:
Some oldest-old individuals can maintain superior cognition despite advanced age. Little is known about the neuropathological changes in the brains of oldest-old superior cognitive performers.
Objective:
Our objective was to examine the associations between Alzheimer’s disease (AD) and non-AD neuropathologic features in relation to superior cognitive performance in oldest-old individuals.
Methods:
We analyzed brain autopsy data from 102 participants with normal cognition from The 90+ Study. Superior global cognitive performers (SGCP) were defined as having Mini-Mental State Examination (MMSE) score ≥28 in the last visit 12 to 2 months before death. To examine the associations between individual and multiple comorbid neuropathologic features with SGCP status we used multiple logistic regression models adjusting for age, sex, and education.
Results:
Alzheimer’s disease neuropathological change (ADNC) and low levels of vascular pathologic change were not associated with superior cognition. In contrast, participants with limbic (OR = 8.37; 95% CI: 1.48–47.44) and neocortical (OR = 10.80;95% CI: 1.03–113.82) Lewy body disease (LBD), or with hippocampal sclerosis (HS) (OR = 5.28; 95% CI: 1.10–25.47) were more likely to be non-SGCP. High total burden of multiple comorbid neuropathologic features was associated with a lower likelihood of being SGCP.
Conclusion:
Oldest-old superior cognitive performers were resilient to ADNC and low levels of vascular pathologic change and were resistant to non-AD neurodegenerative changes and multiple comorbid neuropathologic features. Understanding the factors underlying the ability of superior cognitive performers to resist these changes might provide useful insights on maintenance of superior cognition despite advanced age.
Keywords
INTRODUCTION
Cognitive impairment is considered an almost unavoidable consequence of aging [1, 2], and several autopsy studies have found associations between cognitive impairment and age-related neuropathologic features in the brain [3–7]. However, few studies have examined neuropathologic features in relation to superior cognitive performance. The Northwestern University SuperAging Study defined “SuperAgers” as individuals having similar memory to younger individuals and found significantly lower frequency of Alzheimer’s Disease neuropathologic change (ADNC), i.e., neurofibrillary tangles and amyloid plaques, in the anterior cingulate cortex of SuperAgers [8–12] when compared to age-matched controls. In another study of 10 SuperAgers, they observed sparse to frequent tangles in the hippocampus and no neocortical tangles in 90% (9/10) of SuperAgers [11]. While there is some information on the association between superior cognition in advanced age and ADNC, not much is known about the associations of superior cognition with non-AD neuropathologic features or with multiple comorbid neuropathologic features. Examining brain autopsy data in oldest-old superior cognitive performers could reveal valuable insights on whether their high level of performance results from cognitive resilience despite neuropathologic changes or from resistance to developing such changes [13, 14]. This could inform prevention strategies targeted towards specific neuropathologic features that reduce the likelihood of superior cognitive performance.
Previous autopsy studies on The 90+ Study participants reported that individual and multiple comorbid neuropathologic features were common in oldest-old individuals and were associated with increased likelihood and severity of cognitive impairment [6, 15]. In this study, we explored the superior performance end of the cognitive spectrum using brain autopsy data from The 90+ Study—an ongoing, longitudinal, community-based study of aging and dementia on individuals aged 90 years and older, the oldest-old [15, 16]. Our objectives were: 1) to examine the associations between individual AD and non-AD neuropathologic features with superior cognitive performance in the oldest-old, and 2) to examine the associations between multiple comorbid neuropathologic features with superior cognitive performance in the oldest-old.
METHODS
Participants
The initial participants of The 90+ Study were survivors of the Leisure World Cohort Study (LWCS) [17], an epidemiologic study on the members of a retirement community in Orange County, California. The 90+ Study commenced in 2003 when LWCS participants aged 90 or older on January 1, 2003, were invited to join. A similar invitation was extended on January 1, 2008, and every year thereafter to those turning 90 years old. More recently, volunteers aged 90 years and older who were residents of Orange County, California, and lived within a two hour drive of the study location, were recruited in the study through an open recruitment [18]. While the LWCS participants were recruited regardless of cognitive diagnosis, the volunteers had no or mild dementia. Currently, approximately two thirds of The 90+ Study participants are from the original LWCS and one third are volunteers from open recruitment.
All 1,335 participants (966 from LWCS and 369 volunteers) who agreed to in-person examination were invited to be part of the autopsy program. As of February 2022, 623 participants (308 from LWCS and 315 volunteers) had enrolled in the autopsy program. Of the 623 participants, 481 have died, 452 (94%) came to autopsy, and we have completed the autopsy evaluation and final cognitive diagnosis for 407 participants. Only the 117 participants with normal cognitive diagnosis at the time of death were considered for this analysis (Fig. 1).

Participant flowchart: The 90+ Study. CIND, Cognitive impairment, no dementia; MMSE, Mini-Mental State Examination; non-SGCP, non-Superior Global Cognitive Performers; SGCP, Superior Global Cognitive Performers.
Standard protocol approvals, registrations, and patient consents
All participants or their designated informants provided consent to participate in the study and the study was approved by the University of California, Irvine (UCI) Institutional Review Board (IRB).
