
Abstract
Background:
Auditory event-related potentials (AERPs) have been suggested as possible biomarkers for the early diagnosis of Alzheimer’s disease (AD). However, no study has investigated AERP measures in individuals with subjective memory complaints (SMCs), who have been suggested to be at a pre-clinical stage of AD.
Objective:
This study investigated whether AERPs in older adults with SMC can be used to objectively identify those at high risk of developing AD.
Methods:
AERPs were measured in older adults. Presence of SMC was determined using the Memory Assessment Clinics Questionnaire (MAC-Q). Hearing thresholds using pure-tone audiometry, neuropsychological data, levels of amyloid-β burden and Apolipoprotein E (APOE) ɛ genotype were also obtained A classic two-tone discrimination (oddball) paradigm was used to elicit AERPs (i.e., P50, N100, P200, N200, and P300).
Results:
Sixty-two individuals (14 male, mean age 71.9±5.2 years) participated in this study, of which, 43 (11 male, mean age 72.4±5.5 years) were SMC and 19 (3 male, mean age 70.8±4.3 years) were non-SMC (controls). P50 latency was weakly but significantly correlated with MAC-Q scores. In addition, P50 latencies were significantly longer in Aβ+ individuals compared to Aβ– individuals.
Conclusion:
Results suggest that P50 latencies may be a useful tool to identify individuals at higher risk (i.e., participants with high Aβ burden) of developing measurable cognitive decline. Further longitudinal and cross-sectional studies in a larger cohort on SMC individuals are warranted to determine if AERP measures could be of significance for the detection of pre-clinical AD.
Keywords
INTRODUCTION
Dementia continues to be a growing global issue, with an estimated 57 million people living with dementia in 2019 [1]. This estimate is projected to more than double to 152 million by 2050, if there is no medical breakthrough [1]. Dementia due to Alzheimer’s disease (AD) pathology is the most common form, accounting for 60–80% of all dementia cases [2]. AD is defined by pathological features, including extracellular amyloid-β (Aβ) deposition which is the core protein component of senile plaques, and hyperphosphorylated tau protein which results in the formation of neurofibrillary tangles within neurons [3, 4]. AD neuropathological features and associated neurodegenerative changes lead to synaptic loss, neuronal damage, imbalances in neurotransmitters and finally, manifest into the clinical cognitive symptoms of AD [3, 5]. Clinical symptoms of AD are characterized by a decline in episodic memory function, visuospatial orientation, attention and language as well as impaired daily living activities [3, 6]. The development of AD is slow and progressive, with the neurodegenerative changes beginning up to 20 years or more before symptom onset [7 –10].
New developments in therapeutic strategies for the treatment and prevention of AD highlight the need for early diagnosis of high risk individuals [11]. Earlier stages in the course of AD have the potential to define a target population for AD intervention, as treatments at later stages of the disease have shown little promise in altering the disease course, because substantial neuronal injury and cognitive impairment are already present [12]. Earlier stages of AD clinical spectrum include mild cognitive impairment (MCI) which is usually preceded by subjective cognitive decline (SCD). MCI due to AD is characterised by impairment in cognition and the presence of AD pathology in the absence of major problems with daily living activities [6, 13]. SCD refers to self-reported decline in cognitive function without convincing evidence of objective impairment on cognitive assessments and with preserved function in daily living [14]. Those with SCD are considered to have increased risk of developing cognitive decline which can progress to AD [15 –18]. Biomarkers that target these stages, i.e., the pre-clinical (SCD) and prodromal (MCI) stages of AD, have become critical in facilitating early detection and treatment intervention with a view to alter the diseasecourse. Auditory event-related potentials (AERPs), which present as distinct peaks at different latencies, represent neural activity from different anatomical stations along the auditory pathway and associated brain regions [19]. AERPs have been suggested as non-invasive, cost-effective biomarkers for the early diagnosis of AD, and may be of use for first-line screening to identify high-risk individuals that would normally be investigated using less accessible and relatively expensive (positron emission tomography (PET) or volumetric magnetic resonance imaging) or invasive (lumber puncture for cerebrospinal fluid) diagnostic methods [20 –23]. AERPs have been found to reflect auditory memory [24, 25], attention [24, 26], working memory [24, 27], language comprehension [28, 29], discrimination [30], and decision-making [31].
Previous research investigating AERPs has focused on those with MCI [21 , 32–34], and AD [22 , 36]. These studies suggest that AERP latencies can differentiate between those with AD-related cognitive impairment and healthy age-matched controls, showing that P50, N100, P200, N200, and P300 latencies are significantly longer in AD participants and P300 latency is significantly longer in MCI participants when compared to age-matched controls [37]. However, to date, no study has investigated AERP measures in individuals with subjective memory complaints (SMCs) [37]. SMCs include self-reported concerns about memory, which is a major component of SCDs and has been associated with increased risk of developing AD [38]. SMCs are part of the criteria for multiple prominent diagnostic systems for the intermediate period between normal cognitive aging and dementia, including MCI [39] and age-associated memory impairment [40]. Investigating AERP measures in those with SMC, validated against the gold standard, could aid in identifying people at higher risk of developing dementia, years before the appearance of clinical symptoms of AD [14].
Furthermore, psychological factors, such as depression and social isolation, have also been suggested to be risk factors for dementia [41, 42]. In fact, depression is proposed to be an autonomous symptom of prodromal AD [7]. Additionally, people with hearing loss have higher depression, anxiety and stress rates than those with normal hearing [43], with the co-occurrence of hearing loss and depression further increasing the risk of developing dementia due to AD [7, 43]. Other risk factors of AD include having untreated hearing loss [7], carrying Apolipoprotein E (APOE ɛ4) and having abnormal (high) level of Aβ as measured by Aβ PET [44]. The aim of this paper was to investigate AERP measures in older adults with and without SMC using a standard two-tone auditory oddball design, in order to determine if these auditory measures can provide useful information to objectively identify those at high risk of developing AD in conjunction with more readily accessible specific AD biomarkers. AERPs were compared with participants’ pure-tone audiometry (PTA), neuropsychological data (including depression, stress, and anxiety levels), brain amyloid levels and APOE ɛ4 genotype.
METHODS
Study participants
Sixty-two community-dwelling (non-help-seeking) older adults were recruited from the Western Australia Memory Study (WAMS), an ongoing longitudinal study on aging and dementia. This study received its ethical approval (HPH-139) from the University of Western Australia, Edith Cowan University and Ramsay Health Care WA | SA Human Research Ethics Committee (previously known as, Hollywood Private Hospital) in Perth Western Australia. All procedures were undertaken in accordance with ethics approval. Participants in this study provided informed consent prior to taking part in this study. Cognitive and psychological assessments were performed by a qualified psychometric rater who was trained and certified by the study neuropsychologists. Hearing assessments were conducted by a trained researcher and neuroscientist under the supervision of a qualified audiologist. Participants had no history or current diagnoses of severe psychiatric, neurological or neurodegenerative disorders/diseases.
