
Abstract
Background:
Recent research shows that older adults electing to undergo total knee arthroplasty with general anesthesia have a pre- to postoperative acute increase in molecular free-water within their cerebral white matter. It is unknown if this change is similar for individuals who elect spinal anesthesia methods.
Objective:
To explore white matter microstructural changes in a pilot sample of older adults undergoing total knee arthroplasty and receiving general or spinal anesthesia.
Methods:
We assessed acute perioperative changes in brain white matter free-water in a limited number of older adults electing total knee arthroplasty under spinal anesthesia (n = 5) and matched groups of older adults who received general anesthesia (n = 5) or had no surgery (n = 5). Patterns of free-water changes were also compared in the larger group of older adults electing total knee arthroplasty under general anesthesia (n = 61) and older adults with chronic knee pain who received no surgical intervention (n = 65).
Results:
Our pilot results suggest older adults receiving general anesthesia had pre- to post-surgery free-water increases extensively throughout their white matter whereas those receiving spinal anesthesia appeared to have less consistent free-water increases.
Conclusions:
Our pilot results possibly suggest different patterns of perioperative brain white matter free-water changes based on anesthetic approach. We recommend future, larger studies to further examine the effects of anesthetic approach on perioperative brain free-water. The results of our study have potential implications for acute and chronic cognitive changes, perioperative complications, neurodegenerative processes including Alzheimer’s disease, and understanding neuroinflammation.
Keywords
INTRODUCTION
Diffusion magnetic resonance imaging (MRI) can be used to assess the microstructure of the human brain. Modeling of the data can separate diffusion signals into tissue (intercellular) and extracellular components and provide the metric of free-water volume fraction (FW) [1]. Extracellular FW increases can indicate glial change, including neuroinflammation [1–3]. Using preoperative and postoperative (48 h after surgery) MRI, Tanner and colleagues showed extensive and acute increases in brain white matter FW after general anesthesia and total knee arthroplasty in older adults, possibly indicating widespread neuroinflammation following surgery under general anesthesia [4]. However, neurobiological changes associated with anesthesia approach (general versus spinal) were not examined. It is not known if both anesthetic approaches result in a similar neurobiological response. Given associations between neuroinflammation and the induction of or acceleration of neurodegenerative diseases [5], the current pilot study is an attempt to begin addressing our limited scientific knowledge regarding brain responses (including possible neuroinflammation) to general versus spinal anesthesia.
This project is relevant to older adults, as currently in the United States, low- and high-risk surgical procedures are performed annually on more than half a million patients aged 65 and older [6] and at least 20–35% of older patients undergoing surgery have signs of a mild to major neurocognitive disorder [7–9]. Given the expected rate increase of neurodegenerative disorders in the populace as well as our limited understanding of general versus spinal anesthesia on brain integrity and increasing requests for elective surgeries for quality-of-life improvement (e.g., joint replacements), research examining general versus spinal anesthesia impact on neurobiological changes may be valuable. The purpose of this pilot study was to explore white matter microstructural changes, using a diffusion MRI free-water metric, in a limited sample of older adults undergoing total knee arthroplasty and receiving general or spinal anesthesia.
MATERIALS AND METHODS
This study was conducted following the principles of the Declaration of Helsinki and with the approval of the University of Florida Institutional Review Board in Gainesville, FL. This study included 131 participants, with 61 receiving general anesthesia and 5 receiving spinal anesthesia undergoing total knee arthroplasty, and 65 participants with knee pain who did not undergo total knee arthroplasty as a non-surgical (control) comparison group. The participants who received spinal anesthesia elected that approach in consultation with the medical team. All participants were appropriately informed and gave written informed consent to participate.
Neuroimaging
All MRI acquisitions were performed using a 3T Siemens Verio (Siemens Medical Solutions, Malvern, PA, USA) with an 8-channel head coil. For each participant, two MRI acquisitions were acquired: a preoperative scan performed within 1 week before surgery and a second scan performed 48 h postoperatively. Each scan session included a diffusion acquisition as part of an imaging protocol.
