
Abstract
Background:
Several studies have examined NCAPH2 methylation in amnestic mild cognitive impairment (aMCI) and Alzheimer’s disease (AD), but little is known of NCAPH2 methylation in subjective cognitive decline (SCD).
Objective:
To examine whether methylation of peripheral NCAPH2 are differentially changed at various phases of AD, and whether it could serve as a diagnostic biomarker for SCD.
Methods:
A total of 40 AD patients, 52 aMCI patients, 148 SCD patients, and 193 cognitively normal controls (NCs) were recruited in the current case-control study. Besides, 54 cognitively normal individuals have received amyloid positron emission tomography (amyloid PET) scans. Using bisulfite pyrosequencing method, we measured blood DNA methylation in the NCAPH2 gene promoter.
Results:
The main outcomes were: 1) For SCD, there was no significant difference between SCD and NC regarding NCAPH2 methylation; 2) For aMCI, NCAPH2 methylation at CpG2 were significantly lower in aMCI compared with NC and SCD in the entire population and male subgroup; 3) For AD, NCAPH2 methylation at CpG1 were significantly lower in AD compared with NC among females; 4) A relationship with apolipoprotein E (APOE) ɛ4 status was shown. Receiver operating characteristic (ROC) analysis by combining NCAPH2 methylation, age, education, and APOE ɛ4 status could distinguish between patients with aMCI (area under the curve (AUC): 0.742) and AD (AUC: 0.873) from NCs.
Conclusion:
NCAPH2 methylation levels were altered at the aMCI and AD stage and may be convenient and cost-effective biomarkers of AD and aMCI.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common type of dementia. In 2019, Alzheimer’s Disease International (ADI) estimates that there are over 50 million people living with dementia globally, a figure set to increase to 152 million by 2050 [1]. AD is a distinct clinical-pathologic entity with a very long preclinical period before it enters the symptomatic stages [2]. According to the latest diagnostic framework of AD [2], the cognitive continuum can be artificially divided into four stages: cognitively normal, subjective cognitive decline (SCD), mild cognitive impairment (MCI), and dementia. MCI refers to an intermediate clinical state between normal aging and early dementia [3, 4]. SCD is a status in which subjects have self-perceived memory or cognitive decline compared to their previous normal state, while objective neuropsychological tests are within the normal range. It extends the continuum to an earlier stage before MCI, representing a preclinical stage of AD [5]. Currently there is no cure for AD. Although some types of treatment have been proposed, the time of intervention, due to the complexity of early diagnosis, is often late with respect to the biological onset of the disease and limits the final efficacy of the treatment. Therefore, early diagnosis of AD has been widely accepted to be of great importance. However, the diagnosis of SCD made by clinicians lacks objective examination basis, which increased diagnostic uncertainty. AD and aging can both influence self-cognition and thus reduce the reliability of SCD [6, 7]. Therefore, it is urgent to combine useful biomarkers for effective diagnosis.
The cardinal features of AD pathology are amyloid plaques and neurofibrillary tangles, which were thought to begin many years before the diagnosis of AD dementia [8, 9]. Amyloid positron emission tomography (amyloid PET) is a valid in vivo surrogate for amyloid-β (Aβ) deposits [10, 11]. Brain amyloidopathy as seen on PET can precede the onset of dementia by several years [12]. According to 2018 National Institute on Aging-Alzheimer’s Association (NIA-AA) research, cognitively unimpaired individuals with an abnormal Aβ biomarker are defined as having preclinical AD pathologic changes [2]. However, the PET examination is expensive and radioactive, which limits its clinical application.
The study of monozygotic twins suggested that epigenetics plays a role in AD etiology [13, 14]. DNA methylation is the most studied epigenetic modification and evidence has shown dysregulation of DNA methylation in AD patients [15 –19]. More specifically, West et al. firstly reported hypomethylation of the amyloid precursor protein (APP) gene in the brain of an AD patient [15]. Bollati et al. found elevated LINE-1 methylation in AD patients compared with normal controls [16]. Several studies found an increase in brain-derived neurotrophic factor methylation in AD and aMCI patients compared to normal controls [17 –19].
Previous studies have reported that the peripheral DNA methylation in the NCAPH2 /LMF2 promoter region was significantly lower in AD and aMCI patients as compared to normal controls [20, 21]. However, there have been relatively few studies examined blood NCAPH2 methylation at the SCD stage.
