
Abstract
Background:
Primary progressive aphasia (PPA) is a group of neurodegenerative disorders including Alzheimer’s disease and frontotemporal dementia characterized by language deterioration. Transcranial direct current stimulation (tDCS) is a non-invasive intervention for brain dysfunction.
Objective:
To evaluate the tolerability and efficacy of tDCS combined with speech therapy in the three variants of PPA. We evaluate changes in fMRI activity in a subset of patients.
Methods:
Double-blinded, randomized, cross-over, and sham-controlled tDCS study. 15 patients with PPA were included. Each patient underwent two interventions: a) speech therapy + active tDCS and b) speech therapy + sham tDCS stimulation. A multifocal strategy with anodes placed in the left frontal and parietal regions was used to stimulate the entire language network. Efficacy was evaluated by comparing the results of two independent sets of neuropsychological assessments administered at baseline, immediately after the intervention, and at 1 month and 3 months after the intervention. In a subsample, fMRI scanning was performed before and after each intervention.
Results:
The interventions were well tolerated. Participants in both arms showed clinical improvement, but no differences were found between active and sham tDCS interventions in any of the evaluations. There were trends toward better outcomes in the active tDCS group for semantic association and reading skills. fMRI identified an activity increase in the right frontal medial cortex and the bilateral paracingulate gyrus after the active tDCS intervention.
Conclusion:
We did not find differences between active and sham tDCS stimulation in clinical scores of language function in PPA patients.
Keywords
INTRODUCTION
Primary progressive aphasia (PPA) is a group of neurodegenerative disorders that primarily affects language functions. The current classification for PPA recognizes three clinical subtypes of PPA: semantic variant (svPPA), nonfluent/agrammatic variant (nfvPPA), and logopenic variant (lvPPA) of PPA [1]. Each variant is characterized by several clinical features and a characteristic pattern of brain atrophy. The svPPA is characterized by semantic deficits consisting of object naming, single-word comprehension deficits, and object-identification impairments. svPPA patients typically present predominant left polar temporal atrophy. Patients with the nfvPPA present impaired motor programming, with an effortful and distorted speech consisting of distortions, substitutions, deletions, insertions, or transpositions of speech sounds. Syntactic deficits may also be present in nfvPPA patients. These patients exhibit a left-posterior frontoinsular and perisylvian atrophy. Finally, the lvPPA is characterized by a slow speech rate, with frequent word-finding problems and phonologic paraphasias but without agrammatism or distortions. lvPPA patients also present impaired repetition of sentences and naming impairment but with sparing of single-word comprehension. These symptoms are associated with left inferior parietal and superior temporal pattern of atrophy.
Transcranial direct current stimulation (tDCS), a non-invasive neuromodulation technique, is a promising option for therapeutic intervention on language disturbances [2, 3]. In the last years, a small but growing body of evidence has indicated that tDCS can modulate the language system in patients with neurodegenerative diseases, including patients with PPA [4–12]. These works seem to show significant improvement in some language functions. Also, some studies suggest a beneficial effect of the combination of speech therapy and brain stimulation [13, 14]. However, most of these studies have focused on a relatively restricted set of linguistic abilities.
Here, we presented the results of a pilot study about the efficacy and tolerability of tDCS in patients with PPA. In contrast to most prior studies in which targets of stimulation were more spatially circumscribed, we aimed to use a tDCS montage that maximizes current distribution over a broad network of language areas. As a result, we predicted improvement in a variety of linguistic abilities that could be helpful for all PPA subtypes. Consequently, we used a large battery of language tests to find out which language field could best benefit from tDCS intervention. In addition, we analyzed intervention-related changes over language-related areas using task-based functional magnetic resonance imaging (fMRI) acquisitions.
MATERIAL AND METHODS
Participants
15 PPA patients (four svPPA, five lvPPA, and six nfvPPA) were recruited from the Catalan Frontotemporal Initiative cohort [15]. All participants were fluent in Spanish or Spanish and Catalan native speakers. All diagnoses were performed by a behavioral neurologist following the current diagnostic criteria [1]. Patients were excluded if they had: 1) psychiatric disorders or neurological diseases other than PPA, 2) any contraindication for tDCS [16, 17]; 3) patients with left-hand dominance, 4) severe aphasia defined as Boston Diagnostic Aphasia Examination < 2 or Boston Naming Test < 5 and 5) generalized dementia defined as Mini-Mental State Exam score < 15 [18, 19].