Diffusion-weighted images were collected using a single-shot echo-planar acquisition with two acquisitions, with no diffusion weighting six-gradient directions at b = 100 s/mm2, and 64 gradient directions at b = 1000 s/mm2. The directions were defined using an electrostatic repulsion scheme [10]. Each volume was collected using a TR/TE of 17300/81 ms, an isotropic 2-mm resolution, 73 contiguous slices, and a 256-×256-inch in-plane field of view.
Diffusion-weighted images were first preprocessed using the eddy_correct command as part of the FMRIB Software Library package to correct for eddy current distortions. Further motion correction was performed using in-house code. The b vectors were also rotated following motion and eddy correction. Diffusion-weighted images were then reviewed using a free-water diffusion tensor imaging analysis that evaluated the volume fraction of freely diffusing water, as well as the anisotropic diffusion properties of hindered water in the brain parenchyma. For this experiment, the diffusivity of free-water was set to 3×10–3 mm2/s corresponding to values of freely diffusing water at human body temperatures [1, 11]. This produces maps of fractional anisotropy and FW that can be used for subsequent analyses.
Diffusion analyses were performed using voxel-wise statistics of the diffusion data with tract-based spatial statistics as part of the FMRIB Software Library toolkit. First, each subject’s fractional anisotropy image was registered to a 1×1×1-mm3 space using the FMRIB58_FA image as a template. Next, the fractional anisotropy images were averaged across each group and used to derive a fractional anisotropy skeleton that represented the center of all white matter tracts common to each group. The analyses were then repeated for FW images using the script tbss_non_FA.
Preoperative T1-weighted images were acquired with the following parameters: TR: 2500 ms; TE: 3.77 ms; 176 sagittal 1 mm3 slices, 1 mm isotropic resolution; 256×256×176 matrix, 7/8 phase partial Fourier. Fluid-attenuated inversion recovery images were acquired with the following parameters: 176 contiguous slices, 1 mm3 voxels, TR/TE = 6000/395 ms. T1-weighted and fluid-attenuated inversion recovery images were used to calculate a general measure of “brain burden.” This variable included lateral ventricle volume in cubed millimeters, leukoaraiosis (white matter hyperintensities, which are a marker of cerebrovascular disease [12]) volume in cubed millimeters, and entorhinal cortex thickness in millimeters, with z scores calculated from the entire sample of surgical and non-surgical participants (total n = 131). This was calculated as previously reported [4] except that the composite was created with higher values indicating more “brain burden” (larger ventricles, greater leukoaraiosis volume, and thinner entorhinal cortex).
Participants
All general and non-surgery participants (full control) have been described previously [4]. The current analysis includes preliminary data assessing potential differences secondary to the surgical and anesthetic approaches. To analyze potential perioperative differences, multiple groups of participants were used: spinal anesthetic, general anesthetic, and non-surgical. We post hoc matched the five spinal anesthesia participants on an individual level with five participants who received general anesthesia and five non-surgery participants.
Matching was done on a case-by-case basis using a yoked procedure. We matched primarily based on 1) age, 2) education, 3) sex, with 4) ethnicity/race also considered. We secondarily matched on cognitive function from neuropsychological assessment (refer to Hardcastle et al. [13] for a description of the neuropsychological measures). We matched general anesthesia and control participants to their yoked spinal anesthesia counterpart to keep age within two years, education within one year, sex the same, and where possible, ethnicity/race the same. We previously showed perioperative changes in white matter FW were associated with preoperative cognition [4]. Therefore, as a secondary matching variable, participants were considered a match if the potential match had normative cognitive domain scores (declarative memory, working memory, processing speed) from neuropsychological assessment within 1 standard deviation of the yoked spinal participant. Participants were also given, but not matched using, the Montreal Cognitive Assessment [14]. To make additional inferences without sample size restrictions, the entire general (n = 61) and control (n = 65) groups were also analyzed using the approach described in the statistical analysis section.