The present study aimed to explore blood NCAPH2 gene promoter methylation levels at different stages of AD and to explore whether NCAPH2 methylation levels have already changed at the SCD stage. We also investigated the association between DNA methylation and clinical characteristics of subjects (including age, gender, APOE status, and cognitive function). In addition, fifty-four of the cognitively normal individuals have received amyloid PET imaging test in our study and we examined NCAPH2 methylation levels between Aβ-positive and Aβ-negative cognitively normal individuals to further assess its diagnostic utility at the preclinical stage of AD.
MATERIALS AND METHODS
Subjects
The study participants were from the Sino Longitudinal Study on Cognitive Decline (SILCODE) project [22], which is the first multicenter-based SCD longitudinal observational study in China (ClinicalTrials.gov, NCT 03370744). The study was approved by the Institutional Review Board committee at Xuanwu Hospital in Capital medical university and was performed in accordance with the Declaration of Helsinki. Written consent was obtained from all participants or his/her caregiver. 433 subjects were included in the analysis, comprising 40 patients with AD dementia (15 males; age: 73.96±7.10 years), 52 patients with aMCI (30 males; age: 70.02±6.07 years), 148 patients with SCD (45 males; age: 67.10±5.02 years), and 193 cognitively normal controls (98 males; age: 67.31±5.06 years). Notably, 26 SCD participants and 28 NCs had undergone amyloid-PET (Florbetapir F-18 [AV45]) imaging, individuals were classified as amyloid positive according to an a priori established cutoff of the standardized uptake value ratio (SUVR) > 1.18 [23, 24]; the SUVR was calculated by using the whole cerebellum as the reference region, and the whole cerebral cortex as the regions of interest. Demographic data for each group of participants are shown in Table 1.
Subject Characteristics(mean(SD))
Quantitative data was analyzed by the Kruskal-Wallis H test with Dunn’s-test post hoc for multiple comparisons of independent samples. Categorical data were analyzed by the Chi-Square test or Fisher’s exact test. *p < 0.05, **p < 0.01 compared with NC, # p < 0.05, # # p < 0.01 compared with SCD, b p < 0.05, a p < 0.01 compared with aMCI.
All 433 individuals fulfilled the inclusion criteria of the SILCODE project [22]. All AD dementia patients met the published criteria and a total CDR score≥1 [25]. MCI was diagnosed using the Jak-Bondi approach [26]. The diagnoses were based on evaluations including clinical (such as inquiry and physical examination) and neuropsychological examinations (a set of detailed scales: such as Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), activities of daily living (ADL), etc.), blood tests, urine tests, and multimodal MRI as well as optional glucose metabolism PET and t-fMRI. According to MRI, cerebrovascular disease and intracranial occupancy were excluded. SCD was defined according to the criteria proposed by Jessen et al. in 2014 [27] and our previous references [22, 28], including the following: a) self-experienced persistent decline in memory rather than other domains of cognition (within the last 5 years); b) concerns about cognitive decline, and self-perceived worsened memory than the same age group; and c) performance within the norms on all standardized cognitive scales (adjusted for age, gender, and education) and failure to meet the criteria for MCI or dementia. Individuals who had no cognitive complaints and performed normally on the standardized neuropsychological tests were included as controls. The exclusion criteria included clinical stroke, severe depression, serious psychiatric disturbances, brain trauma or brain tumor, and severe somatic disease, that may account for symptoms, intellectual deficiency or other developmental disorders, and other systemic diseases. The diagnoses were confirmed by two neurologists from the Neurology Department, Xuanwu Hospital, Capital Medical University (Beijing, China). Details about participants’ evaluation can be acquired in the protocol [22].
Genomic DNA extraction and bisulfite treatment
Genomic DNA (gDNA) was extracted from leukocytes using the QIAamp DNA Mini Kit (Qiagen, Hilden, Germany). Bisulfite conversion, in which cytosine is converted to uracil and 5’-methylcytosine remains non-reactive, was performed on 500 ng of genomic DNA using the EpiTect Fast DNA Bisulfite Kit (Qiagen, Hilden, Germany) following the manufacturer’s suggested protocol. Elution was performed with 15μL EB Buffer.
