
Abstract
Background:
Suppressor of tumorgenicity 2 (ST2) is highly expressed in brain tissue and is a receptor for interleukin 33 (IL-33). ST2 exists in two forms, a transmembrane receptor (ST2L) and a soluble decoy receptor (sST2). IL-33 binds to ST2L, triggering downstream signaling pathways involved in amyloid plaque clearance. Conversely, sST2 binds competitively to IL-33, attenuating its neuroprotective effects. High sST2 levels have been reported in mild cognitive impairment (MCI) and Alzheimer’s disease (AD), suggesting that the IL-33/ST2 signaling pathway may be implicated in neurodegenerative diseases.
Objective:
To investigate plasma sST2 levels in controls and patients with MCI, AD, frontotemporal dementia (FTD), and Parkinson’s disease (PD).
Methods:
Plasma sST2 levels were measured using ELISA in 397 subjects (91 HC, 46 MCI, 38 AD, 28 FTD, and 194 PD). Cerebrospinal fluid (CSF) levels of sST2 were measured in 22 subjects. Relationship between sST2 and clinical outcomes were analyzed.
Results:
Plasma sST2 levels were increased across all disease groups compared to controls, with highest levels seen in FTD followed by AD and PD. Dementia patients with higher sST2 had lower cross-sectional cognitive scores in Frontal Assessment Battery and Digit Span Backward. At baseline, PD-MCI patients had higher sST2, associated with worse attention. In the longitudinal PD cohort, higher sST2 significantly associated with decline in global cognition and visuospatial domains. Plasma sST2 levels correlated with CSF sST2 levels.
Conclusion:
Plasma sST2 is raised across neurodegenerative diseases and is associated with poorer cognition. Higher baseline sST2 is a potential biomarker of disease severity in neurodegeneration.
INTRODUCTION
Neurodegenerative disease is the 5th leading cause of mortality worldwide according to the World Health Organization and its incidence has been increasing exponentially in part due to the rapidly aging global population [1–3]. Early detection of neurodegenerative diseases facilitates earlier intervention, delaying disease progression [1]. Thus, it is crucial to explore possible diagnostic biomarkers for neurodegenerative diseases.
The interleukin-33 (IL-33)/Suppressor of tumorgenicity 2 (ST2) system is primarily involved in inflammatory conditions such as asthma, pulmonary fibrosis, and autoimmune diseases [4, 5]. ST2 and IL-33 are highly expressed in the central nervous system (CNS), where IL-33 is expressed in oligodendrocytes [6] and ST2 is expressed mainly in microglia and astrocytes [7]. ST2 is a member of the Toll-like/IL-1-receptor super-family. ST2 ligand (ST2L) binds to IL-33, which in turn induces the Th2 immune response, leading to polarization of microglia toward an anti-inflammatory M2 phenotype [6]. Several studies have suggested that the IL-33ST2 system may be implicated in neurodegenerative diseases [8, 9]. IL-33 can induce regulatory T cells (Treg) to produce anti-inflammatory cytokines, which have been reported to alleviate cognitive decline in an AD mouse model [10]. In contrast, soluble ST2 (sST2) acts as a decoy receptor for IL-33, attenuating the neuroprotective Th2 inflammatory response [5]. The imbalance between the TH1 and TH2/Treg can promote the production of pro-inflammatory cytokines and exacerbate neurodegeneration [11, 12].
ST2 is highly expressed throughout the hippocampus [13]. Neuronal IL-33 augments hippocampal synaptic plasticity and induces microglial phagocytosis of the extracellular matrix, which regulates synapse remodeling and memory formation [14]. Blockade of IL-33/ST2 signaling in vivo by intracerebroventricular administration of sST2 inhibits homeostatic synaptic plasticity in hippocampal CA1 neurons and impairs spatial memory formation in mice [15]. The binding of IL-33 to ST2L triggers downstream signaling pathways that result in clearing of Aβ plaques and rescue of the AD phenotype [5, 16]. In mouse AD models, high sST2 was associated with amyloid plaque accumulation, with administration of IL-33 showing rescue of AD phenotype and improvement in cognitive performance by microglia/macrophages [8, 17].