Anesthesia protocols
Protocols were standardized, with participants receiving total knee arthroplasty with either general or spinal anesthesia.
General anesthesia. Participants received intravenous midazolam (1–4 mg) followed by continuous femoral nerve block and single-injection subgluteal sciatic nerve block. These blocks included (with 20 and 30 mL, respectively) 0.5% ropivacaine as a bolus injection, and the continuous femoral nerve block was continued with 0.2% ropivacaine at an infusion rate of 5 to 10 mL/h. No opioids were added. Propofol, fentanyl, and rocuronium were used for anesthesia induction and intubation. Patients were ventilated with an air/oxygen mixture to maintain an end tidal carbon dioxide at 35±5 mm and FiO2 between 0.5 and 0.7; anesthesia was maintained with inhaled sevoflurane and intravenous fentanyl and rocuronium. Propofol boluses were administered as clinically needed for maintenance.
Spinal anesthesia
Participants received intravenous midazolam (1–4 mg) followed by continuous femoral nerve block and single-injection subgluteal sciatic nerve block. These blocks included (with 20 and 30 mL, respectively) 0.5% ropivacaine as a bolus injection, and the continuous femoral nerve block was continued with 0.2% ropivacaine at an infusion rate of 5 to 10 mL/h. No opioids were added during block placement. Bupivacaine 0.75% (10, 12.5, or 15 mg) was given as appropriate for the body habitus or gender and age of the patient. Injection was via a 22- to 29-gauge pencil-point spinal needle as appropriate for the clinical situation. Patients were ventilated with an air/oxygen mixture to maintain an end tidal carbon dioxide at 35±5 mm and FiO2 between 0.5 and 0.7; anesthesia was maintained with inhaled sevoflurane and intravenous fentanyl and rocuronium. Propofol boluses were administered as clinically needed for maintenance of a light sedation. One participant receiving spinal anesthesia elected to be awake during the surgical procedure.
Surgical protocol
Total knee arthroplasties were performed in a standard manner for all patients and by the same surgeon (HKP). For all patients, the surgeon used a tourniquet set to 250 mmHg that was inflated prior to incision and deflated just prior to closure. Bony preparation was done by intramedullary instrumentation for the femoral side and extramedullary for the tibial side. The anterior and posterior cruciate ligaments were sacrificed for all patients and implants were fixed to the bone using bone cement. Perioperative information, including surgery events (e.g., anesthesia induction, intubation, incision, tourniquet inflation and release, etc.), anesthetic drugs, and intraoperative medications were recorded on a standardized study data collection sheet and data were confirmed with official anesthesia records.
Statistical analysis
Paired two-tailed t-tests were created using FMRIB Software Library General Linear Modelling software. In the first analysis, the pre- and postoperative FW maps were analyzed for the full general and full control (non-surgical) groups. The second analysis involved only studying the pre- and postoperative FW maps for the spinal anesthesia group as well as the matched control and general groups. This second analysis was limited due to the limited size of the spinal anesthesia group (n = 5). For this comparison, subsets of general (n = 5) and control (n = 5) participants were collected that matched the spinal anesthesia group, as described previously. A paired two-tailed tract-based spatial statistics analysis was performed using randomise within each group, comparing the pre- and post-FW maps. Because of the limited size of the groups, a leave-one-out analysis was also performed, where tract-based spatial statistics were rerun using only four of the participants from each group to reject the notion that the results were driven by outliers. This was then repeated five times corresponding to removing one of the five participants from each group.
Based on the limited sample size, we created threshold points for change using a range of t values: t = 0 and the critical one-tailed t values for a sample size of 5 (1.533, p < 0.1; 2.132, p < 0.05; 2.776, p < 0.025). We used one-tailed values because based on our previous work with the larger sample demonstrated only group-level free-water increases and no decreases in white matter following surgery [4], we expected directional (i.e., increased) free-water changes. Increased and decreased free-water voxel counts were then determined for each critical value threshold and compared. Lastly, we created a ratio of free-water increase-to-decrease for each threshold value to assess patterns of change for each group. For ease of graphing, the ratio values were then log-transformed. We also conducted a post hoc Threshold-free Cluster Enhancement (TFCE) with 5000 non-parametric permutations to check if results survived multiple comparison correction.