Bisulfite pyrosequencing assay
For bisulfite pyrosequencing analysis, 50 ng of bisulfite-treated genomic DNA was amplified in an Opticon II system (MJ Research, MA, USA) using HS taq PCR kit (Takara, Otsu Shiga, Japan). PCR amplification primers for NCAPH2 promoter region were as follows: forward: 5’-GTATTTTTTTGGGAGGGAATAGTAAAATG-3’, reverse: 5’-CCACCTCCCAATTCTTAATAAAA-3’. The reverse primer contained biotin at the 5’position. Four CpG sites were examined using bisulfite pyrosequencing assay, and CpG positions were numbered under the sequence. The sequence and positions of the 4 CpG sites in NCAPH2 promoter region are depicted in Supplementary Figure 1. The sequencing primer: 5’-AGTAAAATGGAGTTAGAATTAGTG-3’. Cycling conditions referred to our previous study [29]. For the pyrosequencing reaction, single-stranded DNA templates were immobilized on streptavidin-coated Sepharose high-performance beads (GE Healthcare, Uppsala, Sweden) using the PSQ Vacuum Prep Tool and Vacuum Prep Worktable (Qiagen, Hilden, Germany), according to the manufacturer’s instructions, then incubated at 80°C for 2 min and allowed to anneal to 0.4 mmol/L sequencing primer at room temperature. Pyrosequencing was performed using PyroGold Reagents (Qiagen) on the Pyromark Q96 instrument (Qiagen), according to the manufacturer’s instructions.
APOE genotyping
APOE genotypes (rs429358 and rs7412) were determined by the standard Sanger sequencing method (Sangon, Shanghai, China), using the following primers: 5’-ACGCGGGCACGGCTGTCCAAGG-3’ (forward) and 5’-GGCGCTCGCGGATGGCGCTGA-3’ (reverse). The amplifications were performed in a final volume of 30μl, containing 10 pmol of forward and reverse primers and 50 ng of genomic DNA template, using PrimeSTAR HS DNA Polymerase with GC Buffer (Takara Bio). APOE was amplified using the following conditions: 1 cycle of 98°C for 10 s, 35 cycles of 72°C for 5 s, 1 cycle of 72°C for 5 min.
Statistical analysis
Data statistical distribution was evaluated for normality using the Shapiro-Wilk test. Quantitative variables were analyzed using Dunn’s-test post hoc for multiple comparisons. Chi-square tests or Fisher’s exact test were performed for categorical variables. A general linear regression model was run to perform NCAPH2 methylation comparisons among different groups. Age, gender, APOE ɛ4 genotype, education level, smoking, and diabetes were adjusted in our analysis and the Benjamini– Hochberg correction was conducted for multiple testing. The relationships of methylation levels among four CpG sites and associations between methylation levels and age, MMSE and MoCA score were analyzed using the Spearman’s rank correlation coefficients. An adjusted receiver operating characteristic (ROC) analysis was employed to evaluate the diagnostic value of NCAPH2 methylation combined with age, education, and the APOE ɛ4 status. P values were considered statistically significant at the p < 0.05 level after Benjamin-Hochberg correction.
All statistical analyses was conducted using SPSS 22.0 (SPSS, Inc., Chicago, IL, USA) and R 3.2.3 (AT&T, now Lucent Technologies, Vienna, Austria).
RESULTS
Subject characteristics
Significant differences in age (H = 38.268, p < 0.001) and education (H = 12.254, p = 0.007) were observed among the NC, SCD, aMCI, and AD groups. AD subjects were older and less educated than the NC and SCD subjects. Significant differences in the APOE ɛ4 prevalence were observed among groups (χ 2 = 20.876, p < 0.001). Patients with AD (57.50%) had more APOE ɛ4 carriers than the NC and SCD subjects (25.91 and 24.32%, respectively). Patients with AD showed lower MMSE and MoCA scores than NC, SCD and aMCI individuals (MMSE: H = 146.240, p < 0.001; MoCA: H = 149.213, p < 0.001). Significant differences in sex (χ 2 = 19.339, p < 0.001) and smoking status (χ 2 = 12.761, p = 0.005) could be found among the groups. There were more females and less smokers in the SCD group than the NC and aMCI groups (Table 1).
In 28 NCs and 26 SCD participants who had undergone amyloid-PET imaging, 21 participants in total were Aβ-positive, including 10 participants in NCs (35.7%) and 11 in SCD (42.3%) group, and 33 participants were Aβ-negative. No significant differences were found between Aβ-positive and Aβ-negative cognitively normal individuals regarding age, gender, smoking, diabetes, APOE genotype, and cognitive scores, except the education levels (Table 2).
