
Abstract
Background:
The association between poor oral health and the risk of incident dementia remains unclear.
Objective:
To investigate the associations of poor oral health with incident dementia, cognitive decline, and brain structure in a large population-based cohort study.
Methods:
A total of 425,183 participants free of dementia at baseline were included from the UK Biobank study. The associations between oral health problems (mouth ulcers, painful gums, bleeding gums, loose teeth, toothaches, and dentures) and incident dementia were examined using Cox proportional hazards models. Mixed linear models were used to investigate whether oral health problems were associated with prospective cognitive decline. We examined the associations between oral health problems and regional cortical surface area using linear regression models. We further explored the potential mediating effects underlying the relationships between oral health problems and dementia.
Results:
Painful gums (HR = 1.47, 95% CI [1.317–1.647], p < 0.001), toothaches (HR = 1.38, 95% CI [1.244–1.538], p < 0.001), and dentures (HR = 1.28, 95% CI [1.223–1.349], p < 0.001) were associated with increased risk of incident dementia. Dentures were associated with a faster decline in cognitive functions, including longer reaction time, worse numeric memory, and worse prospective memory. Participants with dentures had smaller surface areas of the inferior temporal cortex, inferior parietal cortex, and middle temporal cortex. Brain structural changes, smoking, alcohol drinking, and diabetes may mediate the associations between oral health problems and incident dementia.
Conclusion:
Poor oral health is associated with a higher risk of incident dementia. Dentures may predict accelerated cognitive decline and are associated with regional cortical surface area changes. Improvement of oral health care could be beneficial for the prevention of dementia.
INTRODUCTION
Dementia is a common disorder among the elderly and becomes more prevalent with advancing age. It can reduce life expectancy, lower the quality of life for patients and their caregivers, and impose a massive and growing economic burden internationally [1]. Because the known modifiable risk factors of dementia account for only 40% of dementia cases, identifying additional preventable risk factors has become an urgent public health priority.
Poor oral health is a major global public health problem, having both high prevalence and major negative impacts [2]. Oral diseases and poor oral hygiene are linked to a series of chronic diseases including cardiovascular disease, diabetes, and cancer [3–5]. Recently, increasing evidence suggested that poor oral health status could raise the risk of cognitive impairment and incident dementia [6–8]. However, the previous findings on the relationship between oral health status and subsequent cognitive decline or dementia were contradictory and inconsistent, possibly because of methodological limitations, such as small sample sizes and insufficient follow-up time [9, 10].
Previous studies have reported that tooth loss was associated with lower total brain volume and gray matter volume [11]. Furthermore, two studies found that tooth loss or poor masticatory performance were associated with smaller gray matter volumes of the premotor cortex, primary motor cortex, hippocampus, parahippocampus, caudate nucleus, and temporal pole [12, 13]. However, neither of these two studies investigated the regional cortical surface area changes underlying the association between poor oral health and the risk of dementia.
We hypothesized that there were associations between oral health problems and incident dementia. Dementia-related oral health problems would be associated with prospective cognitive decline and brain structural changes, and the associations between oral health problems and dementia incidence may be supported by some mechanisms related to brain structures, lifestyles, and health conditions. Thus, using the comprehensive data collected in the UK Biobank [14], we systematically examined the longitudinal associations between six oral health problems (mouth ulcers, painful gums, bleeding gums, toothaches, loose teeth, dentures) and the risk of incident dementia, and further investigated whether those dementia-related oral health problems were associated with prospective cognitive decline and regional cortical surface area. Lastly, we investigated the mediating effects of brain structures/lifestyles/health conditions on the relationships between oral health problems and incident dementia (Fig. 1).

STROBE flow chart.
METHODS
Participants
Data came from the UK Biobank, a large UK-based prospective cohort study [14]. Between 2006 and 2010, 502,493 individuals aged 40 to 69 years old were recruited and completed a touchscreen questionnaire, verbal interview, physical examination, and biological samples. Of the total population, 440,776 participants without baseline dementia had follow-up data on dementia. Then, we excluded 5,585 participants without data on baseline oral health problems, and 10,008 participants without covariates data, leaving 425,183 participants in the study sample. Among them, 135,121 participants had data on cognitive function at baseline and during the follow-up, and 38,675 participants had data on MRI. The UK Biobank involves human participants and was approved by the National Information Governance Board for Health and Social Care and National Health Service North West Multicentre Research Ethics Committee (approval number: 11/NW/0382). Data used in the present study were accessed via the UKB project proposal 19542. Informed consent was obtained from all participants.
Oral health problems
Oral health problems included mouth ulcers, dentures, painful gums, bleeding gums, toothaches, and loose teeth. These self-reported mouth/teeth dental problems were collected by touchscreen questionnaire at baseline by asking participants, “Do you have any of the following?” (Field 6149). Participants can select more than one answer from mouth ulcers, dentures, painful gums, bleeding gums, toothaches, loose teeth, and dentures. Those who did not make a selection or selected “None of the above” or “Prefer not to answer” were excluded from the current analysis.