Neuropsychological and psychological assessments
All participants (n = 62) completed comprehensive neuropsychological and psychological assessments as part of the WAMS. Self and informant report surveys and questionnaires were attained to assess psychological, cognitive and personality characteristics of participants. The WAMS test battery assesses global cognition, memory (short term and working memory), attention, language, executive functions, concentration, orientation, and visuospatial skills. For this study, cognitive and psychological measures included the Montreal Cognitive Assessment (MoCA), Memory Assessment Clinics Questionnaire (MAC-Q), and Depression Anxiety Stress Scales (DASS-21). More information on the neuropsychological and psychological assessments used in the WAMS can be found in Sohrabi et al. [45].
Participants were divided into two groups: a non-SMC (control) and SMC (high-risk) group based on the MAC-Q [46], a self-reported survey scores. The MAC-Q is a 6-item scale designed to capture self-reported concerns of age-related memory decline relative to the respondent’s own baseline at age 20 years. The first 5 items are about specific daily activities that are frequently reported as troublesome among those with age-related memory loss and the final (6th) item is a global item assessing overall decline in memory. Participants are asked to rate all 6 items on a 5-point Likert scale ranging from 1 being “much better now” and 5 being “much poorer now”. An overall index of cognitive decline is calculated by summing scores for all 6 MAC-Q items, with double weighting for item 6. Total score on the MAC-Q can range between 7 and 35, with higher MAC-Q scores indicating greater decline in memory. Participants with an overall MAC-Q score of 25 or more are considered to have SMC.
Amyloid-β imaging
Thirty-seven of the 62 participants underwent an amyloid-β positron emission tomography (Aβ PET) which was conducted for 20 min, 50 min post injection of [18F]-NAV4694. Aβ PET were quantified in Centiloid (CL) using CapAIBL [47 –49]. A CL threshold of 20 was set for Aβ abnormality in accordance with post-mortem data [49, 50]. Participants with CL >20 (resp. CL <20) were categorized as Aβ+ (resp. Aβ–).
Genotyping
Whole blood samples were collected from 49 participants. APOE ɛ4 genotype was determined from DNA extracted from the whole blood sample using genotyping assays performed on Real-Time-PCR systems. APOE ɛ4 carriers were defined as participants with a minimum of 1 ɛ4 allele (i.e., ɛ2/ɛ4, ɛ3/ɛ4, ɛ4/ɛ4) and non-carriers as participants with no copies of the ɛ4 allele (i.e., ɛ2/ɛ2, ɛ2/ɛ3, ɛ3/ɛ3). More information on the APOE genotyping methods used in the WAMS can be found in Sohrabi et al. [51].
Pure-tone audiometry
All participants underwent an otoscopic and a pure-tone audiometric examination. Only participants with normal otoscopic findings were included in the study. Bilateral pure tone audiometry was conducted (air-conduction and bone-conduction) at 0.5, 1, 2, 4, and 8 kHz using the KUDUwave 5000 system, Type 2 clinical audiometer (Emoyo, Johannesburg, South Africa). Tones were presented via insert earphones inserted in the ear canals with circumaural headphones placed over the ears. An automated threshold-seeking paradigm was used to establish hearing thresholds. At each frequency, threshold levels were determined with increasing increments of 10 dB followed by decreasing increments of 5 dB [52]. Participants were required to press a button in response to any tones they heard during the assessment. 4PTA was calculated by averaging thresholds obtained at 0.5, 1, 2, and 4 kHz. Participants with preceding or inherent hearing related issues (e.g., moderate or severe hearing loss, unilateral hearing loss, and unclear otoscopy) were excluded from the study.
Auditory electrophysiological measures
Auditory electrophysiological recordings were performed in a darkened, sound attenuated and electrically shielded room using the Chartr EP system (Version 5.3, GN Otometrics). Participants were awake and seated in a relaxed Fowler’s position during testing. Ag/AgCl recording disc electrodes were placed on the scalp of the participants according to the international electrode system (IES) 10–20 system. Responses were recorded from a vertex (Cz) midline electrode site with a reference electrode on the mastoid ipsilateral to the ear the stimuli are presented to. A ground electrode was placed on the lower forehead. Prior to recording, the skin was prepared for electrode placement with a mild abrasive to obtain electrode impedances under 5 kΩ.
A target detection task using a classic two-tone discrimination (oddball) paradigm was conducted for all participants. Participants were required to listen to a sequence of tones presented via ER-3A insert earphones with a stimulus rate of 0.7 per second. Tones were presented at a clearly audible and comfortable level to the participant, between 60 dBHL and 80 dBHL, based on hearing acuity (PTA) and self-reported comfort level. The tones consisted of standard (non-target) tones (1 kHz) and rare (target) tones (2 kHz) presented in a pseudorandom order. The probability of presentation was 80% standard tones and 20% rare tones and a total of 300 tones were presented per trial (240 standard tones and 60 rare tones). Separate averages were automatically performed by the Chartr EP system software for the standard and rare stimulus conditions. A gain of 30k, a low-pass filter at 30 Hz and a high-pass filter at 1 Hz were used. To minimize artefacts and noise interference as a result of body movement, participants were instructed to close their eyes and stay still during the recording.
Two trials were conducted for each participant, one using a passive paradigm and the other using an active paradigm. In the passive paradigm, the participants were asked not to pay attention to the presented tones. In the active paradigm, the subjects were asked to listen for the rare (target) tones and quickly, but accurately, raise their index finger on their dominant hand when they heard the target. Which trial (passive or active) the subject did first was counterbalanced to reduce carryover effect or practice effect.
Peak latencies of the components were measured relative to the time of stimulus onset. The P50 ERP feature was defined as the maximum positivity between 40 and 80 ms post-stimulus, N100 was the maximum negativity between 80 and 160 ms and P200 the maximum positivity between 150 and 250 ms. N200 was defined as the maximum negativity between 175 and 250 ms that immediately preceded the large P300 wave. The P300 was defined as the maximum positivity between 250 and 600 ms. Testing and analyzing AERP data was performed blinded to the group the participants were allocated to (i.e., SMC versus non-SMC).
