
Abstract
Background:
Various intrinsic (related to dementia) and extrinsic (not related to dementia) factors have been suggested to contribute separately to disability in people living with dementia (PLwD).
Objective:
To investigate if the combination of specific intrinsic and extrinsic factors at baseline is associated with longitudinal declines in activities of daily living (ADL) performance of PLwD at 12-month follow-up.
Methods:
141 community-dwelling PLwD-carer dyads were assessed on their global cognition (ACE-III), apathy (CBI-R), carer management styles (DMSS), medical comorbidities (CCI), and ADL performance (DAD) at baseline, and for a subset of participants (n = 53), at 12-month follow-up. Multiple linear regression models were run to assess: 1) the relationships between PLwD’s DAD scores and the remaining variables at baseline and 2) whether these variables’ scores at baseline were associated with longitudinal change in the PLwD’s DAD scores.
Results:
At baseline, having lower ACE-III (β= 0.354, p < 0.001), higher CBI-R (β= –0.284, p < 0.001), higher DMSS criticism (β= –0.367, p = 0.013), lower DMSS encouragement (β= 0.370, p = 0.014), and higher CCI scores (β= –2.475, p = 0.023) were significantly associated with having lower DAD scores. The PLwD’s DAD scores significantly declined from baseline to follow-up (p < 0.001, d = 1.15), however this decline was not associated with the baseline scores of any of the independent variables. Instead, it was associated with declines in the PLwD’s ACE-III scores from baseline to follow-up (β= 1.021, p = 0.001).
Conclusions:
In our limited sample, cognitive changes seem to be the main factor underlying longitudinal decline in ADL performance for PLwD. Carer management styles appear associated with current ADL performance but not with longitudinal ADL decline.
Keywords
INTRODUCTION
Functional disability, which refers to the inability to perform activities of daily living (ADL), is one of the key criteria for a diagnosis of dementia [1]. People living with dementia (PLwD) can over-time experience a decline in their ADL performance with progression of the syndrome, usually starting with instrumental ADLs (e.g., managing finances, driving, preparing meals), and then moving to more basic ADLs (e.g., maintaining personal hygiene, feeding themselves, going to the toilet) later on [2, 3]. Indeed, functional disability is associated with various negative consequences for the PLwD including a loss of autonomy, decreased quality of life, increased risks of being admitted to a care home and hospital, as well as death [4]. Functional disability in PLwD is also associated with increased carer burden and distress [5–7], as well as increased financial costs for health care settings [8].
Considering the impact that functional disability has for the PLwD, their families, and the community at large, studies have attempted to identify factors associated with this disability. The identified factors can broadly be categorized into intrinsic factors— seen in the PLwD and associated with their dementia pathology, and extrinsic factors— seen in the carers of the PLwD and associated with their care recipient’s dementia pathology. The main intrinsic factors identified include cognitive impairment [9], as well as neuropsychiatric symptoms such as apathy and depression [2, 10]. Although not strictly an intrinsic factor per se, the presence of medical comorbidities, which is highly prevalent among PLwD [11], has also been suggested as a factor associated with functional disability in this population [12, 13], although evidence from some studies suggest no significant association between the two [14, 15]. Meanwhile, the extrinsic factors that have been recognized include carer burden [16], depression [17], and management style (i.e., using a criticism style to manage dementia-related issues) [18]. Lastly, findings from a recent study suggested that it may be the combination of both the above intrinsic and extrinsic factors that may best explain functional disability in PLwD. Specifically, this study reported that the combination of having worse cognition, increased apathy, and carers that use a criticism style was significantly associated with greater functional disability in the PLwD [18].
Despite studies having identified both intrinsic and extrinsic factors as being associated with functional disability in dementia, very little is known about whether the combination of both types of factors are associated with longitudinal decline in ADL performance. Considering that PLwD can exhibit variation in their longitudinal patterns of functional decline [19, 20], addressing this research gap is of high importance as results would offer insight on how clinical interventions and services should be designed to help maintain function for longer. Moreover, results could help identify individuals at higher risk of functional decline over a period of time, who can subsequently be targeted and prioritized alongside their carers early on.