This study has been carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) and was approved by the Hospital Clínic Barcelona Ethics Committee (HCB/2017/0487). Written informed consent was obtained from all patients.
Study design
This study was a double-blinded, randomized, cross-over, and sham-controlled tDCS study. Each patient received two interventions: a) speech therapy + active-tDCS or b) speech therapy + sham-tDCS stimulation. Each intervention consisted of 1 session per day for 10 days of speech therapy combined with active or sham tDCS (Monday –Friday×2 weeks). Each participant was first assigned in pseudorandom order to either active or sham tDCS treatment and three months later to the opposite intervention. Both interventions were scheduled at similar time slots during the day. To ensure a double-blind procedure, the speech therapy intervention and the evaluations were performed by a researcher blinded to the intervention (SBE). Figure 1 summarizes the study design.

Study design. Patients were randomized to the tDCS intervention or the sham intervention. Every intervention consists in 1 session per day for 10 days (from Monday to Friday during 2 consecutive weeks). In a cross-over design, three months after the first intervention, patients performed the other intervention. Evaluations were performed preintervention, postintervention, at one month, and at 3 months. * MRI performed only in a subgroup of 7 patients.
tDCS parameters
The multifocal tDCS montage was planned with the Stimweaver montage optimization algorithm. This montage is aimed at fitting a global language area. tDCS was applied by a multifocal system (StarStim, Neuroelectrics®) using NG Pistim Ag/AgCl circular electrodes with a 1 cm radius placed into the holes of a neoprene cap corresponding to the 10/20 international system for electrode placement, with the central Cz position aligned to the vertex. Seven electrodes were positioned over the scalp at C1, F7, FC1, FC5, Fpz, P7, and PO8 (Fig. 2). The current delivered during the active session lasted 26 min, and it was initially increased and finally decreased in a ramp-up and ramp-down of 15 s. The maximum current delivered by any electrode was 2 mA, while the maximum current delivered through all the electrodes was 4 mA. For the sham condition, the current dosage was composed of a ramp-up of 15 s immediately followed by a 15-s ramp-down at the beginning and at the end of the stimulations to mimic the active stimulation. Electrode impedance was maintained at > 10kΩ and voltage > 26 V.