Single nucleotide polymorphisms (SNPs) within IL-33 are associated with Alzheimer’s disease (AD) risk in Caucasian and Han Chinese. Patients with mild cognitive impairment (MCI) and AD showed lower IL-33 and higher sST2 levels compared to healthy controls [18]. Patients with higher IL-33 expressing cells preserved their cognitive function and hippocampal volume, compared with IL-33 non-expressing patients [19, 20]. However, whether peripheral sST2 levels correlates with cognitive function, disease state and/or severity remains unclear.
To address this gap, this study aimed to investigate plasma levels of sST2 across neurodegenerative diseases compared to healthy controls (HC) and to assess the association between sST2 levels and cognitive and motor scores.
MATERIALS AND METHODS
Subject cohorts
Data was collected from the National Neuroscience Institute, Singapore between 2018 and 2021. Consecutive patients suffering from the following neurodegenerative diseases including MCI, AD, frontotemporal dementia (FTD), and Parkinson’s disease (PD) and healthy controls (HC) were included. Diagnosis of MCI status was based on criteria established by Petersen [21]. Diagnosis of AD status was based on criteria established by the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS) and the Alzheimer’s Disease and Related Disorders Association (ADRDA) [22]. Diagnosis of FTD was based on criteria established by Rascovsky [23]. Diagnosis of PD was based on the National Institute of Neurological Disorders and Stroke (NINDS) clinical criteria [24]. A total of 397 patients were included, consisting of 46 MCI, 38 AD, 28 FTD, and 194 PD subjects and 91 HC. Each participant underwent a standardized examination that included a medical evaluation, neuropsychological test, and clinical interview. Healthy controls were recruited from the community and were free of significant neurological, psychiatric, or systemic disease. Ethics approval was obtained from the Singapore Health Services Centralised Institutional Review Board (CIRB) for the use of human participants in this study and all participants provided informed written consent.
Clinical variables
Global cognition was assessed using the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) [25]. In the dementia cohort, the following neuropsychiatric tests were performed: Alzheimer’s Disease Assessment Scale-cognitive subscale (ADAS-Cog) [26], Frontal Assessment Battery (FAB) [27], Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV) digit span [28], Color Trails test [29], Rey–Osterrieth complex figure test [30], and Boston Naming Test [31].
In the PD cohort, detailed neuropsychiatric tests were carried out yearly for 4 years and data on the following domains were extracted including memory, visuospatial orientation, attention, language and executive function [32]. Motor severity was ascertained using the Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part III motor scores.
Soluble ST2 measurement
EDTA blood was centrifuged at 1,800 g for 10 min within 1 h after collection. Plasma was aliquoted and stored at –80°C until use. Cerebrospinal fluid (CSF) samples were also collected from 22 patients in a similar manner. sST2 was measured in plasma and CSF using Human ST2 Quantikine ELISA (R&D Systems), according to the manufacturer’s protocol. Coefficient of variation (CV) of samples measured in duplicates was <20%.
