
Abstract
Background:
Depression is one of the most common symptoms in patients with dementia.
Objective:
This meta-analysis aimed to evaluate the effect of light therapy on depression associated with dementia by using a single scale.
Methods:
Published studies based on the terms including “Dementia”, “depression”, and “Phototherapy” were searched. Web of Science, PubMed, Embase, CiNii, CNKI, Wanfang Database, and China Biology Medicine disc were adopted to collect randomized controlled studies or cross-controlled studies using the Cornell Scale for Depression in Dementia (CSDD) until February 2022. GRADE and Review Manager Version 5.4.1 were employed to assess the risk of bias. A meta-analysis was conducted by R 4.0.2 software based on the changes in CSDD scores.
Results:
A total of 1,055 studies were retrieved from the databases, and six studies were included after screening. Some 406 people with dementia were included with an average age of over 80 years. Forest plot results showed that light intervention improved depression scores of dementia patients (MD = –2.59, 95% CI: –4.46 to –0.71), and light intensity less than 1,000 lux improved depression symptoms of dementia patients (MD = –2.76, 95% CI: –4.55 to –0.97). An intervention that lasted 8 to 12 weeks was the most effective (MD = –3.77, 95% CI: –6.93 to –0.60), and non-stable interventions such as ceiling LED lights exerted more positive effects (MD = –2.12, 95% CI: –3.38 to –0.85).
Conclusion:
The overall results of the meta-analysis suggested that light intervention can improve the depressive symptoms of older patients with dementia.
Keywords
INTRODUCTION
The number of people with dementia worldwide continues to increase, from 55 million in 2019 to an estimated 139 million in 2050. Every 3 seconds someone in the world develops dementia [1]. Dementia is accompanied by severe behavioral and psychological symptoms of dementia, such as depression, which is one of the most common symptoms. Depression accounts for about 20% to 30% of all patients with dementia [2]. Compared with people without dementia, patients with dementia have twice the risk of depressive symptoms [3], which not only makes patients with dementia depressed and affects their life, but also increases the difficulty of nursing them. Conventional medical treatment often causes side-effects such as nausea and headaches in patients with dementia [4], so safer, non-medical treatments are receiving attention. As one of the non-drug treatment methods, light therapy shows the advantages of convenience and feasibility. Light is an important part of maintaining the body clock [5, 6]. The body clock plays an important role in circadian rhythms, which can affect physiological indicators such as hormone levels, body temperature, sleep, and mood [7, 8]. Older adults need higher light levels to maintain their circadian rhythm due to the deterioration of eye function.
Many studies show that light therapy can improve depression in patients with dementia [9–11]; however, other studies have found that light therapy is ineffective [12–14], or some even make symptoms worse [15, 16]. Some meta-analyses explored the effects of light therapy on depression in the older persons with dementia [17–20]. Although the SMD index can be used for statistical analysis, through the conversion of results into measures of effect in terms of mathematical statistics, some uncertain results may arise because of dementia patients’ specificity. As their degree of dementia worsens, it becomes more difficult for them to complete the corresponding scales. The methods vary with different scales to acquire information, which leads to variation in data sampling. It may produce different results for dementia patients if clinicians combine research data from different psychometric scales in meta-analyses [21]. This will increase the heterogeneity.
These results differ for two reasons: on the one hand, there are many types of depression scales; most depression rating scales are based on information provided by patients themselves. For example, the Zung Self-Rating Depression Scale is completed by the patient, but, Knesevich et al. (1983) noted that 23% of the patients were unable to complete the Zung Self-Rating Depression Scale due to cognitive impairment [22]. In addition to the self-rating scale, the Hamilton Depression Rating Scale is rated by a psychiatrist using information obtained from interviews with the patient, but, patients with moderate or severe dementia cannot be reliably assessed from information obtained from structured interviews alone [23]. It is problematic if findings are based only on the information provided by the patients, because depressed patients have disorders in attention, memory, and judgment and their mood is unstable [24]. The Cornell Scale is administered in two steps: first, the clinician interviews the patient’s caregiver on each of the 19 items of the Cornell Scale and gives the preliminary scores. Then, based on this result, the clinician briefly interviews the patient with observations on-going therewith. After integrating these results, the clinician calculates the final score. In addition to the high level of both sensitivity and specificity, the method of evaluation of Cornell Scale for Depression in Dementia (CSDD) pays more attention to the nuances of people with dementia, implying the Cornell Scale can be scored for depressive symptoms across the entire range of severity of dementia [23]. On the other hand, the effectiveness of factors related to light therapy is unclear such as light intensity, light intervention, and duration of light therapy. Therefore, this study will use a single scale to conduct a meta-analysis on the effects of light therapy on depressive symptoms of dementia patients, to assess the effects of different light intervention methods on depressive symptoms in dementia.
METHODS
Search strategy
The meta-analysis was conducted following the PRISMA guidelines (Supplementary Table 1) [25]. The published studies were searched from a range of databases: Web of Science, PubMed, Embase, CiNii, CNKI, Wanfang Database, and China Biology Medicine disc, from the establishment of the database until February 2022, based on the subject terms including “Dementia, depression, Phototherapy” and free terms including “Dementia*, Amentia, AD, Alzheimer’s Disease, Cortical Lewy Body Disease, Depressive Symptoms, depress*, Phototherapies, Light Therapy, and Bright Light” both in English and Chinese (Supplementary Table 2).