To this end, the main aim of this study is to build on a previous study by our team [18] and investigate whether the identified combination of intrinsic and extrinsic factors that were significantly associated with functional disability in a cohort of PLwD at baseline are also associated with longitudinal decline in their ADL performance over a 12-month period. Additionally, a secondary aim is to explore if medical comorbidities will appear to be significantly associated with functional disability at baseline, in addition to the combination of intrinsic/extrinsic factors that were associated with functional disability in our previous study [18]. We hypothesize that individuals with relatively worse cognition, increased apathy, and with carers who use more of a criticism style at baseline will be the ones who exhibit a greater longitudinal decline in their ADL performance, as these factors have been shown to be associated with increased functional disability at baseline by our previous study [18]. We also hypothesize that at baseline, in addition to the factors of cognition, apathy, and carer management style, having higher medical comorbidities will also be associated with increased functional disability, in line with previous studies [12, 13].
METHODS
This study was conducted as a part of the TASKed project, funded by the Alzheimer’s Society, sponsored by the University of East Anglia, and led by the senior author.
Participants
Only individuals with a clinical diagnosis of either Alzheimer’s disease (AD), vascular dementia (VaD), or mixed dementia, living at home, and being between 40–90 years of age were included in the present study as PLwD. The clinical diagnoses of the PLwD were confirmed through letters obtained from consultant neurologists or psychiatrists at the local memory clinics and mental health services that the PLwD attended. Exclusion criteria for the PLwD was having a comorbid major psychiatric disorder, head trauma, alcohol misuse, brain tumor, or being unable to follow single step commands. Inclusion criteria for the carers of the PLwD was being: fluent in English, above 18 years of age, and providing at least seven hours of unpaid support weekly for the PLwD. Signed informed consent was obtained from all PLwD and their carers. If the PLwD lacked capacity to give informed consent, appropriate measures were implemented in line with the Mental Capacity Act of England and Wales: their carers indicated what the likely wishes of the PLwD would have been regarding their participation on the study. Ethical approval was granted by the National Health Service Health Research Authority (IRAS: 199002, REC: 16/LO/0544), and all conducted experiments conformed with the Declaration of Helsinki.
Variables of interest
The study protocol consisted of two research visits at home by the study team members: one baseline and one follow-up visit held approximately 12 months apart. All dyads underwent the baseline visit, whilst a subset of them also underwent the follow-up visit (see Results section for details). In each visit, the PLwD completed:
Addenbrooke’s Cognitive Examination-III (ACE-III)
A validated and widely used screening test for dementia. It assesses global cognitive functioning by assessing five key domains: memory, attention, language, verbal fluency, and visuospatial abilities [21]. Total score is out of 100, with higher scores reflecting higher cognitive functioning [22]. Scores from this scale being shown to be associated with ADL performance in PLwD in our previous study motivated inclusion of this scale in the current study [18].
On both visits, carers of the PLwD completed:
Disability Assessment for Dementia (DAD)
A validated assessment tool that comprehensively measures ADL performance (both basic and instrumental) in dementia, and specific aspects of performance, through an interview [23]. The assessment consists of 40 items, with each item referring to either basic ADLs (e.g., eating, dressing, continence, etc.) or instrumental ADLs (e.g., managing finances, going on outings, preparing a meal, etc.). The carer indicates the PLwD’s competence in performing these activities (in initiation, planning and organization, and effective performance). Total score is a percentage; items which the PLwD never performed in the past (i.e., pre-morbidly) are excluded from this score; higher scores reflect greater competence in performing ADLs.
Dementia Management Strategies Scale (DMSS)
A self-complete questionnaire to identify the management styles carers use to deal with dementia-related problems [24]. The questionnaire is split into three subscales, each representing a different management style: criticism, encouragement, and active management. Each item in each subscale represents a specific strategy used to deal with dementia-related problems, and the carer indicates how often they employ that strategy. Each subscale is scored independently on a continuous scale, with criticism scored out of 44, encouragement out of 32, and active management out of 36. To enable comparisons between the different management styles, the total scores of each subscale are converted into a percentage. As scores from this scale were shown to be associated with ADL performance in PLwD in our previous study, we decided to include this scale in the current study [18].
