
Abstract
Background:
Executive functions (EF) are central to instrumental activities of daily living (IADL). A novel approach to the assessment of the impact of EF difficulties on IADL may be through the speech acts produced when performing IADL-inspired tasks in a laboratory-apartment. Speech acts may act as a window to the difficulties encountered during task performance.
Objective:
We aim to 1) qualitatively describe the speech acts produced by participants with mild neurocognitive disorder (mild NCD) and healthy controls (HC) as they performed 4 IADL-inspired tasks in a laboratory-apartment, and to then 2) compare their use in both groups.
Methods:
The participants’ performance was videotaped, and speech acts produced were transcribed. Qualitative description of all speech acts was performed, followed by a deductive-inductive pattern coding of data. Statistical analyses were performed to further compare their use by mild NCD participants and HC.
Results:
Twenty-two participants took part in the study (n mild NCD = 11; n HC = 11). Meta-categories of data emerged from pattern coding: strategies, barriers, reactions, and consequences. Mild NCD participants used significantly more strategies and barriers than did HC. They were more defensive of their performance, and more reactive to their difficulties than HC. Mild NCD participants’ verification of having completed all tasks was less efficient than controls.
Conclusions:
An assessment of speech acts produced during the performance of IADL-inspired tasks in a laboratory-apartment may allow to detect changes in the use of language which may reflect EF difficulties linked to cognitive decline.
Keywords
INTRODUCTION
Mild neurocognitive disorder (NCD) [1]— previously referred to as mild cognitive impairment (MCI)— is often regarded as the borderland between normal cognitive aging and early pathological cognitive aging [2]. Early changes in the cognitive domain of long-term memory are well established in mild NCD, as well as in executive functions (EF) [3]. EF are high-level, top-down cognitive processes which are involved in several control processes, namely updating, shifting, and inhibition, central to goal-directed behaviors [4]. EF also play a central role in monitoring and decision-making processes [4], such as those involved in performing instrumental activities of daily living (IADL). IADL are cognitively complex activities, such as taking care of finances, using transportation [5], which rely on the mobilization of higher-order cognitive functions [6–8]. This means that they are particularly sensitive to cognitive decline [9, 10]. In fact, although IADL have long been considered to remain intact during the pre-clinical phase of NCD, people with mild NCD were shown to already have IADL deficits that caused difficulties in their daily lives [11]. Furthermore, EF decline is the cognitive function that is the most correlated to performance in daily life in normal aging, more so than a decline in memory, attention, or visuospatial skills [10]. Therefore, a rigorous and in-depth evaluation of the impact of EF on IADL in the NCD continuum is critical, both to contribute to differential diagnosis between aging and mild NCD, and to identify intervention objectives aimed at maintaining functional independence.
Independence in IADL can be measured using quick, self-report or proxy questionnaires, but several limitations of these tests have been raised in the literature, notably the tendency of older adults to overestimate their difficulties and of caregivers to underestimate them [9, 12]. Furthermore, questionnaires remain a general measure of performance that does not allow an in-depth understanding of difficulties; for example, the nature of the errors made, the strategies implemented by the person and the assistance required to progress on the task in relation to EF [12–14].
IADL are also assessed using performance-based measures within an individual’s home and community [7, 14]. Such measures of independence rely on the performance of everyday tasks (e.g., preparing a meal) in real-life conditions, thus enabling an ecological assessment that is particularly relevant to document the impact of EF on the independence of people with mild NCD [15]. A similar ecological assessment may be performed in a simulated real-life environment, such as a laboratory-apartment [16–18] or in a clinical environment [19]. Several strengths and limitations of performance-based evaluations have been discussed in the literature [14]. The most important strengths identified are the possibility of observing the person in an environment as close as possible to real life as well as ensuring the use of unstructured approach which is more suitable for highlighting the impact of EF on IADL [8, 20]. An unstructured approach is the most suited evaluation context to evaluate all cognitive operations that are involved in goal-directed behaviors and intimately tied to EF [8, 20], i.e., 1) formulating a goal (e.g., shop for groceries needed to prepare a meal for guests), 2) coming up with an action plan to meet these goals (e.g., compile a shopping list of all items needed before heading to the grocery store), then 3) executing said action plan and finally, 4) verifying having met the goal initially set (e.g., all necessary items were purchased at the grocery store) [7, 20]. Moreover, unstructured approaches are critical to simulate IADL performance that would resemble that of real life. In experimental settings, for example, this might be reflected in the examiner being as uninvolved as possible. As such, the examiner’s minimal involvement contributes to a more ecological assessment of IADL performance since, in the real-world, there is no examiner to guide the individual towards the daily tasks to be performed.
