
Abstract
Background:
Preserving activities of daily living (ADL) is the key issue for Alzheimer’s disease (AD) patients and their caregivers.
Objective:
To clarify the ADL level of AD patients at diagnosis and the risk factors associated with decreased ADL during long-term care (≤3 years).
Methods:
Medical records of AD patients in a Japanese health insurance claims database were analyzed retrospectively to determine ADL using the Barthel Index (BI) and identify the risk factors associated with decreased ADL.
Results:
A total of 16,799 AD patients (mean age at diagnosis: 83.6 years, 61.5% female) were analyzed. Female patients were older (84.6 versus 81.9 years; p < 0.001) and had lower BI (46.8 versus 57.6; p < 0.001) and body mass index (BMI) (21.0 versus 21.7 kg/m2; p < 0.001) than male patients at diagnosis. Disability (BI≤60) increased at age≥80 years and was significantly higher in females. Complete disability was most frequent for bathing and grooming. Risk factors for decreased ADL were determined separately by sex through comparing the ADL-preserved and ADL-decreased groups using propensity score matching by age and BI and multivariable logistic regression analysis. In males, decreased ADL was significantly associated with BMI < 21.5 kg/m2, stroke, and hip fracture, and inversely associated with hyperlipidemia. In females, decreased ADL was significantly associated with BMI < 21.5 kg/m2 and vertebral and hip fractures, and inversely associated with lower back pain.
Conclusion:
AD patients with low BMI, stroke, and fractures had increased risks of decreased ADL; such patients should be identified early and managed appropriately, including rehabilitation to preserve ADL.
INTRODUCTION
With the increase of the aging population worldwide, Alzheimer’s disease (AD) and other dementias have been increasing rapidly and have become a public health concern because they are the major causes of disability and dependency in older people [1, 2]. From 1990 to 2019, the incidence and prevalence of dementia including AD increased by 147.95% and 160.84%, respectively [3]. The global number of people with dementia is forecast to increase from 57.4 million cases in 2019 to 152.8 million cases in 2050 [4]. In Japan, the number of people with dementia was 4.1 million in 2019 and is forecast to reach 5.2 million in 2050 [4] with the rapid increase of the population aged≥65 years [5].
AD progresses through three broad phases, consisting of preclinical AD, mild cognitive impairment (MCI) due to AD, and dementia due to AD [1, 6]. Individuals diagnosed with AD have different symptoms, including memory impairment, apathy, disorientation, behavior changes, and even difficulty walking and speaking [1, 2]. Worsening disease in AD patients decreases the scores for activities of daily living (ADL) and quality of life (QOL) in patients and increases caregiver burden and caregiving costs [7–9]. In the year after diagnosis, health service use was found to be dramatically increased in dementia patients [10].
The shortage of nursing care and caregiving services for long-term care are considered serious issues in super-aged countries, including Japan, because a more than 10-year gap exists between life expectancy and healthy life expectancy in these countries [5]. The progression of AD has a major impact on caregivers, in addition to patients. Caregivers for AD patients often assist with one or more ADL, provide emotional support, and manage health conditions [1, 11]. Decreased ADL in AD patients was found to be associated with increased caregiver burden, whereas cognitive decline had less effect on it [12–14]. Therefore, ADL preservation is the key issue for both AD patients and their caregivers.
It is important to recognize the levels of ADL and the risk factors for decreased ADL in AD patients and to make efforts to preserve and improve ADL during long-term care. In the present study, a nationwide database analysis was performed to clarify the level of ADL in AD patients at diagnosis and the risk factors associated with decreased ADL during long-term care for up to 3 years.
MATERIALS AND METHODS
Study design and data source
This was a retrospective case-control study conducted to determine the ADL level of AD patients at diagnosis and the risk factors associated with decreased ADL. This epidemiological study was conducted in accordance with the Guidelines for Good Pharmacoepidemiology Practices [15] and the ethical standards of the institutional review board of Eisai Co. Ltd. and in accordance with the Helsinki Declaration of 1975.