We used one-way analysis of variance to test between-group differences in participant descriptive and demographic variables using SPSS v. 25 (IBM, Chicago, IL).
RESULTS
There were no between groups differences for any variables, except for a trend in which the spinal anesthesia group had lower total Montreal Cognitive Assessment score relative to the control group (p = 0.063; Cohen’s d = 1.58) (Table 1).
Participant descriptive and demographic variables
Control, non-surgical group, n = 5; General, total knee arthroplasty with general anesthesia, n = 5; Spinal, total knee arthroplasty with spinal anesthesia, n = 5; MoCA, Montreal Cognitive Assessment. Declarative Memory is a composite of Hopkins Verbal Learning Test Delay Recall and Recognition Discriminability and Rey Osterrieth Complex Figure Delay Recall. Processing Speed is a composite of total Digit Symbol score, Stroop Word Reading, and Trail Making Test Part A. Working Memory is a composite of Wechsler Adult Intelligence Scale (WAIS) III Digit Backward Span, WAIS III Letter-Number Sequencing, and Spatial Span Backward Span. NHW, non-Hispanic white. Brain Burden includes lateral ventricle volume in mm3, leukoaraiosis volume in mm3, and entorhinal cortex thickness in mm with z scores calculated from the entire sample of surgical and non-surgical participants (total n = 131). This was calculated as previously reported [4] except that the composite was created with higher values indicating more “brain burden” (i.e., larger ventricles, greater leukoaraiosis volume, and thinner entorhinal cortex).