Statistical analysis
Statistical analyses were performed using SPSS Version 26 (SPSS inc., Chicago, IL, USA). Baseline characteristics were compared between disease groups by analysis of variance (ANOVA) or using the Kruskal-Wallis test (depending on normality assumption) for continuous variables, and Chi-square test (or Fisher’s exact test, where appropriate) for categorical variables. Correlations between continuous baseline variables and sST2 levels were calculated using Spearman’s correlation coefficient. Plasma sST2 levels were log-transformed to account for the right skewed distribution for subsequent analysis. For group-wise comparisons of plasma sST2, we used univariate general linear models controlling for potential confounders (including age and gender) and least significant difference (LSD) post-hoc test, followed by the Bonferroni test. Multivariable linear regression was carried out to investigate the associations between plasma sST2 levels and cognitive and motor scores. In the PD cohort, linear-mixed modelling (LMM) was performed to investigate the association of sST2 levels with longitudinal trends in MMSE and individual cognitive domains, adjusted for age, gender, education, and APOE4 genotype. In LMM, restricted maximum likelihood approach was used as the estimation method, with an autoregressive covariance structure and Kenward-Roger method for computing the denominator degrees of freedom for the tests of fixed effects. In this random intercept-only LMM, the beta coefficient (and 95% confidence interval) of the interaction of sST2×time was calculated. Due to the exploratory aim of the longitudinal portion of this study, no prior hierarchical hypothesis was pre-specified. p values <0.05 were considered statistically significant.
RESULTS
Baseline characteristics
Demographic information and clinical characteristics of the participants are presented in Table 1. A total of 397 patients (46 MCI, 38 AD, 28 FTD, 194 PD, and 91 HC) were included in this study. Overall, there was no significant correlation between age and education with sST2. However, males had significantly higher sST2 levels compared to females (p < 0.001). This was also seen in dementia patients (p = 0.008) and PD patients (p < 0.001). Within dementia patients, sST2 levels did not correlate significantly with age and education. Within PD patients, sST2 levels correlated significantly with age (rs = 0.151, p = 0.035), but not with education, disease duration and motor scores.
Demographic and clinical characteristics of all subjects at baseline
PD, Parkinson’s disease; HC, healthy control; LEDD, Levodopa Equivalent Dose; MDS-UPDRS, Movement Disorder Society Unified Parkinson’s Disease Rating Scale; H&Y stage, Hoehn and Yahr stage; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment aContinuous variables reported as mean±standard deviation; Categorical variables reported as frequency (%).
Plasma sST2 levels in neurodegenerative diseases and healthy controls
Plasma sST2 levels were significantly different across all neurodegenerative diseases (p < 0.001; Fig. 1A), controlling for age and gender. Within the dementia cohorts, post-hoc analysis revealed higher sST2 levels in AD (p = 0.002, Bonferroni corrected p = 0.012) and FTD (p < 0.001, corrected p < 0.001) versus HC. Higher sST2 levels were also seen in FTD versus MCI (p = 0.004, corrected p = 0.026), controlling for age and gender. There was no significant difference between AD versus FTD (p = 0.217, corrected p = 1.0). Within the PD cohort, plasma sST2 levels were significantly higher in PD versus HC (p = 0.041; Fig. 1B), controlling for age and gender. When the two cohorts were analyzed, higher sST2 levels were observed in AD versus PD (p = 0.034, Bonferroni corrected p = 0.338) and FTD versus PD (p = 0.001, Bonferroni corrected p = 0.007), correcting for age and gender. In a subset of 22 patients (6 MCI, 8 AD, and 8 FTD) with available CSF samples, plasma sST2 showed significant correlation with CSF sST2 levels (R-sq = 0.684, p < 0.001; Fig. 2).