Cambridge Behavioral Inventory Revised (CBI-R)
A questionnaire measuring dementia-related behavioral changes in the PLwD [25]. The questionnaire assesses items grouped into 10 different sub-scales (i.e., memory and orientation, abnormal behavior, stereotypic and motor behaviors, apathy). Score is the total frequency score of all items in the sub-scale, with higher scores reflecting higher frequency of behavioral symptoms. In this study, although scores from all sub-scales were collected, we focused only on the scores from the apathy subscale, as this was our main variable of interest. With scores from the apathy subscale being shown to be associated with ADL performance in PLwD in our previous study, this motivated the inclusion of this scale in the current study [18].
Charlson Comorbidity Index (CCI)
A validated and widely used index used to predict an individual’s long-term mortality risk based on their medical comorbidity data [26]. The carer indicates all the medical comorbidities listed in the index. The outcome measure is the total CCI score. A score of 0 indicates no comorbidities and the higher the score, the more comorbidities the individual has. When scoring the CCI, the item referring to dementia had been removed due to redundancy, and total scores were adjusted accordingly. This scale was included as an exploratory measure to assess the association of medical comorbidities on ADL performance in PLwD.
Data analysis
The data analysis was conducted in two steps. In step one, we built on previous work from our team which tried to identify intrinsic and extrinsic factors that are associated with the DAD score of the PLwD at baseline [18]. Here, using majority of the same sample as in the previous study, a multiple regression model was run with the PLwD’s baseline DAD scores as the dependent variable and their baseline ACE-III, CBI-R, DMSS criticism, encouragement, and active management scores as the independent variables. Importantly in the current work, we added their baseline CCI scores as an independent variable in the model, to assess if this variable would also be associated with the PLwDs’ DAD scores. In step two, we investigated whether the scores of these same six independent variables at baseline were associated with longitudinal change in DAD score (i.e., from baseline to follow-up). For this, we ran another multiple regression model, with change in DAD scores as the dependent variable and the same baseline scores from the last model as the independent variables. The change in DAD score was calculated by subtracting the follow-up score from the baseline score.
All variables were treated as continuous as opposed to ordinal data to allow a finer grained analysis of how changes in the independent variables affect the dependent variable. For all multiple regression models that were run, multicollinearity of the independent variables were assessed using variance inflation factor values, normality of model residuals were assessed using Shapiro-Wilk tests, and heteroscedasticity of model residuals were assessed using the Studentized Breusch-Pagan test.
All analysis steps were conducted in RStudio software package version 2022.02.1 Build 461, and the results were considered significant at p < 0.05.
RESULTS
Demographics
A total of 183 dyads of PLwD and their family carers in the UK were recruited from September 2016–January 2020. A total of 141 PLwD-carer dyads passed the above-mentioned inclusion/exclusion criteria (see Methods, Participants) and were used for the present study. Of this cohort, 131 PLwD-carer dyads overlap with the sample used in our previous study [18] (which had a slightly different inclusion/exclusion criteria), for which we will be directly comparing some of our results to.
Data were collected from the 141 dyads at baseline, of which 60 were followed-up after a mean duration of 12.20 months (attrition rate = 57.4%). The relatively smaller sample size at follow-up was largely due to two factors: the COVID-19 pandemic, which prevented the study team from holding the second research visit for 39 dyads visited at baseline, as well as participant discontinuation from the study due to either severe decline or withdrawing voluntarily. Of the 60 dyads visited at follow-up, 7 had incomplete data for the variables of interest (due to their carers declining to complete the relevant measures) and were subsequently excluded from the analysis, resulting in a final sample of n = 53. A flowchart depicting the participant sample sizes included at each stage of the study is shown in Fig. 1.