Figure 1 illustrates the tract-based spatial statistics results displayed volumetrically for the full general anesthesia (n = 61) and full control (n = 65) groups. In the brain images, blue indicates voxels where the post free-water was greater than the pre free-water, and red indicates voxels where the pre free-water was greater than the post free-water. The results indicate extensive free-water increases throughout the white matter in the general anesthesia group, particularly in the frontal lobes.
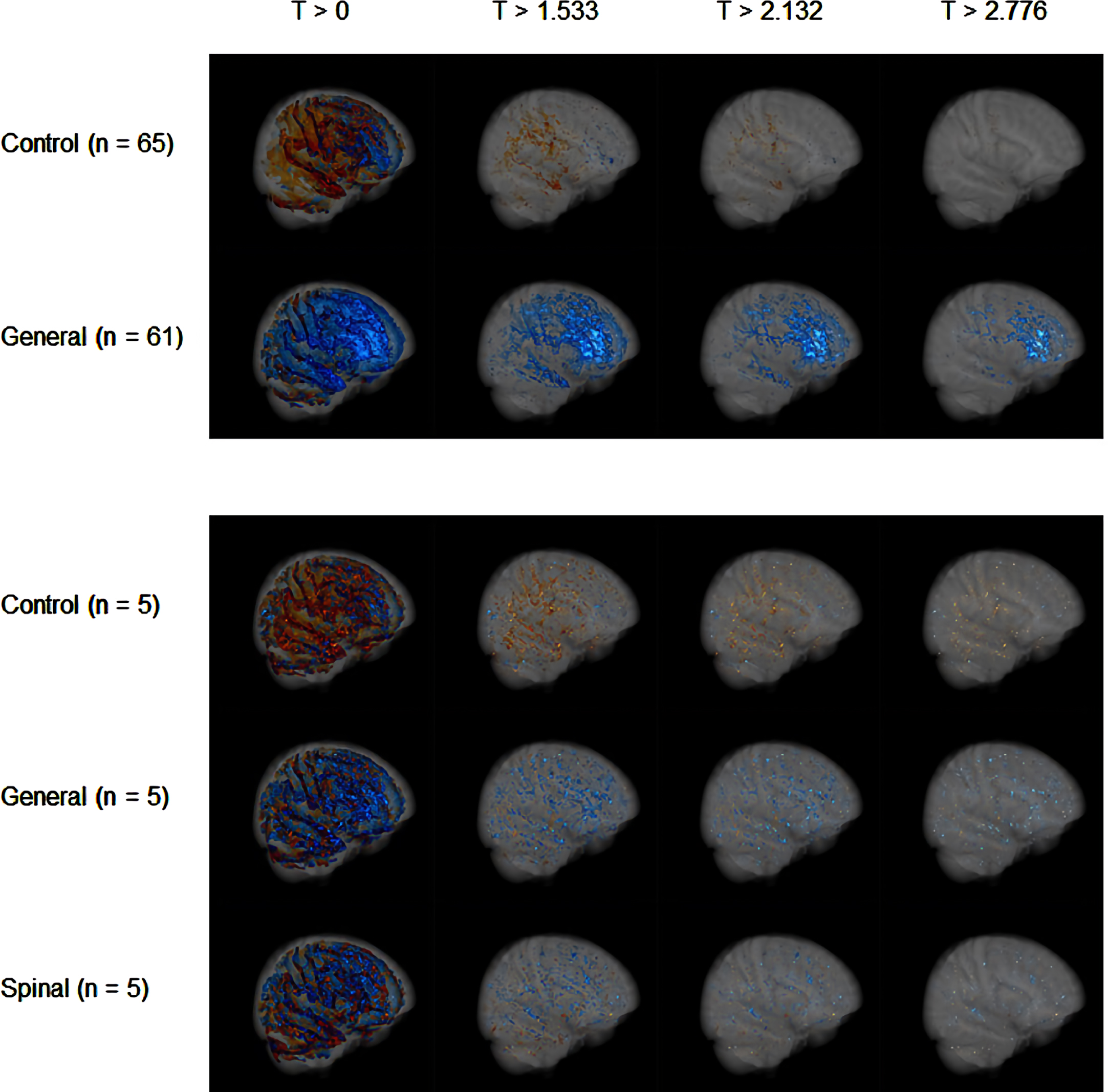
Two-tailed tract-based spatial statistics (TBSS) results illustrating differences between preoperative free-water and postoperative free-water for different t values (selected based on three one-tailed critical t values: p < 0.1, p < 0.05, p < 0.025; degrees of freedom = 4). Red indicates voxels that show larger preoperative free-water values; blue indicates voxels that show larger postoperative free-water values.
Figure 2 (a and c) shows the total number of changed voxels (Fig. 2a) and the log-transformed ratio of increased to decreased voxels (Fig. 2c) for the control group (n = 65) and the general anesthesia group (n = 61). As the t values increase, the control group maintains a voxel ratio < 1, illustrated on the plots with a log ratio < 0. However, the general anesthesia group shows an increase in this voxel ratio as the t values increase.