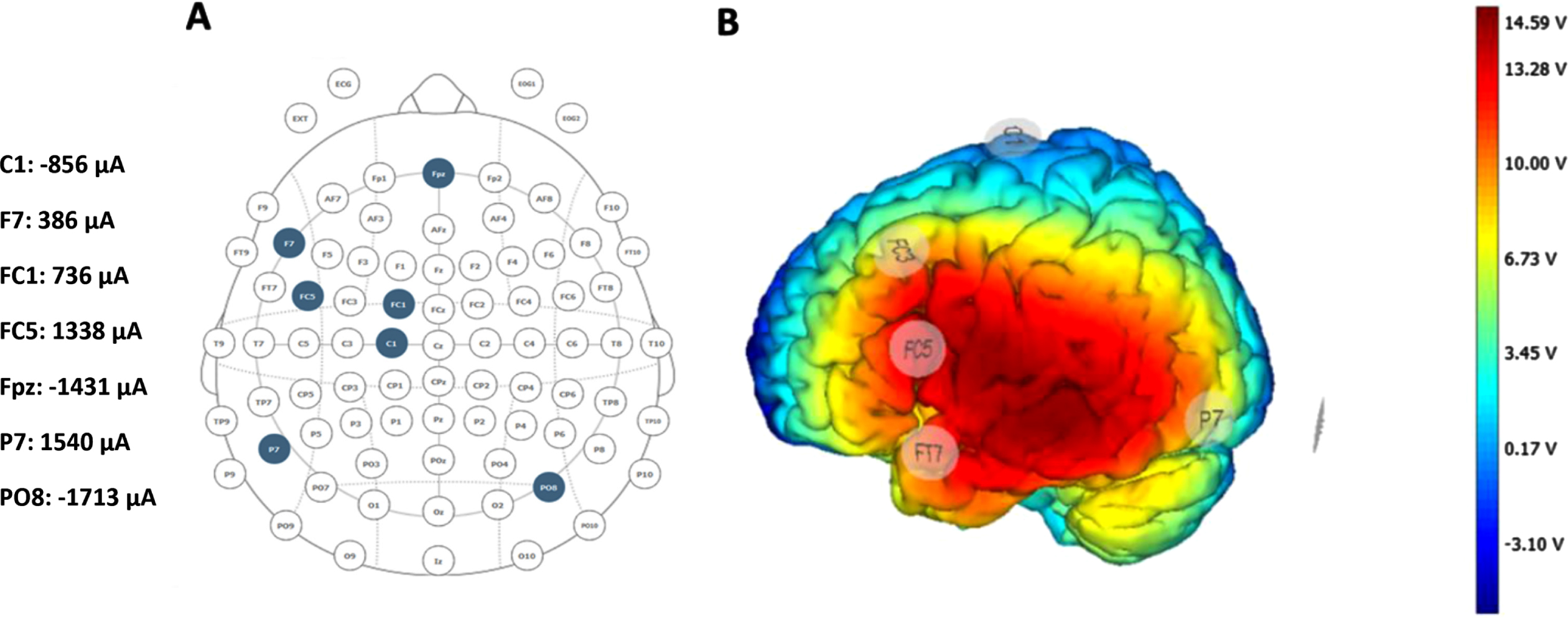
tDCS multifocal montage. A) Electrode positioning, current intensities, and B) electric distribution in the brain cortical surface for the multichannel modeling using the Neuroelectrics Instrument Controller (NIC) engine software. Scale of colors represents the predicted magnitude of the electric field intensity (V). Positive intensity values are shown in red-yellow and negative in blue.
Clinical evaluation
Formal language evaluation was administered immediately before the first stimulation session (t0), immediately following the final stimulation session (t1), at one month after (t2), and 3 months (t3) after the intervention. The neuropsychological evaluation included the following battery of language assessments designed to evaluate a wide range of language abilities: Phonemic fluency: number or words beginning with a specified letter produced in 60 s (trained letters ‘P’, ‘M’, and ‘R’; untrained letters ‘F’, ‘A’, ‘S’); Semantic fluency: number of words from a semantic category produced in 60 s (Animals, fruits, and vegetables as trained tasks; clothes and parts of the body as untrained); Naming (Snodgrass pictures for trained items and Boston Naming Test for untrained ones); Single-word comprehension (Word-to-picture matching from the Cambridge Semantic Memory Test Battery [20] for the trained task and the Boston Diagnostic Aphasia Examination [19] for the untrained task); Semantic association where subjects were asked to choose one of the items that were most closely associated with one target (Camel and Cactus [21] and pyramids and palm trees test [22]); Speech rate: words per minute were measured while subjects read a text.
To investigate for generalization effects each language skill was evaluated by two sets of tests; one of them using items trained during the speech therapy, and the other one using untrained items. Two versions of this language battery were created (A and B), which contained different items for each task, with a similar degree of difficulty for the two of them. Each patient received one battery (A or B) in the first intervention and the other (B or A) in the second intervention (Fig. 1).
At the end of each session, participants were asked to complete a questionnaire to measure the perceived discomfort caused by the intervention on a 10-point-scale (0 = none, 10 = very strong) and the impression-of-change of their language performance (0 = no change, 10 = great improvement). The blinded researcher (SBE) also scored an impression-of-change questionnaire.