Inclusion and exclusion criteria
Studies were selected if they met the following inclusion criteria: 1) The study design was a randomized controlled study or cross-controlled study; 2) Participants had been diagnosed with dementia and had no eye disease; 3) The intervention was light therapy, with no restrictions on interventions, including light boxes, customized lighting interventions, and high-light intensity lamps; 4) The Cornell Scale for Depression in Dementia was utilized to measure the degree of depression in patients with dementia; 5) Valid data can be obtained through the original text, contacting the original author, data conversion, and other methods; 6) All included patients completed the requisite informed consent declaration.
Studies were excluded if they corresponded with these criteria: 1) If they were reviews, conference abstracts, or animal experiments; 2) If they were republished studies; 3) Participants in the study were under 60 years old; 4) The control group was not subjected to a low-light intervention or no intervention; 5) The experimental group received both a light intervention and other treatments; 6) The study did not have access to relevant data, and the authors could not be contacted to obtain data.
Cornell scale for depression in dementia
The CSDD [23] consists of 19 items and five sub-scales, each of which reflects the severity of an observable symptom in the preceding week. The higher the CSDD score, the more severe the depression will become. The CSDD scale was shown to have an internal reliability of –0.67 and an internal consistency, as evinced by Cronbach’s α of 0.84 [23]. The validity of CSDD was assessed by the correlation between the CSDD score and the psychiatrist’s research diagnosis (r = 0.83) [17].
Study selection and information extraction
Two investigators independently selected the included studies by reviewing the titles and abstracts and extracted information from the included studies. If there was a disagreement, a third reviewer made a judgment. The information was extracted including: first author, publication year, sample size, study type, light intervention measures, behavior of subjects, light intensity, duration of intervention, and mean and standard deviation of CSDD scores before and after intervention.
Quality of studies
GRADE was used to evaluate the quality of included studies, and Review Manager Version 5.4.1 was adopted to form a summary of the bias risk [26]. There were five risk assessment contents for each article: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), and incomplete outcome data (attrition bias). The study determined the risk level of bias for each item based on the original text, which was divided into three types: low risk, unclear risk, and high risk (+, ?, -). The results were displayed graphically.
Statistical analysis
R 4.0.2 was used for statistical analysis by extracting data from the included studies [27]. The effect size of the study was based on changes in the means and standard deviations of CSDD scores before and after the intervention between the experimental and control groups. Since most studies only reported the means and standard deviations of depression scores before and after the intervention, the changes were calculated according to the methods from the Cochrane Handbook 5.0.2, for instance MeanE,change = MeanE,final - MeanE,baseline and
RESULTS
Screening and evaluation of studies
Search results and screening process
Some 1,055 studies were initially retrieved according to the seven databases. Six studies were identified for meta-analysis according to the multiple screening steps, such as exclusion of duplicates, selection of literature types, systematic review of title and abstract content and reviewing the full text (Fig. 1).
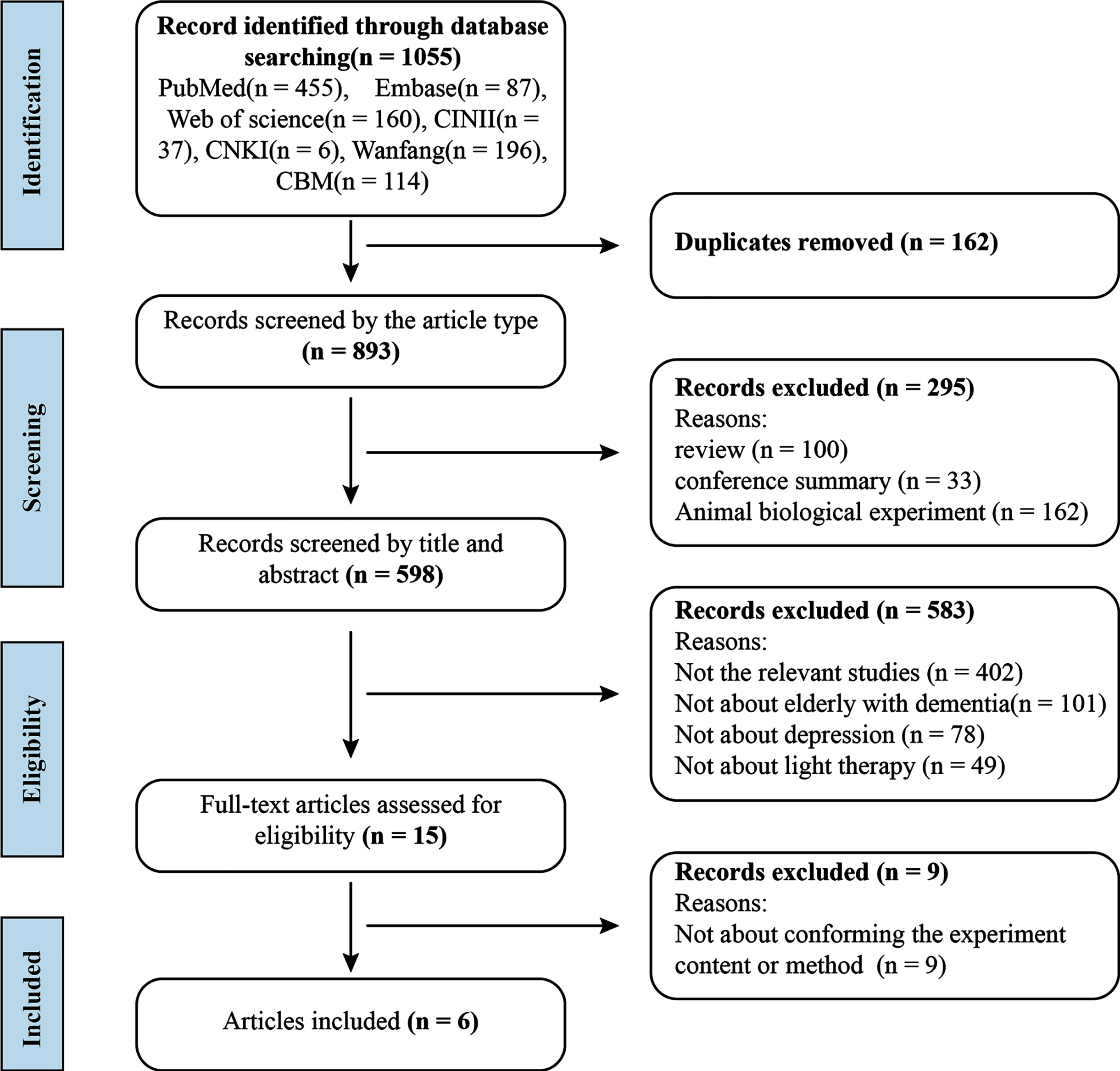
PRISMA flowchart of the literature search on the influence of light therapy for depression of older patients with dementia [25].