Neuropathological assessment
The UCI pathology team procured the brain specimens, which were fixed in formalin and then sent to the Department of Pathology at Stanford University for inspection, dissection, and (immuno)histopathologic evaluation according to current consensus criteria while blinded to cognitive diagnosis and any other participant information. The neuropathologic features were scored as follows: 1) ADNC (0 = not; 1 = low; 2 = intermediate; 3 = high) was based on the National Institute on Aging-Alzheimer’s Association (NIA-AA) “ABC” score, which incorporates Thal Phase for amyloid-β (Aβ) plaques, Braak staging for neurofibrillary tangles, and Consortium to Establish a Registry for AD (CERAD) staging for neuritic plaques [19, 20]; 2) Cerebral amyloid angiopathy (CAA) (0 = none; 1 = mild; 2 = moderate; 3 = severe) [21]; 3) Microinfarcts (0 = none; 1 = 1; 2 = 2; 3 = 3+) [19, 20]; 4) Atherosclerosis (0 = none; 1 = mild when present at branch points in the circle of Willis; 2 = moderate when present at branch points and elsewhere in the circle of Willis; 3 = severe when present on the cerebral convexity); 5) Arteriolosclerosis (0 = none; 1 = mild for partial replacement of vascular smooth muscle cells; 2 = moderate for full replacement of vascular smooth muscle cells; 3 = severe for concentric thickening of the sclerotic vessel wall); 6) Lewy body disease (LBD) (0 = none/olfactory; 1 = brainstem-predominant; 2 = limbic [transitional]; 3 = neocortical [diffuse]) (2 individuals with LBD only in the amygdala were included in the 0 LBD category) [22]; 7) Hippocampal sclerosis (HS) (0 = absent; 1 = present in either right or left or both) [19, 20]; 8) Limbic-predominant age-related TDP-43 encephalopathy neuropathological change (LATE-NC) (0 = none; 1 = amygdala only; 2 = plus hippocampus; 3 = plus middle frontal gyrus) [23]; 9) Age-related tau astrogliopathy (ARTAG) (0 = none; 1 = occasional; 2 = numerous) [24].
Assessment of comorbid pathology indices
To examine the comorbid neuropatholgic features at different severity levels, we followed the methods from a previous study on the Nun Study and the Honolulu-Asia Aging Study (HAAS) [7] to compute summary comorbid neuropathology indices. Each specific neuropathologic feature was given an index value of 0 for absent/negligible levels, 0.4 for intermediate, or 1 to denote severe levels of pathologic change. The index values for the specific neuropathologic features were then added into an index. As done by the previous study, we chose 0.4 as the intermediate level to distinguish the influence of a single severe pathology (comorbid pathology index 1.0) from 2 or 3 intermediate pathologies (comorbid pathology indices 0.8 and 1.2, respectively). Specific neuropathologic feature index values were assigned as follows: 1) AD index value was 0 for low/not, 0.4 for intermediate, and 1.0 for high ADNC; 2) CAA index value was 0 for was low, 0.4 for mild/moderate, and 1.0 for severe CAA; 3) Microinfarcts index value was 0 for no, 0.4 for 1-2, and 1.0 for 3 or more microinfarcts; 4) Atherosclerosis index value was 0 for no, 0.4 for mild/moderate, and 1.0 for severe atherosclerosis; 5) Arteriolosclerosis index value was 0 for no, 0.4 for mild, and 1.0 for moderate/severe arteriolosclerosis; 6) LBD index value was 0 for none/olfactory LBD, 0.4 for brainstem-predominant/limbic LBD, and 1.0 for neocortical (diffuse) LBD; 7) HS index value was 0 for absent, 0.4 for unilateral, and 1.0 for bilateral HS; 8) LATE-NC index value was 0 for no, 0.4 for amygdala, and 1.0 for hippocampal/cortical LATE-NC; 9) ARTAG index value was 0 for no, 0.4 for occasional, and 1.0 for numerous ARTAG. Additionally, to derive binary severe vascular index values, all vascular neuropathologies, i.e., CAA, microinfarcts, atherosclerosis, and arteriosclerosis, were further recoded as- absent (=0) when the specific vascular pathology index value were 0 or 0.4, and present (=1) when the index value was 1.0.
Four different comorbid neuropathology indices were calculated as follows: 1) Total neuropathology index was the sum of all (i.e., ADNC, CAA, microinfarcts, atherosclerosis, arteriosclerosis, LBD, HS, LATE-NC, and ARTAG) neuropathology index values; 2) Vascular index was the sum of CAA, microinfarcts, atherosclerosis, and arteriosclerosis index values; 3) Severe vascular index was the sum of severe vascular index values for CAA, microinfarcts, atherosclerosis, and arteriosclerosis; 4) Neurodegenerative index was the sum of index values for LBD, HS, LATE-NC, and ARTAG.
Cognitive diagnosis
Full clinical evaluations of participants carried out every six months consisted of a neurologic examination, physical examination, full neuropsychological battery [25], review of medical history, examination of medication containers, and interviews with informants. A final cognitive diagnosis was assigned after death in a multidisciplinary consensus conference using all available information from the longitudinal evaluations, brain imaging when clinically available, and medical records. All cognitive diagnosis assignments were done blinded to pathologic evaluation results. Participants were diagnosed as having normal cognition, cognitive impairment but no dementia (CIND), or dementia. A dementia diagnosis was made according to Diagnostic and Statistical Manual of Mental Disorders 4th Edition diagnostic criteria [26]. CIND was assigned when cognitive or functional impairments were present but did not meet criteria for dementia.
