
Abstract
Background:
Antibiotics for systemic use may increase the risk of neurodegeneration, yet antibiotic therapy may be able to halt or mitigate an episode of neurodegenerative decline.
Objective:
To investigate the association of sporadic use of antibiotics and subsequent dementia risk (including Alzheimer’s disease).
Methods:
We used data from the largest public health insurance fund in Germany, the Allgemeine Ortskrankenkasse (AOK). Each of the 35,072 dementia cases aged 60 years and older with a new dementia diagnosis during the observation period from 2006 to 2018 was matched with two control-patients by age, sex, and time since 2006. We ran conditional logistic regression models for dementia risk in terms of odds ratios (OR) as a function of antibiotic use for the entire antibiotic group and for each antibiotic subgroup. We controlled for comorbidities, need for long-term care, hospitalizations, and nursing home placement.
Results:
Antibiotic use was positively associated with dementia (OR = 1.18, 95% confidence interval (95% CI):1.14–1.22), which became negative after adjustment for comorbidities, at least one diagnosis of bacterial infection or disease, and covariates (OR = 0.93, 95% CI:0.90–0.96). Subgroups of antibiotics were also negatively associated with dementia after controlling for covariates: tetracyclines (OR = 0.94, 95% CI:0.90–0.98), beta-lactam antibacterials, penicillins (OR = 0.93, 95% CI:0.90–0.97), other beta-lactam antibacterials (OR = 0.92, 95% CI:0.88–0.95), macrolides, lincosamides, and streptogramins (OR = 0.88, 95% CI:0.85–0.92), and quinolone antibacterials (OR = 0.96, 95% CI:0.92–0.99).
Conclusion:
Our results suggest that there was a decreased likelihood of dementia for preceding antibiotic use. The benefits of antibiotics in reducing inflammation and thus the risk of dementia need to be carefully weighed against the increase in antibiotic resistance.
Keywords
INTRODUCTION
As the elderly population increases, the number of dementia patients will also increase, as the strongest risk factor for developing dementia is advancing age [1, 2]. In 2019, approximately 55 million people worldwide were affected, and the number of dementia patients will increase rapidly; 40 percent more people are expected to be living with dementia in 2030 than today [1, 3]. Dementia is driving up care and health insurance costs, which increases costs for governments, communities, families, and individuals. This makes research on risk and protective factors an important step toward dementia prevention[1, 5].
Many risk factors have already been identified [6], but only a few studies have explored the risk of the use of antibiotics for systemic use (ASU) on dementia incidence [7, 8]. ASUs eliminate the colonization of the human body with pathogenic bacteria and prevent systemic inflammation, and are thought to promote or maintain health [9]. However, they also affect the gut microbiome [10] and increase antimicrobial resistance, which can have an overall negative impact on the health of individuals and ultimately entire populations. They are effective against a broad spectrum of bacteria, act throughout the organism, and can be used in a variety of ways [11].
There are two competing hypotheses regarding the association between ASU and dementia incidence. On the one hand, ASU that act against a wide range of bacteria cause an unbalanced gastrointestinal microbiome because they affect the composition of the gut microbiota; they reduce its biodiversity and delay healthy, balanced bacterial colonization of the gut over a long period of time [7, 12–14]. Antibacterial-induced dysbiosis of the microbiome can have a direct and indirect, as well as short- and long-term, impact on health [12, 15]. Modifications of the gut microbiome are associated with cognitive function and various neurological and neurodegenerative diseases, and the microbiome can influence the brain and neurological activities as well as causing possible memory impairment and dysfunction [7, 17]. Thus, the use of ASU could be associated with an increase in dementiarisk.