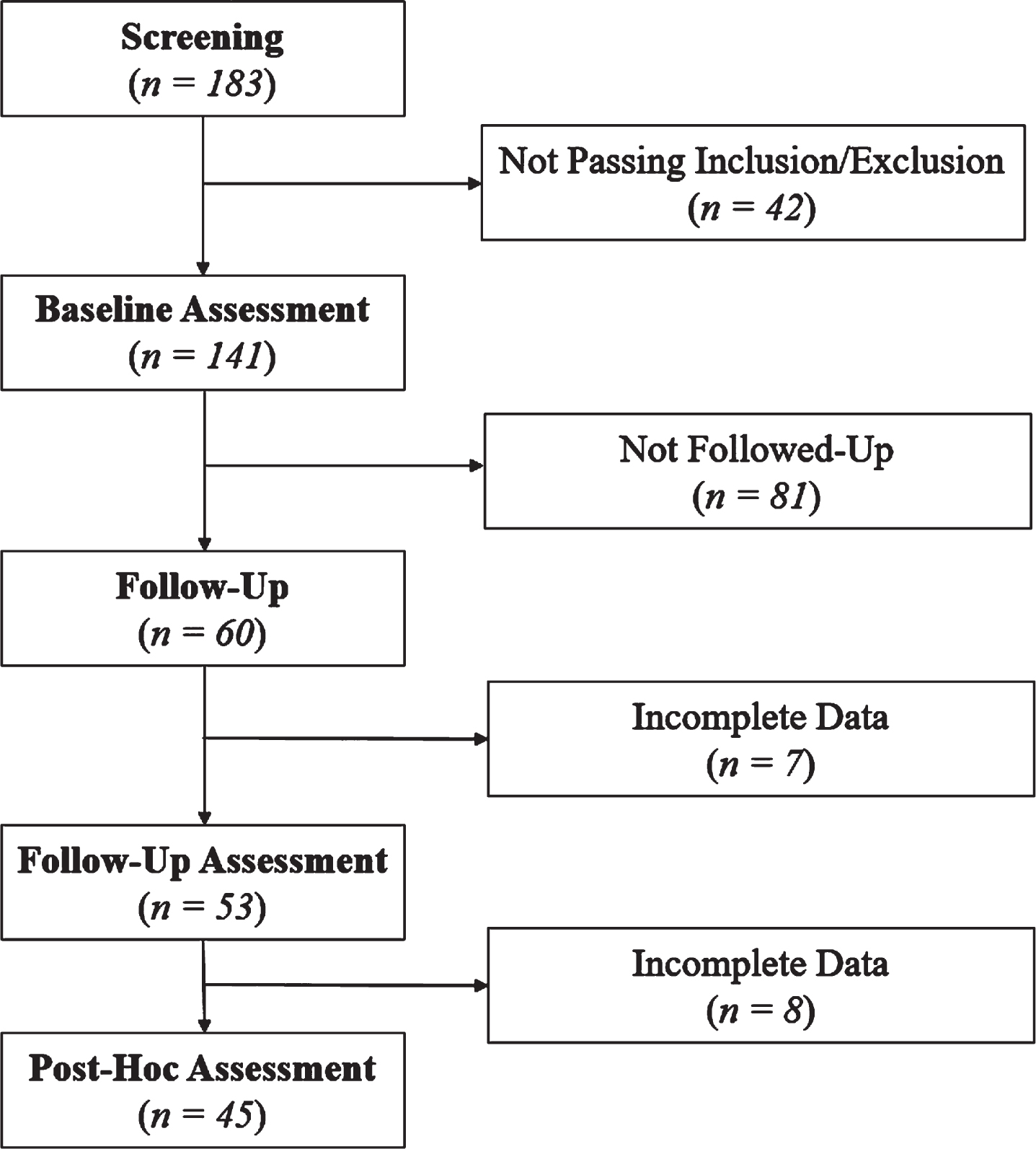
Flowchart illustrating participant sample sizes included at each stage of the study.