Basic information for the inclusion of studies is summarized in Table 1; six studies [10–12, 31–33] measured depression scores all using the CSDD scale for depressive symptoms in dementia. Among them, five studies were randomized controlled trials and one study was a pre- and post-cross-over trial. Six studies were conducted in different locations, one in The Netherlands, one in Great Britain, one in Norway, and three in the USA. The total number of participants was 406, with 209 in the experimental group and 197 in the control group, ranging from 21 to 47 in each group. The average age of the participants was 80 years old, who are mostly from the specialized nursing homes, nursing facilities, or nursing communities specializing in the care of people with dementia and conduct disorders.
Characteristics of included studies (n = 6)
RCT, randomized controlled trial; EG, experimental group; CG, control group; AD, Alzheimer’s disease; FTD, frontotemporal dementia; LBD, Lewy body dementia; VaD, vascular dementia; F, female; M, male.
Most of the participants had Alzheimer’s disease, vascular dementia, or another type(s) of dementia, as diagnosed by the Diagnostic and Statistical Manual of Mental Disorders (4th Edition) (DSM-IV), Mini-Mental State Examination (MMSE) score dementia diagnosis or clinician’s assessment of dementia diagnosis before the trial began. The mean MMSE scores of the participants in the included studies ranged from severe to moderate levels of dementia: 4.0 (Q1 1.0, Q3 9.2) [10]; 5.9 (SD 5.5) [12]; 7.22 (SD 6.85) [11]; 14.4 (SD 6.6) [33]; F = 16.5 (SD 5.0), M = 14.7 (SD 4.3) [31] and no MMSE scores [32].
The light interventions varied in terms of method of light intensity, intervention duration, and type of intervention. In the included studies, the intervention light intensity ranged from 159.3 lux to 10,000 lux in the experimental group, while it was less than 300 lux in the control group. Two studies provided bright light therapy with high illumination (10,000 lux). Both studies employed light boxes [11, 12]. The traditional light-box treatment lasted for about half an hour each time. The participants must keep staring at the light box in front of the lamp, during which they cannot move freely. Two studies provided bright light therapy at 1,000 lux by way of ceiling-mounted fluorescent tubes that allow participants to move freely within designated spaces [10, 33]. Another two studies used daylight (159.3 lux) [32] or custom lighting (350–750 lux) [31]. Four studies lasted for 2 weeks [12], 4 weeks [31], 8 weeks [11], or 12 weeks [32]. One study had an intervention over 3.5 years, and the data were collected at 6 weeks, 6 months, 1 year, 1.5 years, 2 years, 2.5 years, 3 years, and 3.5 years [33]. Another study involved an intervention over 24 weeks, and the data were collected at 8 weeks, 16 weeks, and 24 weeks [10].
Quality of evidence
The quality of evidence in this study is illustrated in Figs. 2 3. The results showed a total of 30 ratings in included studies, including 20 for low risk, seven for unclear risk, and three for high risk. Random sequence generation and allocation concealment belonged to selection bias, which occurred during the selection and allocation of objects. Konis et al. (2018) [32] mentioned non-random clustering experiment, so it was judged as high risk. For the two types of bias, blinding of participants and personnel and blinding of outcome assessment, the judgment was mainly based on whether the blindness was achieved. Four articles mentioned the blinding in the study [10, 33]. Although these studies used different types of intervention, the participants and employees were not told whether they were in the intervention group or the control group. They knew only that the experiment was investigating different types of light effects. Another two studies did not mention the blinding of participants and personnel [12, 32]. The risk of attrition mainly depended on the completeness of the outcome data. In the study undertaken by Riemersma-van der Lek et al. (2008) [33], some follow-up information was missing in many cases, so it was classified as high risk. The rest of the uncertain, unmentioned content belonged to unclear risks. In conclusion, the overall quality of evidence was high in this meta-analysis.