Neuroimaging procedure
MRI parameters
We also performed neuroimaging analyses in a subgroup of 7 patients (2 svPPA, 3 nfvPPA, and 2 lvPPA). These participants performed 4 MRI acquisitions, one before and one after each intervention. MRI was acquired in a 3 Tesla Siemens scanner (Magnetom PRISMA) with a 32-channel head coil. The MRI protocol included accelerated multi-band sequences adapted from the Human Connectome Project and provided by the Center of Magnetic Resonance Research at the University of Minnesota. All participants underwent fMRI interleaved acquisitions [T2*-weighted EPI scans, repetition time (TR) = 2000 ms, echo time (TE) = 29 ms, 353 volumes, 40 axial slices, slice thickness = 2 mm, field of view (FOV) = 220 mm, matrix size = 128×128] during the performance of a verbal fluency task. In addition, gradient field map acquisitions and a high-resolution T1-weighted structural image were obtained for each subject with a magnetization prepared rapid acquisition gradient-echo (MPRAGE) three-dimensional protocol (TR = 2300 ms, TE = 3 ms, inversion time = 900 ms, FOV = 244 mm, 1 mm isotropic voxel, matrix size = 256×256).
Verbal fluency task
Task programming was carried out using the Presentation package software (Neurobehavioral Systems), as described in the bibliography [23]. The fMRI paradigm of verbal fluency consisted of a block design where each block was formed by three periods of activation alternating with one-period ‘fixation’ (rest). Activation conditions consisted of ‘repetition’ (repeating continuously the word that appears on the screen; e.g., mountain), ‘semantic fluency’ (generating words from a given category; e.g., plants, furniture, colors), and ‘phonemic fluency’ (generating words beginning with a particular letter). Each load lasted 20 s and was repeated 6 times (8 min in total). Categories and letters for the semantic and phonemic fluency tasks were selected from the Lexesp-Corco database [24].
Outcomes
The primary outcome measures were a) tolerability of the tDCS intervention in PPA patients and b) the changes observed for each task in z-scores between pre and post-immediate intervention. Adverse events were registered for each intervention. Participants were invited to answer a safety questionnaire scoring how uncomfortable the intervention was (0 = no discomfort; 10 maximum discomfort). Secondary outcomes included: a) changes observed for each task in follow-up visits, b) number of subjects who showed measurable language improvement at any follow-up visit after the intervention, c) changes in fMRI activity patterns.
Statistics
All data analyses were performed using RStudio (version 4.0.2). To normalize comparisons across different tests, scores on each test were separately converted to z-scores based on the mean and standard deviation across all participants and time-points. Descriptive results were estimated as the mean and the standard deviation of frequency. Paired T-tests were used to compare these differences between each intervention (active versus sham tDCS). Additionally, the effect side of the tDCS intervention was estimated using paired Cohen’s d test. Multiple comparison adjustments with Bonferroni correction were performed when required. The number of subjects who showed score improvement after the intervention was compared with the χ2 test. Additionally, a linear mixed model was performed to evaluate the effects of tDCS across the different time-point evaluations. All tests were 2-sided, and the significance threshold was set at p < 0.05.
Data from the fMRI were analyzed with the FEAT-FSL software (FMRIB’s Software Library version 5.0.6.; http://fsl.fmrib.ox.ac.uk/fsl/; [25]). We first performed a preprocessing of all individual fMRI scans, which included non-brain tissue removal, motion correction, distortion correction with gradient field map acquisitions (effective EPI echo spacing 0.56 ms; EPI TE = 36 ms; 10% signal loss), spatial smoothing and temporal filtering. Then, at the first level analysis, data were fit to a general linear model (GLM) containing the task time-series with a gamma convolution of the hemodynamic response function [26]. Four regressors related to the different task blocks and their first temporal derivatives were modeled in this GLM: ‘fixation’, ‘repetition’, ‘semantic fluency’ and ‘phonemic fluency’. Then, we defined 2 main contrasts of interest: ‘phonemic fluency > repetition’ task and ‘semantic fluency > repetition’. The results of the first-level analyses were further fit into higher-level or group-level statistics, performed using Local Analysis of Mixed Effects [27]. We created a group GLM design to evaluate: 1) session (pre-tDCS versus post-tDCS)×condition (active versus sham) interactions and 2) patterns of change between sessions (pre-tDCS versus post-tDCS) for each condition (active and sham). All these analyses were performed at a voxel-wise level and the statistical significance of the resulting maps was set at p < 0.05 and z > 3.1 (cluster wise Family-Wise Error corrected).