Subject Characteristics in Cognitively Normal Individuals with Aβ-negative and Aβ-positive (mean(SD))
Quantitative data was analyzed by the Mann-Whitney U test or two independent-samples t-test. Categorical data were analyzed by the Chi-Square test or Fisher’s exact test. *p < 0.05.
Correlations between NCAPH2 methylation and the characteristics of the patients
We examined the associations between the levels of NCAPH2 methylation and the patient characteristics (age and cognitive scores) using the Spearman’s rank correlation coefficient. Age is an important factor in AD. A significant negative correlation was found between each CpG methylation level and age in SCD patients as well as between methylation levels of CpG3 and age in AD patients (Supplementary Table 1). There was a significant negative correlation between the methylation levels of CpG4 and MMSE score in aMCI patients as well as between the methylation levels of CpG4 and MoCA score in AD patients (Supplementary Table 1).
Group comparisons of the NCAPH2 Methylation levels
Part of sequence NCAPH2 promoter region from pyrosequencing and a total of four CpG sites examined in this study are shown in Supplementary Figure 1. The methylation levels of the four CpG sites were closely related to each other (Supplementary Figure 1, ρ> 0.30, p < 0.001). Thus, we conducted correlation tests for each CpG site as well as their mean values.
In multivariate analysis adjusting for age, gender, education, history of smoking, type 2 diabetes, and APOE genotype, we found significantly lower NCAPH2 methylation at the CpG2 site in patients with aMCI than the NC and SCD individuals (aMCI versus NC, p = 0.025; aMCI versus SCD, p = 0.032, Fig. 1 C).
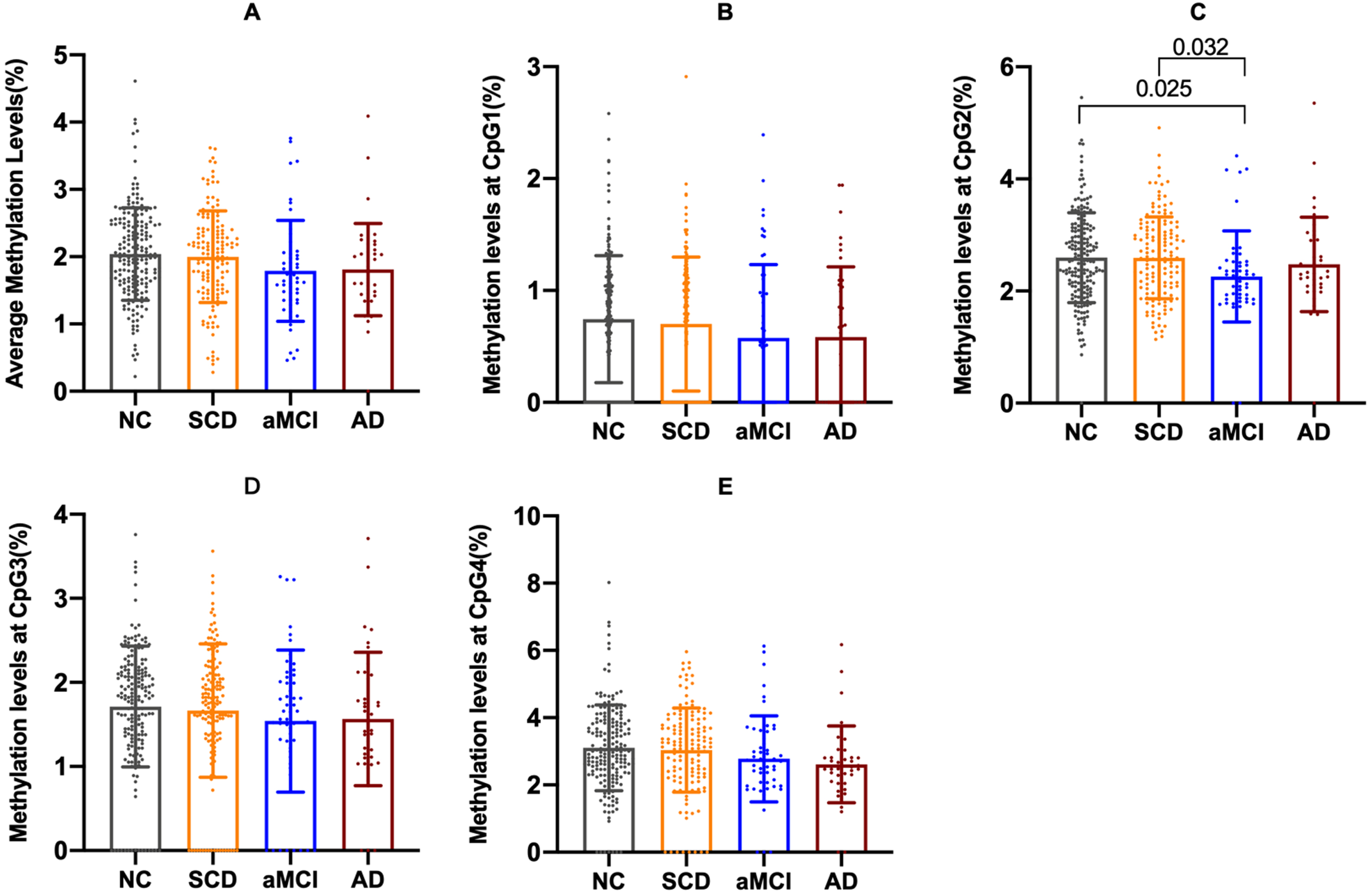