On the other hand, pathological changes in the brain and cerebral immune responses are intimately involved both in infectious delirium and Alzheimer’s disease [18]. There is strong evidence that most neurodegenerative diseases are propelled by systematic inflammation caused by peripheral infections such as bacterial sepsis, periodontitis but also autoimmune disease all of which are able to drive an activation of local immune responses in the brain [19–26]. Infection-related episodes of inflammation, particularly in the elderly, exacerbate processes in the brain that underlie cognitive decline, meaning that infections can accelerate cognitive decline in people with, but also without, clinical symptoms [19]. ASU treatment could attenuate the infectious inflammatory process, thereby decelerating the process to clinically measurable symptoms of dementia [22] and reducing the dementia risk [27]. Thus, the use of ASU should be associated with a decrease in dementia risk.
We tested these two competing hypotheses by conceiving a nested case-control study using German health claims data. We examined the risk of incident dementia in patients who had filled at least one ASU prescription compared to those without.
METHODS
Analysis sample
We used a random longitudinal sample of 250,000 insurants of Germany’s largest public health insurance fund, the Allgemeine Ortskrankenkasse (AOK). The sample was drawn in the first quarter of 2004 and followed quarterly through the end of 2019. The data provide demographic information about sex, year and month of birth, month and year of death (if applicable), the place of residence, and whether the person lived in an institution or not. Furthermore, the sample includes information on all inpatient and outpatient diagnoses, coded according to the German modification of the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). The data contain filled prescriptions of drugs coded according to the Anatomical Therapeutic Chemical Classification (ATC) code of active ingredients anddrugs.
We included individuals who were born before 1945, excluding individuals with a valid dementia diagnosis in 2004 and 2005. By using a two-year washout period, we attempted to approximate incident dementia cases. All patients were censored at the time of death, at change of insurer, or at the end of 2018 (to permit the validation of dementia diagnoses). We also censored at time of the first filled prescription with aminoglycoside ASU (J01G), combinations of ASU (J01R), and other ASU (J01X) because very few patients were prescribed these ASU. Of the 250,000 individuals in our original sample, 153,697 individuals were included in our data sample according to our inclusion criteria. 35,072 individuals had diagnosed dementia between the beginning of 2006 and the end of 2018. The observation ends at the time of the first dementia diagnosis. Details of the exclusion criteria are available in Supplementary Figure 1. All subgroups of ASU included are described below under “Definition of antibiotics for systemic use”.
Study design
For our nested case-control study, using incidence-density sampling (Stata command sttocc), we matched each incident dementia case to two controls without dementia by age (in five-year groups), sex, and time since 2006 to minimize bias in using cases and controls with different follow-up times [28]. For controls, the index date was set to the date of dementia diagnosis of the matched cases. Our final data sample consisted of 105,216 individuals, with 35,072 dementia cases through the end of 2018 and 70,144 matched controls. We considered the sporadic use of antibiotics until the quarter of dementia diagnosis, controls until the index date due to the matching process. Sporadic antibiotic use is defined as at least one filled ASU prescription.
Definition of dementia
We used the following ICD-10 codes to define dementia: dementia in AD (F00), vascular dementia (F01), dementia in other diseases classified elsewhere (F02), unspecified dementia (F03), delirium superimposed on dementia (F05.1), Alzheimer dementia (G30), and circumscribed brain atrophy (G31.0). To avoid the problem of false-positive diagnoses, we used an established internal two stage validation strategy [29, 30]. First, we only used labeled outpatient diagnoses as verified by medical doctors, and inpatient discharge and secondary diagnoses. In the next stage, we considered diagnoses valid if they were confirmed by a concurrent inpatient and outpatient diagnosis and by two diagnoses from two different types of physicians within the same quarter. If a person died within the same quarter in which the dementia was first diagnosed, a diagnosis was still considered to be valid.
Definition of antibiotics for systemic use
We used the following ATC-codes to identify the following prescribed ASU (J01): tetracyclines (J01A), beta-lactam ASU (J01C), other beta-lactam ASU (J01D), sulfonamides and trimethoprim (J01E), macrolides, lincosamides, and streptogramins (J01F), and quinolone ASU(J01M).