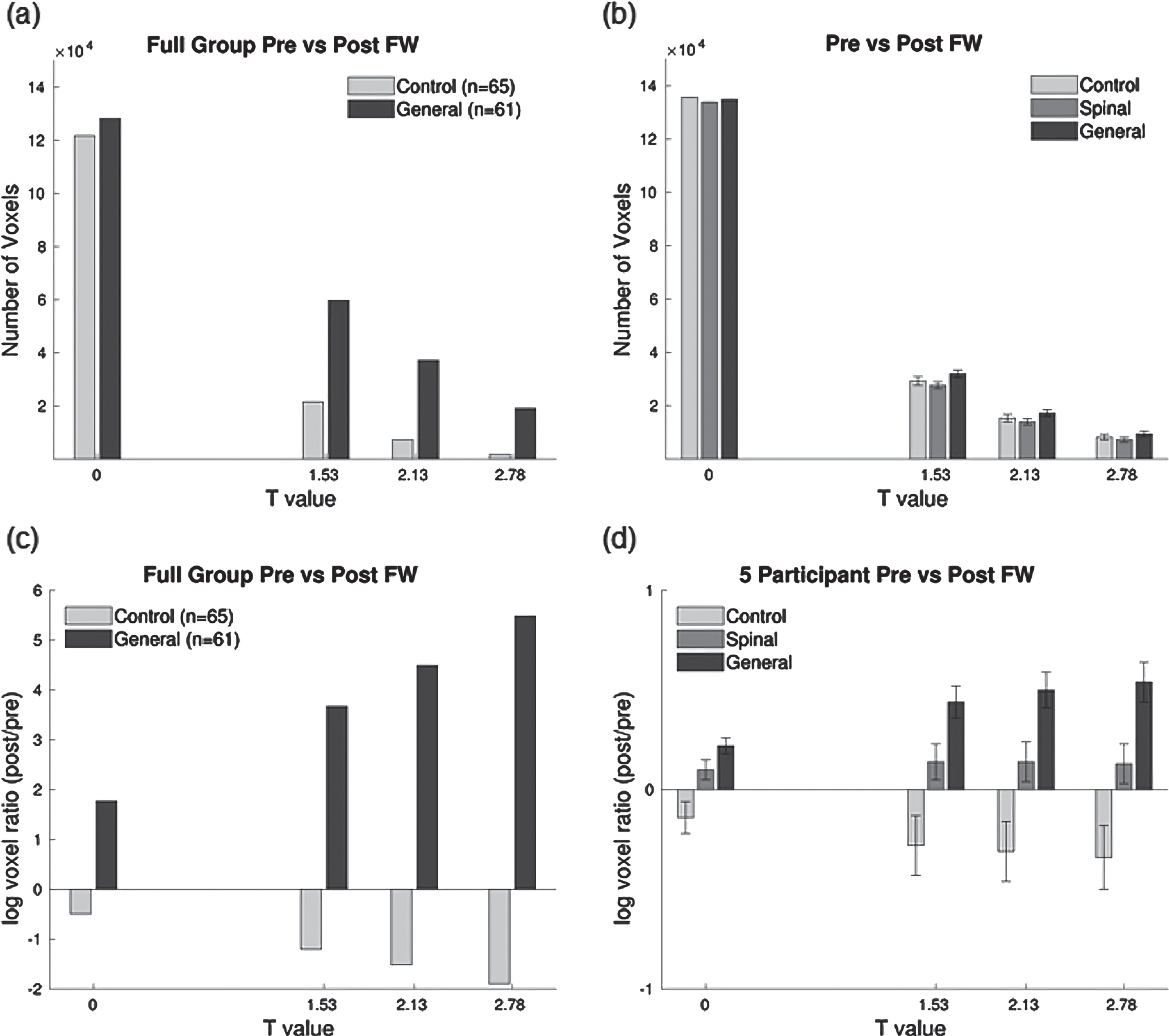
Bar plots illustrating the group dependence on the ratio of voxels that showed an increase in free-water versus voxels that showed a decrease in FW between preoperative and postoperative time points for different t values (selected based on three one-tailed critical t values: p < 0.1, p < 0.05, p < 0.025; degrees of freedom = 4). The left bar plot shows the results when performing analyses on the entire control and general groups. The right bar plot shows results when performing analyses using only five matched participants between general, spinal, and control groups. The plots in b and d quantify the mean and standard deviation of the log voxel ratios, including the leave-one-out analysis for the three groups. The number of changed voxels appears similar between groups (b) but each of the three groups has a different pattern of increase to decrease ratios (d).
The results of the tract-based spatial statistics analysis for the pre- versus post-free-water in the spinal anesthesia group (n = 5) along with the matched general anesthesia (n = 5) and control (n = 5) groups can also be seen in Figs. 1 and 2. The plots in Fig. 2 (b and d) quantify the mean and standard deviation of the log voxel ratios, including the leave-one-out analysis for the three groups. The number of changed voxels appears similar between groups (Fig. 2b) but each of the three groups has a different pattern of increase to decrease ratios (Fig. 2d). No results survived TFCE correction.