Oral diseases diagnoses
The diagnosis data came from the UK routinely-collected healthcare data including hospital in-patient records, primary care records, death register data, as well as primary care data. We excluded the self-reported cases. Diagnoses in hospital in-patient records, primary care records, and death register data were recorded using the International Classification of Diseases (ICD10) coding system. Diagnoses in primary care data were recorded using Read codes (version 2 [Read v2] and version 3 [CTV3 or Read v3]). We retrieved data on three common oral health diseases: dental caries (ICD10 coding: K02); pulp and periapical tissues diseases (K04), and gingivitis and periodontal diseases (K05). Participants diagnosed with oral diseases before their registration dates were regarded as cases of baseline oral diseases.
Dementia diagnosis
Incident all-cause dementia events were retrieved from algorithmically-defined dementia (Field 42018) and the UK routinely-collected healthcare data. For the current analyses, data on dementia in Alzheimer’s disease (F00), vascular dementia (F01), dementia in other diseases classified elsewhere (F02), unspecified dementia (F03), and Alzheimer’s disease (G30) was obtained from hospital in-patient records and death register data. Data on dementia in Alzheimer’s disease (F00, G30), and vascular dementia (F01) were used in the stratified analyses. The validity of the dementia diagnoses based on the UK routinely-collected healthcare data was presented in a previous study. The study indicated that healthcare data can be used to identify all-cause dementia in prospective studies [15].
Cognitive assessment
All cognitive tests were administered visually via touchscreen, and scoring was calculated automatically. The format and psychometric properties of the cognitive test used in the UK Biobank have been described by Cullen et al. [16, 17]. These tests assessed reaction time (mean time in milliseconds to press a button in response to matching cards, Field 20023), numeric memory (longest numeric string recalled in reverse, Field 4282), reasoning (total correct of 13 items, Field 20016), prospective memory (successfully carrying out instruction after a filled delay, Field 20018), and visual memory (’pairs matching’ test: total errors when recalling positions of matching cards, Field 399). Higher values indicated better performance on the reasoning and numeric memory tests, but worse performance on the reaction time and pairs matching tests. The numeric memory test was removed from the UKB baseline assessment battery part-way through recruitment, for reasons of time, resulting in lower sample sizes on this test than on the other four tests. Prospective memory data were dichotomized as either “correct on the first attempt” or not. Two trials of ‘pairs matching’ tasks were administered, one with three pairs of symbols and one with six pairs. Because there was a ceiling effect on the three-pair trial, only the score on the six-pair trial of the test was analyzed in the present study [16]. Cognitive function was assessed over four-time points: the initial assessment visit (2006–2010), the first repeat assessment visit (2012–2013), the imaging visit (2014+), and the first repeat imaging visit (2019+).
Structural magnetic resonance imaging data
Since 2014, the imaging extension to the existing UK Biobank study started to scan subjects from the existing cohort, and the imaging data was only for research. Neuroimaging data were collected with a standard Siemens Skyra 3T scanner with a 32-channel head coil [18, 19]. Detailed imaging protocol can be found in an open-source document (https://biobank.ndph.ox.ac.uk/showcase/showcase/docs/brain_mri.pdf). Quality-controlled T1-weighted neuroimaging data were used in the current study. Neuroimaging data were processed with FreeSurfer, and the surfer templates were used to extract imaging-derived phenotypes [20]. The surface area of 68 cortical regions aparc (ID 192) atlas was used in this study.
Covariates
Relevant covariates included age at baseline (Field 21022); sex (Field 31); race, categorized as white and no-white (Field 21000); APOE ɛ4 carry status, derived from UK Biobank; educational levels (Field 6138); Townsend deprivation index (Field 189), calculated by the information on social class, employment, car availability, and housing; body mass index (BMI, Field 21001); smoking status (Field 20116), alcohol drinking (Field 20117); average blood pressure and diabetes. Average blood pressures were calculated by the mean values of two tests at baseline of systolic blood pressure (Field 4080) and diastolic bold pressure (Field 4079). The baseline diagnosis of diabetes was derived from self-reported and UK routinely-collected healthcare data, including any occurrence of insulin-dependent diabetes mellitus (E10), non-insulin-dependent diabetes mellitus (E11), malnutrition-related diabetes mellitus (E12), other specific diabetes mellitus (E13), and unspecific diabetes mellitus (E14). Of note, the APOE ɛ4 genotype was imputed based on merged UK10K and 1000Genomes phase 3 panels, and other covariates were imputed by random fill.
Statistical analysis
To evaluate the validity of the self-reported data on oral health problems, we used the logistic regression models to assess the relationships between baseline oral health problems and oral disease diagnoses, adjusting for age, sex, race, and APOE ɛ4 carrier status. We also compared the number of participants with oral health problems between groups stratified by oral diseases.
Multivariable Cox proportional hazards regression was used to investigate the associations between oral health problems and incident dementia. Follow-up was calculated in persons from recruitment until the date of first dementia diagnosis, death, loss to follow-up, or the last date with available information from hospital admission (July 2022). In the present study, we used three models to evaluate the associations between baseline oral health problems and incident dementia. Model 1 was controlled for baseline age, sex, race, and APOE ɛ4 carry status. Model 2 additional adjustment variables included educational level, Townsend deprivation index, and BMI. Model 3 additionally adjusted for smoking, alcohol drinking, blood pressure, and diabetes. We defined the oral health problems that were significantly associated with all-cause dementia as dementia-related oral health problems.