Covariates
The comorbidity burden was calculated using the Elixhauser comorbidity score, which includes 30 diseases [31].We combined the occurring comorbidities into a total score so that the burden of disease could be assessed with a single numeric score. Furthermore, we controlled for diseases and bacterial infections usually treated with ASU, such as gastrointestinal infections (A00-A09), pneumonia (J1[234678], J110, J84, J150-J159, P23[012345689], P350), respiratory infection (H67, J01-J02, J200-J202), bladder and urinary tract infections (N30, N33, N37, N39), skin infections (L01, L02, L03, L08, A46) and for bacterial infections associated with an increased risk of cognitive impairment and dementia such as sepsis [32, 33], bacterial meningitis [34], meningococcal infection [35], and Lyme disease [36]. The diseases and bacterial infections were combined into one variable indicating whether or not a disease or bacterial infection was diagnosed in a specific quarter. We controlled whether or not patients lived in a nursing home and whether or not they had been hospitalized at least once since the start of observation. In addition, we controlled for the presence or absence of severe long-term care dependency, with severe long-term care dependency defined as care level 3 (up to the end of 2016) or care grade 5 (from 2017 onwards). More details are available in the Supplementary Method 1. For each subgroup of ASU, we created a dummy variable consisting of all the other remaining subgroups of ASU. This dummy variable indicates whether or not at least one of the remaining ASU was filled in a pharmacy in the current quarter. Additionally, we included age on a continuous scale. All predictors except age were coded as time-dependent binary variables with a value of one from the first occurrence onward and zero otherwise. We measured the covariates for cases at the time of dementia diagnosis and for control subjects at the indexdate.
Analysis strategy and statistical methods
To examine the risk of dementia associated with ASU, we estimated odds ratios (OR) with conditional logistic regression models [37] for the total group of ASU, and for each of the six ASU groups separately.
First, crude models were estimated which controlled for age and sex due to the study design and for age on a continuous scale. Second, adjusted models were estimated by including the Elixhauser comorbidity score, diagnosis of at least one bacterial infection/disease, other control variables, and the other ASU. Third, lag-times of ASU use from one up to three years were implemented, which measured the time since the first prescription of (the specific) ASU was filled. Fourth, the number of quarters with at least one filled prescription were included in the models by cumulating the number of quarters with ASU across all and across the specific groups of ASU.
As a sensitivity analysis, all analyses were performed for patients with diabetes only and only for patients living in nursing homes, as the risk of inflammation and dementia is particularly high in these patients [38, 39]. All analyses were performed using Stata 16.0.
Ethical approval
Access to the health claims data was granted and approved by the Scientific Institute of the AOK (WIdO), while access to the complete database was not possible, due to current data protection regulations. All analyses of this study are based on anonymized administrative claims data which never identify patients directly. As individuals are anonymous, the results presented here do not in any way affect the persons whose records were used. No ethical approval was required, therefore this study complies with the tenets of the Declaration of Helsinki.
RESULTS
Descriptive results
Because of the matching process by age, sex, and follow-up time, the proportion of age and sex and the follow-up time were identical for cases and controls. Both the 35,072 cases and the 70,144 controls had a follow-up time of 5.67 years, the mean age was 81.55 years for cases and 81,33 years for controls, and 64.11% were women (Table 1). At the date of diagnosis, the prevalence of ASU was slightly but significantly higher among case than control patients, with 73% of case patients and 70% of control patients having filled an ASU (J01) (Table 1). Filled prescription of quinolone ASU (J01M) (Table 1, case 42%, control: 38%, p < 0.001), and macrolides, lincosamides, and streptogramins (J01F) were most frequent (Table 1, case 32%, control 32%, p = 0.7613); those of tetracyclines (J01A) the least frequent (Table 1, case: 18%, control 18%, p = 358). In terms of chronic diseases and infections the case group generally had a worse health profile than did the control group. In the case group there were more than three times as many gastrointestinal infections (Table 1, cases 4.76%, controls 1.19 %, p < 0.001), pneumonia infections (Table 1, cases 7.42%, controls 2.260%, p < 0.001), and patients with severe long-term care (Table 1, cases 3.63%, controls 0.93%, p < 0.001) than in the control group. The proportions of people living in nursing homes (Table 1, cases 15.24%, controls 3.59%, p < 0.001) and those receiving inpatient care (Table 1, cases 49.36%, controls 10.48%, p < 0.001) were almost four times higher than in the control group.