Despite their relevance, several limitations of performance-based tests have been identified, such as the length of evaluation (e.g., 3 h) and required formal training [9, 14]. Most IADL performance tests also are not unstructured and are more oriented towards evaluating execution only [14], therefore limiting their ability to document the impact of EF on IADL specifically.
Another way of approaching the evaluation of the impact of EF difficulties on IADL could be to use the spontaneous verbalizations that older adults make when engaged in a complex task, in response to certain difficulties or obstacles encountered; in other words, when EF are particularly challenged. These verbalizations could provide a new perspective on the issue, approaching the topic from the point of view of the older adults with or without cognitive deficits as they engage in complex tasks. Indeed, spontaneous verbalizations during the task could become a window to the difficulties encountered or the strategies implemented by the person, both being influenced by EF, and expressed through speech acts. A speech act is something expressed by an individual that not only provides information, but also performs an action [21]. Speech acts are utterances which may serve various functions when communicated, such as ordering, answering or requesting amongst others [22].
To our knowledge, there are no existing studies on the topic and therefore, qualitative description may represent the method of choice for a first exploration of the question. Qualitative description involves a comprehensive summary of events as they occur in their natural state as well as low-inference interpretation of data, all to reflect the meaning of these events to individuals [23, 24]. In choosing this method, we aimed for our analysis to describe the speech acts produced by participants in response to complex tasks performed within an assessment of IADL.
A better understanding of the difficulties expressed (or not) and the efforts made to circumvent them (or not) in healthy older adults and in those with NCD would make it possible to: 1) document tangible manifestations of IADL difficulties; 2) see if they can be linked to EF, and in particular to the operations involved in goal-directed behaviors; 3) compare populations along the NCD continuum to identify potential key differences.
Therefore, the main objective of the study was to explore if the use of speech acts could help in better understanding how EF deficits impact IADL in normal aging and NCD. More specifically, we aimed to: 1) describe speech acts produced by participants with mild NCD and healthy controls (HC) as they performed IADL tasks in an unfamiliar ecological setting where EF are particularly involved; 2) compare these speech acts between mild NCD participants and HC.
MATERIALS AND METHODS
Design
Qualitative description was performed to describe all speech acts produced by older adults with mild NCD and HC, and descriptive statistical analyses were performed to further describe the speech acts produced in each group.
Qualitative description
When the aim of research is to gain an in-depth understanding of the meaning of a phenomenon or events from the perspective of the people at the center of that phenomenon or those events, qualitative description proves to be an ideal method of analysis [24]. Indeed, qualitative description involves a comprehensive summary of events as they occur in their natural state (as far as possible, in an experimental context), using everyday language to describe these events and making a low-inference interpretation of the data, all in order to reflect the meaning of these events for people [23, 24]. As such, a qualitative description [25] of all speech acts produced by both mild NCD participants and HC was performed as they executed four scripted IADL tasks in the laboratory-apartment.
We opted for a deductive-inductive approach as it was methodologically optimal for three reasons. Since our study design was not based on a preexisting model, the inductive aspect (1) allowed for the “data to speak”, for speech acts to be coded with minimal interpretative bias on our part and, (2) in line with the iterative nature of coding and analysis of qualitative data, for the incorporation of newly emerging speech acts throughout the process; the deductive aspect (3) allowed us to integrate a basic structure adapted from two operations of goal-directed behaviors [8] to organize data coding, again with limited bias to the speech acts coded. For the aims of this paper, we focused exclusively on the operations carrying on task (which we named “task execution”) and verifying attainment of goal (which we named “verifying completion of all tasks”), as defined in the IADL Profile [8].
Participants
The present study was part of a larger research project, which was approved by the aging and neuroimaging research ethics committee of the Centre intégré universitaire de santé et de services sociaux du Centre-Sud-de-l’Île-de-Montréal. In compliance with guidelines on human experimentation, consent forms were signed by each participant, in which they agreed to be recorded while they performed tasks in the laboratory-apartment.
In the larger project, HC were recruited through a convenience sample, mainly from research pools of volunteers in Montreal (Quebec, Canada) [15]. Participants with mild NCD (clinical diagnosis established according to consensus criteria by Petersen [26], Winblad et al. [27]) were also recruited through a convenience sample, via memory clinics of the Institut universitaire de gériatrie de Montréal (IUGM) [15]. Some participants were also recruited through lists of participants from previous research projects or from the community. Inclusion and exclusion criteria are detailed in Table 1.