Then, we further explored the associations between oral health problems and two main subtypes of dementia (Alzheimer’s disease (AD) and vascular dementia). In addition, to test the robustness of these associations, we performed two sensitivity analyses. Firstly, we excluded participants with follow-up periods of less than 3 years and 5 years to reduce the possible reverse causality bias and repeated the main analyses using the model 3. Secondly, as late-onset dementia was more likely to be found in older participants, we performed sensitivity analyses after excluding participants with a baseline age of fewer than 50 years old.
To explore the associations between dementia-related oral health problems and longitudinal cognitive decline, linear mixed-effects models were used to estimate β-coefficients and standard errors for the associations between oral health problems and annual change in 5 cognitive assessments scores, with follow-up time (in years) as the time scale. The fixed effect included baseline oral health status, follow-up time, and their interaction. The random effect was random intercept, allowing the individual differences at baseline. Age, sex, race, and APOE ɛ4 carry status were adjusted. In the sensitivity analyses, we additionally adjusted for baseline age, sex, race, APOE ɛ4 carry status, educational level, Townsend deprivation index, BMI, smoking, alcohol drinking, blood pressure, diabetes, and baseline cognitive scores as well. To further explore the relationships between oral health problems and cognitive decline in the non-dementia population, we excluded participants who developed dementia during the follow-up and repeated the main analyses and sensitivity analyses.
To explore the associations between dementia-related oral health problems and regional cortical surface area, we used linear regression to estimate β-coefficients and standard errors of the associations between oral health problems and the standardized surface area of 68 cortical regions measured by MRI imaging. Main analyses were adjusted for age, sex, race, and APOE ɛ4 carry status. We also performed sensitivity analyses adjusting for baseline age, sex, race, APOE ɛ4 carry status, educational level, Townsend deprivation index, BMI, smoking, alcohol drinking, blood pressure, and diabetes. For the oral health problem significantly related to both brain structures and dementia incidence, structural equation models (SEM) were used to investigate whether the association of oral health with incident dementia was mediated by brain structures. The latent variable of brain structure was derived from the cortical surface area significantly correlated with the oral health problem.
We further explored other potential mediators underlying the associations between oral health problems and incident dementia. Mediation models were used to examine the mediating effects of smoking, alcohol drinking, diabetes, and blood pressure, adjusting for baseline age, sex, race, and APOE ɛ4 carry status.
In the current study, the results were presented as hazard ratio (HR) with a 95% confidence interval (CI) or standard estimate (β) with standard error (se). A two-tailed p-value after Bonferroni correction of less than 0.05 was considered to be statistically significant. The statistical analyses were performed in R (v 4.0.4) using the packages of survival (v 3.2-11), lme4 (v 1.1-30), and lavaan (v 0.6-9).
RESULTS
Sample characteristics
A total of 425,183 participants without baseline dementia were included in longitudinal analyses of associations between oral health status and incident dementia. During the follow-up period, 7,372 (1.73%) incident dementia events were recorded. Among the 7,372 dementia participants, the mean age at baseline was 62.24 (standard deviation [SD] 4.77), 3,514 (47.7%) participants were female, and the mean follow-up period was 9.00 years (SD 2.93). 2,228 participants had AD, 1,229 participants had vascular dementia, 2,728 participants had unspecific dementia, 581 participants had dementia in other diseases, and 606 participants had dementia (algorithmically-defined) that could not be classified. Among the 417,811 dementia-free participants, the mean age at baseline was 56.85 (standard deviation [SD] 8.01), 226,351 (54.2%) participants were female, and the mean follow-up period was 8.89 years (SD 2.86) (Table 1).
Baseline characteristics of study participants by incident dementia status
*Diagnosed at baseline (without self-reported diagnoses).
Validity of the self-reported oral health problems data
Dental caries was associated with higher rates of mouth ulcers (p = 0.015), painful gums (p < 0.001), loose teeth (p = 0.003), toothaches (p < 0.001), and dentures (p < 0.001). Pulp and periapical tissues diseases were associated with higher rates of painful gums (p < 0.001), bleeding gums (p = 0.001), loose teeth (p < 0.001), toothaches (p < 0.001), and dentures (p < 0.001). Gingivitis and periodontal diseases were also associated with higher rates of mouth ulcers (p < 0.001), bleeding gums (p < 0.001), painful gums (p < 0.001), loose teeth (p < 0.001), toothaches (p < 0.001), and dentures (p < 0.001) (Supplementary Table 1). Besides, we also found there were higher rates of baseline oral health problems in groups diagnosed with dental caries, pulp and periapical tissues diseases, or gingivitis and periodontal diseases, compared with groups without the above diseases (Supplementary Tables 2–4).
The associations between oral health problems and incident all-caused dementia in sensitivity analyses
Adjusted for baseline age, sex, race, APOE ɛ4 carry status, educational level, Townsend deprivation index, BMI, smoking, alcohol drinking, blood pressure, and diabetes. HR, hazard ratio; CI, confidential interval; p, p-value.