Comparison of NCAPH2 methylation levels among NC, SCD, aMCI, and AD groups in all subjects. A-E) The levels of blood NCAPH2 methylation for each CpG and average methylation among the four groups are shown in scatter plots with SD. All data were adjusted for age, gender, education level, smoking, diabetes and APOE ɛ4 genotype. (Significant p values at the p = 0.05 level after Benjamin-Hochberg correction were shown). AD, Alzheimer’s disease; aMCI, amnestic mild cognitive impairment; SCD, subjective cognitive decline; NC, normal controls.
The APOE ɛ4 variant is the strongest risk factor for AD. An association between APOE ɛ4 status (at least one ɛ4 polymorphism versus no-ɛ4 polymorphism) and the NCAPH2 DNA methylation was observed in the total population after adjusting for age, gender, education, history of smoking, type 2 diabetes, and APOE genotype. Significantly lower NCAPH2 average methylation as well as CpG3 and CpG4 methylation levels were found in the APOE ɛ4 carriers compared with non-carriers (average: p = 0.004; CpG3: p = 0.005; CpG4: p = 0.002. Figure 2A-E). Intriguingly, in the APOE ɛ4 non-carriers, a significant decrease of NCAPH2 methylation levels at the CpG2 site were observed in the aMCI group compared to NCs (p = 0.030; Supplementary Figure 2 C). However, among APOE ɛ4 carriers, no significant methylation differences in various clinical groups were observed (Supplementary Figure 2F-J).
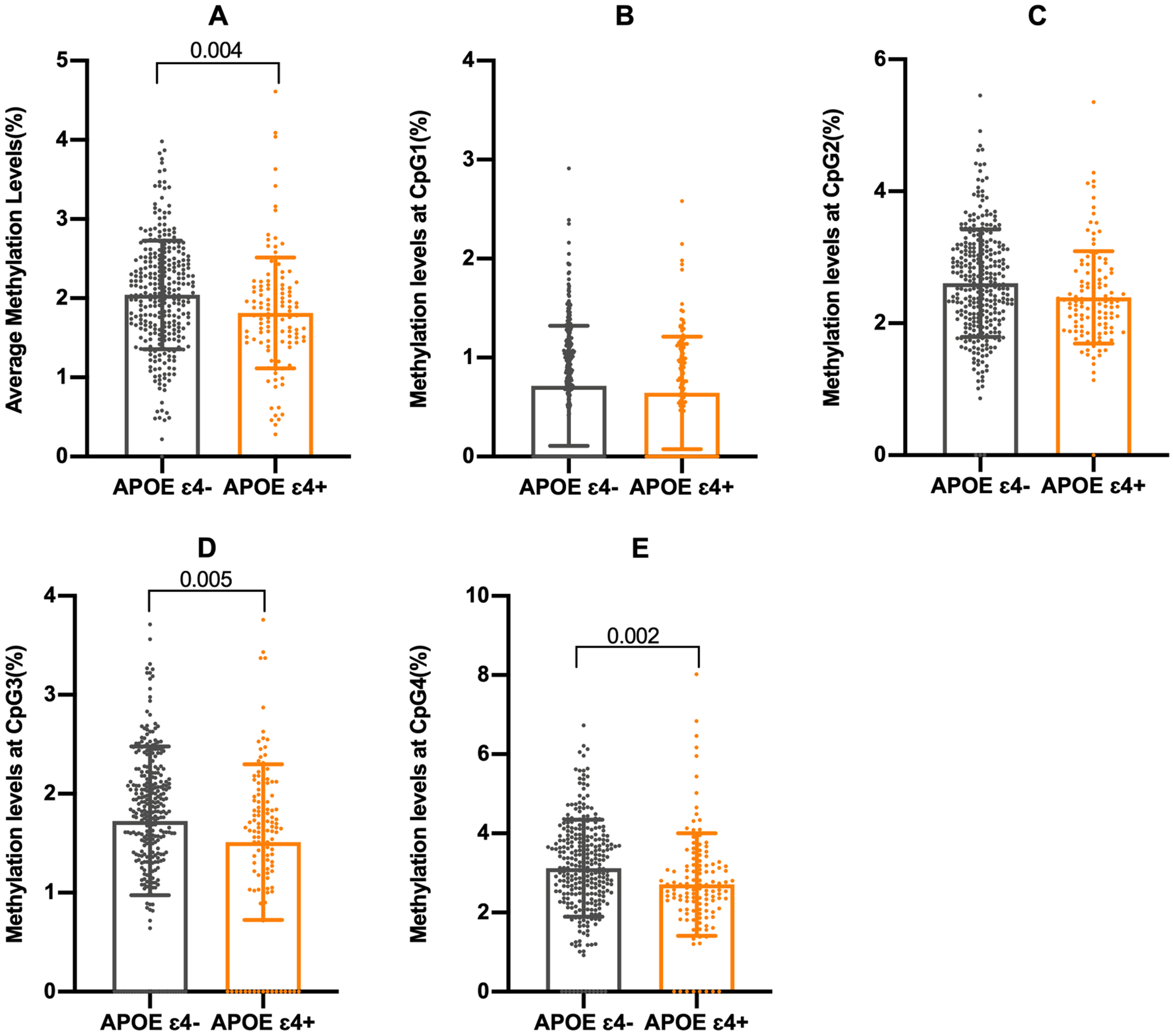
Association between NCAPH2 methylation and APOE status. A-E) Subjects (the entire population) carrying at least one ɛ4 polymorphism showed lower methylation at CpG 3, 4 and average methylation when compared to those with no-ɛ4 polymorphism. All data were adjusted for age, gender, education level, smoking, diabetes, and APOE ɛ4 genotype. The NCAPH2 methylation levels are shown in scatter plots with SD. (Significant p values at the p = 0.05 level after Benjamin-Hochberg correction were shown).