Characteristics of the study population
ASU, antibiotics for systemic use; sd, standard deviation. Source: AOK data 2006– 2018.
Model results
Total group of ASU (J01)
For the total group of ASU, there was a positive association with a subsequent diagnosis of dementia after adjustment for age and sex (Table 2, model 1: OR = 1.18, 95% CI: 1.14–1.22). Further adjustment for the Elixhauser comorbidity score attenuated some of the positive association (Table 2, model 2: OR = 1.04, 95% CI: 1.01–1.07). After controlling for at least one bacterial infection or disease, the association became negative (Table 2, model 3: OR = 0.92, 95% CI: 0.89–0.95). Additional adjustment for other control variables did not change the association (Table 2, model 4: OR = 0.93, 95% CI: 0.90–0.96).
Stepwise-adjusted odds ratio and 95% confidence intervals by prescribed antibiotics for incident dementia
N = 105,216; OR, Odds ratio; CI, confidence interval; ASU, antibiotics for systemic use. Model 1: adjusted for age and sex. Model 2: adjusted for age, sex and Elixhauser comorbidity score. Model 3: adjusted for age, sex, Elixhauser comorbidity score and diagnosis of at least one bacterial infection/disease. Model 4: adjusted for age, sex, Elixhauser comorbidity score and diagnosis of at least one bacterial infection/disease and other control variables. Source: AOK data 2006–2018.
Subgroups of ASU
Adjusting for age and sex, there was an increased OR for preceding use of antibiotic subgroups beta-lactam antibiotics, penicillins (J01C), other beta-lactam antibiotics (J01D), sulfonamides and trimethoprim (J01E), and quinolone antibiotics (J01M) (Fig. 1, model 1: J01C: OR = 1.11, 95% CI: 1.08–1.15; J01D: OR = 1.12, 95% CI: 1.09–1.16; J01E: OR = 1.17, 95% CI: 1.13–1.21; J01M: OR = 1.17, 95% CI: 1.14–1.21). There were no significant associations for the other groupsof ASU.
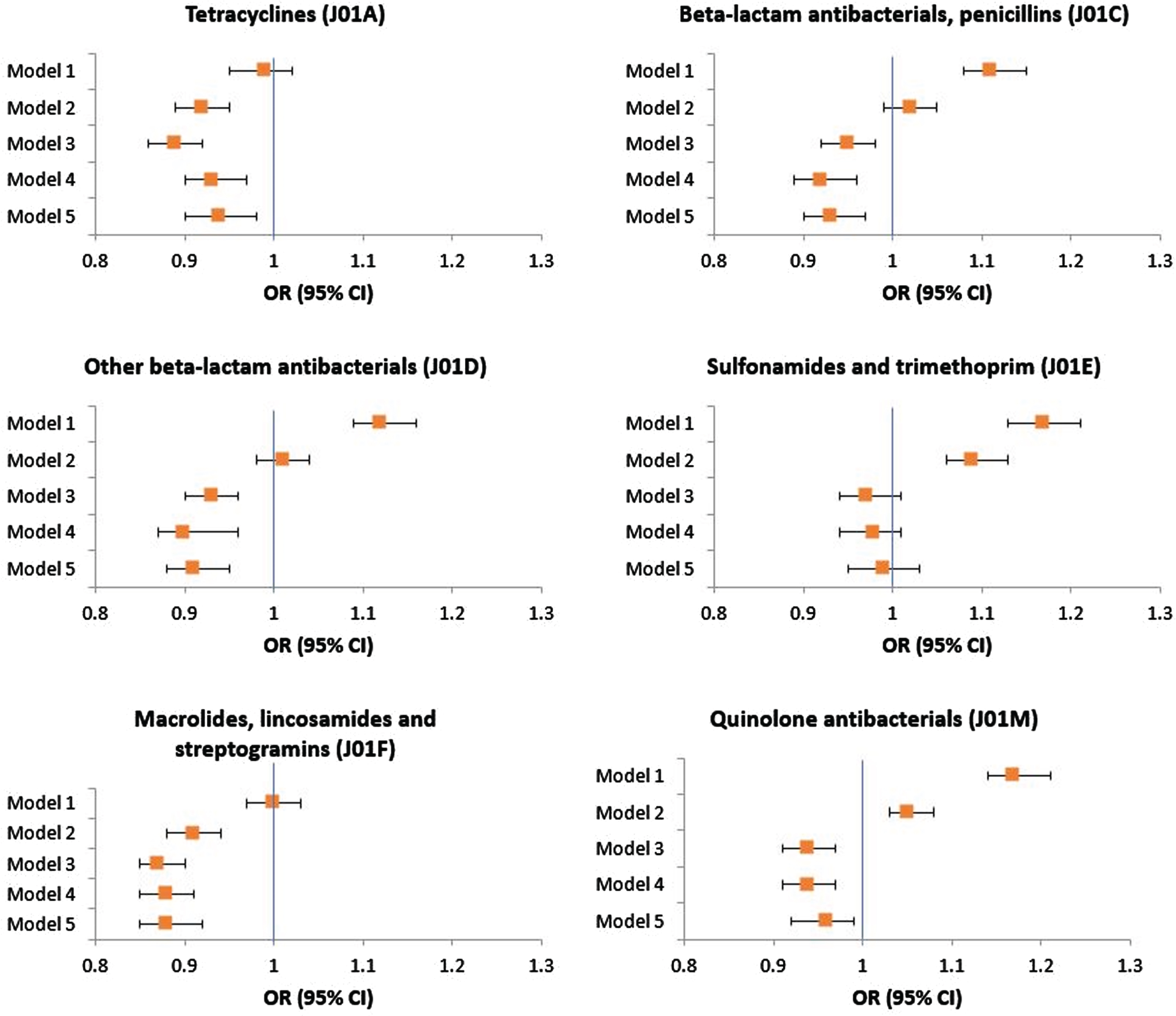