Inclusion and exclusion criteria for the HC and mild NCD participants under study
A comprehensive evaluation of participants prior to the experimentation was conducted in order to assess their cognitive status and gather data on their performance on various cognitive domains linked to functional difficulties in IADL, namely memory and executive functions [28, 29]. To prevent multiple testing problems and minimize task impurity associated with testing of executive functions [30], composite scores based on z-scores of performance on executive and memory assessments were calculated [15]. The executive function composite score was obtained by adding 1) the ratio between the time required to complete the switching condition (trail B) and the baseline condition (trail A) in the Trail Making Test (TMT) [31], 2) the ratio between time required to complete the color naming in the discordant condition (3rd condition) and the concordant condition (2nd condition) in the DKEFS Color Stroop Test [32], 3) the total score of the DKEFS Towers [32], and 4) the visuo-executive sub-score of the Montreal Cognitive Assessment (MoCA) [33]. The memory composite score was obtained by adding 1) the total number of words recalled over the five trial of the Rey Auditory Verbal Learning Test (RAVLT) (maximum of 75) [34] and 2) the recall sub-score of the MoCA [33].
Procedure
The larger project
The aim of the larger project was to assess an alternative and innovative approach to functional assessments in predicting mild NCD [15], by using sensor technology in a laboratory-apartment. To do so, participants performed 5 IADL in a one-bedroom, laboratory-apartment situated in a university department. Their functional performance was evaluated with sensor-based observations (motion, contact, and electric sensors around the laboratory-apartment) and performance-based measures (rated with videotapes). Participants’ performance of these tasks was videotaped by an examiner (E) present in the laboratory-apartment throughout the experiment. As is the case in unstructured assessments of IADL performance, unless a participant was putting their safety at risk or if the E felt that the participant was completely blocked, as to compromise the execution of a task, interventions were kept to a minimum. An instruction sheet containing five tasks was given to the participants before entering the apartment and they were free to keep and consult this sheet as they wished, throughout the course of the experiment. A participant engaging the E was reminded to “refer their instruction sheet” and encouraged to “do as if they were home alone”. While participants were free to execute tasks in the order they wished during the assessment, the goal was to complete all five tasks within 45 minutes, a time constraint inspired by the Six Elements Test [35] and added to force participants to be well organized in their task performance order.
Tasks were based on laboratory validated tasks used in previous projects [36], except for the task of obtaining information on bus departures that was based on the IADL Profile [7, 37]. The five tasks were the following: Place your belongings (bag and coat) in the closet. Prepare a light meal, including: a) an egg, two toasts with jam for one person, b) a hot beverage, a cup of coffee with milk and sugar, c) set the table for one person, d) do not eat the meal prepared, clean up and put away the material after the meal. Clean the bathroom, including: a) flush the toilet, b) wash the mirror and sink with a cleaning product. Call to inquire about bus departures from Montreal to Toronto on that day, then give the information to the E. Answer the phone that will ring during the experiment and perform the task indicated by the interlocutor (fold and store three pieces of clothing placed on the bed, in the bedroom, in the chest of drawers next to the bed, top drawer in the middle).
The present study
The data source for the present study consisted of the video recorded performances of participants in the larger project, i.e., in the laboratory-apartment (between 45–90 min), as they performed 4 of the 5 IADL described above. Data for task 4 (obtaining information) is not included in the present study as it entailed very specific verbal exchanges with the E (e.g., varying levels of assistance required of the E and varying participants’ reactions to said assistance) which differed greatly from the other 4 tasks.
Considering our focus on the speech acts produced during said performances, the first author (R.-P.F.) proceeded to the verbatim transcription of the video data, using an approach to reflect all spoken utterances of the participants including, for example, filler speech. Since the other two authors (N.B. and S.M.B) did not watch the videos, the verbatims explicitly detailed participants’ speech acts along with detailed information about their prosody, tone, emotional reactions, facial expressions, pointing behaviors, reading behaviors, looks given to the examiner, movements around the apartment, changes in the experimental settings and explanations for pauses to facilitate coding validation and provide added context for analyses.
Qualitative data analysis
The coding procedure implemented was that of Miles and collaborators [25]. Speech acts used by only one participant were not included as we deemed these reflected that one participant’s verbal idiosyncrasies more than their cognitive status (whether it be HC or mild NCD) and, as such, should not be used to extrapolate to the group as a whole (control or patient, respectively).
Descriptive coding
The first cycle consists in attributing a strictly descriptive label to data “chunks” [25], which could be described more specifically, in regard to our research objectives, as units of information extracted from participants’ verbatims. The first component in our descriptive labels reflected whether the speech acts were used during task execution or during verification of goal attainment (deductive approach to coding). To do so, coding rules were put in place, based on the IADL Profile [8]. As such, a speech act was deemed to be part of the task execution stage when it was used by a participant who had entered the laboratory-apartment and was in motion, whereas a speech act was deemed to be part of the verification of goal-attainment stage if the participant had first verbalized having completed all tasks on their instruction sheet. The second and main component of our descriptive labels was the actual use of speech acts by participants. In the verbatim extract below, a participant is putting away materials after preparing their meal. They decide to explore the cabinets, and upon finding a muffin pan, they tell the E that they could make muffins.