Statistics
Statistical analysis was performed using IBM SPSS Statistics, version 25.0 (IBM Corp, Armonk, NY). Based on the Kolmogorov-Smirnov Test and the Shapiro-Wilk Test the majority of the data in this study was normally distributed, therefore, parametric statistical analysis was used to compare cognitive (MoCA), psychological (DASS-21), 4PTA and AERP measures between SMC and non-SMC participants. Group comparisons were analyzed using a Welch’s t-test in order to account for unequal variance and sample size between the groups. A Welch’s t-test was also used to compare measures between APOE ɛ4 carriers and non-carriers. Pearson’s correlation analysis was used to investigate the relationship between cognitive, psychological, genetic and auditory measures. Pearson’s correlation coefficients were also used to assess the correlation of AERP measures between active and passive paradigms. Regression analysis was used to test if AERP latencies could predict Aβ burden (in CL) or if Aβ burden could predict cognitive outcomes when age, gender and genotype are controlled for. Regression analysis was also used to test if higher Aβ levels could predict worse cognitive outcomes (MAC-Q and MoCA scores) when factors such as age, gender and genotype were controlled for. The Benjamini-Hochberg procedure [53] was used to control for false discovery rate, therefore, all p-values presented have been adjusted accordingly. Data are reported as mean±standard deviations. A p-value of <0.05 was considered statistically significant.
RESULTS
Participant characteristics
Participant demographic information is reported in Table 1. A total of 62 participants (14 male and 48 female; mean age 71.9±5.2 (SD) years) took part in this study, of which, 43 (11 male and 32 female; mean age 72.4±5.5 years) participants scored ≥25 on MAC-Q (mean MAC-Q 28.7±3.1) and were therefore categorized as SMC. The remaining 19 participants (3 male and 16 female; mean age 70.8±4.3 years) scored <25 on MAC-Q (mean MAC-Q 20.3±4.8) and were categorized as non-SMC (controls). MoCA scores did not differ significantly between SMC (26.8±2.8) and non-SMC (27.9±1.8) groups. There was no statistical (p = 0.6) difference in years of education between SMC (14.3±2.6 years) and non-SMC participants (14.6±2.3 years). Both groups had bilateral 4PTA (average of 0.5, 1, 2, and 4 kHz) within normal hearing threshold limits (<25 dBHL) and statistical analysis revealed no significant difference between the non-SMC (22.3±7.3 dBHL) and SMC (24.1±9.3 dBHL) groups, p = 0.44. Additionally, 4PTA hearing thresholds in the left and right ear did not significantly differ between groups (SMC versus non-SMC) or within the groups (left versus right ear) (Table 1). Males (27.9±9.8 dBHL) had higher 4PTA (both ears combined) thresholds in comparison to females (22.3±8 dBHL); however, there was no statistical significance (p = 0.13). Similarly, 4PTA in the right and left ears were higher in males (right ear = 27.2±10.2 dBHL, left ear = 28.7±10.5 dBHL) than in females (right ear = 21.6±8.4 dBHL, left ear = 21.7±8.2 dBHL), though again this did not reach statistical significance, p = 0.13 and p = 0.11, respectively.
Characteristics of study participants
*significant. M, male; F, female; PTA, pure-tone audiometry; L, left ear; R, right ear; MAC-Q, Memory Assessment Clinics Questionnaire; MoCA, Montreal Cognitive Assessment; DASS, Depression Anxiety Stress Scales.
Psychological measures
Participants with SMC (2.6±2.3) presented with significantly higher depression scores in comparison to non-SMC (1.1±1.1) participants, t(59.8) = 3.5, p = 0.01, as based on DASS-21 and participant depression scores correlated moderately, and significantly with MAC-Q scores, r(61) = 0.5, p = 0.01, 95% CI [0.28, 0.72] (Fig. 1). There was no significant difference in anxiety and stress scores, based on DASS-21, between SMC and non-SMC participants, p > 0.05.
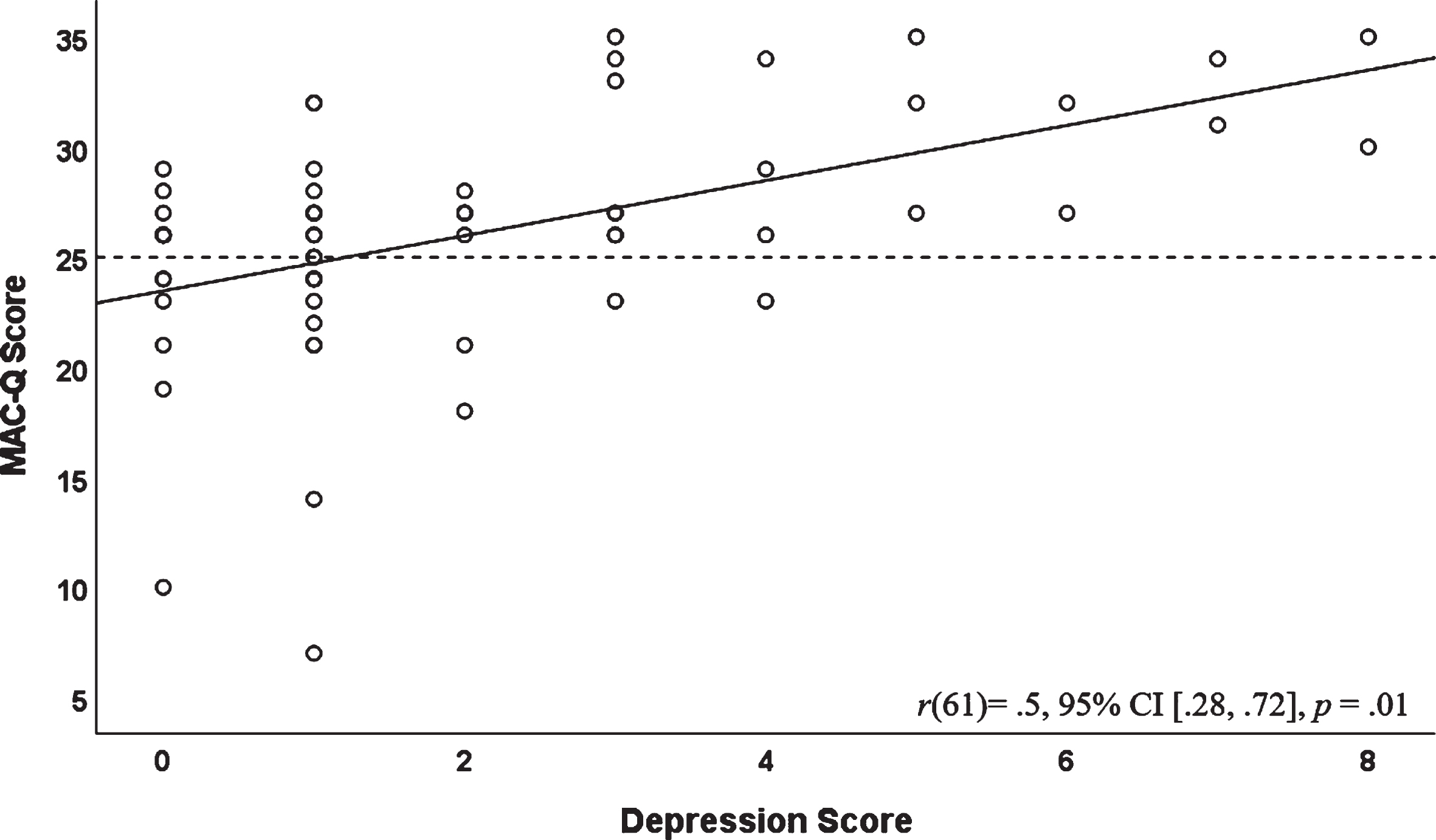
Correlation between MAC-Q scores and depression scores (based on DASS-21). Higher DASS-21 scores indicate higher levels of depression and stress. Solid line indicated line of best fit, dotted line indicates MAC-Q SMC cut-off score. Pearson’s correlation coefficients (r) and p-value and 95% confidence intervals (CI) are presented on the bottom right corner of each panel.