Participant demographics, both at baseline and follow-up, are shown in Table 1. Carer demographics, both at baseline and follow-up, are shown in Table 2.
Participant Demographics
Intrinsic and extrinsic factors associated with DAD score at baseline
The results of the first multiple regression model showed that at baseline, the ACE-III (β= 0.354, p < 0.001, 95 % CI [0.164,0.544]), CBI-R apathy subscale (β= –0.284, p < 0.001, 95% CI [–0.425,–0.143]), DMSS criticism (β= –0.367, p = 0.013, 95% CI [–0.657, –0.076]), DMSS encouragement (β= 0.370, p = 0.014, 95% CI [0.075,0.666]), and CCI scores (β= –2.475, p = 0.023, 95% CI [–4.610, –0.340]) of the PLwD were all significantly associated with their DAD scores. Meanwhile, the DMSS active management scores were not significantly associated with the DAD scores (β= –0.089, p = 0.542, 95% CI [–0.380, 0.200]). The current model explained 34.96% of the total variance of the DAD scores (p < 0.001). In this model, none of the independent variables exhibited multicollinearity (i.e., they all had variance inflation factor values less than 5), the residuals were normally distributed, and did not exhibit heteroscedasticity.
Considering that age [27] and diagnosis type [28] (i.e., AD, VaD, mixed dementia) can influence functional disability, as a post-hoc analysis we re-ran our multiple regression model by including age and diagnosis as additional independent variables. We found that the variables of ACE-III (β= 0.376, p < 0.001, 95% CI [0.183,0.575]), CBI-R apathy subscale (β= –0.262, p < 0.001, 95% CI [–0.403, –0.120]), DMSS criticism (β= –0.428, p = 0.004, 95% CI [–0.722, –0.135]), DMSS encouragement (β= 0.341, p = 0.023, 95% CI [0.046, 0.637]), and CCI scores (β= –3.063, p = 0.006, 95% CI [–5.269, –0.856]) continued to be significantly associated with DAD scores even after controlling for age and diagnosis. In addition, we also found that having a diagnosis of Mixed Dementia was associated with having a significantly higher DAD score on average than having a diagnosis of AD or VaD (β= 15.809, p = 0.026, 95% CI [1.903, 29.715]). Meanwhile, age did not appear to be significantly associated with DAD scores (β= –0.034, p = 0.891, 95% CI [–0.528, 0.460]). The current model explained 36.07% of the total variance of the DAD scores (p < 0.001).
Longitudinal changes in intrinsic, extrinsic factors, and DAD scores
We found that the DAD scores of the PLwD significantly decreased from baseline to follow-up (p < 0.001). We also found that the ACE-III scores significantly decreased from baseline to follow-up (p < 0.001), and scores of the CBI-R apathy subscale (p = 0.003), DMSS criticism (p = 0.013), and CCI scores (p = 0.02) significantly increased from baseline to follow-up, all denoting clinical worsening. No significant longitudinal changes were seen in the DMSS encouragement (p = 0.242) and active management (p = 0.111) style scores (see Table 3 for details).
Carer Demographics
Longitudinal Change in Clinical Assessments of the Person with Dementia and Carers (n = 53 for DAD; n = 45 for remaining domains)
***p < 0.001, **p < 0.01, *p < 0.05, ns = not significant.
Association of intrinsic and extrinsic factors at baseline with longitudinal change in DAD score
The results of the second multiple regression model showed that the baseline scores of neither the ACE-III (β= –0.058, p = 0.721, 95% CI [–0.384, 0.268]), CBI-R apathy subscale (β= –0.128, p = 0.288, 95% CI [–0.368, 0.111]), DMSS criticism (β= –0.273, p = 0.257, 95% CI [–0.753, 0.206]), DMSS encouragement (β= 0.091, p = 0.670, 95% CI [–0.336, 0.519]), DMSS active management (β= 0.073, p = 0.727, 95% CI [–0.349, 0.496]), nor CCI scores (β= –1.210, p = 0.519, 95% CI [–4.957, 2.537]) were significantly associated with the longitudinal decline in DAD scores (overall p = 0.438). In this model, none of the independent variables exhibited multi-collinearity (i.e., they all had variance inflation factor values less than 5), the residuals were normally distributed, and did not exhibit heteroscedasticity.