DISCUSSION
This pilot study examined acute molecular intra and extracellular FW white matter differences for older adults without dementia electing total knee arthroplasty under general or spinal anesthesia. We provide preliminary evidence suggesting different patterns of perioperative changes in white matter FW between the general and spinal anesthesia groups. The pattern of data suggests that both general and spinal anesthesia surgery participants have perioperative increases in white matter FW. Our data suggest FW changes in the spinal anesthesia group may be muted compared to that of the general anesthesia group but both groups appear to have different patterns of FW changes relative to a matched control group. This pilot study builds on our previous work [4] and raises the possibility of different acute neural responses linked to anesthetic approach for major orthopedic surgery. Identifying if differences are robust and clinically meaningful will require larger, longer-term studies.
General, spinal, and non-surgery
Given the pilot nature of the study and limited sample size, we used different statistical thresholds with tract-based spatial statistics to assess within-group patterns in FW changes in brain white matter. Across thresholds, the three groups (general anesthesia, spinal anesthesia, and non-surgery) had similar numbers of white matter voxels with perioperative differences in FW (“perioperative” includes a pseudosurgery for the non-surgery group). While this could be partially attributable to noise in the data given the limited sample size (see “Limitations and Future Directions”), the patterns of changes were different between the surgery and non-surgery groups in both the limited and full samples. With the limited samples, the non-surgery group had relatively more voxels with FW decreases than increases. In contrast, the two anesthetic approach groups had more voxels with increased than decreased FW. In addition, the general group appeared to have the largest increase to decrease ratio, with the spinal anesthesia group having a smaller increase to decrease FW voxel ratio. Given the limited sample size, interpretation of spinal and general anesthesia results is done with caution.
General and non-surgery
For the larger sample including general anesthesia and control participants, which is a replication of our previous results [4], there were apparent differences in patterns of FW change. The control group, with stricter thresholding, showed little change in FW. What changes there were indicated general decreases in FW. Previously, we showed [4] that when correcting for multiple comparisons using a threshold-free cluster enhancement no white matter voxels significantly changed in the non-surgical control group. This indicates general stability of the FW metric over a 1-to-2-week period without surgery. Any interpretation of changes in FW in the non-surgery group in the present analysis where multiple comparison correction was not performed (to match the approach for the smaller samples where multiple comparison correction would be overly stringent) should be made with caution.
In contrast, the larger general group had many areas of significantly increased white matter extracellular FW. Again, this replicated our previous work assessing perioperative FW white matter changes with the same sample [4].
The analysis method of free-water imaging separates diffusion signals into tissue and extracellular components [1]. While FW may not be specific to neuroinflammation, extracellular FW increases can indicate glial change, including neuroinflammation [1–3]. If the FW increases indicate a reactive inflammatory response, this response could be harmful, neutral, or beneficial depending on the nature and extent of the response [15]. It is possible that reactive inflammation could interact with the presurgical level of chronic inflammation by increasing the baseline level of chronic inflammation. Chronic neuroinflammation has been linked with Alzheimer’s disease, Parkinson’s disease, and multiple sclerosis (see [15, 16] for review), which are typically accompanied by brain atrophy and difficulty on immediate memory tasks.
Of particular interest in the larger general anesthesia and spinal-matching subsample is the apparent concentration of increased FW in the frontal lobes, although we note that there were FW increases throughout the brain white matter. Frontal white matter carries connections to the rest of the brain but has large pathways to subcortical and parietal regions [17, 18]. Frontal-subcortical circuitry includes connections between dorsolateral and medial frontal regions, the caudate nucleus, and the thalamus [17]. The thalamus is important for response to anesthesia as are frontoparietal regions and networks [19–22]. While we did not test whether FW changes are directly linked to the anesthetic, it is not surprising that FW increases after major surgery under anesthesia particularly affect frontal white matter.