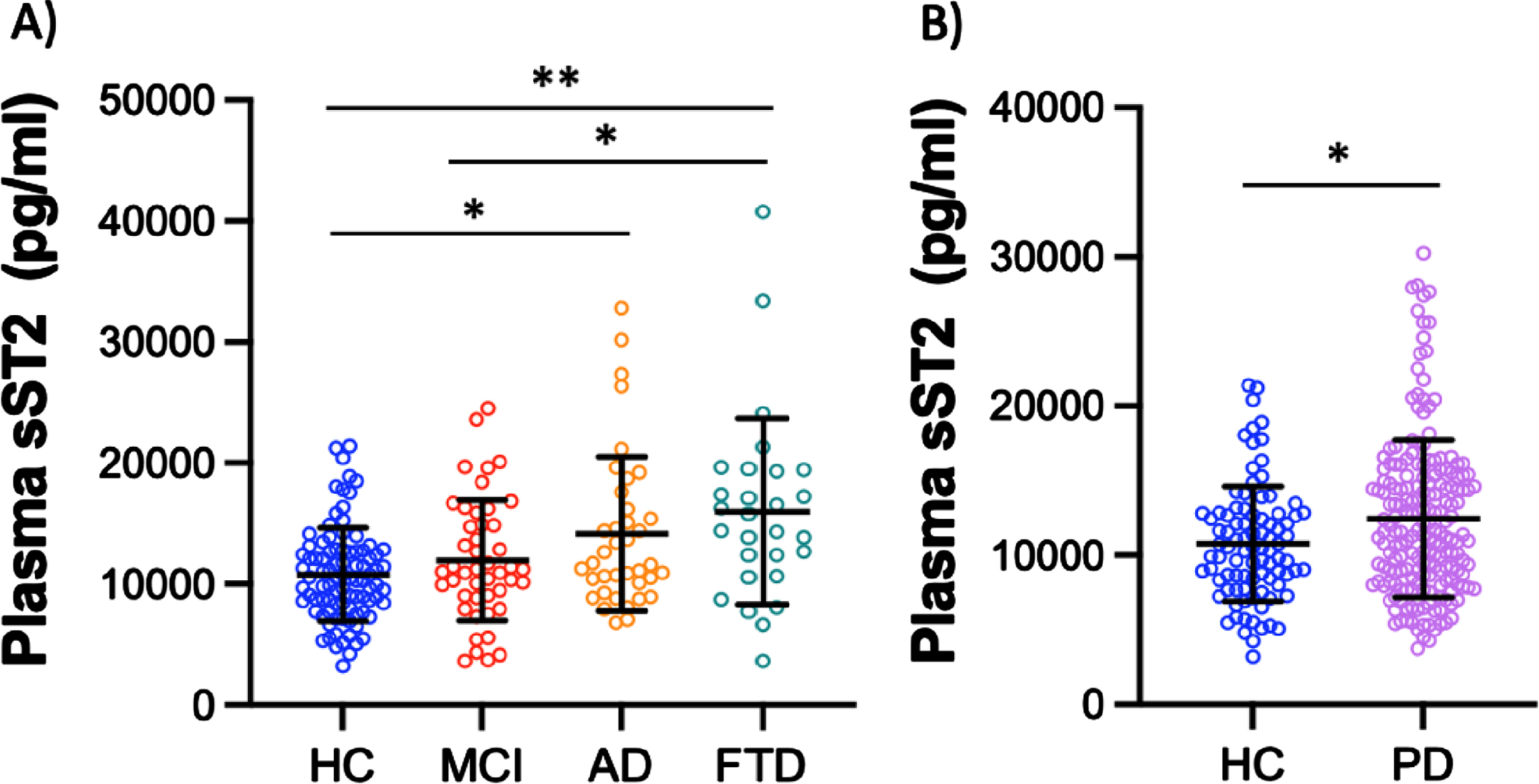
Plasma sST2 levels across disease groups A) In the Dementia cohort; B) In the early PD cohort *p < 0.05, **p < 0.01, p values are adjusted for age, gender, and multiple comparisons via Bonferroni.