P2: (Participant is putting away material after having completed the meal preparation task; he decides to inspect the freezer as he puts away the material he has cleaned; no material was retrieved from freezer for task execution). What’s in there? Empty (laughs, then continues looking through cabinets; upon seeing a muffin pan, he says).
This specific speech act would first be described as part of task execution (the participant is finishing the meal preparation task) and would then be described as a statement (versus a question) addressed to the E (versus speaking to themselves), about the presence of material unrelated to the task at hand (the meal preparation did not require making muffins). Such coding lasted until data saturation was reached, meaning until all speech acts had been given descriptive labels [25]. For this study, the first author (R.-P.F.) was the coder, and the second and third authors (N.B. and S.M.B.) both validated coding independently. If a disagreement occurred between two authors, the other author would weigh in and resolve it. The coder and the validators all remained blind to participants’ cognitive status (mild NCD or HC) throughout the entire first cycle of coding, to ensure impartial and unbiased coding and validation, respectively. A rigorous coding guideline was developed by creating a comprehensive list of codes with their detailed definition. This first list encompassed all speech acts produced by all participants during their performance in the laboratory-apartment.
Pattern coding
All subsequent cycles of coding are referred to as pattern coding. Pattern coding is an inferential process which condenses large amounts of codes into a smaller number of more meaningful analytic units (categories) to help the researchers focus their analysis [25]. This entails that patterns emerge from the first cycle of coding or, in other words, that categories can now be built to regroup and organize multiple codes with similar thematic content [25]. As we move on from descriptive coding to pattern coding, data analysis is performed with a deeper focus on meaning or purpose, rather than simply describing the speech acts used by participants. To facilitate subsequent advanced cycles of pattern coding— which focused on analyzing the types of speech acts that were used by mild NCD participants versus HC— the main coder (R.-P. F) was made aware of participants’ cognitive status while both independent coding validators (N.B. and S.M.B.) remained blind. From there, the initial list of codes encompassing all speech acts used by participants, regardless of their cognitive status, was split into two new lists. The first one comprised all mild NCD data extracted from the initial list (i.e., speech acts used by mild NCD participants), while the second one comprised all HC data extracted from the initial list (i.e., speech acts used by HC). Each new list was then analyzed individually until data saturation was reached in both, the codes’ definitions, which were initially written to describe data for all participants, were thoroughly reworked. Data saturation was attained when we reached a total of 11 participants in each group.
Subsequent pattern coding cycles aimed at transforming categories of speech acts into meta-categories, allowing data to be condensed into a matrix for the stage of task execution and an event-state network for the stage of verification of completion of all tasks [25]. The meta-categories were given a “functional label”: meta-categories of speech acts which reflected participants inching closer to goal attainment (e.g., by asking a question which helped them understand what to do next) were labelled as
Quantitative descriptive analyses
Once pattern coding of qualitative data was completed, mean frequencies were calculated for each meta-category of speech acts produced by mild NCD participants and HC. Moreover, T-tests were performed (data were following a normal distribution) to compare groups and therefore further describe each group’s production of strategies and barriers during task performance.
RESULTS
Participants’ characteristics
The study sample included 11 participants with mild NCD and 11 HC. Participants’ demographic and cognitive measures are presented in Table 2. There was a larger proportion of men in the mild NCD group, χ2(1) = 4.55 p < 0.01. Total years of education and age of participants in both groups were comparable. The mild NCD group presented more symptoms of depression [38] than the HC group U = 21.50, p < 0.01*. The mild NCD group’s performance on the MoCA [33] was significantly lower than that of the HC, T(1, 20) = 3.09, p < 0.01, as were their composite executive (T(1, 12.6) = 7.40, p < 0.01) and memory (T(1, 14.5) = 9.82, p < 0.01) scores. Composite scores were based on z-scores of performances on executive and memory assessments included in the cognitive assessment battery.
Mild NCD participants and healthy controls’ demographics and cognitive measures
±Chi-Square; +Independent Samples t Test; *Mann-Whitney U test; n.s., significance level below 0.05; NCD, neurocognitive disorder.
Objective 1: Describe speech acts produced by mild NCD and HC participants
During task execution
The task execution stage consisted of all speech acts used by mild NCD participants (n = 11) and HC (n = 11) during the execution of the tasks described on the instruction sheet. We considered participants to be in the task execution stage once they entered the laboratory-apartment and got in motion.
Strategies: The main types of strategies used by mild NCD participants and HC during task execution were (1) confirming their understanding of instructions, (2) actively validating their understanding of instructions, (3) organizing tasks and (4) validating their performance (Table 3).