The Japanese health insurance claims database provided by the Japan Medical Data Center (JMDC) was used. The collected data include medical claims (for hospitalization and outpatient treatment) and diagnosis procedure combination (DPC) assessment forms, which are documents that the Japanese Ministry of Health, Labour and Welfare requests medical institutions to provide [16, 17]. The forms consist of a comprehensive evaluation of diagnostic categories and are a method of calculating medical expenses for defining daily hospitalization expenses for each diagnostic category. To protect personal information, data from medical institutions are collected as anonymized information on the basis of a personal identifier for each medical institution with which individuals cannot be identified. The database is widely available, on a fee-paying basis, for use in surveys, research, and commercial purposes and can be accessed after completing the contract for use of specific data. The database contains survey data for more than 9 million cases from more than 200 acute care hospitals in Japan, and publication of studies using this database has been increasing in recent years [16, 17]. The data extracted included administrative claims and clinical information for all inpatients discharged from participating hospitals. The database contains an anonymized patient identifier, sex, age, hospitalization summaries, disease history, medical claims data, and other data related to patients’ conditions.
Disease definitions and analysis population
According to the International Statistical Classification of Diseases: 10th Revision (ICD-10), AD patients were identified with a definitive diagnosis code of F00 and G30 in the data collected from April 1, 2014 to May 31, 2022.
To understand disease comorbidities, the records of relevant comorbid diseases were collected for 6 months before and after diagnosis using ICD-10 codes for cancer (code: C), diabetes mellitus (E10-14), hyperlipidemia (E78), depression (F32-33), insomnia (F51, G47), stroke (G45, I60–64, I69), hypertension (I10–15 codes), pneumonia (J12–18), chronic obstructive pulmonary disease (COPD: J40–47), lower back pain (M40–48, M50–54), osteoporosis (M80–82), vertebral fractures (S30-39), and hip fractures (S70-79).
In the analysis of BMI, the cut-off for low BMI was defined as 21.5 kg/m2, because the target BMI recommended for the population aged≥65 years ranged from 21.5 to 24.9 kg/m2 in the 2020 version of the Dietary Reference Intakes for Japanese officially announced by the Ministry of Health, Labour and Welfare, Japan [18].
Evaluation of ADL decrease and analysis of risk factors associated with decreased ADL
Records for ADL at diagnosis and during the observation period of up to 3 years were collected from the in-hospital database recorded at discharge. The ADL level was evaluated by the Barthel Index (BI), which was essential for evaluating disability of self-care activities in the BI items, including feeding, transfers, grooming, toilet use, bathing, ambulation, stair climbing, dressing, bowel care, and bladder care. BI was evaluated at diagnosis and during the observation period, and patients without a record of the ADL score at baseline or during the observation period were excluded. The BI score ranged from 0 to 100. Patients with a BI≤60 were defined as patients with ADL disability [19, 20]. In the analysis of disability changes in BI items, complete disability was defined as a zero score for each BI item.
In the separate analysis of decreased ADL by sex, patients with BI≥65 at baseline were divided into the ADL-preserved group and the ADL-decreased group, based on the lowest BI during the observation period of up to 3 years. The ADL-preserved group included patients with the lowest BI≥65, whereas the ADL-decreased group included patients with the lowest BI≤60 during the observation period of up to 3 years. The ADL-decreased group was compared with the ADL-preserved group to identify the risk factors associated with decreased ADL after propensity score matching by age and BI at baseline. Matching was performed on a 1 : 1 basis, separately for male and female patients, between the ADL-decreased group and the ADL-preserved group without replacement using a caliper width of 0.15 standard deviations of the logit of each propensity score. Adequate variable balance after matching was confirmed with a standardized mean difference (SMD) of less than 0.1 [21].
Statistical analysis
Statistical analysis was performed using R 4.2.1. Student’s t-test for continuous variables and Fisher’s exact test for categorical variables were used to assess differences between two groups. A logistic regression model was used to perform multivariable analysis with the lowest BI status during the observation period as the outcome and low BMI (<21.5 kg/m2) and the presence of 13 major comorbidities as covariates. Age and baseline BI were considered as confounders for matching, as mentioned above. The database used for this analysis is constrained by the fact that ADL data were only obtained at the time of admission; therefore, logistic regression analysis was used with the lowest BI status as the endpoint, rather than an analysis method with an assumption of time-series constancy, such as a Cox proportional-hazards model-based analysis.