Relationships between oral health problems and incident dementia
In the Cox proportional hazards regression analyses of all-cause dementia (significant p < 0.0028 [0.5/18]), painful gums (HR = 1.47, 95% CI [1.317–1.647], p < 0.001), loose teeth (HR = 1.22, 95% CI [1.106–1.349], p < 0.001), toothaches (HR = 1.38, 95% CI [1.244–1.538], p < 0.001), and dentures (HR = 1.28, 95% CI [1.223–1.349], p < 0.001) were associated with an increased risk of all-cause dementia, after adjusting for baseline age, sex, race, and APOE ɛ4 carry status. However, there was no evidence for the association between mouth ulcers, bleeding gums, and incident dementia. When stratifying the main analyses by dementia subtypes (significant p < 0.0028 [0.5/18]), the significance remained in associations of dentures (HR = 1.20, 95% CI [1.097–1.311], p < 0.001) with a higher risk of AD. A higher risk of incident vascular dementia was still observed in participants with painful gums (HR = 2.11, 95% CI [1.660–2.669], p < 0.001), loose teeth (HR = 1.42, 95% CI [1.131–1.782], p = 0.002), toothaches (HR = 1.30, 95% CI [1.057, 1.587], p < 0.001), and dentures use (HR = 1.55, 95% CI [1.383–1.744], p < 0.001) with vascular dementia (Fig. 2, Supplementary Table 5).
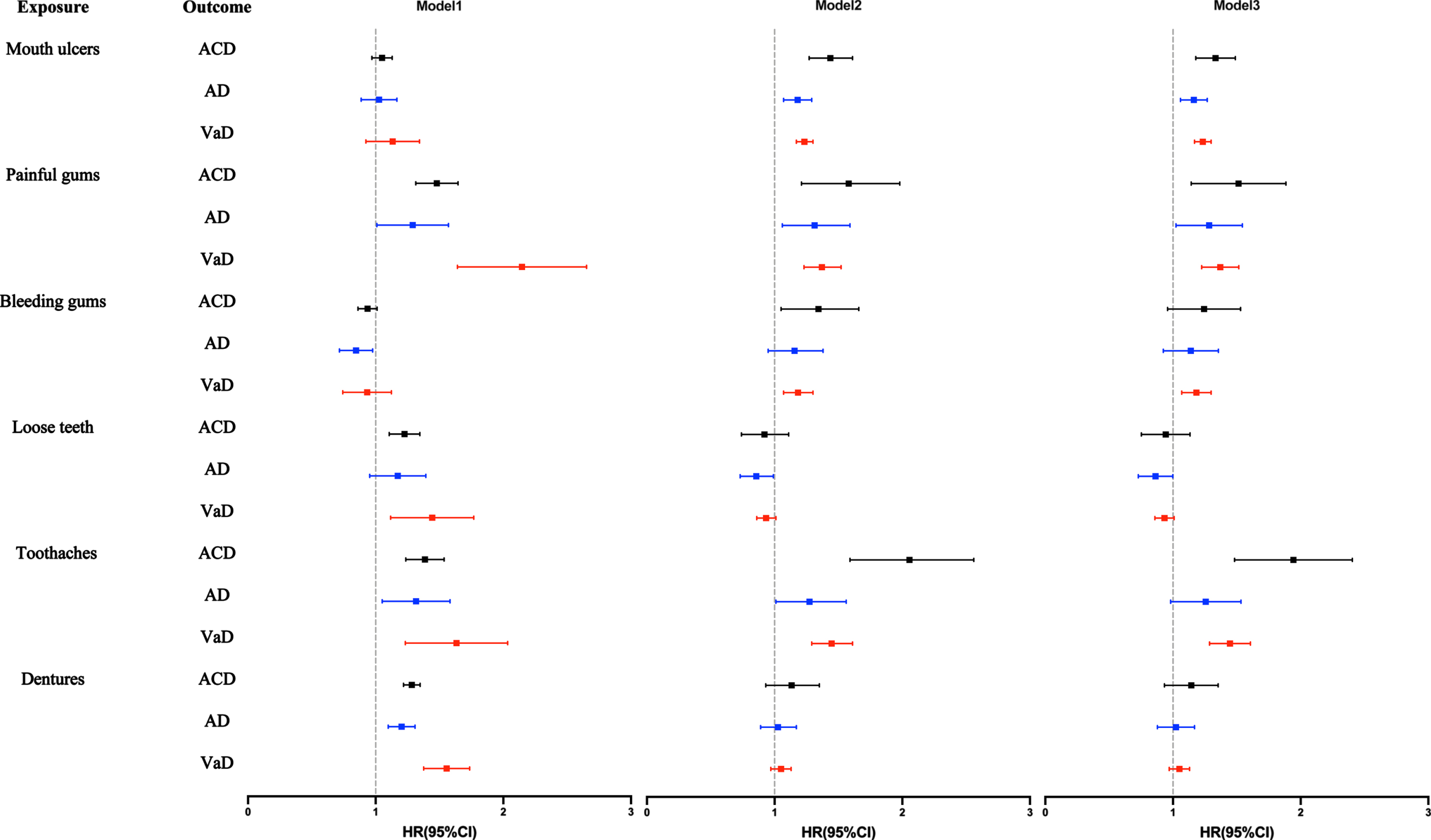
Associations between oral health problems and risk of incident all-cause dementia, Alzheimer’s disease, and vascular dementia. The results are derived from Cox proportional hazard regression models. Model 1: Adjusted for baseline age, sex, race, and APOE ɛ4 carry status. Model 2: Adjusted for baseline age, sex, race, APOE ɛ4 carry status, education, socioeconomic status, and BMI. Model 3: Adjusted for baseline age, sex, race, APOE ɛ4 carry status, education, socioeconomic status, BMI, smoking, alcohol drinking, blood pressure, and diabetes. HR, hazard ratio; CI confidence interval; ACD, all-cause dementia; AD, Alzheimer’s dementia; VaD, vascular dementia.