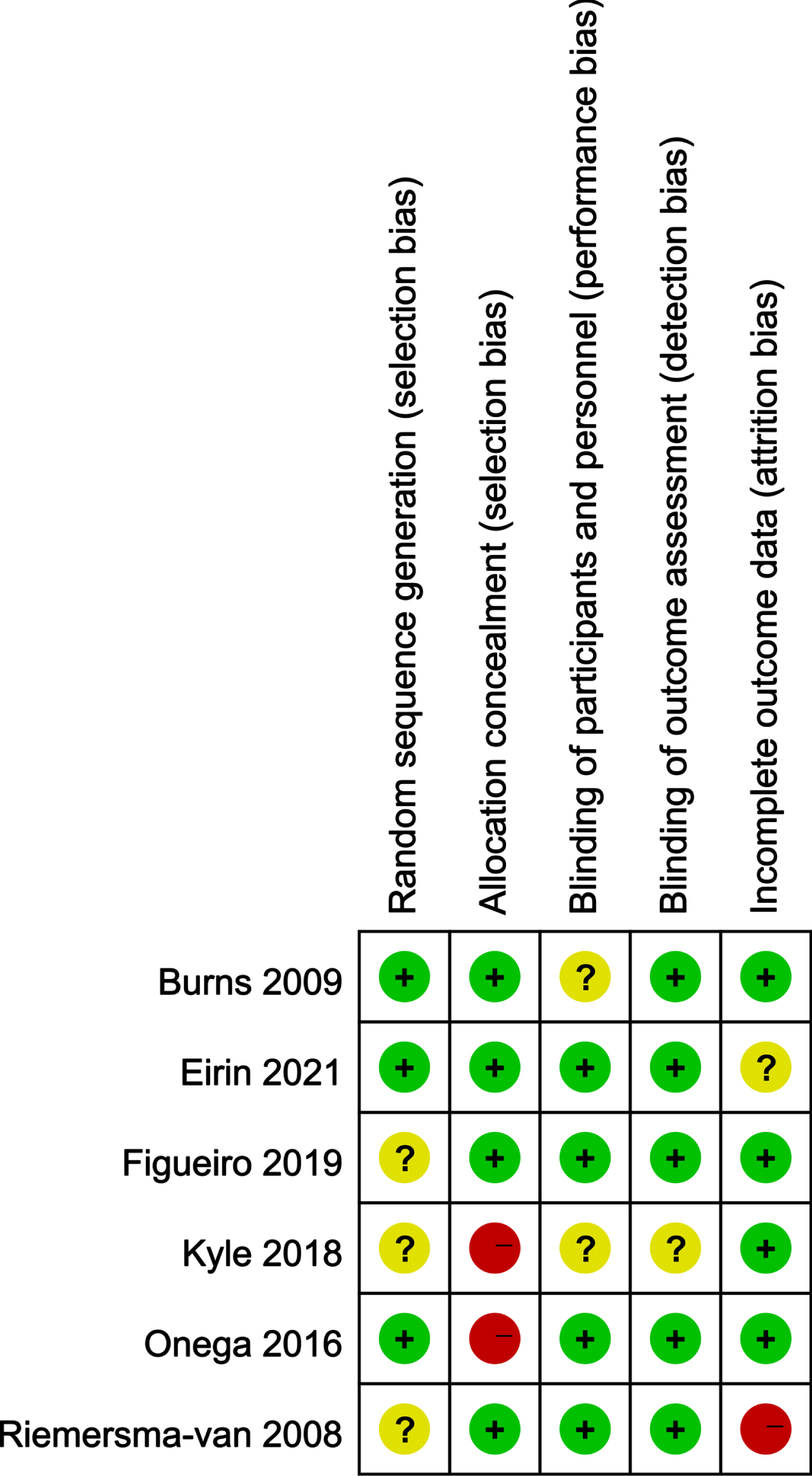
Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
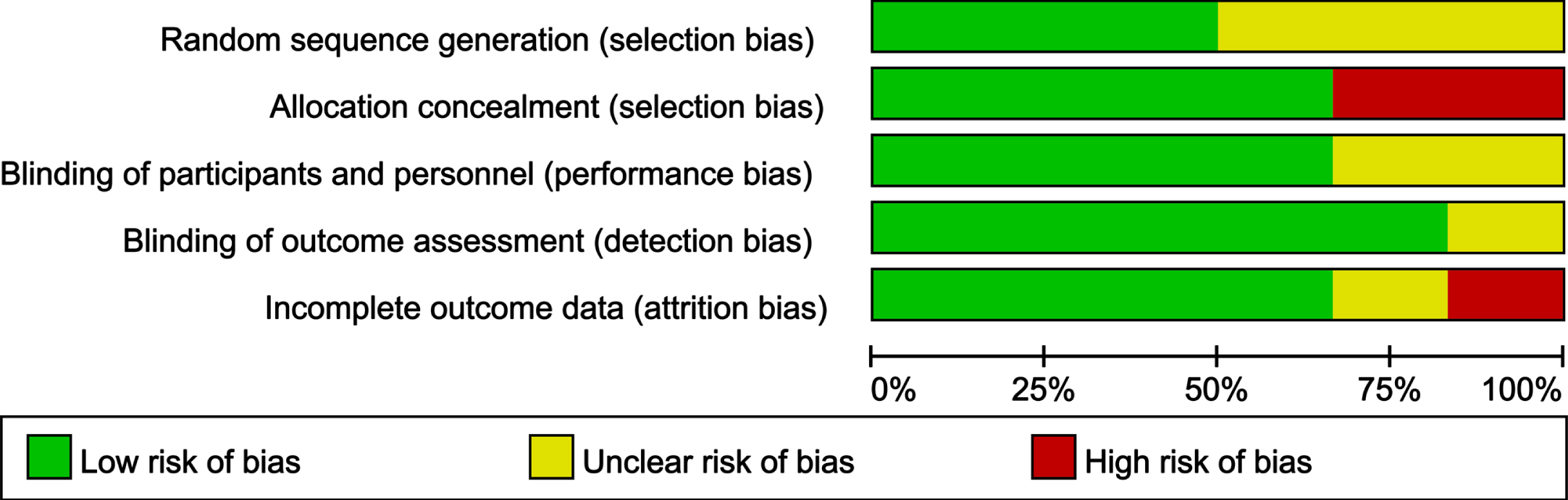
Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
The effect of light therapy on depression of dementia
This study used the random-effects model for meta-analysis due to the statistical heterogeneity among the six studies (I2 = 72%, p < 0.01) (Fig. 4). There was statistical difference in the mean changes in light experimental group and control