Superior global cognitive performer definition
The neuropsychological battery included the Mini-Mental State Examination (MMSE) to assess global cognition [27]. For this work, we assessed maintenance of superior global cognition until the time of death. Superior global cognitive performers (SGCP) were defined as individuals who had: 1) normal diagnosis in the consensus conference and, 2) an MMSE score of 28 or above in the last visit 12 to 2 months before death. Non- superior global cognitive performers (non-SGCP) were individuals who also had normal diagnosis in the consensus conference but had an MMSE score below 28. This cut-off was based on a previous study on The 90+ Study participants reporting a mean MMSE score of 28 in cognitively normal participants [28]. To limit the possibility of classification error due to poor cognitive performance resulting from terminal illness, we did not consider MMSE scores in the last 2 months of life.
Statistical analysis
We describe participant characteristics and proportion of participants overall and by SGCP status. We calculated the different comorbid indices, examined their distribution by SGCP status, and then categorized the indices into smaller groups according to their distribution, such that each category had sufficient number of SGCP and non-SGCP participants. The total neuropathology index was categorized as <1.8 (reference group), 1.8-<3, 3-<4, and 4+. We did not categorize the vascular index as there was no clear relationship pattern with SGCP status. The severe vascular index was categorized as 0 (reference group), 1, 2, and 3. The neurodegenerative index was categorized as 0 (reference group), 0.4-<1, and 1+. To examine the associations with individual and multiple comorbid neuropathologic features, we calculated odds ratios (OR) and 95% confidence intervals (CI) using multiple logistic regression models adjusting for age at visit (last visit when MMSE was done), sex, and college education (yes/no). For all analyses, our outcome of interest was SGCP status, and we modeled the probability of being a non-SGCP. Therefore, in our results, an OR above 1 would indicate a higher likelihood of being a non-SGCP which also indicates a lower likelihood of being a SGCP. Conversely, an OR below 1 would indicate a lower likelihood of being a non-SGCP which also indicates a higher likelihood of being a SGCP.
Secondary analyses
To assess the robustness of our analysis, we did additional secondary analyses. First, since some of the neuropathologic features had low prevalence in our study population, which could lead to sparse data bias, we conducted exact logistic regressions for all neuropathologic features in relation to superior cognition. Second, we tried two alternative MMSE cut-off points (27 and 29) to define superior cognitive performers. To examine the associations of superior cognition using these alternative cut-offs with individual neuropathologic features, we repeated the multiple logistic regression analyses adjusting for age at visit, sex, and college education to calculate OR and 95% CI. All analyses were performed using SAS 9.4 (SAS Institute; Cary, NC, US).
RESULTS
Out of 117 autopsied participants with normal cognitive diagnosis, 102 had at least one MMSE score between 12 to 2 months before death (Fig. 1). Overall, the average age of our study participants at the time of their last visit was 97.1 years. Most participants were women (59.8%) and college-educated (56.9%). Among these participants, 71 (69.6%) were classified as SGCP while 31 (30.4%) were non-SGCPs. There was no significant difference in age, sex, education, LWC participation, and brain weight between SGCPs and non-SGCPs (Table 1).
Characteristics of autopsied cognitively normal participants: The 90+ Study
MMSE, Mini-Mental State Examination.
Distribution of individual and multiple comorbid pathologies by SGCP status
The distribution of neuropathologic features by SGCP status are shown in Table 2. ADNC was not different between SGCP and non-SGCP participants with most participants in both groups having low and intermediate ADNC (66.2% of SGCPs versus 61.3% of non-SGCPs). When separately examining the distribution of the A score, Braak tangle stage, and C scores we found no difference in the SGCP and non-SGCP. Among vascular neuropathologic features, CAA was observed in about half of the participants in both groups. Severe CAA was less common in SGCPs (5.6%) compared to non-SGCPs (16.1%). Microinfarcts were slightly more common in SGCPs (22.5%) compared to non-SGCPs (19.4%). Mild or moderate atherosclerosis was present in more than 70% of participants in both the SGCPs and non-SGCPs while mild or moderate arteriolosclerosis was present in above 85% participants in both groups. The severe vascular pathologic changes were infrequent in both groups and none of the participants in either group had severe arteriolosclerosis. The non-AD neurodegenerative neuropathologic features were less frequent in SGCPs than in non-SGCPs. HS was observed in 4.2% of SGCPs compared to 16.1% of non-SGCPs. LBD was observed in 9.9% of SGCPs compared to 35.5% of non-SGCPs. LATE-NC was observed in 19.3% of SGCPs compared to 32.3% non-SGCPs. HS and LATE-NC co-existed in 4 participants, all of whom were non-SGCPs (not shown in table). Occasional ARTAG was observed in half of the participants in both groups, while numerous ARTAG were observed in 5.6% of SGCPs versus 12.9% non-SGCPs (Table 2).
Associations between individual neuropathological features and superior global cognitive performance in the oldest-old
aMultiple logistic regression adjusting for age at visit for last MMSE, sex, and education used to calculate Odds ratio (OR) and 95% Confidence Interval (CI). Values in bold are statistically significant. bOR calculated for 2+ microinfarcts. 1 SGCP with 3+ microinfarct was included in this analysis. cOR calculated for hippocampal/cortical LATE-NC. 2 persons non-SGCPs with LATE-NC in cortex were included in this analysis. AD, Alzheimer’s disease; ARTAG, Age-related tau astrogliopathy; LATE-NC, Limbic-predominant age-related TDP-43 encephalopathy neuropathological change; NIA-AA, National Institute on Aging-Alzheimer’s Association.