In model 2, we additionally adjusted educational level, socioeconomic status, and BMI, and the associations between oral health problems and incident all-caused dementia were largely unchanged (Fig. 2, Supplementary Table 5). Painful gums (HR = 1.44, 95% CI [1.288–1.610], p < 0.001), loose teeth (HR = 1.18, 95% CI [1.069–1.304], p = 0.001), toothaches (HR = 1.36, 95% CI [1.227–1.517], p < 0.001), and dentures (HR = 1.23, 95% CI [1.174–1.296], p < 0.001) were associated with an increased risk of all-cause dementia. Participants with dentures (HR = 1.18, 95% CI [1.074–1.287], p < 0.001) at baseline had a higher risk of AD, while only painful gums (HR = 2.02, 95% CI [1.594–2.563], p < 0.001), loose teeth (HR = 1.55, 95% CI [1.209–1.984], p = 0.001), and dentures (HR = 1.43, 95% CI [1.273–1.610], p < 0.001) were still related with a higher risk of incident vascular dementia in model 2.
In the model 3, only participants with painful gums (HR = 1.40, 95% CI [1.252–1.565], p < 0.001), toothaches (HR = 1.33, 95% CI [1.194–1.477], p < 0.001) and dentures (HR = 1.19, 95% CI [1.133–1.252], p < 0.001) at baseline had a higher risk of all-cause dementia, additionally adjusting for smoking, alcohol drinking, blood pressure, and diabetes. Participants with dentures (HR = 1.16, 95% CI [1.059–1.272], p = 0.001) at baseline had a higher risk of AD. Painful gums (HR = 1.91, 95% CI [1.504–2.420], p < 0.001), loose teeth (HR = 1.48, 95% CI [1.258–1.901], p = 0.002), and dentures (HR = 1.33, 95% CI [1.177–1.494], p < 0.001) were also related with a higher risk of incident vascular dementia.
Taken together, we found that painful gums, toothaches, and dentures at baseline were associated with a higher risk of all-cause dementia and vascular dementia in all three models. Only dentures at baseline were associated with a higher risk of AD.
To reduce the possible reverse causality bias, we excluded participants with follow-up periods of less than 3 years and 5 years. Painful gums (> 3 years: HR = 1.34, 95% CI [1.195–1.507], p < 0.001; > 5 years: HR = 1.29, 95% CI [1.137–1.454], p < 0.001), toothaches (> 3 years: HR = 1.33, 95% CI [1.195–1.485], p < 0.001; > 5 years: HR = 1.33, 95% CI [1.186–1.486], p < 0.001), and dentures (> 3 years: HR = 1.20, 95% CI [1.137–1.259], p < 0.001; > 5 years: HR = 1.20, 95% CI [1.135–1.262], p < 0.001) were consistently associated with a higher risk of dementia incidence. Additionally, we also found that painful gums (HR = 1.37, 95% CI [1.220–1.533], p < 0.001), toothaches (HR = 1.30, 95% CI [1.164–1.448], p < 0.001), and dentures (HR = 1.19, 95% CI [1.135–1.255], p < 0.001) were related to increased risk of dementia in older age group (> 50 years old).
Relationships between oral health problems and cognitive decline
In the mixed linear models where “oral health status x Time” was treated as the predictors (significant p < 0.0033 [0.5/15]), the dentures were significantly associated with accelerated decline in cognitive function, adjusted for baseline age, sex, race, and APOE ɛ4 carry status (Fig. 3). Compared to the decline rate of participants without dentures, participants with dentures experienced a faster increase in reaction time (β for additional annual change = 0.004, standard error [se] = 0.001, p = 0.002), and a more rapid decrease in numeric memory (β for additional annual change = –0.020, se = 0.006, p = 0.001) and prospective memory (β for additional annual change = –0.004, se = 0.001, p < 0.001) (Supplementary Table 6). However, we did not observe a significant association with other oral health problems related to dementia incidence and the rate of cognitive change. In sensitivity analyses, dentures were only associated with faster impairments in reaction time (β for additional annual change = 0.005, se = 0.001, p < 0.001), and prospective memory (β for additional annual change = –0.009, se = 0.003, p = 0.002). adjusted for baseline age, sex, race, APOE ɛ4 carry status, educational level, Townsend deprivation index, BMI, smoking, alcohol drinking, blood pressure, diabetes, and baseline cognitive scores (Supplementary Table 6).

Associations between dentures and prospective cognitive decline. The results are derived from mixed linear models adjusted for sex, age at baseline, race, and APOE ɛ4 carry status. The y-axes represent the performance of cognitive test: left: the period of reaction time (ms), higher is worse; middle: score of numeric memory test, possible score range 2 to 12, lower is worse; right: the possibility of “correct on the first attempt” in the prospective memory test, lower is worse. This figure shows follow-up time-related cognitive trajectories in reaction time, numeric memory, and prospective memory. β, standardized estimate; p, p-value.