Mean frequencies of mild NCD participants and healthy controls’ categories of speech acts used during task execution
n.s., significance level≤0.05; NCD, neurocognitive disorder.
Confirming their understanding of instructions was a more passive strategy used by participants which could be as simple as answering “OK” upon the E giving detailing the interferent task to be completed (P41, Table 4) or upon the E asking the participant to do what they thought they should do, when they questioned the instructions (P31, Table 4).
Table showing examples of meta-categories of speech acts used as strategies by mild NCD participants and HC during task execution
Actively validating their understanding of instruction was a more active strategy used by participants to validate that they understood what was expected of them, such as P6 (Table 4) validating the small mirror leaned up against the sink was indeed the one to be cleaned as part of the bathroom cleaning task. Similarly, P37 (Table 4) validated if they were allowed to use the material on the kitchen island, although a portion of it was covered by sheets (to protect sensors below).
Organizing tasks was by far the most prominent, complex and task-centered strategy used by participants of both groups. It encompassed all the speech acts which helped participants’ spatiotemporal organization of their actions in order to execute tasks as expected. For example, P22 (Table 4) was first searching for the bathroom, in order to begin cleaning it and, upon finding the bathroom, they were now ready to begin washing the mirror. Similarly, P31 (Table 4) is narrating their actions as they pause the preparation of their egg, in order to go to the bedroom to start the interferent task. Upon its completion and their return to the kitchen area, they can be heard saying they must now restart their egg.
Validating their performance was a strategy observed in participants when they needed encouragement or, on the contrary, when they felt they were doing a good job. Some participants validated their performance defensively, such as in the case of P10 who validated their performance by critiquing that of a previous participant who had left a pan poorly washed (Table 4). On the other hand, after staining a tablecloth, P11 validated with the E that this would not affect their performance, jokingly asking if they’d “lose points” and if the E would still “hire them” (Table 4).
Barriers: The main types of barriers used by mild NCD participants and HC during task execution were (1) not taking instructions into account, and (2) being distracted from the task at hand (Table 3).
Not taking instructions into account was observed when participants chose not to listen to instructions provided by the E or not to accept the assistance provided by the E, or when they failed to follow their instruction sheet in order to complete a task as expected. In Table 5, P2 is shown not listening to the E who attempted many times to redirect them to their instruction sheet, while P21 is shown not cleaning the bathroom because they deemed it clean enough as it was, although it was listed on their instruction sheet.
Table showing examples of meta-categories of speech acts used as barriers by mild NCD participants and HC during task execution
Being distracted from the task at hand was observed when participants made comments, joked or asked questions which prevented them for pursuing task execution. Some distractions were task-centered (e.g., giving an opinion about the material they are used to execute the task) while others were unrelated to the task they were executing (e.g., noises heard outside the laboratory-apartment). In Table 5, P2 is shown to be distracted by the contents of the freezer and a muffin pan they stumbled upon after finishing the meal preparation task. P34 is seen taking a short break from drying the dishes with a cloth to share their opinion of the advantages of a dish rack with the E (Table 5).
Reactions: The main types of reactions of mild NCD participants and HC during task execution were (1) justifying their performance and (2) reacting emotionally (Table 3).
Justifying their performance was a reaction observed in participants when faced with task demands or difficulties while executing a task. Most often, participants justified their performance by comparing task demands with their habits at home, such as when P2 justified not using the cleaning product at hand to clean the bathroom sink (instead opting for glass cleaner) as they usually used water and vinegar at home (Table 6). In other cases, participants justified their performance when they expected difficulties to arise from their lack of experience with the material at their disposal in the laboratory-apartment. Indeed, P11 feared they would have a hard time making coffee with the coffee maker as they only drink espresso (Table 6).
Table showing examples of meta-categories of “reaction” speech acts used by mild NCD participants and HC during task execution
Lastly, swearing was an emotional reaction observed in participants most often when faced with task demands or difficulties while executing a task or, in rare cases, when they were surprised by the outcomes of their actions. For example, P6 was growing increasingly impatient as they attempted to locate the coffee in the kitchen, going as far as implying it had been hidden on purpose and hinting that they would soon quit if they did not find it (Table 6). P31, on the other hand, is laughing and swearing because they decided to remove their egg from the stovetop and it was very runny in their plate.
During goal attainment verification
We considered a participant to be in the verification stage following a clear verbalization reflecting an actual verification of having completed all tasks (e.g., by reading aloud the instruction sheet, using it as a checklist of sorts). As such, simply verbalizing being done was not considered a verification behavior, nor was simply answering “yes” if asked by the examiner if done.