RESULTS
Participants
Table 1 summarizes the demographics and cognitive performance of all patients at baseline. Thirteen participants completed both interventions. The other two subjects only complete the active tDCS intervention (one because of disease progression and the other loss of follow-up).
Demographic and neuropsychological features of the participants
MMSE, Mimi-Mental State Examination; PPA, primary progressive aphasia.
Safety and tolerability
tDCS was well tolerated in all cases. Mild itching under one of the anodes during the initial and final minutes of stimulation was the most frequent adverse event reported in both interventions. One subject reported a mild headache during the sham intervention. No major adverse events were reported. No significant differences were found between active and sham tDCS interventions regarding safety questionnaires (p = 0.436). Table 2 shows the information on adverse events and the safety questionnaire of all patients.
Adverse events presented by each participant and scores about how uncomfortable the intervention was (0 = no discomfort; 10 maximum discomfort) in both interventions
Effects of tDCS compared with sham
Immediate post-intervention
No differences were found between the active tDCS intervention and the sham tDCS intervention in the immediate postintervention evaluation (p = 0.443). Table 3 summarizes the results for each test. Scores in the trained phonemic fluency were significantly higher for active-tDCS (median = 0.54; sd = 0.62) compared to sham-tDCS (median 0.20; sd = 0.55) (t = 2.36; p = 0.035; cohen de effect size (d) = 0.655). The improvement on the trained semantic association was also significantly higher for active-tDCS (median = 0.79; sd = 0.46) than to sham-tDCS (median 0.39; sd = 0.52) (t = 1.73; p = 0.033; d = 0.479). Finally, the results in untrained reading speed was significantly better for active -tDCS (median = 0.31; sd = 0.45) compared to sham-tDCS (median –0.02; sd = 0.19) (t = 2.89; p = 0.016; d = 0.870). None of these results sustained correction for multiple comparisons. We did not find differences between interventions in any of the other evaluations.
Results for the tDCS and the sham intervention in the baseline evaluation (t0), the postintervention evaluation (t1), and difference between interventions (t1-t0) Results are shown in z-scores. Results were summarized in means with the standard deviation in brackets