Auditory electrophysiological measures (AERPs)
AERP data are summarized in Fig. 2 and Supplementary Table 1. There were no significant differences in any of the AERPs between non-SMC and SMC groups in response to rare or frequent tones for both paradigms (Fig. 2). P50 (passive paradigm) and N100 (active paradigm) latencies in response to frequent tones were significantly correlated with age, r(62) = 0.33, 95% CI [0.08, 0.58], p = 0.03 and r(62) = 0.33, 95% CI [0.09, 0.57], p = 0.03, respectively (Fig. 3). There were no significant differences in AERP latencies between males and females. No significant differences in AERP latency measures were observed between SMC and non-SMC participants regardless of whether responses were elicited using active or passive paradigms. However, there was a weak, but significant, positive correlation between MAC-Q score and P50 latency in response to frequent tones using a passive paradigm, r(59) = 0.26, 95% CI [0.00, 0.5], p = 0.05 (Fig. 4). Latency of some AERPs also showed significant correlations with stress and/or anxiety scores, though again the correlations were weak. Specifically, P200 elicited in response to rare tones using an active paradigm correlated with stress score (r(60) = 0.26, 95% CI [0.01, 0.51], p = 0.05) and P300 in response to rare tones using a passive paradigm correlated with stress (r(61) = 0.3, 95% CI [0.06, 0.55], p = 0.03) and anxiety (r(61) = 0.28, 95% CI [0.03, 0.53], p = 0.04) scores (Fig. 5). There were no correlations between AERPs and depression. Comparisons between active and passive paradigms showed no significant differences in AERP measures except for P200 latency in response to rare tones (14.4±29.6 ms), (t(59) = 3.8, p = 0.01) (Table 2).
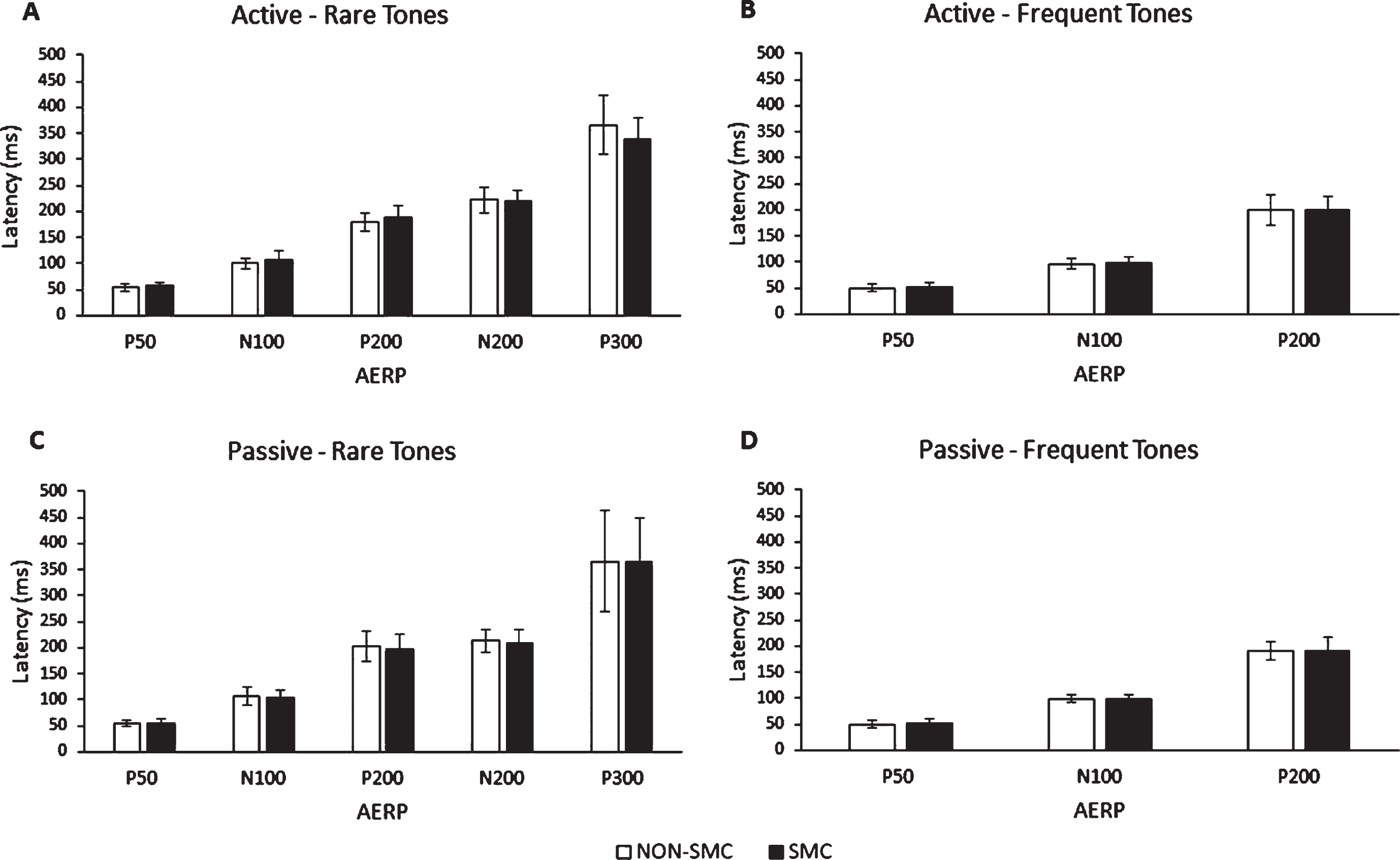
Latencies (Mean±SD) for the different AERPs for non-SMC (white) and SMC (black) groups in both passive and active paradigms. A) AERPs in response to rare tones in an active paradigm, B) AERPs in response to frequent tones in an active paradigm, C) AERPs in response to rare tones in a passive paradigm, and D) AERPs in response to frequent tones in a passive paradigm.