Consequences: Apart from correctly verifying having completed all tasks, which was observed in few mild NCD participants, and most of the HC, all other speech acts observed during the verification of goal attainment are contrastive in that none were observed in the HC group. They will be discussed below.
Objective 2: Compare speech acts produced by mild NCD participants and HC
During task execution
Strategies: While most HC and all mild NCD participants
Qualitatively speaking, while both mild NCD and HC groups
Barriers: Overall, mild NCD participants used significantly more barriers than HC during task execution. Mild NCD participants
Reactions: The mild NCD group as a whole was shown to be much more reactive to their difficulties. Overall, they
Both mild NCD participants and HC showed
Our results also highlighted a
The three most reactive mild NCD participants, including the one presented in the example above, were responsible for 89% of all avoidant emotional speech acts produced and 80% of all emotional speech acts overall (Supplementary Table 3).
During goal attainment verification
Consequences: Few HC felt the need
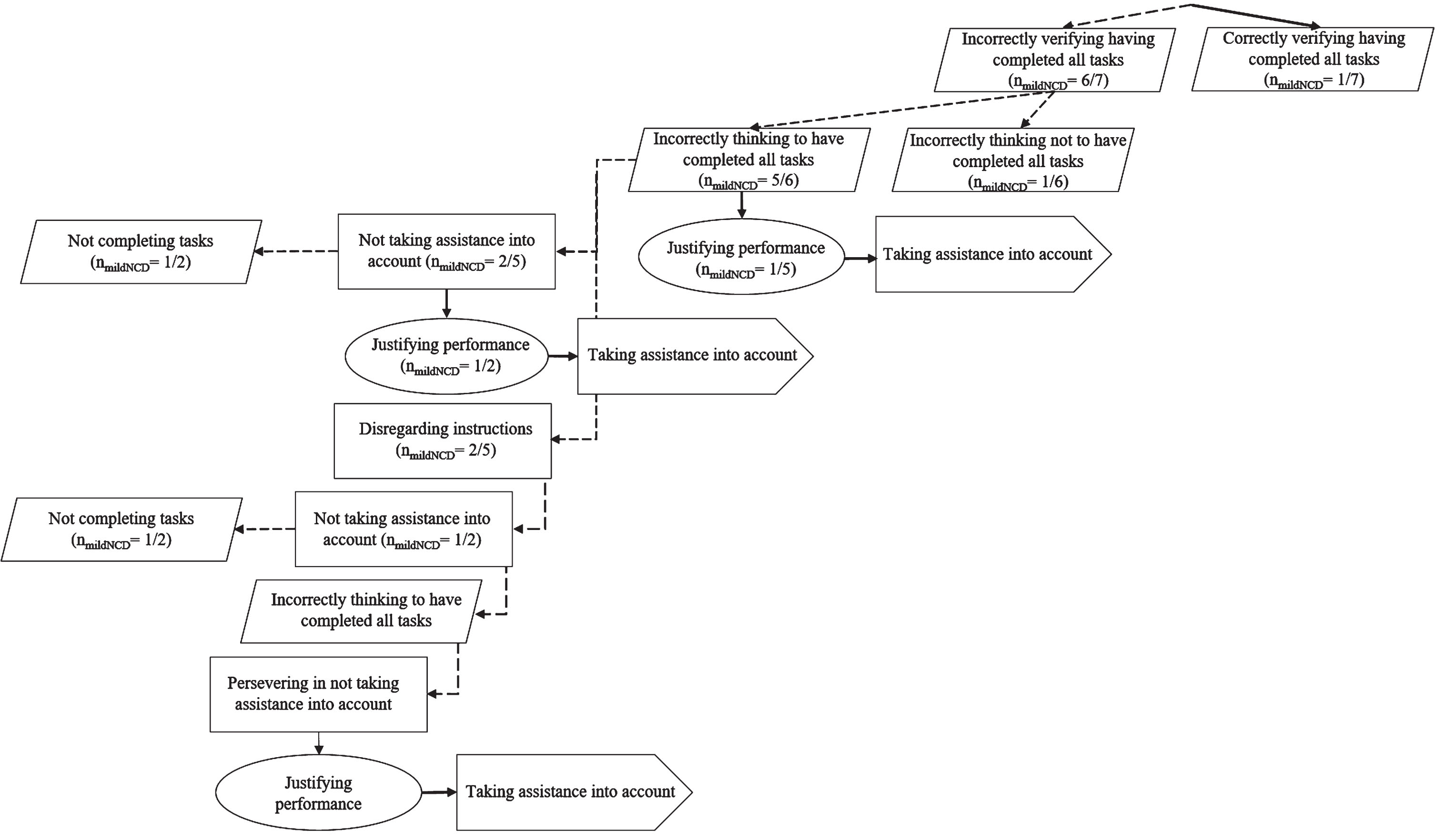
Use of strategies and barriers during verification of completion of all tasks and its impact on goal attainment.