Further sex-based subgroup analysis found significant association with AD and aMCI for NCAPH2 methylation after adjusting for age, gender, education, history of smoking, type 2 diabetes, and APOE genotype. Among the females, NCAPH2 methylation levels at the CpG1 site were significantly lower in the AD group compared with the NC group (p = 0.035, Supplementary Figure 3B). Among the males, significantly lower CpG2 methylation levels were observed in patients with aMCI than the NC and SCD individuals (NC versus aMCI: p = 0.030; SCD versus aMCI: p = 0.009, Supplementary Figure 3 H). And higher NCAPH2 methylation levels at the CpG2 site were found in patients with AD than patients with aMCI (p = 0.038, Supplementary Figure 3 H). However, there was no significant differences in the NCAPH2 methylation between males and females after adjusting for confounding factors (p > 0.05).
To differentiate aMCI from NCs, receiver operating characteristic (ROC) analysis was applied (sensitivity 0.625 and specificity 0.763) for comparisons between the aMCI group and NCs, which included NCAPH2 methylation with age, education and the APOE ɛ4 status in the model. We found that the model with NCAPH2 methylation increased the prediction efficiency (model added NCAPH2 methylation: area under the curve (AUC), 0.742; 95% CI 0.664 to 0.820; p < 0.0001; model with no NCAPH2 methylation: AUC, 0.696; 95% CI 0.613 to 0.780; p < 0.0001; Fig. 3A).

Receiver operating characteristics (ROC) curve analysis by combining NCAPH2 methylation (or not) and age, education, and the APOE ɛ4 status in the model to distinguish amnestic mild cognitive impairment (aMCI) (A) or Alzheimer’s disease (AD) (B) from controls. The red line indicates the model added NCAPH2 methylation as covariate. The blue line indicates the model with no NCAPH2 methylation as covariate.