Stepwise-adjusted odds ratio and 95% confidence intervals by prescribed antibiotics for incident dementia. N = 105,216; OR, Odds ratio; CI, confidence interval; ASU, antibiotics for systemic use. Model 1: adjusted for age and sex. Model 2: adjusted for age, sex and Elixhauser comorbidity score. Model 3: adjusted for age, sex, Elixhauser comorbidity score, diagnosis of at least one bacterial infection/disease. Model 4: adjusted for age, sex, Elixhauser comorbidity score, diagnosis of at least one bacterial infection/disease and other control variables. Model 5: adjusted for age, sex, Elixhauser comorbidity score, diagnosis of at least one bacterial infection/disease, other control variables and the use of ASU of the other subgroup. Source: AOK data 2006–2018.
In addition, controlling for Elixhauser comorbidity score and the diagnosis of at least one bacterial infection or disease, there was a significantly decreased OR for all subgroups of ASU, except sulfonamides and trimethoprim (J01E), with dementia (Fig. 1, model 3: J01A: OR = 0.89, 95% CI: 0.86–0.92; J01C: OR = 0.95, 95% CI: 0.92–0.98; J01D: OR = 0.93, 95% CI: 0.90–0.96; J01E: OR = 0.97, 95% CI: 0.94–1.01; J01F: OR = 0.88, 95% CI: 0.85–0.90; J01M: OR = 0.94, 95% CI: 0.91–0.97). The association persisted after controlling for additional control variables. Additionally, we controlled each OR of the subgroups for the use of the other subgroups of ASU. The control does not change the association from the previous model (Fig. 1, model 5: J01A: OR = 0.94, 95% CI: 0.90–0.98; J01C: OR = 0.93, 95% CI: 0.90–0.97; J01D: OR = 0.92, 95% CI: 0.88–0.95; J01E: OR = 0.99, 95% CI: 0.95–1.03; J01F: OR = 0.88, 95% CI: 0.85–0.92; J01M: OR = 0.96, 95% CI: 0.92–0.99). A tabular overview of all OR is available in Supplementary Table 1A-F. We confirmed the results in sensitivity analyses with diabetic patients only and with nursing home residents only (results not shown; available on request).