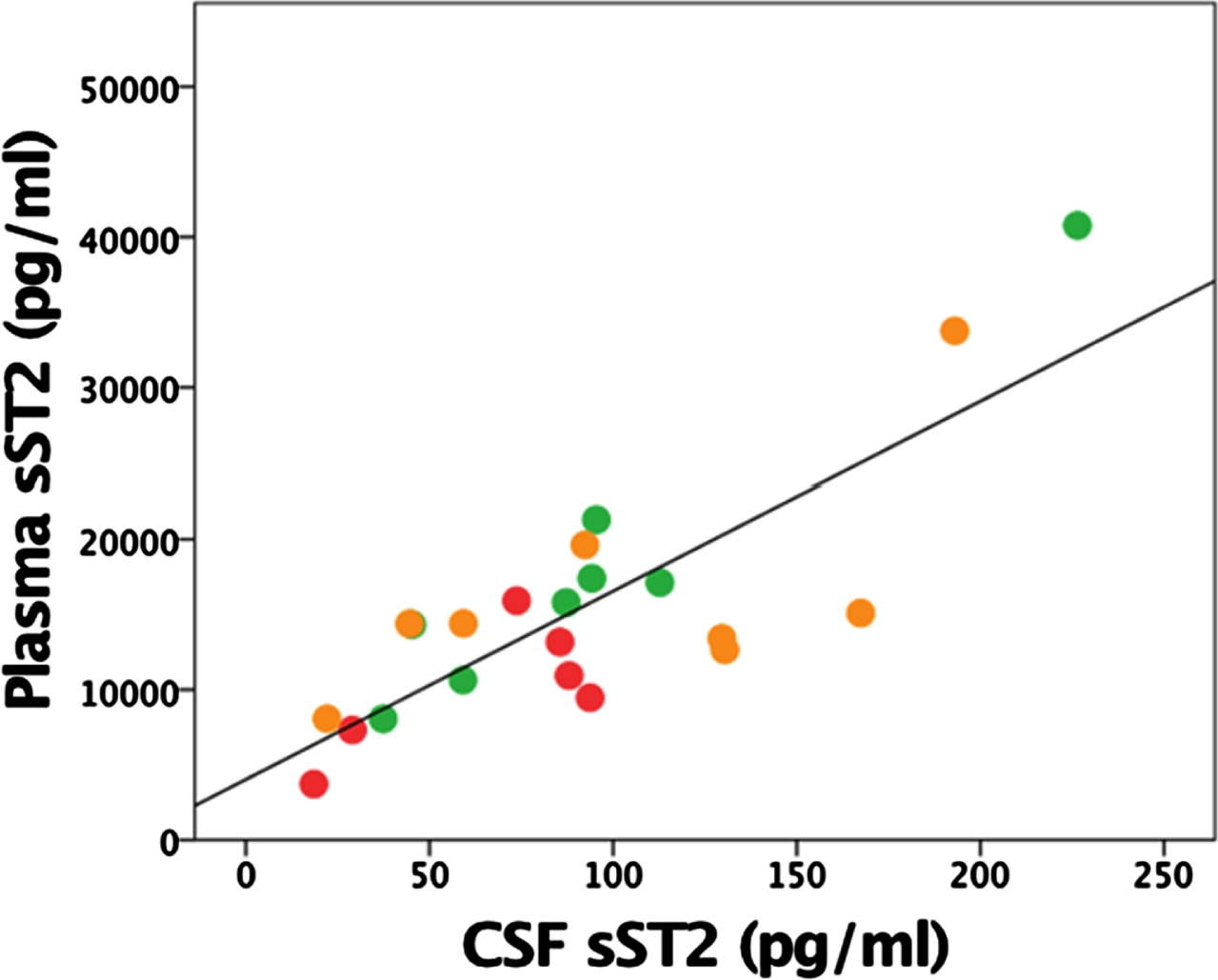
Plasma and CSF sST2 levels.
Association of plasma sST2 levels with cognitive scores in the dementia cohort
Among dementia patients, higher plasma sST2 levels were significantly associated with poorer digit span backward scores (β= –3.00, 95% CI = –5.73 to –0.27, p = 0.032), controlling for age, gender and education. Higher plasma sST2 levels also showed a trend towards poorer FAB scores, nearing significance (β= –4.65, 95% CI = –9.48 to 0.19, p = 0.059), controlling for age, gender, education and APOE4 carrier status. In a subset of 25 dementia patients with longitudinal scores (9 MCI, 8 AD and 6 FTD), plasma sST2 was significantly associated with worse MoCA scores at mean follow-up duration of 1.8 years (β= –12.87, 95% CI = –22.9 to –2.75, p = 0.015), controlling for age, gender, education, APOE4 carrier status, and baseline MoCA scores.