When comparing the number of subjects who improved their scores, we did not find any significant difference for any evaluated test between active and sham interventions (Table 2).
Follow-up
Considering all tests together, the linear mixed model showed improvement in all scores at the post-intervention immediate and at 1-month follow-up evaluations for both, active and sham tDCS, (p < 0.01), but no differences between active and sham tDCS (Table 3). The improvement was not significant at 3 months follow-up evaluation (p = 0.083).
Figure 3 represents changes across all evaluation periods in relation to the baseline evaluation for both interventions and each task. For most tasks, the general pattern of outcomes showed improvement immediately following both interventions and decaying over time. No differences between interventions were found when each test was studied separately.
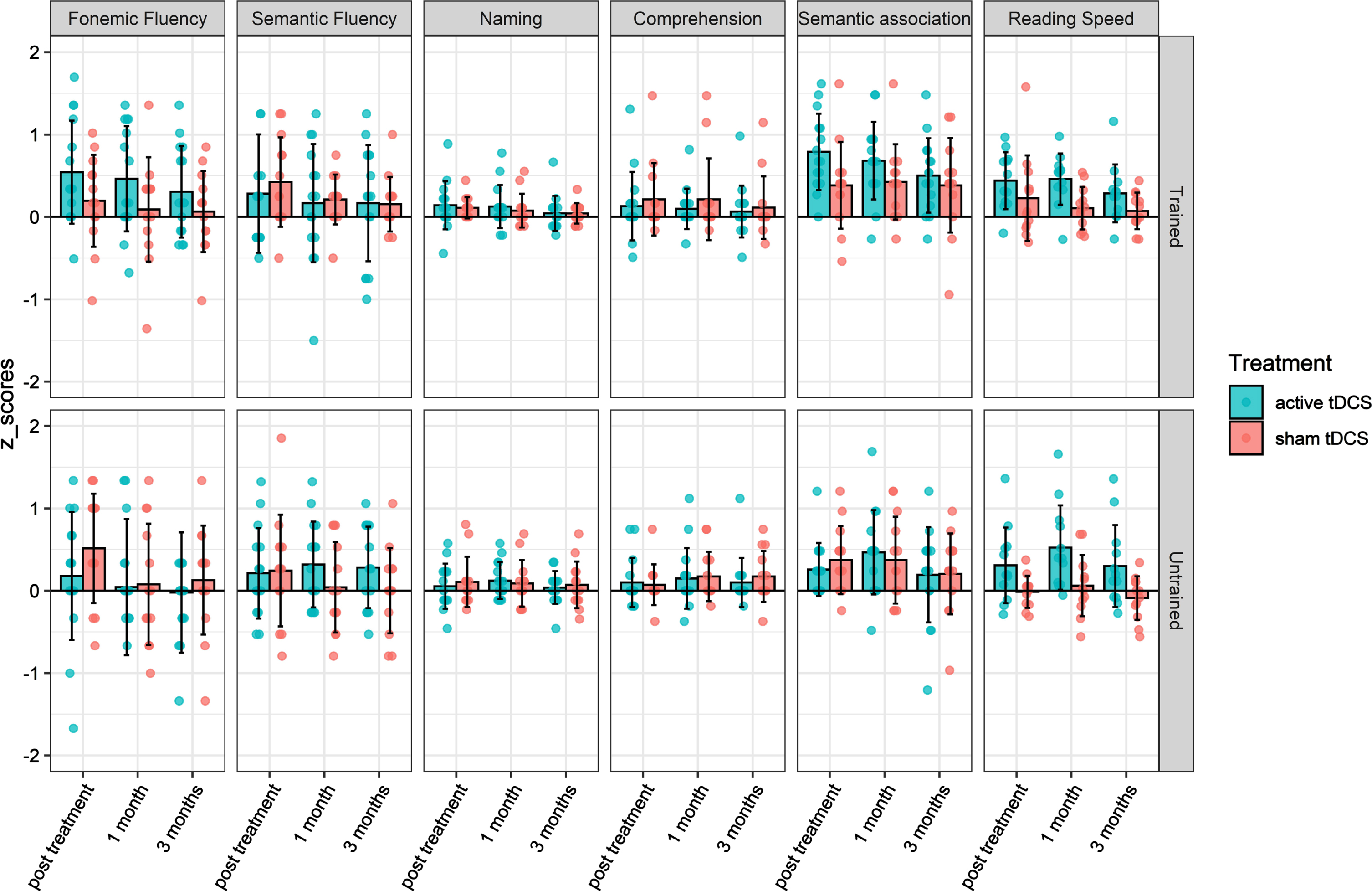
Change in performance in each time-point from baseline. The y-axis represents z-score change from the baseline and the x-axis represents each time-point. Real tDCS outcomes are painted in green and sham outcomes painted in red.
Effects of tDCS by PPA variant
No significant differences were found between interventions when we assessed separately each PPA variant. The Supplementary Material shows results for each variant separately.
Subjective efficacy questionnaires
No statistical differences were found in the efficacy questionnaires fulfilled by the subjects across interventions (median of 6 out of 10 points for both arms; p = 0.929). Any subject reported a difference higher than two points between both arms. In the same sense, no differences were found in the efficacy questionnaires fulfilled by the blinded evaluator.
fMRI results
Regarding the evaluated brain activity associated with our contrast of interest ‘semantic fluency > repetition’ we identified a session (pre-tDCS versus post-tDCS)×condition (active versus sham) interaction in a cluster encompassing the right frontal medial cortex and bilateral paracingulate gyrus (Fig. 4). Furthermore, the change pre-tDCS versus post-tDCS was additionally investigated for each type of intervention. Pairwise analysis for the active condition showed increased activation after the active tDCS application in the same area, while no significant differences were found as regards the sham condition. On the other hand, there was no significant session×condition interaction for the ‘phonemic fluency > repetition’ maps.