Lag-time analysis
With one year lag-time, there was a negative association with a subsequent diagnosis of dementia for the total group of antibiotics (Fig. 2, OR = 0.88, 95% CI: 0.85–0.91), tetracyclines (J01A) (Fig. 2, OR = 0.95, 95% CI: 0.91–0.99), beta-lactam antibacterials, penicillins (J01C) (Fig. 2, OR = 0.92, 95% CI: 0.88–0.95), other beta-lactam antibacterials (J01D) (Fig. 2, OR = 0.93, 95% CI: 0.89–0.97), macrolides, lincosamides, and streptogramins (J01F) (Fig. 2, OR = 0.88, 95% CI: 0.85–0.91), and quinolone antibacterials (J01M) (OR = 0.93, 95% CI: 0.90–0.96). There was also a significant negative association for lag-times of two to three years for the total group of antibiotics (J01) (Fig. 2, OR = 89, 95% CI: 0.86–0.93) and all subgroups, with exception of sulfonamides and trimethoprim (J01E) (Fig. 2, J01A: OR = 0.94, 95% CI: 0.90–0.99; J01C: OR = 0.92, 95% CI: 0.89–0.97; J01D: OR = 0.91, 95% CI: 0.86–0.95; J01E: OR = 0.99, 95% CI: 0.94–1.04; J01F: OR = 0.90, 95% CI: 0.86–0.93; J01M: OR = 0.94, 95% CI: 0.91–0.98).

Odds ratio and 95% confidence intervals of incident dementia one to three years after first prescription of antibiotics. OR, Odds ratio; CI, confidence interval; ASU, antibacterials for systemic use. All models were adjusted for age, sex, Elixhauser comorbidity score, diagnosis of at least one bacterial infection/disease, other control variables and the use of ASU of the other subgroups. Source: AOK data 2006–2018.
Number of quarters with filled prescriptions
For a quarter with one filled antibiotic prescription, the OR was increased (Table 3, OR = 1.02, 95% CI: 0.98–1.07). This positive association changed to a negative association with the number of quarters in which antibiotics were prescribed (Table 3, OR = 0.80, 95% CI: 0.76–0.84). The subgroups beta-lactam antibiotics, penicillins (J01C), other beta-lactam antibiotics (J01D), and macrolides, lincosamides, and streptogramins (J01F), also revealed positive associations with a diagnosis of dementia (Supplementary Table 2). The results for sulfonamides and trimethoprim (J01E) are striking, with neither one quarter nor up to five quarters of prescriptions associated with a subsequent diagnosis of dementia (Supplementary Table 2).
Odds ratio of cumulative number of quarters by prescribed antibiotics for incident dementia
OR, Odds ratios; CI, confidence interval; ASU, antibiotics for systemic use. aadjusted for age, sex, Elixhauser comorbidity score, diagnosis of at least one bacterial infection/disease and other control variables. Source: AOK data 2006–2018.
DISCUSSION
For ASU, negative associations with dementia incidence were observed for the total antibiotic group (J01) and for the antibiotic subgroups except sulfonamides and trimethoprim (J01E). Differentiation by time since the first filled prescription did not change this association, which was present up to three years after the first filled prescription. For the total group of antibiotics (J01) and all subgroups of antibiotics, again with the exception of sulfonamides and trimethoprim (J01E), there were negative associations between increasing number of quarters with a filled prescription and a subsequent diagnosis of dementia.