group (MD=–2.59, 95% CI: –4.46 to –0.71). This finding shows that light therapy can improve depression in dementia patients.
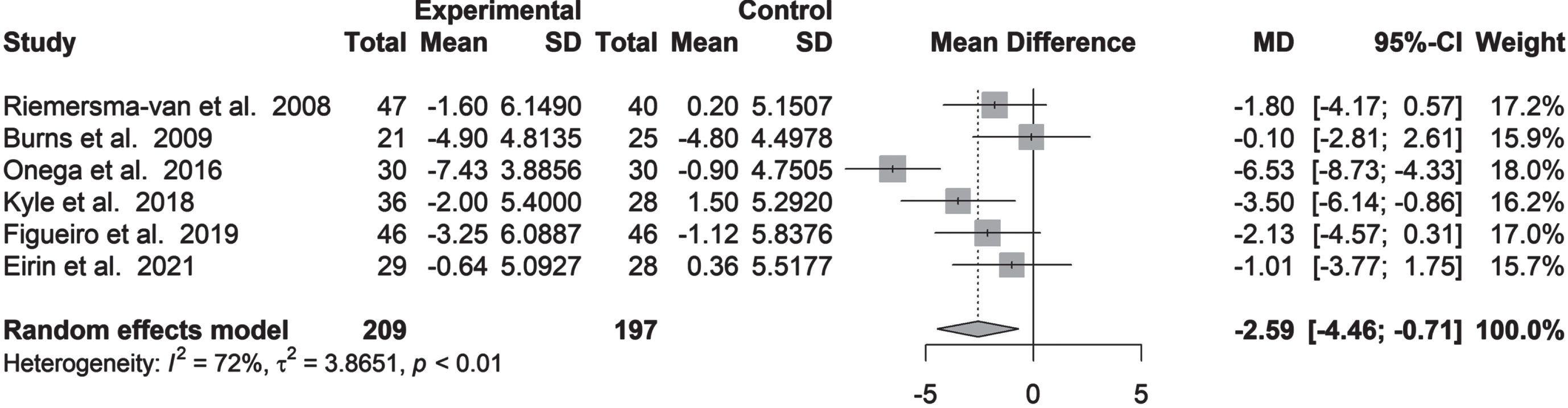
Forest plot: mean difference of depression in light therapy.
The funnel plot method (Fig. 5) and Egger’s test method could be used to estimate publication bias. The results of Egger’s test showed that there was no publication bias in the study (p = 0.074), as also evinced by the funnel plot from the data presentation.