ROC analysis was also conducted (sensitivity 0.919 and specificity 0.699) for comparisons between the AD group and NCs, which included NCAPH2 methylation with age, education and the APOE ɛ4 status in the model. We found that the model with NCAPH2 methylation slightly increased the prediction efficiency (model added NCAPH2 methylation: AUC, 0.873; 95% CI 0.806 to 0.940; p < 0.0001; model with no NCAPH2 methylation: AUC, 0.847; 95% CI 0.767 to 0.928; p < 0.0001; Fig. 3B).
NCAPH2 methylation levels between Aβ-negative and Aβ-positive cognitively normal individuals
No significant difference in the NCAPH2 methylation levels between Aβ-negative and Aβ-positive cognitively normal individuals were observed (Fig. 4).

NCAPH2 methylation levels between Aβ-negative and Aβ-positive cognitively normal individuals at each CpG site. The values are shown as mean with SD. Aβ-, Aβ-negative individuals; Aβ+, Aβ-positive individuals.
DISCUSSION
In the present study, we analyzed methylation in the NCAPH2 promoter at different clinical stages of AD and found differential NCAPH2 methylation levels in AD and aMCI. And the differential NCAPH2 methylation changes were associated with age, gender, APOE ɛ4 allele and cognitive performances. An adjusted ROC by combining NCAPH2 methylation, age, education and the APOE ɛ4 status could differentiate between aMCI (AUC: 0.742) and AD groups (AUC: 0.873) from NCs. However, there was no significant difference in the NCAPH2 methylation between patients with SCD and NCs, and the non-significant result between Aβ-positive and Aβ-negative cognitively normal individuals further indicated its poor performance in the diagnosis of preclinical AD.
There are consistencies and inconsistencies compared with previous blood NCAPH2 methylation studies [20, 29]. Our results are consistent with Kobayashi N’s study showing that NCAPH2 methylation levels in peripheral blood were decreased in aMCI and AD [20]. What’s more, our present study showed NCAPH2 methylation associated with APOE genotype and were gender-specific, which weren’t found in the previous study[20]. There are several reasons to explain the conflicting results, including the different methods of methylation analysis, sample size and ethnicity difference. In Kobayashi N’s study, differences in methylation levels were compared by using analysis of covariance (ANCOVA) method, sample size was smaller and the subjects were Japanese mainly. The present study have found no SCD-related differential NCAPH2 methylation changes, which was inconsistent with our previous study [29]. However, the different sample numbers and the nonspecific diagnosis of SCD could be responsible for the divergent results.
There was a negative association between NCAPH2 methylation and MMSE for aMCI and MoCA for AD, implying cognitive impairment, which was supported by a previous study involved an association between blood DNA methylation signatures and cognitive impairment [30]. A significant negative correlation between NCAPH2 methylation with age was also found. Aging is the most well-studied risk factor for developing AD, and is closely related to differential DNA methylation patterns [31]. In various brain regions and peripheral blood cells, aging was associated with global hypomethylation and hypermethylation [32, 33].
APOE ɛ4 is the greatest genetic risk factor of sporadic AD [34]. Several pathways which might interpret the pathogenic mechanism of the APOE4 in AD have been identified, including tau dysfunction resulted from kinase and phosphatase activities modifications and regulating Aβ aggregation and impairing Aβ clearance in the brain [35]. In our study, patients with AD had more APOE ɛ4 carriers than the NC and SCD subjects. And subjects carrying at least one ɛ4 polymorphism showed lower NCAPH2 methylation levels than those with no-ɛ4 polymorphism. However, possession of the APOE ɛ4 does not ensure that an individual will develop AD, thus it is very important to identify AD risk factors in the APOE ɛ4-negative individuals. Intriguingly, in the APOE ɛ4 non-carriers, a significant decrease of NCAPH2 methylation levels at the CpG2 site were observed in the aMCI group compared to NCs. The results indicated that the combination of NCAPH2 methylation with the greatest risk allele could be very meaningful to identify the pathogenesis of AD, especially in the APOE ɛ4-negative individuals.