To examine comorbid pathology indices by SGCP status, we first evaluated their distribution (Fig. 2). The total neuropathology index scores ranged from 0 to 4.8 with SGCPs having lower index scores while non-SGCPs tended to be on the higher index score range, as shown by the red stacked bars in Fig. 2A. Overall, most participants had scores between 1.8 to 2.8 (Fig. 2A). The vascular index scores ranged from 0 to 2.4 but did not show a clear pattern of distribution based on SGCP status (Fig. 2B). The severe vascular index scores ranged from 0 to 3 with SGCPs having lower scores (Fig. 2C). The neurodegenerative index scores ranged from 0 to 2.4 with most SGCPs having lower scores. However, the only participant with a score of 2.4 in the neurodegenerative pathology index was a person categorized as SGCP (Fig. 2D).
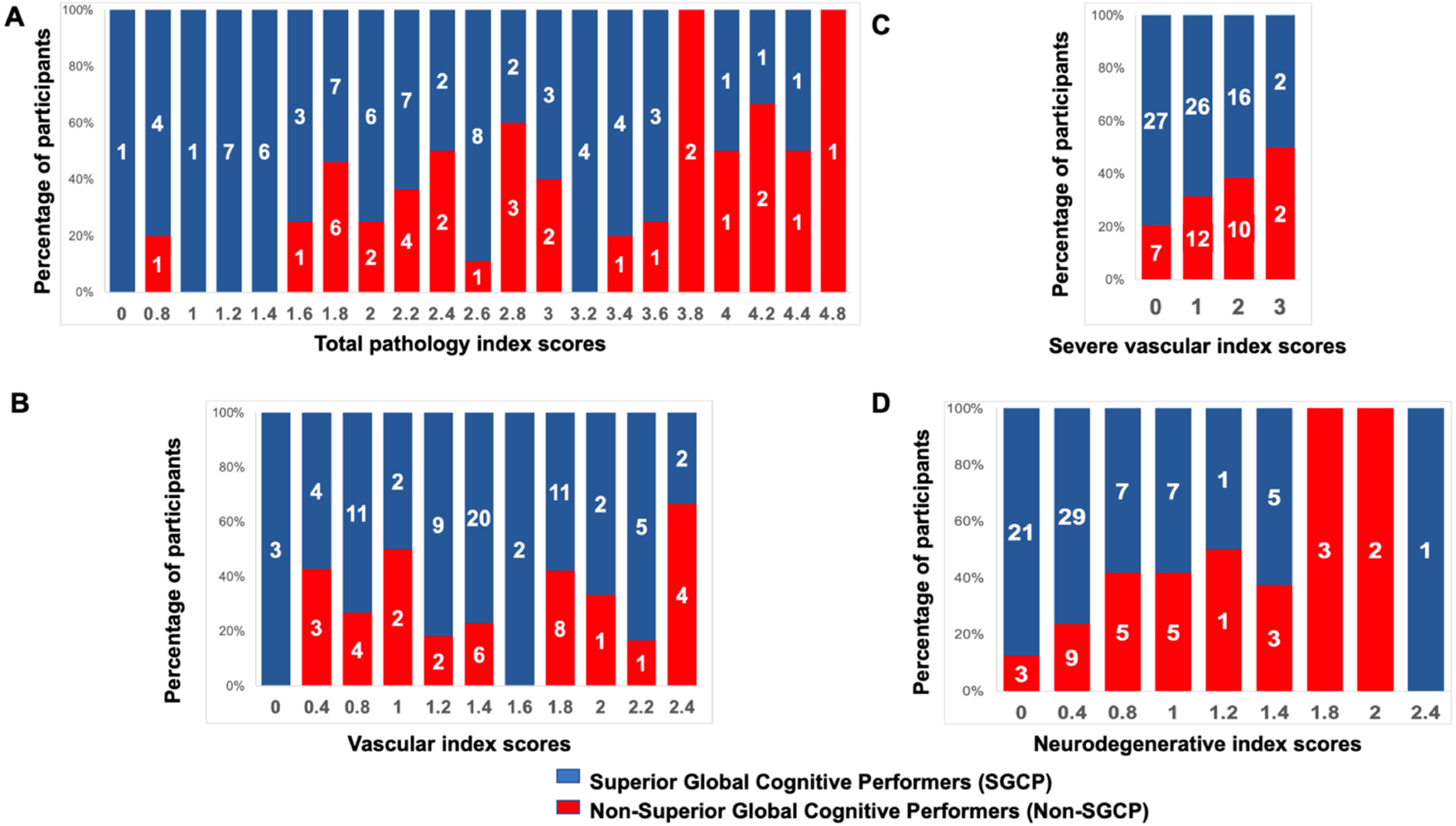
Distribution of the comorbid neuropathology index scores by superior global cognitive performance in the oldest-old. Numbers inside bars denote frequency.
Association of ADNC and total neuropathology index with superior cognitive performance
We used logistic regression models adjusting for age, sex, and education to examine the associations of ADNC, A score, Braak tangle stage, and C score, as well as total pathology index with SGCP status. There was no association between ADNC severity level and SGCP status. The ORs ranged from 0.53 to 1.24, and there was no clear pattern of association with different levels of ADNC severity (Table 2). Similarly, there was no association between the individual ADNC pathologies (A score, Braak stage and C score) with SGCP status (Table 2).
There was a significantly higher likelihood of being a non-SGCP with increasing total neuropathology index score. Compared to the reference category (0-<1.8 score), for the total neuropathology index category 1.8-<3 the OR was 5.87 (95% CI:1.23,28.05), for 3-<4 category the OR was 3.75 (95 CI: 0.62, 22.82), and for 4+ category the OR was 18.31 (95% CI: 2.34,143.19) (Fig. 3A).