Correlation between AERPs (P50 and N100) and age. A) Correlation between age and P50 in response to frequent tones elicited using the passive paradigm, B) Correlation between age and N100 in response to frequent tones elicited using the active paradigm. Black line indicated line of best fit. Pearson’s correlation coefficients (r) and p-value and 95% confidence intervals (CI) are presented on the bottom right corner of the panel.
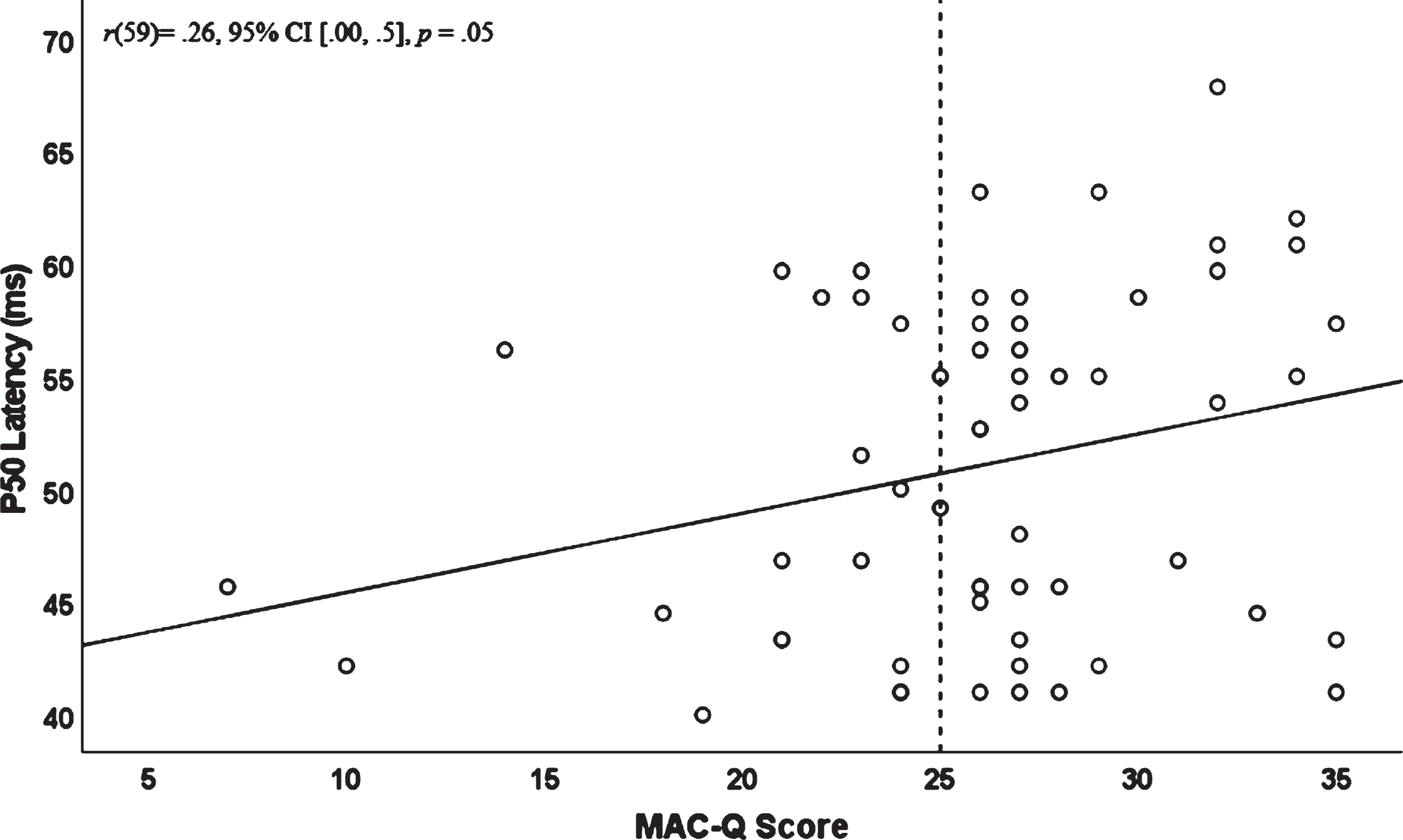
Correlation between MAC-Q score and P50 latency in response to frequent tones using a passive two-tone discrimination paradigm. Black line indicated line of best fit, dotted line indicates MAC-Q SMC cut-off score. Pearson’s correlation coefficients (r) and p-value and 95% confidence intervals (CI) are presented on the bottom right corner of the panel.