DISCUSSION
The main objective of the study was to explore if the use of speech acts could help in better understanding how EF deficits impact IADL in normal aging and NCD. More specifically, the specific objectives of the study were to: 1) describe speech acts produced by participants with mild NCD and HC as they performed IADL tasks in an unfamiliar ecological setting where EF are particularly involved; 2) compare these speech acts between mild NCD participants and HC. Our results suggest that the use of speech acts is a potentially relevant mean to understand, from the older adults’ perspective, how they approach IADL tasks in an unfamiliar context, what strategies they used, what barriers they set up, their reactions to difficulties, as well as the consequences of their choices of actions. We have documented these elements in the context of two goal-oriented operations supporting IADL and dependent on EF (execution and verification) as the tasks were realized in a new, unfamiliar setting.
More specifically, with regard to objective 1, our results showed that during task execution mild NCD participants and HC used four types of strategies that brought them closer to goal attainment: (1) confirming their understanding of instructions, (2) actively validating their understanding of instructions (3) organizing tasks, and (4) validating their performance. Both groups also used two types of barriers which delayed goal attainment: (1) not taking instructions into account, and (2) being distracted from the task at hand. Moreover, both the mild NCD group and the control group reacted to task demands and difficulties by: (1) justifying their performance and (2) reacting emotionally. During the verification of goal attainment, most HC who verified having completed all tasks were correct in their assessment, and produced no further speech acts. On the other hand, most mild NCD who verified having completed all tasks were incorrect in their assessment, which led to loops of barriers, reactions and consequences and thus delayed goal attainment.
With regards to objective 2, our results showed that mild NCD participants used significantly more speech acts during task execution than HC did, as well as more strategies to ensure goal attainment. Indeed, they organized task execution significantly more. Yet, mild NCD participants also used significantly more barriers that delayed goal attainment.
In addition to providing an in-depth description of speech acts produced by participants while performing IADL, the results of our study can be related to EF and their impairments in an NCD context. Mild NCD participants’ overall greater use of speech acts during task execution might reflect inhibition deficits, as one of the main guidelines given to participants when performing tasks in the laboratory-apartment was to “refer to their instruction sheets” if questions arose. Inhibition, also known as inhibitory control, encompasses both self-control (behavioral inhibition) and interference control (cognitive inhibition and selective attention) [39]. It consists of the ability to control one’s attention and thoughts, to choose how to behave and react in order to do what is more appropriate or necessary to achieve a goal, while discarding what could potentially take us away from it [39]. Using significantly more speech acts during IADL task execution might as such reflect difficulties in self-control.
Our results also suggest that mild NCD participants used significantly more barriers that hindered or delayed goal attainment, which may reflect difficulties in interference control. Mild NCD participants were more distracted, and their distractions were not as task-centered as those of the HC group. Indeed, mild NCD participants being distracted by irrelevant stimuli (e.g., discussing material unrelated to the task at hand, or noises heard outside of the laboratory-apartment) is consistent with inhibition difficulties found in the literature on the mild NCD population [40]. Such distractions were not observed in the HC group. Interference control is what makes it possible to select both the stimuli in our environment that we need to pay attention to and those that we need to ignore in order to complete an activity, or achieve a goal [39].
Using significantly more organizational speech acts during task execution might also reflect working memory (WM) difficulties. WM is the ability to remember information that is no longer perceptible (e.g., the details of a task to be performed on the instruction sheet) and to process it mentally (e.g., repeating the task, and its subcomponents) so that it can be used to achieve a goal, namely the performance of complex tasks (e.g., completing the task successfully) [41]. WM and inhibition control are mutually supportive: by keeping a goal in mind, it becomes easier to distinguish relevant stimuli from those that need to be inhibited, just as it is easier to manipulate multiple pieces of information and recombine them in new ways (e.g., creating an efficient itinerary) to avoid focusing exclusively on one idea [39]. Hence, using significantly more organizational speech acts during task execution might reflect both greater inhibition as well as WM difficulties in mild NCD participants.
Cognitive flexibility is based on inhibition and WM, and can be described as the ability to change perspective, to adapt to the changing demands or priorities of a situation or environment, for example in the way one approaches a problem to be solved or a goal to be achieved when a first avenue proves ineffective or insufficient and an alternative therefore proves necessary [39]. Our results suggest that mild NCD participants did not take instructions into account significantly more than HC. Some mild NCD participants even persevered in not taking instructions into account, while perseveration was not observed in the HC group. As such, perseverating in not taking instructions into account might reflect an increased difficulty of mild NCD participants to disengage from their initial course of action [15], which in turn might reflect cognitive flexibility difficulties.