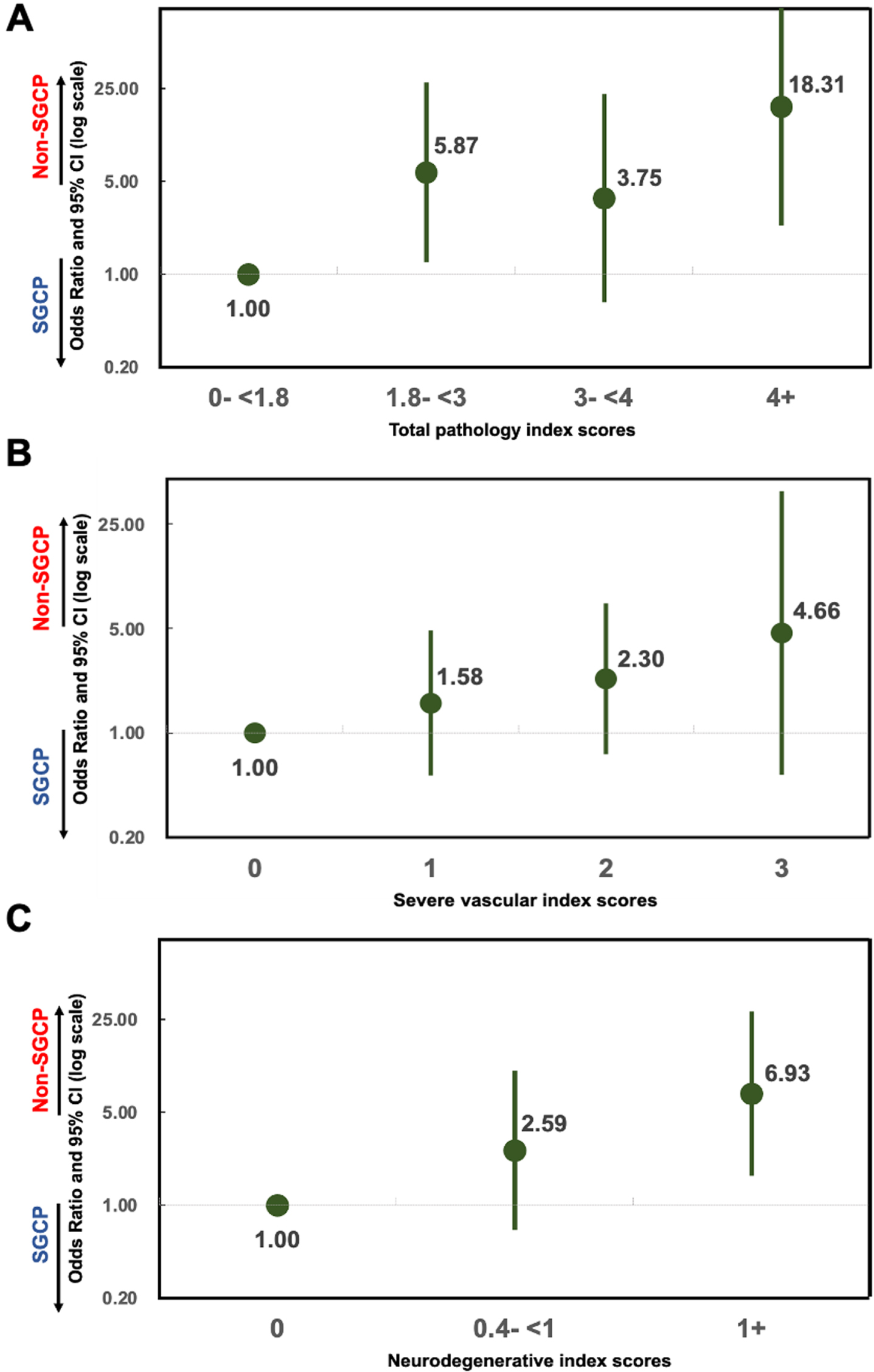
Association between comorbid neuropathology indices and superior global cognitive performance in the oldest-old. A) Association with total neuropathology (ADNC, CAA, microinfarcts, atherosclerosis, arteriosclerosis, LBD, HS, LATE-NC, and ARTAG) index scores. B) Association with severe vascular (CAA, microinfarcts, atherosclerosis, and arteriosclerosis) index scores. C) Association with neurodegenerative (LBD, HS, LATE-NC, and ARTAG) index scores. ADNC, Alzheimer’s disease neuropathological change; ARTAG, Age-related tau astrogliopathy; CAA, cerebral amyloid angiopathy; HS, hippocampal sclerosis; LATE-NC, limbic-predominant age-related TDP-43 encephalopathy neuropathological change; LBD, Lewy body disease; Non-SGCP, Non-Superior Global Cognitive Performers; SGCP, Superior Global Cognitive Performers.
Association between individual and multiple vascular neuropathologic features and superior cognitive performance
Logistic regression models adjusting for age, sex, and education were also used to examine the associations of individual and comorbid vascular neuropathologic features with SGCP status. There were trends that participants with severe vascular pathologic changes were more likely to be non-SGCP (Table 2). For example, the ORs for severe CAA compared to no CAA was 2.77 (95% CI:0.62–12.36), for 2+ microinfarcts compared to no microinfarcts 2.28 (95% CI:0.30–17.52), for severe atherosclerosis compared to no atherosclerosis was 5.72 (95% CI: 0.42–78.78) and no participant had severe arteriolosclerosis. However, none of these ORs reached statistical significance.