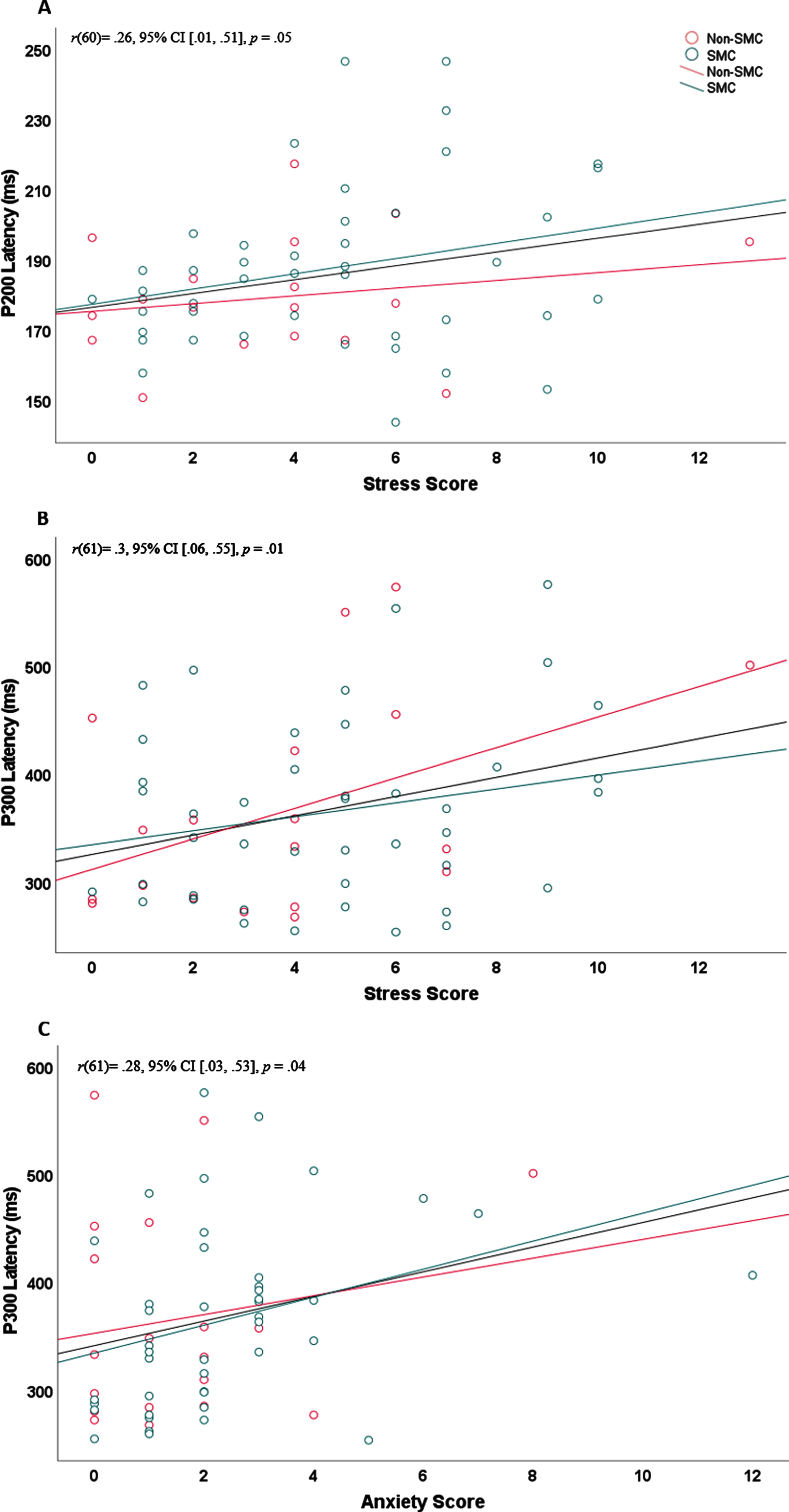
Correlation between participant AERP latency and psychological scores. Black line represents correlation line of best fit for the whole sample (both SMC and non-SMC participants combined), green line and dots represent SMC participants and red line, and dots represent non-SMC participants. A) P200 elicited in response to rare tones using an active paradigm correlation with stress score, B, C) P300 elicited in response to rare tones using a passive paradigm correlation with (B) stress and (C) anxiety scores. Pearson’s correlation coefficients (r) and p-value and 95% confidence intervals (CI) are presented on the top left corner of each panel.
Mean difference (milliseconds) in AERP measures between passive and active two-tone discrimination paradigms
NS, not significant.
APOE ɛ genotyping
Forty-nine of the 62 participants were tested for APOE ɛ4. Of these 49 participants, 14 were APOE ɛ4 carriers (3 male, 11 female, mean age 72.2±4.3 years) and 35 were non-carriers (24 male, 11 female, mean age 71.9±5.3 years). In total, 31.25% (5/16) of non-SMC and 27.27% (9/33) of SMC participants were APOE ɛ4 carriers. No significant difference was observed between APOE ɛ4 carriers and non-carriers on 4PTA, MAC-Q, MoCA, and DASS scores. AERP latencies of APOE ɛ4 carriers and non-carriers were not significantly different, p > 0.05. There were no significant differences in AERP latencies within SMC participants between APOE ɛ4 carriers (n = 8, mean age 73.7±4.1 years) and non-carriers (n = 24, mean age72.4±5.8 years).
Amyloid imaging (PET)
Thirty-seven of the 62 participants underwent amyloid imaging using PET, 12 of these participants (32%) (1 male, 11 female, mean age 73.1±5 years) were Aβ+. The remaining 25 participants that underwent amyloid imaging (67%) (6 male, 19 female, mean age 71.1±5.7 years) had normal Aβ levels (i.e., Aβ–). There were no significant differences in MAC-Q (t(31.1) = 1.1, p = 0.35) or MoCA (t(13.5) = 1.3, p = 0.29) scores between Aβ+ and Aβ– individuals. However, Aβ+ participants had significantly longer P50 latencies elicited in response to rare tones using a passive paradigm (n = 12, 57.4±6.4 ms) in comparison to Aβ– participants (Passive: (n = 23, 51±6 ms), t(21.3) = 2.9, p = 0.05, although there was no significant difference in P50 latency between Aβ+ (n = 10, 58.5±3.3 ms) and Aβ– (n = 25, 53.6±7.7) when elicited using active paradigm, t(32.6) = 2.6, p = 0.06) (Fig. 6). There was no significant difference in CL value observed between SMC (n = 23) and non-SMC (n = 14) groups (p > 0.05). Regression analysis revealed that Aβ levels were predictive of cognitive scores, including; MAC-Q (R 2 = 0.1, F(1,30) = 4.8, p = 0.038) and MoCA (R 2 = 0.18, F(1,30) = 8.1, p = 0.02), but none of the AERP latencies significantly predicted CL values (p > 0.05).