Mild NCD participants also proved more reactive to the difficulties they encountered during task execution, using speech acts to justify their performance, as well as swearing more frequently and using much coarser language than HC. For the most reactive mild NCD participants, avoidant speech acts were also used to attempt to delegate the execution of a task to others, to blame others for their difficulties, and even to threaten to abandon a task deemed too difficult. The use of those highly reactive speech acts was not observed in the HC group. Along with slightly higher anxiety in the group as a whole, we propose that mild NCD participants’ greater reactivity may also be partially explained by their awareness of their cognitive status, which can have a significant impact on how individuals self-monitor their performance and adapt to difficulties [42].
Lastly, our results on mild NCD participants’ and HC’s verification of having completed all tasks (i.e., goal attainment) raised some important questions about their use of strategies as compensation means to effectively complete all tasks. Following task execution, few HC verified having completed all tasks, yet all those who did were correct in their assessment. In stark contrast, most mild NCD participants were incorrect in their assessment of having completed all tasks. Upon that realization, most replicated similar patterns to those observed during task execution: instead of readily taking into account the assistance offered to them to promptly complete all tasks, mild NCD participants produced loops of barriers, further delaying goal attainment, sometimes persevering until the very end. In their study on compensation strategies in older adults, Tomaszewski Farias et al. [43] had the knowledgeable informants of 125 older adults (with various cognitive statuses; normal cognition, mild cognitive impairment, dementia) complete questionnaires regarding their everyday compensation use, as well as their cognitive and functional abilities. The authors’ first hypothesis was that compensation strategy use would be highest in those with mild cognitive impairment, due to these individuals’ increased need for compensation as well as otherwise relatively intact cognitive abilities to use such strategies [43]. Compensation strategies are known to contribute to greater resilience among older adults, even in the face of cognitive decline [43]. Compensation refers to a set of behaviors aimed at mitigating or adapting to loss: as such, compensation strategies are generally employed proactively to delay or minimize loss of function [43]. Various types of cognitively based compensation strategies have been identified in the literature as being used among older adults, primarily to support memory loss [44]. As such, mild NCD participants’ significantly greater use of strategies to organize task execution (e.g., narrating their actions) might reflect an attempt to compensate WM difficulties (i.e., by keeping active in mind what action was just completed, what action should be done next).
Tomaszewski Farias et al. [43] also hypothesized that a higher frequency of compensatory strategy use would predict a better level of everyday functioning, regardless of their participants’ cognitive abilities [43]. In this case, our results suggest otherwise. Indeed, although mild NCD participants used significantly more strategies during task execution, this did not, however, translate into a more accurate verification of having completed all tasks. Our results therefore suggest that the use of more compensatory strategies does not guarantee a better performance, and hint at the importance of the quality of the strategies used. Verification of goal attainment being a crucial component of IADL performance in real life, further studies should investigate the use of strategies along with barriers throughout task execution, and their impact on task completion.
Our study presents some limitations which must be addressed. Our study’s analyses are limited to the strategies and barriers that emerged from the speech acts spoken aloud by participants. We cannot account for participants’ internal speech and, as such, some strategies and barriers were bound not to be included our analyses. Our study also did not document speech acts that might have been produced during goal formulation or planning, since the procedures used to evaluate IADL did not allow for this. The main author was the only coder, and the second and third authors were co-validators of the coding: it may have been more reliable to have naïve coding validators. We also did not document non-verbal communication behaviors. As our sample size was small, and the main objective of our study was qualitative, we did not compute correlations between the documented speech acts and the cognitive profile of our participant, in particular EF. Future studies could explore further the potential of speech acts as a window on EF deficits. Furthermore, while the laboratory-apartment is an experimental setting that approximates a real-life setting, it is not equivalent to a person’s actual home or community [19]. Therefore, participants’ performance of our IADL-adapted tasks might differ from their performance of those tasks in real life. Recent evidence on the functional performance of hospitalized frail older adults with EF difficulties suggested that a home setting may be preferable for a more accurate assessment of their abilities, and that unfamiliar settings may in fact lead to underestimating their performance [45]. Future research on the topic could take into account verbal and non-verbal communicative behaviors to provide a deeper understanding of the impact of EF on goal-oriented task performance, in familiar versus unfamiliar settings.
In conclusion, our results support the idea that patterns of speech acts in the NCD continuum may help better understanding how EF difficulties impact IADL performance from the older adults’ own perspective. As such, this approach may be complementary to traditional questionnaires and performance-based assessments.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
Nathalie Bier is supported by a Research Scholar from the Fonds de la recherche du Québec- Santé (FRQ-S). This project was supported by a grand obtained from the Réseau québécois de recherche sur le vieillissement (RQRV).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.