Post-hoc analysis
As the scores of none of the independent variables at baseline were associated with the longitudinal decline in DAD scores of the PLwD, we decided to investigate whether changes in the scores of the independent variables from baseline to follow-up would be associated with the longitudinal decline in DAD scores. Hence as a post-hoc analysis, we ran another multiple regression model. Here, the change in DAD scores of the PLwD was the dependent variable. For the independent variables, we selected only the instruments where the scores of the PLwD significantly changed over 12 months (i.e., ACE-III, CBI-R apathy subscale, DMSS criticism, and CCI scores). The change in scores of these instruments, from baseline to follow-up, were then used as the independent variables in the model. In this model, 8 PLwD had to be removed due to a lack of follow-up data for one or more of the independent variables, leaving a total of 45 participants for this analysis (see Fig. 1).
Our results showed that the longitudinal change in the ACE-III was significantly associated with the change in DAD scores (β= 1.021, p = 0.001, 95% CI [0.435, 1.607]), while a trend towards significance was seen for the change in CCI scores being associated as well (β= 4.286, p = 0.060, 95% CI [–0.203, 8.775]). The longitudinal changes in the scores of the CBI-R apathy subscale (β= 0.031, p = 0.803, 95% CI [–0.218, 0.280]) and DMSS criticism (β= –0.124, p = 0.593, 95% CI [–0.592, 0.342]) were not associated with change in DAD score. This model explained 20.11% of the total variance in the change in DAD scores (p = 0.0108). In this model, none of the independent variables exhibited multicollinearity (i.e., they all had variance inflation factor values less than 5), the residuals were not normally distributed and did not exhibit heteroscedasticity.
DISCUSSION
This was one of the first studies to investigate whether the combination of intrinsic and extrinsic factors at baseline were associated with longitudinal changes in functional disability in PLwD. Additionally, this study examined whether medical comorbidities, when combined with the intrinsic and extrinsic factors from our previous study [18] could explain the variations seen in functional disability for the PLwD at baseline. In line with our hypothesis, we found that at baseline, having a higher number of medical comorbidities was associated with increased functional disability for the PLwD. We also found that neither the level of general cognition, apathy, carer criticism/encouragement/active management, or medical comorbidities for the PLwD at baseline were significantly associated with longitudinal decline in their ADL performance over a 12-month period. This was not in line with our hypothesis that the combination of these intrinsic and extrinsic factors at baseline would be associated with longitudinal declines in ADL performance. Longitudinal declines in ADL performance were instead associated only with decline in general cognition for the PLwD.
Our results from the baseline multiple regression model suggested higher medical comorbidities as a factor that is significantly associated with functional disability in dementia, which is in support of results from other studies [13, 29]. The PLwD in our sample exhibited a range of medical comorbidities including depression, diabetes, peripheral vascular disease, and cerebrovascular accidents. The exact mechanisms underlying how medical comorbidities impact functional disability in dementia depends upon the specific type of comorbidity, however studies increasingly suggest that the presence of medical comorbidities can negatively impact one’s cognitive and physical function, which can in turn affect their functional abilities. For instance, the presence of diabetes (a disease closely associated with dementia) has been shown to be associated with lesions to white matter tissue in the brain, which can over time contribute to cognitive decline in affected individuals [30]. Indeed, cognitive decline often results in individuals being unable to engage in self-management and wellness activities (i.e., preparing healthy meals, exercise, maintain hygiene, etc.), which can subsequently have a negative impact on their functional abilities [31]. From a physiological standpoint, medical comorbidities can give rise to a number of physical issues (e.g., breathlessness, mobility issues, low energy levels, low handgrip strength, etc.), all of which can affect the PLwD’s ability to perform various functional activities [32–34]. Alternatively, having multiple diseases (especially those commonly occurring together) can often result in the diseases interacting with one another and attenuating potential compensatory pathways, resulting in greater functional disability [35, 36]. In addition to the diseases themselves, co-medication for multiple diseases can interact with one another and result in adverse drug reactions, leading to greater functional disability through means of impacting cognitive and physical function [37]. Overall, our results suggest that burden of medical comorbidities, in combination with cognitive ability, level of apathy, and carer management style of the PLwD can explain the variation in functional disability levels seen in this population at baseline.