To further explore the associations between oral health problems and cognitive decline in the non-dementia population, we excluded the participants who developed dementia in the follow-up period. Participants with dentures experienced a faster decrease in numeric memory (β for additional annual change = –0.019, se = 0.006, p = 0.001) and prospective memory (β for additional annual change = –0.004, se = 0.001, p < 0.001) in main analyses (Supplementary Table 7). After additionally adjusting for educational level, Townsend deprivation index, BMI, smoking, alcohol drinking, blood pressure, diabetes, and baseline cognitive scores, we found that dentures were associated with more rapid impairments in reaction time (β for additional annual change = 0.005, se = 0.001, p < 0.001) and prospective memory (β for additional annual change = –0.009, se = 0.003, p < 0.002).
Relationships between oral health problems and regional cortical surface areas
In linear regression analyses for MRI data (significant p < 0.0002 [0.5/204]), dentures were associated with smaller areas of the inferior temporal cortex in the left hemisphere (β= –0.079, se = 0.016, p = 6.159E-07), inferior parietal cortex in both side hemisphere (left: β= –0.076, se = 0..017, p = 4.048E-06, right: left: β= –0.064, se = 0.016, p = 5.889E-05), and both side middle temporal cortex (left: β= –0.067, se = 0.016, p = 1.905E-05, right: left: β= –0.067, se = 0.016, p = 1.601E-05) (Supplementary Table 6, Fig. 4). We found no statistical links between other oral health problems and the cortical areas after Bonferroni correction. In the fully-adjusted models, the associations between dentures and areas of the inferior temporal cortex in the left hemisphere (p = 0.001), both sides inferior parietal cortex (left: p = 0.002, right: p = 0.013), and both sides of the middle temporal cortex (left: p = 0.012, right: p = 0.006) were in the same direction, while the p-values could not pass the Bonferroni corrections (Supplementary Tables 7–10).
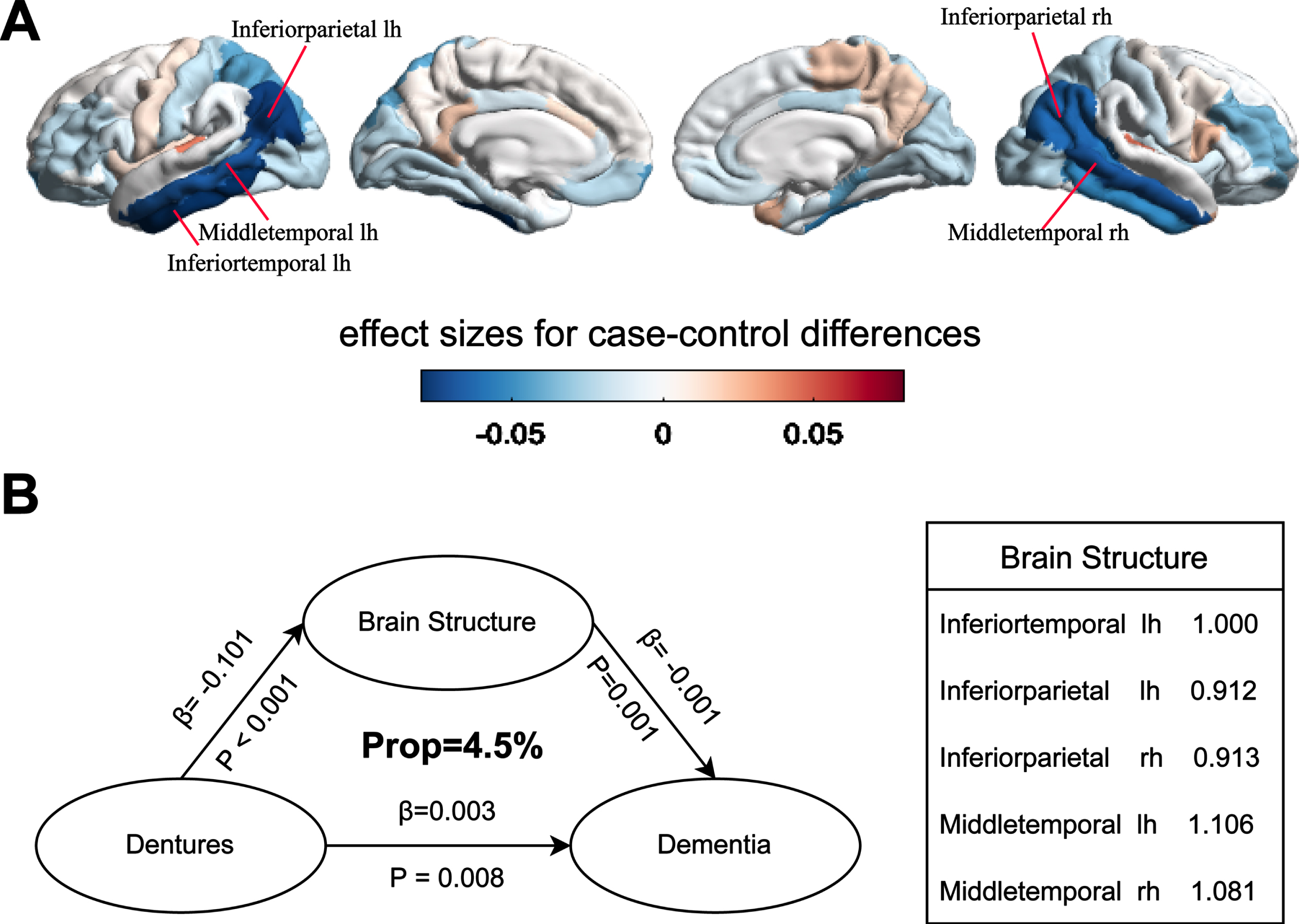
Associations between dentures, regional brain surface area, and incident dementia. A) Associations between dentures and regional brain surface area. Compared with the control, participants with dentures had smaller surface areas of the inferior temporal cortex, inferior parietal cortex, and middle temporal cortex. B) Structural equation model incorporating dentures, brain structures, and incident dementia. Brain structure was a latent variable showing with the right box. All paths represent significant associations (p < 0.05). The brain structure mediated the association between dentures use and incident dementia (path1: β= –0.101, p < 0.001; path2: β= –0.001, p = 0.001), and the mediating effect was 4.5%.