Our results support the hypothesis that the sporadic use of ASU is associated with a decrease in dementia risk, once comorbidities and the presence of at least one bacterial infection or disease are controlled for, which was particularly evident for tetracyclines (J01A), beta-lactam antibacterials, penicillins (J01C), other beta-lactam antibacterials (J01D), macrolides, lincosamides, and streptogramins (J01F) and quinolone antibacterials (J01M). Our finding is in line with previous studies in patients with an existing cognitive impairment, which predominantly provided evidence of a positive effect of ASU on cognitive function. Administrations of the ASU rifampin and doxycycline, from the tetracycline drug class (J01A), significantly improved cognitive function after six months in patients with Alzheimer’s disease and patients with mild to moderate dementia [40]. A follow-up study [8], however, could not confirm these results, but found cognitive deterioration in ASU users.
Analyses with the broad-spectrum ASU amoxicillin, from the beta-lactam ASU drug class (J01C), comparing cognition in Alzheimer’s disease patients suffering from bacterial infection by helicobacter pylori to the control groups without such infection and the control group with failed amoxicillin treatment showed significant differences in cognition between groups [41]. Cognitive and functional parameters improved in patients receiving successful antibacterial therapy, but not in the other groups. The effect may result from the control of pathogenic bacterial infection and the suppression of infection-associated systemic inflammatory processes. Systemic inflammation may harm brain function through several mechanisms including the sustained presence of pro-inflammatory mediators, the impairment of peripheral organ function, changes of brain perfusion or changes of the microbiome [42]. In keeping with this, harmful bacterial infections may also trigger dysbiosis of the gut microbiome, damage the gut barrier, and stimulate microorganisms to synthesize and release molecules that exert toxic effects in the brain [7, 43]. Bacterial metabolites, e.g. short chain fatty acids, escaping the intestines can promote systemic disease and trigger neuroinflammatory responses in the brain [10]. Antibacterial therapy may eliminate pathogenic bacteria, thereby preventing or attenuating neuroinflammation [20–22, 43]. Immunological changes that occur in infection-induced delirium are similar to those that induce neuronal damage in Alzheimer’s disease [18]. Infection-related inflammatory episodes accelerate the processes underlying cognitive dysfunction and decline, which may explain why infections accelerate cognitive decline in people with or without overt clinical symptoms and are thus associated with increased dementia risk, especially in the elderly, regardless of their severity [20, 44]. Antibacterial therapy may also halt or prevent relapse of infection, which may explain the reduced effect in our time-delay analysis.
The effects of the different antibiotic treatments, with their various modes of action and antimicrobial spectra, and different distribution kinetics, point in the same direction. It might be possible that this result is due to the inflammatory process, and it is reasonable to assume that antibacterial therapies can in principle halt infection-induced inflammation, at least for a short period of time.
As mentioned above, rifampin and doxycycline, both belonging to the tetracycline drug class (J01A), have been found to cause cognitive deterioration [8]. One possible explanation may lie in the connection between the gut microbiome and the brain:
Alterations of the gut microbiome have been linked to cognitive aging and various neurological and neurodegenerative disorders. Thus, the microbiome can negatively impact on brain function and cause memory impairment. The gut microbiome and the brain affect each other in several ways through the so called gut-brain axis ultimately affecting human health [7, 17]. ASU act systemically, i.e., throughout the patient’s body, and can disrupt the gut-brain axis. ASU enter the intestines and can change the microbiome there, thus disrupting the health-maintaining functioning of the gut [12–14, 46]. Furthermore, the gut microbiome releases proinflammatory substances during an inflammatory process [43, 47–49]. The results of these antibacterial effects can be memory impairment and other cognitive dysfunctions [7]. Recent findings in a mouse model of tauopathy show an ApoE isoform and microbiota-dependent progression of neurodegeneration. Mice raised under germ-free conditions or shortly treated with antibiotics early in life to disrupt the gut microbiome exhibited reduced neurodegeneration [10, 50], which is in line with ourfindings.