Our results from the longitudinal multiple regression model suggests that although individuals’ level of global cognition, apathy, burden of medical comorbidities, as well as their carers’ more frequent use of criticism and encouragement management styles were associated with the level of their functional disability in a cross-sectional approach, the same combination of these variables were not associated with longitudinal decline in their ADL performance over a 12-month period. To the best of our knowledge, this is the first study to investigate if the combination of both intrinsic and extrinsic factors for functional disability are associated with longitudinal changes in PLwD’s ADL performance. Previous studies have either only identified factors associated with functional disability at a single time point or investigated intrinsic/extrinsic factors separately in their association with functional decline in PLwD [18, 38–42]. Our results are not in support of findings from previous studies, which have reported carers’ more frequent use of problem-focused coping strategies and PLwD’s higher neuropsychiatric symptoms (which includes apathy) at baseline respectively as being associated with greater longitudinal decline in ADL performance of PLwD [41, 42].
These discrepancies in our results with previous studies could be due to differences in study methodology, with the previous studies having a relatively larger sample size and assessing longitudinal change over a greater time-period (i.e., 4–6 years). More importantly, however, is that the previous studies differed from the current study in the instruments used for the outcome measure (i.e., functional disability), using the Clinical Dementia Rating scale and the Rapid Disability Rating Scale instead of the DAD used here. Although there is no current gold-standard assessment tool for functional disability in dementia [43], future studies should explore which measurement scale has the most ecological validity with regards to accurately capturing changes in functional disability overtime for PLwD. Furthermore, the previous studies used a) the Ways of Coping Checklist, which measures carers’ use of 8 different coping behaviors to look after their own wellbeing, which is different to the DMSS used here, which measures carers’ use of three management styles to practically deal with the PLwD and b) the Neuropsychiatric Inventory to measure behavioral symptom prevalence, which encompasses a range of symptoms compared to our sole focus of apathy in the CBI-R. This considered, we speculate that longitudinal functional decline in PLwD may partly be explained when looking at specific coping strategies of the carer which are not captured by the DMSS, as well as when considering the level of neuropsychiatric symptoms as a whole in the PLwD, as opposed to solely apathy levels. An interesting direction for future studies would be to explore if the development of models which involve the combination of carers’ frequency of using problem-focused coping behaviors and the PLwD’s level of neuropsychiatric symptoms at baseline can accurately predict those with greater longitudinal functional decline in the future.
Our post-hoc analysis results showed that the PLwD who had greater deterioration in their cognitive abilities over the 12-month period were the ones who had greater decline in their ADL performance, suggesting cognitive decline as the main underlying factor for functional decline in this population. With the various cognitive domains, but especially executive function and memory, and the interactions between them being suggested to underlie the ability to perform various functional tasks, it comes as no surprise that deficits in cognition contribute to functional decline [3, 9]. The nature of this relationship may be bidirectional, as decline in functional abilities have also been shown to accelerate cognitive decline in older adults [44]. Overall, this result is in support of findings from previous studies and adds to the growing body of work which show a correlation between cognitive and functional decline in dementia [40, 46]. A worthwhile direction for future studies would be to assess whether it is longitudinal decline in the PLwD’s overall cognitive abilities or specific sub-domains (i.e., executive function and memory) that is relatively more associated with longitudinal declines in their ADL performance.