Mediating effects underlying the associations between oral health problems and incident dementia
As dentures were significantly associated with both dementia incidence and regional cortical surface areas, we further specified the mediation association between dentures, regional cortical surface areas, and dementia incidence using structural equation modeling. The model fitted the data well (comparative fit index = 0.961, root-mean-square estimate = 0.101), and all associations in the model were significant (with p < 0.05) and in the expected direction (Fig. 4). The brain structure related to dentures mediated the association between dentures use and incident dementia (path1: β= –0.101, p < 0.001; path2: β= –0.001, p = 0.001), and the mediating effect was 4.5%.
We also found smoking, alcohol drinking, and diabetes could mediate all three oral health problems-dementia associations. For the association between painful gums and dementia, smoking (mediating effect = 1.9%, p < 0.001), alcohol drinking (mediating effect = 1.3%, p < 0.001), diabetes (mediating effect = 10.2%, p < 0.001), and blood pressure (mediating effect = 0.7%, p < 0.001) had mediating effects. For the association between toothaches and dementia, smoking (mediating effect = 1.7%, p < 0.001), alcohol drinking (mediating effect = 2.4%, p < 0.001), diabetes (mediating effect = 8.7%, p < 0.001), and blood pressure (mediating effect = 0.5%, p = 0.005) had mediating effects. Only smoking (mediating effect = 2.0%, p = 0.002), alcohol drinking (mediating effect = 1.2%, p < 0.001), and diabetes (mediating effect = 9.3%, p < 0.001) mediated the association between dentures and incident dementia (Supplementary Table 13).
DISCUSSION
In this population-based prospective study, we found that 1) painful gums, toothaches, and dentures were associated with increased risk of incident dementia; 2) dentures were associated with accelerated decline in cognitive functions, including longer reaction time, worse numeric memory, and worse prospective memory; 3) dentures were associated with smaller surface areas of the inferior temporal cortex, inferior parietal cortex and middle temporal cortex; and 4) the association between dentures and the risk of incident dementia was mediated by the change of cortical surface area. Smoking, alcohol drinking, and diabetes could mediate all three oral health problems-dementia associations.
The present study used self-reported oral health problems as the main exposures. We examined the associations between oral health problems and diagnoses of dental caries/pulp and periapical tissues diseases/gingivitis and periodontal diseases and found oral health problems were correlated with a higher prevalence of oral diseases. Therefore, we supposed that oral health problems were closely related to oral diseases and have the potential to reflect an average oral health status to some extent.
Our findings revealed that poor oral health statuses, such as having painful gums, toothaches, and dentures, could be a risk factor for incident dementia. Previous studies showed poor periodontal health, including periodontitis, tooth loss, deep periodontal pockets, and alveolar bone loss, was associated with cognitive decline, dementia, and AD [7–9, 21, 22]. As the main sources of painful gums, toothaches, loose teeth, and denture use, periodontal disease was one of the most common chronic inflammatory diseases [23, 24]. Periodontal disease could be marked as a “low-grade systemic disease” by the release of proinflammatory cytokines into the systemic circulation and elevation of C-reactive protein (CRP), which was thought to be a strong risk factor for developing a variety of systemic diseases including AD [25]. In sensitivity analyses, we found the associations between painful gums, toothaches, dentures, and dementia were still significant when we excluded participants with follow-up periods less than 3 and 5 years, indicating the possible causal relationships between poor oral health and dementia incidence. The results were also robust in an older subgroup of participants, suggesting the associations between oral health status and late-onset dementia.
In our study, we found the associations between oral health problems and incident dementia differed depending on the classification of dementia, with the risk being stronger for vascular dementia and weaker for AD. Only dentures were associated with both incident AD and vascular dementia, while painful gums and toothaches were exclusively associated with vascular dementia. This may suggest a closer relationship between oral health and vascular dementia. Diet and nutrition may explain this finding. Individuals with oral pain or chewing disability were more likely to have diets high in saturated fats and cholesterol, possibly owing to the ease of chewing these foods relative to fiber-rich food. Changes in diet may raise the risk of stroke and vascular dementia [26, 27]. Our findings showed that the associations between loose teeth and vascular dementia weakened when we additionally adjusted for education, socioeconomic status, lifestyles, and health conditions. This indicated the potential mechanisms, and further studies were required to test such mechanisms.