Unlike the vascular index, which showed no clear relationship pattern to SGCP status, for the severe vascular index, increasing scores tend to be associated with increased likelihood of being a non-SGCP, although the ORs were not statistically significant (Fig. 3B).
Association between individual and multiple neurodegenerative neuropathologic features and superior cognitive performance
As above, logistic regression models adjusting for age, sex, and education were used to examine the associations of individual and comorbid neurodegenerative neuropathologic features with SGCP status. Compared to participants with no LBD, those having LBD were more likely to be non-SGCP, and the association was significant for limbic LBD (OR = 8.36:95% CI:1.47–47.44) and neocortical LBD (OR = 10.80; 95% CI:1.02–113.82). Participants with HS were more likely to be non-SGCP compared to those without (OR = 5.28; 95% CI:1.10–25.47). Compared to participants with no LATE-NC, for all levels of LATE-NC there was a non-significant but increased likelihood of being a non-SGCP. Compared to participants without ARTAG, those with numerous ARTAG had increased, although non-significant, likelihood of being a non-SGCP (Table 2).
There was a significantly higher likelihood of being a non-SGCP with increasing neurodegenerative index score, with OR = 6.93 (95% CI = 1.66–28.83) in participants with 1+ scores compared to participants with score 0 (Fig. 3C).
Secondary analyses
Given the sparse data for some of the neuropathologic features, we conducted exact logistic regression to confirm the robustness of our findings. For most neuropathologic features, the magnitude of the unadjusted ORs from the exact logistic regression analyses were very similar to the maximum likelihood estimates (MLE) of ORs from unadjusted and adjusted logistic regressions (Supplementary Table 1). The only exceptions were neocortical LBD and HS presence, for which the 95% CI were wider and the ORs slightly attenuated and thus non-significant (Supplementary Table 1).
We also conducted secondary analyses changing the MMSE cut-off for superior performance to 27 and 29 and examined the associations with neuropathologic features. With the lower cut-off of 27, more participants (87 out of 102) were categorized as superior performers and fewer (15 participants) were non-superior performers (Supplementary Table 2). The results for the association of individual neuropathologic features with superior cognition remained mostly unchanged with the following few differences (Supplementary Table 2). For ADNC, the ORs increased in magnitude ranging from 0.9 to 6.6 (versus 0.53 to 1.24 with the original cut-off of 28) but remained non-significant with wider 95% CIs and no clear pattern of association. All levels of CAA were associated with non-significant increased likelihood of being a non-superior performer. For limbic LBD the OR was attenuated (OR = 3.62) and not associated with being non-superior performer. The OR for HS was higher (OR = 7.08) and remained significantly associated with being non-superior performer (Supplementary Table 2).
With the higher MMSE cut-off of 29, fewer individuals (49 out of 102) were superior cognitive performers and more (53 participants) non-superior performers. Even with this cut-off, the results for the associations continued to remain mostly unchanged with the following few differences. Mild (OR = 0.12) and moderate (OR = 0.17) CAA were associated with significantly decreased odds of being a non-superior performer, whereas with the original cut-off of 28 these associations were non-significant. For limbic (OR = 5.25) and neocortical (OR = 3.11) LBD, the ORs were attenuated and not significantly associated with being non-superior performer. For HS, the OR was attenuated (OR = 2.27) and not significantly associated with increased odds of being a non-superior performer (Supplementary Table 3).
Switching the MMSE cut-off values to lower and higher levels resulted in attenuation of some of the ORs, but the direction of association remained consistent. The secondary analyses did not have much of an impact on our overall results and conclusions and suggest the robustness of our findings.
Comparison of autopsied and non-autopsied participants
A substantial proportion of The 90+ Study participants invited to join the autopsy program did not consent to autopsy. Therefore, we compared the autopsied and non-autopsied individuals to explore differences between the two groups. Compared to those who did not consent to autopsy, the autopsy group included fewer women (66.9% versus 74.3%), were slightly younger (93.0 versus 93.8 years), had higher education (51.9% college or higher versus 38.1%), and fewer were LWC participants (49.4% versus 92.4%) (Supplementary Table 4).
DISCUSSION
Our study aimed to evaluate the neuropathological findings in superior global cognitive performers that distinguish them from non-superior performing peers using autopsy data from 102 cognitively normal participants of The 90+ Study. Neither ADNC nor vascular neuropathologic features were associated with superior cognitive performance. However, among the few cognitively normal participants with severe vascular pathologic changes, we observed a suggestion of higher likelihood of not having superior cognition, i.e., lower likelihood of superior cognition. Participants with LBD and HS were more likely to be non-SGCP, i.e., less likely to have superior cognition. There was a trend that presence of LATE-NC was related to higher likelihood of being non-SGCP, i.e., a lower likelihood of superior cognitive performance, although the results were not statistically significant. Presence of higher levels of multiple comorbid neuropathologic features (as indicated by the comorbid neuropathology indices) were associated with increased likelihood of being non-SGCP, i.e., a lower likelihood of superior cognitive performance.