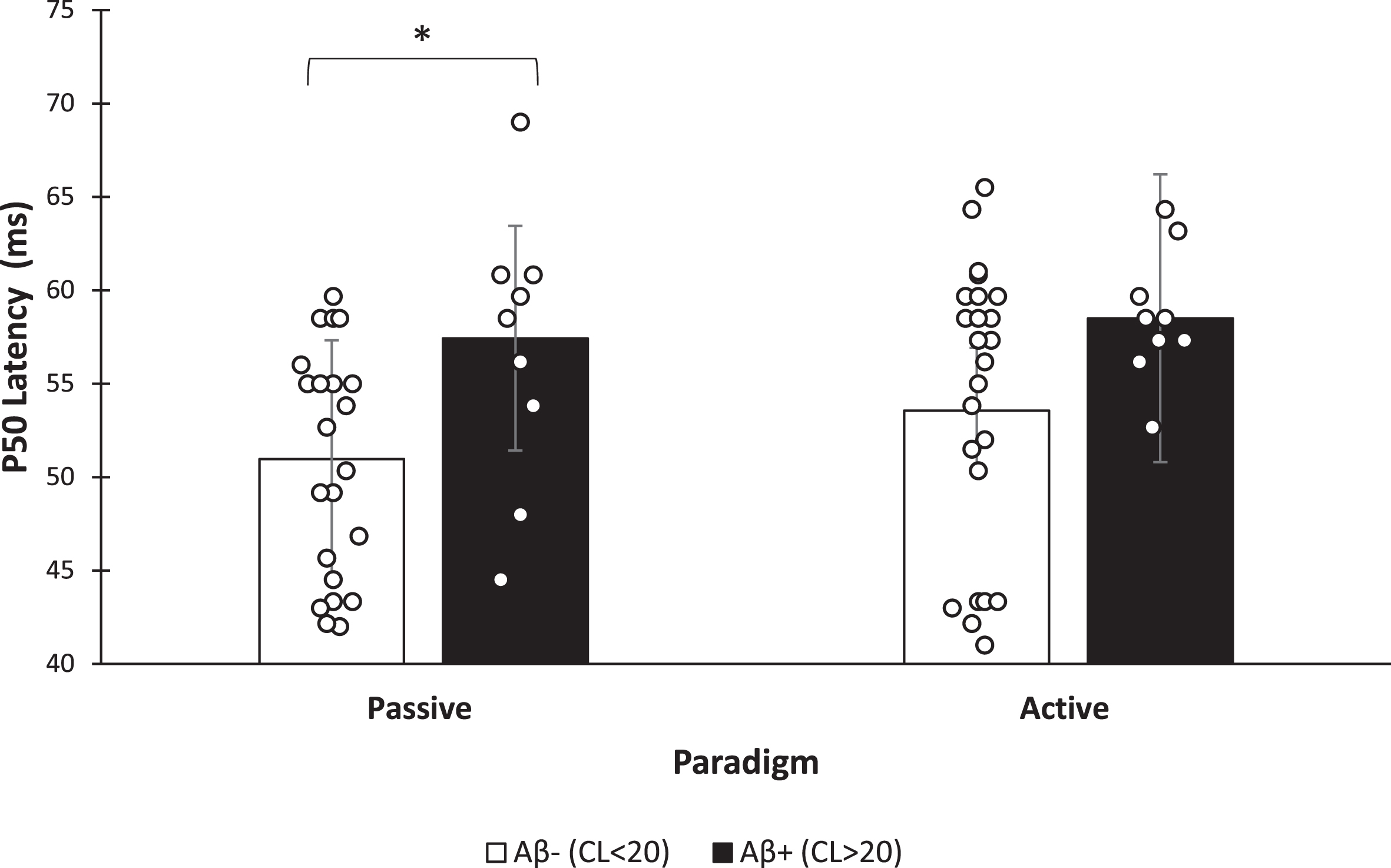
Mean P50 latency (ms) differences between Aβ+ (n = 12) (black bars) and Aβ– (n = 25) (while bars) groups. Bars indicate group average and scatter plots indicate individual P50 latencies for amyloid positive and amyloid negative participants using both passive and active paradigms. Error bars indicate standard deviation. CL, Centiloid. * p < 0.05.
DISCUSSION
In this study, we investigated the associations between AERPs, PTA, neuropsychological data, Aβ burden and APOE ɛ4 genotype in older adults with SMC in comparison to age-matched adults without SMC. Participants with SMC had significantly higher depression scores than non-SMC participants and there was a significant correlation between MAC-Q and depression. There were no significant differences in 4PTA or AERP latencies between SMC and non-SMC participants. Higher Aβ levels were significantly associated with lower cognitive outcomes (MAC-Q, and MoCA scores). Participants with abnormal level of Aβ (CL >20) had significantly longer P50 latencies when compared to Aβ– participants. In addition, P50 latency was weakly but significantly correlated with MAC-Q scores.
Passive versus active two-tone oddball paradigms
The two-tone oddball paradigm is often employed as an active task in which participants must indicate (either behaviorally or by counting) that a target tone has been perceived [54]. AERPs elicited using an oddball paradigm are typically based on models which assume active task participation [54, 55]. However, paradigms that elicit AERPs without needing active discrimination responses from participants could permit the mental assessment of uncooperative populations and the assessment of auditory information processing without the need of a secondary task [55]. This study is the first to compare the active and passive oddball paradigm in older adults and our results show that only P200 latencies were significantly different between the two paradigms, whereas all other latencies investigated were the same between the paradigms. These data are in broad agreement with previous research on young adults [55, 56] and children [57 –59] which showed that P300 waves obtained with the passive and active discrimination tasks are morphologically the same, with the same scalp distributions. Our data suggest that the passive two-tone discrimination paradigm can be used to elicit some AERP components (P50, N100, N200, and P300) in older adults in which the active discrimination paradigm cannot be performed. It should be noted that the results from this study do not incorporate amplitude data, meaning that the similarity between the responses from the passive and active paradigms seen in this study are true for AERP latency only.
Psychological factors and cognition
Similar to previous research [60 –62], SMC participants in this study had significantly higher depression scores compared to non-SMCs. Studies have reported a strong correlation between SCD/SMC and depression [14 , 64], with SCD/SMC being a primary complaint among older adults with depression [65]. It remains as yet to be resolved whether older adults with a depressed mood are more likely to report SMCs [66], or alternatively, whether depression could be caused by an awareness of cognitive decline [67]. Nonetheless, it has been suggested that the identification of co-occurring depressive symptoms and SCD could be a useful recruitment strategy to identify those at higher risk of developing dementia [15]. This is supported by a recent study that found that the co-occurrence of depression and SCD resulted in a higher incidence of MCI and dementia within 7.2 years [68].
AERPs and cognition
The results from this study indicate that AERP latencies are not different between SMC and non-SMC participants. However, many of the non-SMC participants were close to the MAC-Q cut-off score of 25 for SMC, which may be a contributing factor to this lack of effect seen in AERP latency and future studies may benefit from inclusion of a control (non-SMC) group with lower MAC-Q scores. In view of the limited spread of scores in the MAC-Q, correlations between AERPs and MAC-Q scores were also investigated, as they do not rely on cut-off scores but rather compare across the study population. This analysis showed that P50 latencies were significantly correlated with subjective memory complaints, measured as MAC-Q score. The P50, also known as P1 or P100 [69], is suggested to reflect sensory gating, that is, the biological substrates that preserve the integrity of cognitive function by filtering irrelevant information before reaching higher-order structures [70 –73]. The inhibition of redundant information is considered a precondition for efficient cognitive processing and impairment in this function could be a marker for cognitive impairment [74].
When elicited using a paired-click paradigm, P50 sensory gating has been suggested to represent protective mechanisms that, when impaired, can lead to impaired cognitive functioning [70 , 75]. Although research into P50 in AD is limited, a study by Thomas et al. [74] found that AD participants had reduced sensory gating, determined using P50 amplitude in response to paired clicks, when compared to healthy age matched controls. The authors suggested that early inhibitory deficits are present in AD participants, and contribute to impairment in executive functions and working memory [74]. When elicited using an oddball paradigm, as in the current study, P50 is suggested to reflect stimulus classification speed, and has been found to have a higher amplitude in MCI participants compared to healthy age-matched controls and importantly, in MCI participants who converted to dementia compared to those who did not convert [76]. Furthermore, P50 amplitudes were found to be significantly higher in AD participants and high risk participants who had at least one first-degree relative with AD, indicating increased sensitivity to incoming stimuli [77]. Our data are in line with the results described above and suggest that an increased degree of subjective memory complaints is accompanied with impaired sensory classification and sensory gating as reflected by longer P50 latency.