Claims data and dementia registries are valuable for tracking dementia, but these record a dementia diagnosis with an average delay of about 5.5 years [51, 52]. Dementia is a gradual process that can begin years before the first clinical symptoms, so patients who are still recorded as ostensibly healthy in the data may already be suffering from the onset of cognitive change. Sporadic antibacterial use may attenuate or prevent the boosting effect of infection on cognitive change. While the acute episode could be prevented, cognitive decline cannot be completely halted and continues to progress insidiously. As a result, clinical symptoms only become apparent later and patients receive a delayed diagnosis. Our result—that the risk of dementia declined with increasing number of quarters with prescriptions—further supports this hypothesis. One quarter of prescriptions may not be sufficient to halt the boosting effect of infections.
The initial increased risk of ASU users compared to non-users can be fully explained by their comorbidity pattern and the presence of at least one bacterial infection or disease. This suggests that ASU are taken more often by comparatively morbid patients. Morbid patients with a higher number of comorbidities are generally sicker and at higher risk of being prescribed ASU. For example, patients with chronic diseases such as diabetes are more likely to have infections that need to be treated with ASU. However, these patients are also at a higher risk of developing dementia. Only after adjusting for comorbidity pattern and the presence of at least one bacterial infection or disease, the effect that dementia patients were less likely to be exposed to antibiotics than their control group becomes evident and supports our second hypothesis.
Limitations
Health claims data are only available for individuals using the medical system and they are intended to be used for billing rather than for an epidemiological analysis. Important risk factors associated with dementia are not included in these data, such as educational attainment, physical activity, and lifestyle factors such as tobacco or alcohol use [53]. We attempted to account for these factors by including comorbidities and nursing home status, which in turn are associated with a person’s socioeconomic status. In addition, our data do not capture prescriptions from the inpatient sector. Our effects may therefore be underestimated, as people who only received a prescription in hospital are in the non-user group. All patients with a prescription for ASU have an indication for that prescription, which itself may be associated with dementia. We have attempted to capture this by adjusting for diagnosis of at least one bacterial infection/disease. There are other factors known to be associated with the gut microbiome that are not captured by the health data used. Environmental factors, diet, and genetic conditions all play important roles in relation to a healthy gut microbiome. Supportive probiotic bacteria can be ingested through diet, which help provide the body with the necessary substances to prevent inflammation and associated diseases [7]. Another limitation is that the actual onset of dementia is unknown. However, we address this issue by excluding individuals with dementia in 2004 and 2005. We only have data on individuals aged 50 years and older, so we do not have information on exposure to administered ASU or comorbidities before the age of 50 and before the year 2004. In addition, the documented prescriptions for ASU do not indicate whether these were actually taken by patients, and the actual antibacterial use may be different. But in general, patients’ adherence to ASU is considered high [54]. Our analysis of the effect of the cumulative number of ASU is limited by the small number of patients within the groups, which biases the results of the effect of prescription number and dementia risk.
The effects of the different antibiotic classes point in the same directions. Analyses with cohort data are needed to validate our results and examine individual antibiotics in more detail.
Conclusion
We believe that the association between dementia and sporadic antibiotic use in this case-control study provides valuable hypotheses. The reduction of dementia risk may be due to attenuation of inflammation, which in turn may reduce neurodegeneration. Our results are in line with previous findings that have emphasized the importance of preventing systemic inflammation in the elderly. Seemingly, the benefits of treating infections with ASU and the associated reduction in dementia risk must outweigh the risk of developing antibiotic resistance. Our analyses are intended to provide a first overview of how each class of ASU affects the risk of developing dementia. We hope that our results will stimulate further analyses of individual ASU groups or specific ASUs to unravel their potential benefit on cognition.
Footnotes
ACKNOWLEDGMENTS
The authors are grateful to the Scientific Research Institute of the Allgemeine Ortskrankenkasse (AOK), (German: Wissenschaftliches Institut der AOK, WIdO), for providing the data.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
Dr. Anne Fink is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review. The authors have no conflict of interest to report.