Association of plasma sST2 levels with cognitive and motor scores in PD cohort
In the PD cohort, sST2 did not show significant association with cognitive and motor scores; but in PD patients fulfilling MDS Task Force Level II criteria for PD-MCI [33] (n = 92); however, there was trend towards higher sST2 levels in PD-MCI versus HC (p = 0.048, Bonferroni adjusted p = 0.144), controlling for age and gender. We then looked at the association between sST2 and cognitive domains within the PD-MCI group and found that higher plasma sST2 levels significantly associated with worse attention (β= –1.043, 95% CI = –1.828 to –0.259, p = 0.010), controlling for age, gender, education, and APOE4 carrier status. Plasma sST2 was not significantly associated with other cognitive domains.
In PD patients with longitudinal scores, higher baseline plasma sST2 levels were associated with significant decline in MMSE scores as well as visuospatial domain performance over a 4-year follow-up, adjusted for age, gender, education, and APOE4 carrier status (Table 2). Within PD-MCI patients, there was a trend of greater decline in visuospatial and executive domain performance over 4 years.
Multivariable analysis of baseline plasma sST2 levels with cognitive measures in PD patients over time
Adjusted for age, gender, education, APOE4 Linear Mixed Model analysis: interaction of biomarker x Year versus longitudinal outcome.
DISCUSSION
In this study, we report for the first time that plasma sST2 levels are higher across various neurodegenerative diseases including AD, FTD, and PD compared to MCI and HC. Additionally, higher plasma sST2 levels are associated with poorer cognitive scores in the dementia and PD groups, especially in the cognitive domains of working memory, executive and visuospatial function. This presents sST2 as a candidate biomarker not only of disease state but also cognitive dysfunction across the most common neurodegenerative diseases.
The involvement of immunomodulatory cascades in the pathophysiology of neurodegenerative diseases, particularly AD, have been widely established in literature [34, 35]. In recent years, studies have emerged revealing the IL-33/ST2 pathway as an important component of the immunomodulatory cascade [13, 36–39], including in neuroinflammation and AD [4, 40]. Three single nucleotide polymorphisms (SNPs), rs1157505, rs11792633, and rs7044343, within IL-33 have also been associated with AD risk in a Caucasian cohort [40]. These SNPs were further evaluated in Han Chinese, with the IL-33 rs11792633 polymorphism significantly associated with a reduced risk of late onset AD (LOAD) in patients and the T allele as a protective factor for LOAD [41, 42].
There are two isoforms of ST2, namely transmembrane (ST2L) and soluble (sST2) [5]. ST2L is a receptor for IL-33 [43]. IL-33 binds to ST2L, triggering downstream signaling pathways that result in clearing of Aβ plaques and rescue of the AD phenotype [5]. On the other hand, sST2 is a decoy receptor for IL-33 as it binds competitively to IL-33, preventing the IL-33/ST2L interaction, attenuating neuroprotective effects of IL-33 and resulting in an accumulation of misfolded proteins [5] and potentiation of the AD phenotype [8]. In mouse AD models, higher levels of sST2 were associated with accumulation of amyloid plaques and potentiation of AD, with administration of IL-33 showing rescue of AD phenotype and improvement in cognitive performance by microglia/macrophages [8, 17]. Another study observed that mice lacking IL-33 developed AD pathology with tau abnormality and neurodegeneration in the cerebral cortex and hippocampus, accompanied with cognitive impairment [44].