ADNC was very common, found in 87% of our study participants but was not associated with superior cognitive performance. This finding is expected given that ADNC is almost ubiquitous in this oldest-old cohort [14], and has been commonly reported in individuals without dementia in a recent meta-analysis on 17 population based autopsy studies with age of death 65 years and above [29]. Furthermore, a previous analysis on eight participants from The 90+ Study reported the presence of plaques and tangles—the hallmarks of ADNC—in the brains of “SuperAgers” [30]. However, previous autopsy studies in the Northwestern University SuperAging Study cohort reported that compared to age-matched controls, fewer neurofibrillary tangles and amyloid plaques were observed in the anterior cingulate and entorhinal cortex of “SuperAgers”, defined as 80 and older individuals having similar memory to participants 20 to 30 years younger [8, 12]. Methodological differences including difference in superior cognitive performer definition, brain regions evaluated, and larger sample size could all have contributed to the incongruence with our study results.
We also found that maintenance of superior cognitive performance in this oldest-old cohort was associated with lower levels of comorbid neuropathologic features in the brain. While no study has analyzed multiple comorbid neuropathologic features in cognitively superior individuals, previous reports from The 90+ Study and other cohorts [7, 33] have shown the association between mixed neuropathologic features and increased likelihood and severity of cognitive impairment. Results from the Nun Study and HAAS reported that comorbid neuropathologic features were common and the cumulative burden was the most relevant determinant of cognitive impairment [7]. A large study on clinic-based population from the NIH-funded Alzheimer Disease Research Centers on individuals with and without dementia with mean age 81 years reported that mixed neuropathologic features were common and high comorbid neuropathology was associated with lower MMSE scores [5]. Results from the Nun Study and HAAS also reported that cognitive resilience, despite high levels of neurofibrillary tangles, was strongly associated with minimal comorbid neuropathologic features [7]. Another study from the Religious Orders Study (ROS), and the Rush Memory and Aging Project (MAP) on older adults with a mean age of 87 years reported comorbid ADNC, vascular and non-AD neurodegenerative neuropathologic features as well as their increasing severity were related to faster rate of cognitive decline in individuals without dementia [32, 34]. Results from Adult Changes in Thought (ACT) study comparing vascular neuropathologic features in ADNC resistant groups to their age-matched AD dementia groups reported that resistant individuals had less arteriolosclerosis, microinfarcts and CAA, and maintained high cognitive scores over time [35]. Given the commonality of ADNC in our study participants, it is possible that the added presence of vascular and neurodegenerative neuropathologic features lead to worsening of cognitive performance in cognitively normal oldest-old.
Among vascular neuropathologic features, CAA and microinfarcts were less common while lower levels of atherosclerosis and arteriolosclerosis were relatively common in all participants. However, very few cognitively normal participants had severe levels of any vascular neuropathology, and none had severe arteriolosclerosis. No previous autopsy study has explored vascular neuropathologic features in relation to superior cognitive performance. However, vascular neuropathologies have reportedly been associated with cognitive impairment. CAA has been associated with an increased likelihood of dementia and a faster rate of global cognitive decline [36]. Previous studies in our cohort [4] as well as other cohorts [37–40] reported that microinfarcts independently and in presence of ADNC were associated with increased odds of dementia and cognitive impairment. A previous autopsy study on Brazilian population aged >50 years found an association between high-grade atherosclerosis and dementia [41]. A study on participants of the Baltimore Longitudinal Study of Aging with mean age 87.6 years observed high prevalence of atherosclerosis and found it to be an independent risk factor for dementia [42]. In our study, there were trends that participants with severe vascular pathologic changes were less likely to be superior cognitive performers, but none of the associations were statistically significant. Given the high mortality in the presence of vascular disease, it is possible that individuals with severe vascular pathologic changes do not survive to become oldest-old [43–45]. As a result, there could be low prevalence of severe vascular pathologies in cognitively normal participants and consequently, limiting the power of our data to determine whether absence of severe vascular pathologic changes is indeed related to maintaining superior cognition.
With multiple comorbid severe vascular pathologic changes as determined by the severe vascular index, we observed a trend showing decreased likelihood of superior cognitive performance. A previous study in the ROS-MAP participants reported mixed vascular disease associated with faster cognitive decline, especially in the presence of atherosclerosis and arteriolosclerosis [46]. Our findings are consistent with available literature and allude to severe vascular pathologic changes independently and in combination having a more deleterious effect on cognition, while at lower levels their effect is not as prominent. However, given the small sample size of individuals with severe vascular pathologic changes, the interpretation of our results warrants caution.
Among neurodegenerative neuropathologic features, LBD and HS were rare in these cognitively normal oldest-old and were associated with a lower likelihood of superior cognition. About 20% of our participants had LATE-NC and showed trends of association with a lower likelihood of superior cognition. Despite the comorbidity with HS [47], only 4 of our 102 participants had HS with LATE-NC and none had superior cognition. In the autopsy study on Northwestern SuperAging study participants, the authors found a single case of HS and 2 cases of LBD out of 10 SuperAger cases studied [11]. Our results are consistent in reporting a low prevalence of these neuropathologic features in superior cognitive performers.
We further observed that high levels of total burden of non-AD neurodegenerative neuropathologic features was less likely in superior cognitive performers. Despite limited evidence on the association with superior cognition, in published literature there is a known association of both individual and comorbid non-AD neurodegenerative neuropathologies with global cognitive impairment and dementia [39, 48–50]. Previous studies have reported that LBD independently and in presence of ADNC were associated with increased odds of dementia [5, 39] and cognitive decline [34]. Studies from our cohort [14] and other cohorts [23, 49] have reported association of independent and comorbid LATE-NC and HS with global cognitive impairment. Our findings add to the evidence by reporting an association between superior cognitive performance in oldest old and absence of independent and comorbid non-AD neurodegenerative neuropathologic features.