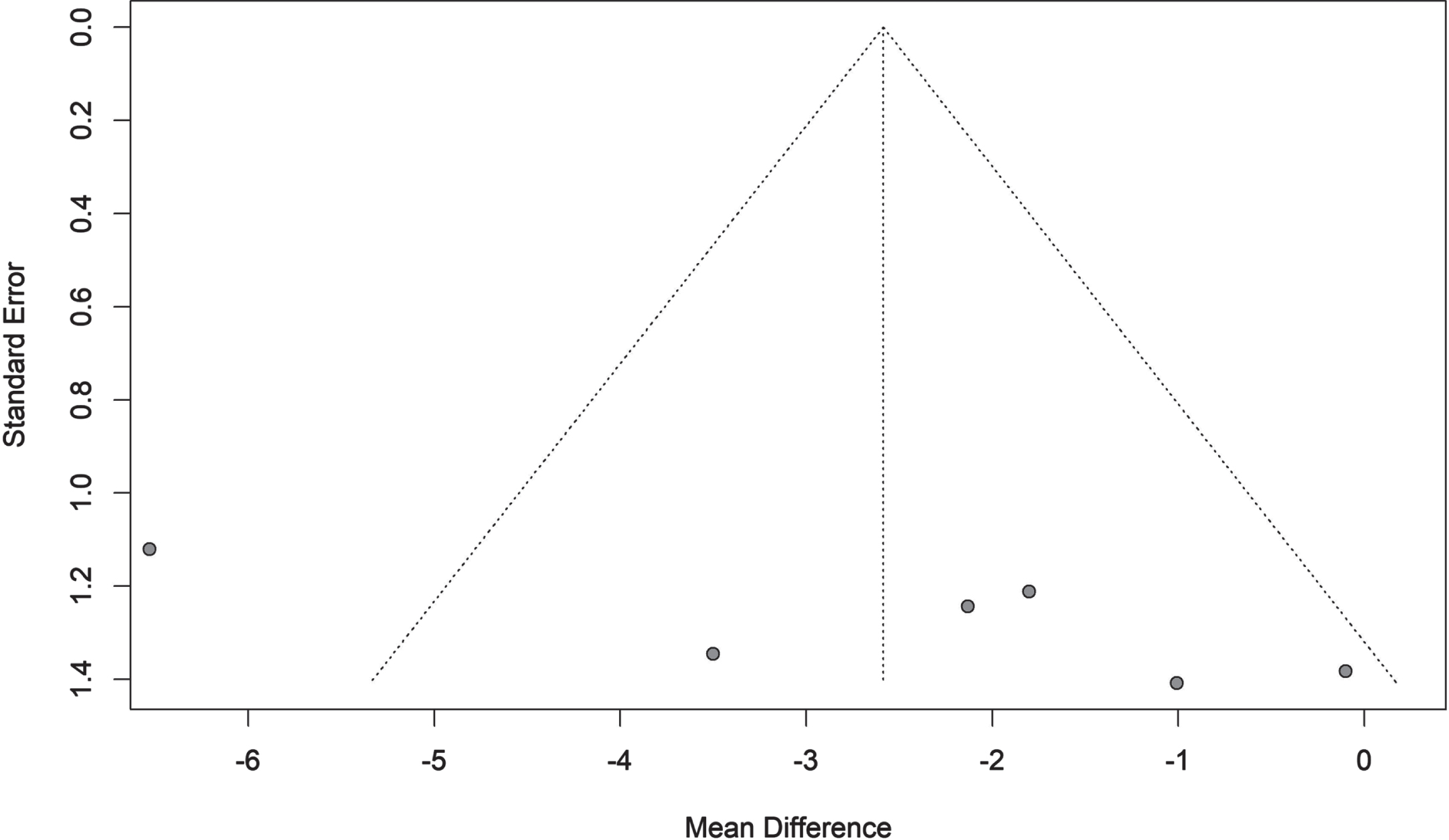
Funnel diagram.
The results of sensitivity analysis implied that the results of meta-analysis remained stable and statistically significant after the exclusion of any study data (Fig. 6).

Sensitivity analysis diagram.
The effect of light intensity on depression of dementia
All six studies reported the effect of light intensity on depression of patients with dementia. According to the light intensity, the experimental groups could be divided into three groups such that: the illumination was 10,000 lux [11, 12], 1,000 lux [10, 33], and less than 1,000 lux [31, 32]. There was no improvement in depression and no statistical differences in the mean difference of the experimental groups compared with the control groups at an illumination of 10,000 lux and 1,000 lux sub-groups (MD = –3.37, 95% CI: –9.67 to 2.93) (MD = –1.46, 95% CI: –3.26 to 0.34). When the illumination was less than 1,000 lux, the fixed-effects model was used for analysis due to no heterogeneity between studies (I2 = 0%). The improvement effect of the light treatment group was better than that of the control group, and the result was statistically significant (MD = –2.76, 95% CI: –4.55 to –0.97). This suggested that a light intensity of less than 1,000 lux had some effect on depression in dementia patients (Fig. 7).

Forest plot of subgroup analysis of light intensity (= 10,000 lux,=1,000 lux,<1,000 lux).
Duration of light therapy on depression of dementia
The effect of intervention duration on depression of dementia was reported in the included studies. In the work undertaken by Riemersma-van der Lek et al. (2008) [33], only 6-week and 6-month data were included, among the 6-week, 6-month, 1-year, 1.5-year, 2-year, and 2.5-year data, due to the decrease of the number of people for whom data were missing compared with the baseline number in the data pertaining to 1-year to 2.5-year (missing data accounted for more than 30% of the total number of participants). In Kolberg et al. (2021) [10], the data at 8 weeks, 16 weeks, and 24 weeks were included, because the number of people in each group was less missing than the number at baseline (Fig. 8). The study was divided into three subgroups based on the duration of light therapy: within 6 weeks (≤6 W), 8 weeks to 12 weeks (8 W to 12 W), and 16 weeks to 6 months (16 W to 6 M). No statistical significance was found within 6 weeks and in 16 weeks to 6 months subgroups, with decreases in depression scores of 1.43 points (95% CI: –2.88 to 0.01) and 0.82 points (95% CI: –2.52 to 0.87). In the subgroup of 8 to 12 weeks’ duration, there was a better improvement in the effect on depression in dementia (MD = –3.77, 95% CI: –6.93 to –0.60). This finding suggested that a duration of 8 weeks to 12 weeks of light therapy significantly improved depression in dementia patients.

Forest plot of subgroup analysis of light intervention weeks (≤6 w, 8 w–12 w, 16 w-6 m).