A more subtle form of neuroinflammation is also present in MCI, defined as having an objective decline in cognitive performance not meeting criteria for a dementia diagnosis [22]. In MCI pathophysiology, studies have demonstrated the involvement of the IL-33/ST2 pathway [18] and illustrated its effect on cognition [19] where patients expressing IL-33 preserved their cognitive function compared with IL-33 non-expressing patients [19]. Another study showed that MCI patients who did not convert to AD had higher IL-33+ cells correlating with better preserved hippocampal volumes compared to AD converters [20]. IL-33 has been found to be significantly decreased in the serum and CSF of AD and MCI cases, while sST2 was increased in the serum of AD and MCI cases [18], supporting the hypothesis that IL-33 plays a complex anti-inflammatory role that is attenuated in AD- and MCI-associated neuroinflammation. Decreased circulating IL-33 levels in AD might be attributed to the increased decoy receptor sST2 in the blood of AD patients [18]. Additionally, the IL33/ST2 pathway has also been implicated in behavioral changes in both human [45] and murine [46] models. Mice lacking in IL-33 were found to develop several behavioral deficits including impaired social recognition [46]. In humans, IL-33 levels were affected in affective disorders such as depression and bipolar disorder [45]. Highest levels of sST2 were seen in our FTD cases, most of whom were of the behavioral variant FTD subtype, presenting with prominent behavioral and neuropsychiatric impairment.
Our study is the first to explore the effect of the IL-33/ST2 axis in PD, and we demonstrated a trend towards higher sST2 levels in PD patients with MCI. Plasma sST2 was also associated with worse attention domain at baseline and decline in global cognition, visuospatial and executive functions over time, which are domains known to be affected in PD [47–49]. PD is characterized by an accumulation of Lewy bodies in the brain parenchyma and degeneration of midbrain dopaminergic neurons [50]. PD murine models have shown higher levels of IL-33 in astrocytes in the midbrain and striatum compared to age-matched controls [51, 52], but the corresponding levels of sST2, were not explored in that study. In vitro studies have shown that 1-methyl-4-phenylpyridinium (MPP+), a metabolite of the parkinsonian neurotoxin 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP), induces IL-33 release from astrocytes [52]. A high level of plasma sST2 would act as a decoy receptor and mitigate the effects of the rise in IL-33, inhibiting the IL-33/ST2 axis and possibly resulting in the motor and cognitive symptoms characteristic of the PD phenotype [51]. Therefore, while IL-33 administration could be a potential therapy for AD, the role of IL-33 in PD and PD-MCI remains to be further investigated.
The neuroprotective role of IL-33 has been supported by numerous preclinical studies. Our study demonstrating higher levels of sST2 across various neurodegenerative diseases adds to existing evidence that the IL33/ST2 pathway is implicated in their pathogenesis and may yield new therapeutic options for AD, FTD and PD. Strengths of this study include the fact that this is the first report of sST2 as a potential biomarker in FTD and PD. Additionally, we were able to show significant correlation of plasma with CSF sST2 levels in patients who had corresponding CSF sST2 levels measured. This is important given the more accessible nature of blood compared to CSF biomarkers.
Conclusion
Overall, higher levels of sST2 were seen across MCI, AD, FTD, and PD compared to controls, making sST2 a potential biomarker for neurodegenerative diseases. Higher baseline sST2 is associated with worse cognitive function and is a potential biomarker of disease severity, particularly in neurodegeneration. These results suggest that impaired IL-33/ST2 signaling may play a role in the pathophysiology of neurodegenerative disorders. Future studies involving larger dementia sample sizes are recommended to validate our findings.
Footnotes
ACKNOWLEDGMENTS
The authors thank our patients and their families for their valuable contribution to the study.
FUNDING
This study was funded by Singapore’s National Medical Research Council (ASLN by the Clinician-Scientist New Investigator Grant (CNIG/1165/2017) and Transition Award (MOH-TA18may-0003); EKT and LCST by the Open Fund Large Collaborative Grant (MOH-OFLCG18May-0002)). This study (IS) is funded in part by the SingHealth Medical Student Talent Development Award.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Anonymized data that support the findings of this study are available from the corresponding author upon reasonable request.