Frontal-subcortical and frontoparietal circuits are important for attention, working and immediate memory, among other functions [23–25]. Our previous work suggested a positive association between presurgical working memory/immediate memory and acute FW increases [4]. While we did not assess relationships between preoperative brain structure or pathology and FW changes in this study, previous research gives evidence that preoperative brain integrity (e.g., less atrophy, lower amounts of markers of cerebrovascular disease) and cognition before surgery under general anesthesia are risk factors for postoperative complications [4, 26–28]. It is possible that acute FW changes in frontal regions plays a role in postoperative complications, although this remains speculative.
It remains unknown if FW increases specifically indicate neuroinflammation, chronic neuroinflammation, or acceleration of neurodegeneration. Results suggest that the choice of anesthetic approach might result in different levels of acute FW changes, but the longer-term clinical implications of this finding in cognitively well adults is unknown. FW is a metric used to examine neuroinflammation in neurodegenerative disorders (e.g., Alzheimer’s disease, Parkinson’s disease; see [29–31]), but its value in the postoperative environment as an in vivo metric is still novel. Testing these hypotheses will require, at a minimum, larger sample sizes of individuals electing major surgical intervention under general or spinal anesthetic approaches.
Limitations and future directions
Several limitations need to be highlighted. First, the spinal anesthesia sample is small. The larger study was prospectively and carefully designed to study the effects of total knee arthroplasty under general anesthesia, but five participants elected spinal anesthesia. They were followed to generate pilot data. When comparing general anesthesia, spinal anesthesia, and non-surgery groups (n = 5 for each group), all had similar numbers of voxels where FW changed significantly. Importantly, it is likely these numbers of voxels match, in part, because of higher unexplained variance (noise) due to a limited sample. For example, comparing patterns in Fig. 2 (a and b), we see with larger sample sizes the control and general groups have dissimilar numbers of voxels where FW is different from baseline. However, the preliminary data must be interpreted with significant caution, because while the numbers of changed FW voxels were similar across the three groups the patterns of increased to decreased FW voxels were visibly different. Results did not survive a more robust TFCE analysis but that was expected given limited power. A larger sample will address this limitation. If possible, a randomized study would be most effective.
Another limitation is that while free-water is sensitive to inflammation, it is not specific to it [3]. Other etiologies (e.g., edema) could be contributing factors. Addressing this limitation would require other imaging modalities (e.g., spectroscopy) to confirm neuroinflammation. Cerebrospinal fluid markers of inflammation could also be collected to confirm the interpretation of FW as a marker of neuroinflammation, although outside of spinal anesthetic approaches such collection is invasive. Additionally, we did not assess if various intraoperative factors including blood pressure variability, total anesthetic amount, and respiratory rate, or other perioperative factors like body temperature correlate with brain FW changes.
Future directions include acquiring larger samples of older adults undergoing major surgery with spinal anesthesia. We previously showed individuals with lower preoperative brain integrity had less increase in white matter free-water [4]. These same techniques may be applied to compare microstructural changes in participants receiving total knee arthroplasty under general versus spinal anesthesia. While recent research suggests no differences in the clinical outcomes of mobility and delirium in older hip surgery patients undergoing general or spinal anesthesia [32, 33], our findings suggest there might be acute differences in brain response to the procedures. Future research using larger samples will need to assess whether the apparent differences are robust and clinically meaningful. Research also is needed to examine the interaction between severity of preoperative memory impairment and type of anesthesia response on acute and longer-term brain and cognitive changes.
Footnotes
ACKNOWLEDGMENTS
We thank the participants for providing their time and efforts to the investigation. We thank the coordinators (Donna Weber) and the investigative team for their extraordinary efforts with data collection. We would like to thank Corey Astrom, ELS, Christina Hendricks, MA, and Bryan Penbrethy, MFA for their editorial expertise and assistance with this manuscript.
FUNDING
This work was supported by the National Institutes of Health grant nos. R01 NR014181 (to CCP), K07AG066813 (CCP), 9AZ19 (CCP), and UL1TR001427 (CTSI) and institutional and/or departmental sources. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Aging or the National Institutes of Health.
CONFLICT OF INTEREST
Catherine Price is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
All other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author.