Light intervention on depression of dementia
Light interventions could be divided into stability and instability subgroups. Stability referred to fixed lighting by light boxes, while instability referred to the ceiling light intervention, natural light intervention and mixed light intervention in addition to light boxes. The result of the stability subgroup was not statistically significant with the rating dropping 3.37 points (95% CI: –9.67 to 2.93). There was no heterogeneity in the instability subgroup (I2 = 0%, p = 0.63), and the result showed an improvement on depression in dementia (MD = –2.12, 95% CI: –3.38 to –0.85) (Fig. 9).
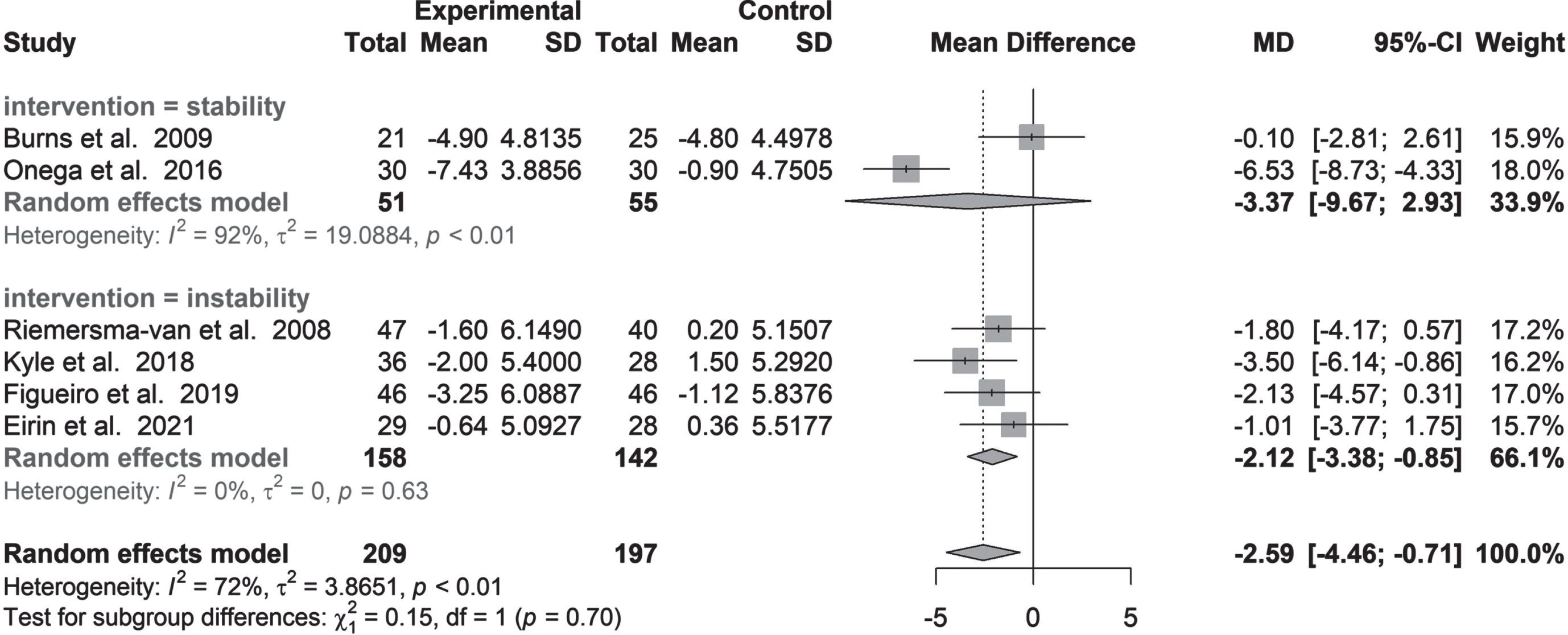
Forest plot of subgroup analysis of light intervention methods (stability, instability).
DISCUSSION
This meta-analysis study assessed the effect of light therapy on depression in dementia patients, resulting in a total of six articles. All included studies used the CSDD scale to ensure the uniformity of the measurement. According to the results of meta-analysis, light therapy had a certain improvement effect on the depression of dementia patients.
Light intensity is an important factor in light therapy. Light intensity of less than 1,000 lux showed some advantages in the alleviation of depression in dementia which matched the studies of Figuerio et al. (2019) [31] and Figuerio et al. (2014) [34]. This leads to lower treatment costs and fewer adverse effects [35]. In previous studies, an intensity of 1,000 lux or more was found to have been effective in the study by Dowling et al. (2007) (2,500 lux) [36] and Kolberg et al. (2021) (1,000 lux) [10]. The meta-analysis [17] suggested that light therapy with an intensity of 2,500 lux or more was more effective for cognitively impaired persons, including five experiments [11, 36–38], but, there was no statistical significance in the results of therapy at 1,000 lux and 10,000 lux in this study. This finding is generally consistent with those of previous studies [12, 15]. It does not mean that the illumination above 1,000 lux imparted no effect: the reason for this difference may be that the control group in these trials received light therapy with a low light intensity of 100 lux [12] to 300 lux [10, 33]. It also had a positive effect on the reduction of depressive symptoms in patients with dementia. Light intensity in the control groups attenuated the difference in change between the intervention and control groups. The study showed that the threshold for the efficacy of light therapy in depression may be lower than the current cognition, and future experimental designs should ensure a fixed the light intensity in the control group.