Gender differences are common in AD. In each age stratum, the incidence rates of AD were higher for women than for men and the age-adjusted odds ratio for women was 3.1 for AD [36]. Previous studies suggested that there were gender-based aberrant DNA methylation in mice [37] and humans [38]. In sex-based subgroup analyses, we found that NCAPH2 methylation levels at the CpG1 site were significantly lower in female AD patients than female normal controls (p = 0.035) and NCAPH2 methylation levels at the CpG2 site were significantly lower in male aMCI patients than male normal controls and SCD patients (NC versus aMCI: p = 0.030; SCD versus aMCI: p = 0.009). However, NCAPH2 methylation levels at the CpG2 site in male AD patients were higher than male aMCI patients (p = 0.038), which was consistent with the previous studies [20, 21]. It showed that NCAPH2 methylation might have gender-based differences in the association with AD and aMCI and sex difference was an important factor for AD. However, further longitudinal studies with larger sample sizes are needed to confirm our findings.
We also established a prediction model to detect AD and aMCI by combining age, education, APOE status with NCAPH2 methylation. Logistic regression is commonly used in studies of prediction models. We found that the model with NCAPH2 methylation increased the prediction efficiency to differentiate between aMCI and AD groups from NCs, thus making early diagnosis of AD possible. However, NCAPH2 gene methylation in blood might not distinguish SCD patients from controls effectively.
There is heterogeneity since the diagnosis of SCD mainly depend on patients’ self-experienced cognitive decline. Some of our enrolled SCD patients might not develop AD in the future, which might account for our non-significant results. In addition, fifty-four of the cognitively normal subjects had received amyloid PET imaging test in our study. Aβ-positive individuals determined by amyloid PET are at high risk for developing future AD, and those who are Aβ-positive can also be considered as individuals with preclinical stage of AD according to the 2018 NIA-AA research [2]. However, no significant difference in the NCAPH2 methylation levels between Aβ-negative and Aβ-positive cognitively normal individuals were observed, which further illustrated blood NCAPH2 methylation might not suitable to be used as preclinical biomarker of AD, although it might need a much larger sample size to validate.
NCAPH2 is the gene that codes for non-SMC condensing II complex subunit H2. As a subunit of condensin II, whose complexes are associated with mitosis, NCAPH2 contributes to telomere stability and prevents DNA damage signaling [39], which is essential for chromosome integrity. What’s more, condensin II is reportedly associated with neural stem cell divisions and its loss can induce DNA damage and p53 nuclear accumulation, eventually leading to apoptosis [40]. Changes in NCAPH2 expression may cause neural loss and atrophy in the hippocampus, which is one of the brain regions most commonly affected in AD [21]. Gene methylation rates are generally associated with gene expression [41]. We could expect that NCAPH2 expression changes due to decreased methylation levels would contribute to neurodegeneration in AD and aMCI.
Study strengths were as follows: we examined a relatively large number of participants with blood analysis of NCAPH2 methylation levels at different stages of AD and included cognitively normal individuals receiving amyloid PET imaging test. Further, we adjusted the models for several potential confounders. The application of pyrosequencing method, the gold standard method for DNA methylation analysis [42], is also considered a study strength.
There were also several limitations of this study. First, there were only 40 AD patients and 52 aMCI patients in the present research. The deficient number of cases may impact the credibility of the article, especially for the gender-based stratified analysis with AD. Second, whether methylation rates of NCAPH2 in peripheral blood are equivalent to those in the brain has not been thoroughly examined. Though several studies have shown that the methylation rate in blood is correlated with that in the brain [43, 44], it should be verified whether NCAPH2 is still hypomethylated in the brain. Further studies examining the various stages of AD are warranted to test whether the NCAPH2 methylation changes are concordant in the brain and blood. Third, DNA methylation from whole blood consists of a mixture of DNA methylation from various leukocyte subtypes [45]. The proportions of leukocytes could potentially affect the results. Finally, our results were based on a cross-sectional study. Further longitudinal studies with larger sample sizes are needed to confirm our findings.
In conclusion, the data has shown decreased NCAPH2 methylation levels in aMCI patients as well as female AD patients, and these alterations were associated with clinical presentation of patients. And hypomethylation in NCAPH2 promoter in blood can serve as a useful biomarker for detecting AD and aMCI. Our study may be an important step in understanding epigenetic pathogenic mechanism contributing to AD and may be crucial to identify individuals who are at high risk for developing AD.
Footnotes
ACKNOWLEDGMENTS
The authors sincerely thank all the subjects who participated in this study and the neurologists who helped us identify the study subjects.
FUNDING
This work was supported by the National Key R&D Program of China 2021YFC2501205, and the Science Innovation 2030 - Brain Science and Brain-Inspired Intelligence Technology Major Project #2021ZD0201100 Task 1 #2021ZD0201101 and #2021ZD0201800 Task 1 #2021ZD0201801.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.