The results of our study have potential clinical implications. Our findings suggesting that it may not be possible to predict longitudinal functional decline for PLwD using their baseline measurements of the various intrinsic and extrinsic factors, underscores the importance for clinicians to periodically conduct assessments of functional ability for PLwD (either in the clinic or through at home visits). Here, individuals exhibiting relatively greater changes in their functional abilities across assessments, compared to those that are more stable, could potentially be identified as being at risk for greater functional decline in the future. These individuals should ideally be targeted for the development of novel interventions that may help alleviate their functional disability. Although interventions such as cognitive training and cognitive stimulation have been suggested by previous studies to have promise in reducing functional disability in PLwD [47], in general the evidence for the effectiveness of these strategies is still low [48]. These approaches have instead been suggested to potentially be more useful for healthy older adults who may be at high risk for dementia, to alleviate their cognitive and subsequently, functional decline [48]. Importantly, our findings suggest that other extrinsic factors remain to be explored, in particular other modifiable extrinsic factors which may influence declines in ADL performance over time. This may subsequently help inform training for carers as well as contribute to the development of future prediction models and clinical interventions.
Despite our findings, there are some limitations to our study that need to be mentioned. Some participants dropped out of the study from baseline to follow up due to severe cognitive decline, resulting in a potential selection bias for the longitudinal analysis with only participants with relatively less severe decline completing the study. Furthermore, for our multiple regression models in the longitudinal analysis, our sample size was n = 53 and we had 6 independent variables. Since it is recommended to have a minimum of 10 observations per independent variable for regression models, it may be likely that the null results we obtained was due to our analysis lacking statistical power [49]. This limitation in sample size also prevented us from exploring and adding interactions between the independent variables as additional explanatory variables into the model. Another limitation is that we did not consider the factors of genotype [50], severity [51] and type of dementia [39], and age [19], which have all been suggested as influencing rates of functional decline in PLwD by previous studies. Furthermore, in the current study our outcome measure of functional disability (i.e., the DAD score) was based on information provided by the carers. With previous studies suggesting that carers can overestimate/underestimate their ratings of care recipients’ functional abilities [52], the extent to which the DAD scores of our PLwD truly reflect their functional abilities is at present unclear. It is more likely that the DAD only captures the ADL performance of the PLwD, and not be indicative of their functional abilities as a whole. To overcome these limitations, future studies should aim to replicate our analyses using larger samples and investigate if at baseline, the combination as well as interaction of factors such as genotype, dementia stage/severity, and age with various extrinsic factors are associated with longitudinal decline in functional abilities for PLwD. Future studies should also aim to assess PLwD’s functional abilities using performance-based assessments [1, 53], which can make more objective assessments of functional status and potentially detect subtle declines in functional abilities over time, which may not be possible when using carer-based assessments. Lastly, although we tried to ensure that the same researchers conducted the study visits at baseline and follow-up, this was not always possible due to changes in team members, time constrictions, and team member availability. Hence although all researchers were trained in the data collection process, inter-rater variability remains a limitation in our study.
In conclusion, we show that although the combination of various intrinsic and extrinsic factors were associated with functional disability for PLwD at baseline, these same factors were not associated with longitudinal decline in ADL performance of these individuals over a 12-month period. Our study provides a platform for future studies to investigate other extrinsic factors that may be longitudinally associated with functional disability, which can generate knowledge that can be used in future to help maintain ADL performance in PLwD.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all our research participants from across the East of England. We would also like to thank the following colleagues who worked with us on this study: Kayte Rowe, Emma Talbot, Lauren Wright, Zoe Inman, Prof. John O’Brien, Gloria Calderon, Siobhan Rust, Rachel Winson, Chelsea Radakovic, Carmel Moore, Trish Boyton, Kaitlin Dudley, and Ana Paula Trucco.
FUNDING
This work was supported by a project grant from the Alzheimer’s Society (grant number AS-SF-241). This work was also funded in part by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration East of England (NIHR ARC EoE) at Cambridgeshire and Peterborough NHS Foundation Trust. The views expressed are those of the authors and not necessarily those of the NIHR or Department of Health and Social Care.
CONFLICT OF INTEREST
The authors have no conflict of interest to report. J.C. is an Associate Editor of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.