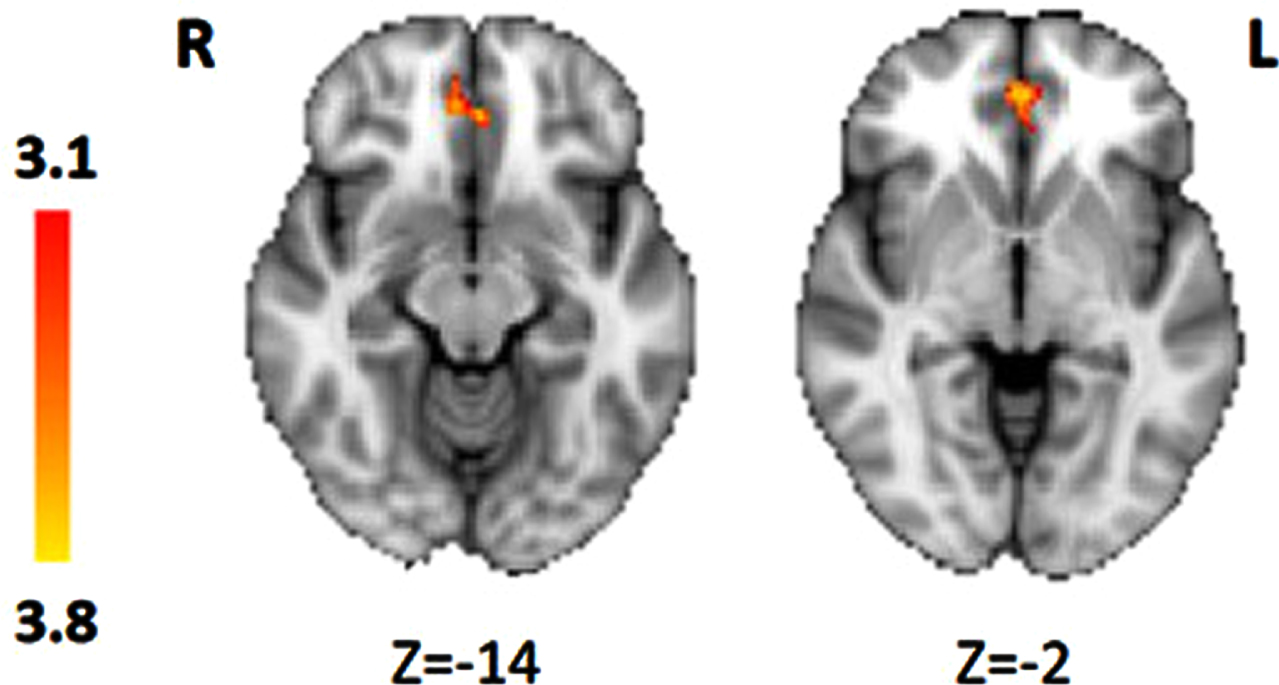
Significant maps for the session (pre-tDCS versus post-tDCS)×condition (active versuss sham) interaction during the ‘semantic fluency > repetition’ contrast, showing increases of activation in the active condition compared to sham after the tDCS intervention in the right frontal medial cortex and bilateral paracingulate gyrus (corrected p < 0.05 and z > 3.1).
DISCUSSION
The present work is a double-blinded, sham-controlled, and cross-over study of the safety and efficacy of tDCS in combination with speech therapy in 15 PPA patients. We evaluate the tDCS efficacy in all three variants of PPA. Previous work assessing the tDCS efficacy in PPA or other aphasiac disorders widely differs on the location of the stimulation. For that reason, and to be able to compare between the different variants of PPA, we performed a multifocal stimulation not only in the impaired language area but in a significant portion of the left hemisphere (Fig. 2). In the same way, the efficacy of the interventions was assessed by a large battery of six different language abilities to cover the different impaired features of the different PPA subtypes and to identify if some language functions are more prone to improvement with the tDCS therapy than others. In addition, we also evaluated differences in fMRI pre and post-interventions in a subgroup of patients.
In consonance with previous work, our study reveals that the tDCS intervention is safe and was well tolerated in PPA patients [10, 28–30]. No severe adverse events occurred during or after the interventions.