Dentures were associated with a higher risk of incident dementia, and more rapid cognitive decline including longer reaction time, worse numeric memory, and prospective memory. However, the association between dentures and faster decline of numeric memory attenuated after adjusting for lifestyles, health conditions, and baseline cognitive scores. In the non-dementia population, dentures were still associated with accelerated cognitive impairments, especially prospective memory. Despite being rehabilitated, denture wearers still had impaired masticatory efficiency [28]. Previous studies found poor chewing ability was related to lower cognitive functions, measured with different cognitive testers such as Mini-Mental State Examination, and other executive functions, such as world fluency, Stroop color-word test, and trail-making B [29].
We also found dentures were related to the smaller surface area of the inferior temporal cortex, inferior parietal cortex, and middle temporal cortex, which were associated with a variety of cognitive functions including working memory, short-term visual memory, object recognition, declarative memory, semantic knowledge, and intention understanding [30, 31]. Of note, after adjusting for smoking, alcohol drinking, diabetes, and blood pressure, the above associations were still in the same direction but attenuated. This may suggest more complex relations between oral health status and brain structures. Furthermore, the association between dentures and the risk of incident dementia may be mediated by the changes in regional cortical areas. Some other studies found poor chewing ability was associated with smaller gray matter volume of the premotor cortex, primary motor cortex, hippocampus, parahippocampus, caudate nucleus, and temporal pole, and suggested that deficient masticatory efficiency may be associated with brain signatures of a widespread area, as well as cognitive impairment [12, 13].
We noticed that the mediating effects of brain structures on the association between dentures and dementia were only 4.5%, which was small. In addition, the mediating effects of smoking, alcohol drinking, and diabetes on the associations between oral health problems and dementia were also relatively small, ranging from 1.2% to 10.2%. Among those factors, diabetes was the one that had the largest mediating effect. Therefore, we supposed that the relationships between oral health problems and dementia were connected by a group of complex traits, and further studies were required.
The strengths of the present study included the large population and the long follow-up period, which improved the precision of our findings. Furthermore, we were the first to explore the mediation effect of brain structure on the association between oral health and incident dementia, providing new insight into the mechanism of the oral-cognition relationship. The current study also had several limitations. First, due to the long preclinical phase of dementia, we cannot rule out the possibility of reverse causality. However, we have restricted analyses to participants without dementia at baseline and conducted sensitivity analyses after excluding participants with follow-up periods less than 3 and 5 years to minimize the possible reverse causality. Secondly, we used self-reported oral health problems as exposures, which were relatively vague markers. We did some validation analyses and found close associations between self-reported oral health problems and diagnosed oral diseases. However, the possible recall bias and reported bias should also be paid attention to. Thirdly, the use of hospital in-patient, primary care, and death records to capture dementia could introduce misclassification bias. While there was evidence for a relatively low false-positive rate, the rate of false negatives still was largely unknown [15]. Lastly, the cognitive assessments employed in UK Biobank were novel due to the need to conduct brief computerized cognitive assessments in a very large population, and it was not possible to create cognitive domain scores using available data of cognitive tests [17]. It did not include classic tests of learning and delayed memory and it used bespoke tasks, which were not directly comparable to standard clinical measures [32]. Thus, further studies using more detailed cognitive assessments are needed.
Our findings suggested that poor oral health including painful gums, toothaches, and dentures was associated with an increased risk of incident dementia. Participants with dentures experienced more rapid prospective cognitive decline. Furthermore, dentures were associated with smaller surface areas of the inferior temporal cortex, inferior parietal cortex, and middle temporal cortex, and the brain structural change may underlie the association of dentures and increased risk of incident dementia. Smoking, alcohol drinking, and diabetes may also have mediating effects on the associations between oral health problems and incident dementia. Given the strength of the association between poor oral health and incident dementia, the promotion of oral health care would be beneficial for the prevention of dementia incidence. However, the underlying mechanisms of this association still need further investigation.
Footnotes
ACKNOWLEDGMENTS
This research has been conducted using the UK Biobank Resource under Application Number 19542. We would like to thank all the participants and researchers from the UK Biobank.
FUNDING
This study was supported by grants from the Science and Technology Innovation 2030 Major Projects (2022ZD0211600), National Natural Science Foundation of China (82071201, 82071997), Shanghai Municipal Science and Technology Major Project (2018SHZDZX01), Research Start-up Fund of Huashan Hospital (2022QD002), Excellence 2025 Talent Cultivation Program at Fudan University (3030277001), Shanghai Talent Development Funding for The Project (2019074), Shanghai Rising-Star Program (21QA1408700), 111 Project (B18015), and Zhangjiang Lab, Tianqiao and Chrissy Chen Institute, the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, and Shanghai Center for Brain Science and Brain-Inspired Technology, Fudan University. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
CONFLICT OF INTEREST
Prof. Jin-Tai Yu is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
All other authors have no conflict of interest to report.