Resistance is inferred when observed levels of dementia-related neuropathologic features is lower than expected based on individual characteristics while cognitive resilience is inferred from a higher level of cognitive functioning than expected despite high neuropathologic burden [13, 14]. Our results indicate that superior cognitive performance in oldest-old can be explained by concepts of both resilience and resistance. In cognitively normal oldest-old, the superior global cognitive performers were resilient to ADNC, i.e., they maintained superior cognition despite having ADNC. On the other hand, other neurodegenerative neuropathologic features, particularly LBD and HS, were very rare indicating resistance, i.e., their ability to escape the development of these changes in the brains. For vascular neuropathologic features, the results were mixed showing resilience at lower levels and potential resistance to higher levels of vascular pathologic change needed to maintain superior cognitive performance.
One of the major strengths of our study is the sample size given the advanced age of our population. Our results are derived by analyzing autopsy data from 102 cognitively normal individuals who died at a mean age of 97 years. Second, we used cognitive test scores between 12 to 2 months before death. In published literature there is no consensus definition for superior cognitive performance. Most studies define superior cognitive performance at a specific age range relative to either age-matched peers or younger cohorts. However, individuals who are superior performers at a particular age might decline progressively over time and this decline would be faster in oldest-old. By relying on MMSE performance in the last year of life, we could ensure that the participants identified as SGCPs maintained high performance throughout life. By excluding test scores from the last two months before death, we could avoid misclassifying a SGCP who had lower scores due to terminal illness. Third, unlike other studies that identify superior performers in memory, we used MMSE which is a measure of global cognition. This is important as superior memory performance does not always indicate superior performance in other domains [51, 52]. By evaluating global cognition, we aimed to identify individuals with superior performance in memory as well as other cognitive domains.
Our study had some limitations. First, despite the relatively large sample size, very few participants had severe levels of vascular and neurodegenerative neuropathologic features which could lead to sparse data bias. One hallmark sign of sparse data bias in multivariate analysis is that, as more variables are added to the regression model the coefficient estimates get further away from the null [53]. However, this was not the case in our study as the adjusted and unadjusted ORs were very similar. In addition, the ORs from the exact logistic regression, which can be used to address sparse data bias when sample sizes are small, showed very similar associations to the ORs from MLE logistic regressions suggesting the robustness of our findings. Nonetheless, we should be cautious in drawing inference on the associations of vascular and neurodegenerative neuropathologic features with superior cognition, and future work should examine these associations in other datasets of oldest-old individuals. Second, MMSE test scores are related to education level and our participants were highly educated [54, 55]. We found about 70% cognitively normal participants were SGCPs. It is possible that in some cases the high MMSE scores are due to better test taking abilities and not necessarily superior cognition levels. Nonetheless, since all participants were cognitively normal at the time of death, we expect most participants to have relatively high MMSE scores. Moreover, in our secondary analyses we examined all associations using alternative lower and higher cut-off values of MMSE, and yet got very similar results. These additional findings suggest that our findings are robust. Third, The 90+ Study participants are mostly White college-educated women. However, given that among individuals aged 85 and older there are two females for every male, and around 81% are Non-Hispanic White [56], our results are somewhat generalizable to oldest-old US population in terms of sex and race distribution. Nonetheless, we acknowledge that the lack of ethnoracial and educational diversity in our cohort precludes us from generalizing the findings from this study to a more diverse population. Fourth, since we did not examine cognitive trajectories and only assessed cross-sectional superior cognition at the time of death, we did not test preserved cognition over time. As a result, individuals starting with MMSE scores below the cut-off and maintaining the same over time would not qualify as SGCP despite no cognitive decline, Future work should analyze individuals with stable cognitive trajectories over time and examine the association with neuropathologic features. Last, The 90+ Study participants who consented to the autopsy study had significant demographic differences from the non-autopsied participants. This could make our findings less reflective of the general population.
To our knowledge, this is the first study that examines associations between individual AD and non-AD neuropathologic features as well as multiple comorbid neuropathologic features with superior cognitive performance. We report new evidence about the neuropathologic features in the brains of oldest-old individuals who maintain superior cognition till the time of death. Our findings suggests that while AD and low levels of vascular pathologic changes are common in oldest-old superior cognitive performers, they remain resistant to severe vascular and non-AD neurodegenerative changes, in particular, LBD and HS. They also have lesser total burden of comorbid neuropathologic features. Therefore, preventive measures targeted towards increasing resistance and resilience to non-AD comorbid neuropathologies in the brain might be useful in maintenance of superior cognition despite advanced age.
Footnotes
ACKNOWLEDGMENTS
We thank the participants and staff of The 90+ Study.
FUNDING
This research was funded by grants from the NIH (R01AG21055, UF1 AG057707, and P30AG066519). The study sponsors had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
CONFLICT OF INTEREST
Roshni Biswas, Claudia Kawas, Syed A Bukhari, and Maria Corrada declare no conflicts of interest.
From 2019-2022, Luohua Jiang served as a paid advisor on the Scientific Advisory Board of Birkeland Current, a small business that was funded by National Institute on Aging to develop a medical device that monitors impacts of cognitive decline on Activities of Daily Living.
Thomas Montine receives royalties from Up To Date.
DATA AVAILABILITY
The data supporting the findings of this study are available from the corresponding author upon reasonable request.