The outcome for the duration of intervention subgroup exerted the greatest effect on the duration of the intervention from 8 to 12 weeks. This finding is generally consistent with the previous studies of Dowling et al. (2007) (10 w) [36], Onega et al. (2016) (8 w) [11], and Konis et al. (2018) (12 w) [32]; however, the differences in those in the subgroup treated within 6 weeks were not statistically significant, which matched the studies of Hickman et al. (2007) [15] and Lyketsos et al. (1999) [14]. Hickman et al. (2007) did not support the use of ambient bright light therapy with 3 weeks as a treatment duration for depressive symptoms in persons with dementia [15]. This suggests that a certain amount of time should be allowed for light therapy to alleviate depression in dementia. In the subgroup of 16 weeks to 8 months in duration, it was not statistically significant. This phenomenon may be related to the cognitive decline of dementia patients as the duration of treatment increases, and will lead to more severe depressive symptoms as also mentioned in Sloane et al. (2015) [38]. Further studies are needed to analyze the relationship between the rate of cognitive decline and the rate of deterioration of depression.
Intervention using light therapy has always been one of the important concerns of scholars. Stability intervention with a light box is a traditional light intervention with high-intensity illumination. Its treatment time is generally between 0.5 h and 2 h. Dementia patients in real trials may have difficulty in following treatment regimens for various reasons and may even suffer more side-effects [39]. In previous studies, some experiments with the light box have shown that light therapy is effective for depression in older patients with dementia [11, 36], but others have shown the opposite results. Instability interventions have been the focus in recent years [12, 14]. Compared with the light box, the instability intervention methods were more convenient to the lifestyles and movements of dementia patients, which reduced the influences of the management of the light box and the activities of other dementia patients. Moreover, it was easier to be replaced in keeping with the interior decor of the building by installing the lamps on the ceiling and floor, which increased the possibility of use in nursing homes. In this study, the subgroup subject to the instability intervention methods benefitted more when ceiling LED installation was adopted, which coincided with the findings of other studies [9, 38], but there was no statistical significance in the subgroup that used the light box. It was interesting that Konis et al. (2018) [32] also educed positive effects by using a method involving daylight exposure. As far as it is possible to introduce more natural light to the interior, this aligns with best architectural practice in terms of light in environmental design concepts. It has a positive meaning for the promotion and application of light therapy in nursing homes. At the same time, it is also noteworthy that, although the instability intervention has many positive factors, the current research does not standardize the description of the light environment in dementia patients. Due to the characteristics of the activities of older adults, vertical illumination is more likely to reflect the luminous flux received by dementia patients than horizontal illumination. It is possible that actual retinal exposure was overestimated by horizontal illumination [15]. On the other hand, older adults with dementia may receive a different light intensity, facing different directions under vertical illumination, however, current research has not paid enough attention to this issue, and most studies do not report it. Therefore, it is necessary to report the spatial distribution of the light environment and the dwelling space of the older persons more accurately.
In terms of population and depressive detection methods, older persons with dementia are special cases: over time, it becomes harder for older people with moderate to severe dementia to complete the self-evaluation scales. The information becomes questionable when provided by the moderate to severe dementia patients, due to their disorders in attention, memory, and judgment [24]. The study of Figueiro et al. (2015) [13] used custom intervention lighting with low illumination and high color-temperature: the result showed that depression score questionnaires that were completed by the participants with Alzheimer’s disease and related dementia (the Geriatric Depression Scale-Short Form) showed a positive effect of the intervention, whereas the CSDD, which was filled out by caregivers, did not. The contradictory results were attributed to the methodological differences between self and proxy-reports [40]. In a recently meta-analysis study, Fong et al. [41] concluded that light therapy did not reduce depression. Among the six included studies [10–12, 42] in their review, the CSDD scale [10–12, 33], the Neuropsychiatric Inventory-Nursing Home (NPI-NH) [36], and the Dutch Behaviour Observation Scale for Intramural Psychogeriatrics (GIP) [42] all were included. The reason for the inconsistency between our findings and theirs might be the use of multiple depression scales in their review. Different depression scales may be one of the reasons why previous meta-analysis did not draw positive conclusions [18–20, 41], so, the scales included in the studies should be selected carefully for a meta-analysis of depression symptoms in older adults with dementia.
This research also has some limitations, for example a smaller number of articles and sample numbers were included in the study. Limited by the number of studies, only part of the effect of light intensity was analyzed without consideration of the influence of the color temperature of the light used in this study. Beyond that, the specific implementation of each study differs. As all these limitations may affect the meta-analysis, further, better designed research is required.
Conclusion
The overall results of the meta-analysis indicate that light therapy is an effective intervention for improving the depressive symptoms of older patients with dementia; 8 to 12 weeks of treatment has a more positive effect. Ceiling-mounted LED lamps have also shown promising application prospects in light therapy. With the enhanced cooperation of clinicians and architects, the effective design of light environments has positive significance for improving the quality of life of dementia patients in older care facilities where a large number of dementia patients live.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to declare.
FUNDING
This work was supported by the National Natural Science Foundation of China (No. 51878126) and the Scientific Research Foundation for Advanced Talents, Dalian University of Technology (DUT21RC (3)105).
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.