AERPs and APOE ɛ
Individuals with subjective concerns about memory and cognition that are also carriers of the major genetic risk of AD (i.e., APOE ɛ4) show increased cerebral amyloid and abnormal CSF amyloid and tau levels and are at higher risk of being at the preclinical stage of AD when compared to individuals with similar concerns but who are not APOE ɛ4 carriers [78, 79]. APOE ɛ4 genotype and SMCs combined have also been suggested to predict a greater risk of further cognitive decline than the two independently [80]. Our data show that SMC individuals carrying the high-risk AD genetic genotype (i.e., APOE ɛ4) do not differ in AERP latency from non-carriers. Furthermore, in this study there was no significant difference observed between APOE ɛ4 carriers and non-carriers on cognitive measures (i.e., MAC-Q, MoCA) or psychological measures (DASS), and not all APOE ɛ4 had SMC. A small sample size, as discussed below, may have contributed to the lack of significance in AERP latencies and cognitive measures between APOE ɛ4 carriers and non-carriers. A longitudinal follow-up study on a larger sample of SMC or SCD participants that are also APOE ɛ4 carriers would be required to determine if AERP latencies can contribute to the diagnosis of pre-clinical AD.
AERPs, cognition, and Aβ burden
When controlling for age, gender, and APOE ɛ4 status, Aβ burden (as measured by Aβ PET imaging) has been found to significantly predict subjective memory complaints (MAC-Q) in the absence of measurable cognitive impairment. A meta-analysis of 64 studies representing 7,140 participants found that increased amyloid burden was associated with poorer cognitive performance in participants without MCI or dementia [81]. Additionally, cognitively normal participants with abnormal levels of Aβ are considered to have a 2.3-fold increased risk of developing MCI and 2.6-fold increased risk of developing AD in approximately 4 years [82]. Furthermore, participants with prodromal AD with abnormal level of Aβ have been found to exhibit a 1.9-fold increased risk of developing AD compared to those with normal Aβ levels [82]. Our results show that P50 latency is significantly longer in Aβ+ in comparison to Aβ– participants with no symptomatic cognitive impairment. As elevated brain amyloid is a key biomarker of AD pathology [83, 84], considering results from this study, longer P50 latency could be associated with higher brain amyloid and could be a potential additional tool for AD screening. More research is required to understand the correlation of prolonged P50 latency with PET brain amyloid positivity and to further determine the usefulness of P50 in distinguishing those with high amyloid burden from those with low amyloid burden, i.e., those at high risk from those at low risk of AD. Furthermore, although gender was controlled for when conducting statistical analysis, it should be noted that most participants that underwent Aβ PET imaging in the current study were female, i.e., 30 females and 7 males.
While a skewed sex ratio would not impact the findings from this study (as it was controlled for), future research could benefit by addressing this difference, as that the association between AERPs and Aβ burden with respect to gender could be investigated.
Study limitations and future directions
A challenge to current research in the SCD field is the fact that self-reported decline in memory, even if persistent, is a common experience with aging [85, 86]. Indeed, the current data in a cohort of 62 older adults show that although only a subset met the criteria for SMC, many of the non-SMC participants approached the MAC-Q cut off. Additionally, etiologies of subjective decline in cognition or memory are highly heterogeneous [14, 65]. Therefore, in populations with a lower risk for underlying AD pathology, SCD is unlikely to represent a pre-MCI and Pre-AD stage [87]. Pre-clinical AD is suggested to be present in help-seeking SCD individuals, recruited from clinical setting, rather than those who are recruited from the general population [87 –90]. Population based studies recruit participants at random and then systematically query cognitive concerns, whereas memory clinic participants are often self-referred as a result of spontaneously expressed cognitive concerns [87]. Recruitment and selection factors operating in different research settings provide an important reflection of the degree of underlying AD pathology. A study by Perrotin et al. [91] found higher degree of hippocampal atrophy and depressive symptoms associated with SCD in help-seeking SCD participants compared to community-recruited SCD participants, providing a meaningful aspect of SCD with respect to underlying brain pathology. Therefore, research setting may have an impact on study outcomes. For this study, all participants were recruited from the community and not all were carriers of the APOE ɛ 4 allele or had abnormal level of Aβ (amyloid positive). Notably, COVID-19 impact on this study resulted in a small sample size with large gender differences, and only a small portion of the participants were carriers of the APOE ɛ4 allele or had abnormal level of Aβ. To achieve 80% power for detecting a small effect (i.e., r = 0.1–0.3) at a significance criterion of α= 0.05, the required sample size would have to be N = 128 (64 participants per group). Therefore, larger differences in AERP measures between the groups would be needed to achieve significance in the current sample size of 62 participants. This could be a potential explanation as to why AERP latencies are not significantly different between SMC and non-SMC groups.
Conclusion
This is the first study to investigate AERP latencies in individuals with SMC as well as the relationship between AERP latency and amyloid burden. Our data indicate that cerebral Aβ load could significantly predict cognitive outcomes (MAC-Q and MoCA scores) and Aβ+ participants had a significantly longer P50 latency when compared to Aβ– participants. Additionally, P50 latency was significantly correlated with MAC-Q, suggesting that increased degree of subjective memory complaints is accompanied with impaired sensory classification and sensory gating as reflected by longer P50 latency. Collectivity, results from this study indicate that P50 latencies have the potential to contribute to the identification of individuals at higher risk of developing AD dementia. Future research with participants that possess multiple risk factors of AD, including subjective memory complaints, presence of APOE ɛ4, high brain amyloid levels and depression, could provide a categorical population for investigating the usefulness of AERPs in early AD diagnosis. While this research provide insight into the usefulness of AERP measures in identifying individuals at higher risk of developing cognitive decline, further larger cross-sectional as well as longitudinal studies on help-seeking SCD participants are required to determine if AERP measures could be of significance for the detection of pre-clinical AD. Future research should also investigate the association between AERP amplitudes and subjective cognitive and memory decline, as well as, the differences in AERP amplitudes in response to passive and active two-tone oddball tasks.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This work was supported by the Australian Government Research Training Program Scholarship at The University of Western Australia; Australian Alzheimer’s Research Foundation; and Ear Science Institute Australia.
CONFLICT OF INTEREST
Hadeel Y. Tarawneh is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
The authors have no other conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.