Our results did not find differences in any of the evaluated language tasks between the active and the sham tDCS interventions. We found a trend for better outcome with the active tDCS intervention in the trained phonemic fluency, the trained semantic association and the untrained speed-reading tasks, but these differences were not statistically significant after the multiple comparisons correction. Previous works had also shown a possible benefit of active tDCS in semantic association. Teichman et al. reported the efficiency of left-excitatory and right-inhibitory tDCS over the anterior temporal areas in patients with svPPA [10]. As far as we know, no previous studies have evaluated the effect of tDCS in reading. Some reasons could explain our negative results. First, the multifocal approach performed in our study, although has been proven to be able to increase cortical excitability, could not be effective in modulating the language network in PPA patients [31–33]. Second, the small size of our sample implies a low statistical power. This would make it possible that existing differences between interventions might not be detected by our study.
Linear mixed model including intervention and time-point evaluations. Scores were calculated as a composite of all evaluated tests
Of note, we found an improvement in language abilities in a considerable number of subjects after both, active and sham tDCS stimulations. A growing evidence base supports the utility of speech treatment approaches in PPA [34–36]. Although previous studies had shown a positive impact of speech therapy, the design of our study cannot conclude whether the language improvement is due to the speech-therapy, a learning effect in the test scores, or a placebo effect. In any case, this finding points out the relevance of using a sham intervention as a control in tDCS studies.
We also evaluated the mid-term outcomes of the interventions. Even if we did not find differences between active and sham tDCS stimulation, the participants showed improvement in the language scores immediately after the intervention that decayed over time. The linear mixed model revealed significantly better outcomes in the post-intervention and the one-month follow-up, but not in the 3 months follow-up. These results, seen in both trained and untrained tasks, suggest a benefit attributable to speech therapy, a factor common to both interventions [35, 37–39].
The brain fMRI evaluations showed significant changes after both interventions in a subgroup of patients: increased activity in the right frontal medial cortex and the bilateral paracingulate gyrus. These two areas do not correspond with any of the cortical areas stimulated, however distal changes induced by tDCS and capture by fMRI activity patterns have been reported in previous investigations [40]. Increased activity in the active tDCS group was observed in the anterior cingulate/paracingulate cortex, a brain region that holds a potential role in language processing, in particular for tasks that require cognitive control. The frontal medial cortex has also been involved in word-generation studies [41, 42]. As the 3 PPA variants exhibit fluency repetition impairment due to different language deficits, these changes in brain activity might reflect compensatory mechanism that support tDCS-induced language improvements [43].
Our study has some relevant limitations. First, as mentioned before, the sample of our study is small. This is justified because PPA is a rare disease. However, a small sample size implies a low statistical power, especially for the differences found in subgroups of PPA variants. Another limitation of the study is the lack of control groups (without any type of brain stimulation or even without speech-therapy) that provide information about the natural course of the disease. By contrast, one of the strengths of our study is that we evaluated a large battery of different language capabilities in the three different PPA subtypes. This approach would allow defining which potential PPA variants and which language skills are more likely to benefit from tDCS stimulation in case effectiveness is observed with larger sample size.
In summary, tDCS was safe and well-tolerated in PPA patients. However, our study did not find differences in language outcomes between speech therapy associated with active or sham tDCS stimulation. The fMRI analyses showed increased activity after the active tDCS intervention of unknown clinical significance. Nevertheless, this finding suggested that tDCS could be a relevant therapeutic technique in PPA patients because it holds the potential to modulate brain functioning during a language task paradigm.
Footnotes
ACKNOWLEDGMENTS
The authors wish to thank the generous collaboration of all participants and their relatives.
FUNDING
This study was funded by Pla Estratègic de Recerca I Innovació en Salut [PERIS 2016–2020, n° grant: SLT002/16/00408]. Sergi Borrego is supported by the Premi Emili Letang and FBBVA Joan Rodés Josep Baselga grants [Hospital Clinic de Barcelona]. I.Illán-Gala. is supported by the Juan Rodés Contract [JR20/0018 and Health Research Project PI21/00721 from Instituto de Salud Carlos III] and the Global Brain Health Institute [GBHI ALZ UK-21-720973].
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
DATA AVAILABILITY
Sharing of non-identifiable data will be considered at the reasonable request.