RESULTS
A total of 16,799 AD patients (mean age at diagnosis: 83.6 years, 61.5% female) were analyzed (Table 1). Female patients were older (84.6 versus 81.9 years; p < 0.001) and had lower BI (46.8 versus 57.6; p < 0.001) and body mass index (BMI) (21.0 versus 21.7 kg/m2; p < 0.001) than male patients at diagnosis. Average BI was lower in female patients (46.8) than in male (57.6) patients, and the percentage of patients with BI≤60 was significantly higher in female (64.0%) than in male (52.0%) patients. BI was evaluated only once during the observation period in 63.9% of patients, and the rate was higher in female (65.2%) than male (61.8%) patients.
Characteristics and comorbidities of AD patients
Age, BMI, and BI were extracted from the patient records at the time of diagnosis and are shown as average (Ave) and standard deviation (SD) values. Disease comorbidity was extracted for 6 months before and after diagnosis and is shown as patient number (N) and the rate (%). AD: Alzheimer’s disease, BI: Barthel index, BMI: body mass index, COPD: chronic obstructive pulmonary disease.
The rates of stroke, diabetes mellitus, cancer, pneumonia, and COPD were higher in male than in female patients, whereas the rates of hyperlipidemia, osteoporosis, depression, vertebral fracture, and hip fracture were higher in female than in male patients (Table 1). It is important to note that the rates of comorbid osteoporosis, hip fracture, and vertebral fracture were 3.1-fold, 3.1-fold, and 1.5-fold higher, respectively, in female than in male patients.
Figure 1 shows the age distribution of male and female patients at AD diagnosis, which peaked at 83 years in male and 86 years in female patients. The number of AD patients was higher in female than in male patients at age≥78 years. The percentage of patients with disability (BI≤60) increased at age≥80 years and was significantly higher in female than in male patients at age≥75 years (Fig. 1).
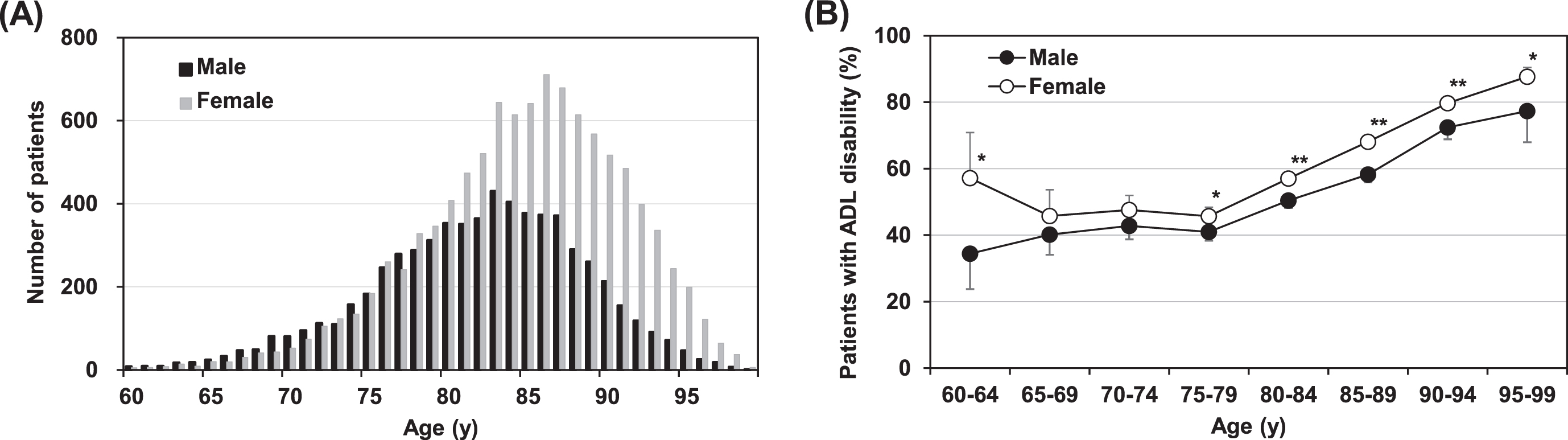
Age distribution of AD patients and the rate of AD patients with ADL disability. A) The numbers of male (black column) and female (gray column) AD patients are shown by age at diagnosis. B) The rate of male (black circle) and female (white circle) patients with ADL disability (BI≤60) by age at diagnosis. AD, Alzheimer’s disease; ADL, activities of daily living, *p <0.05, **p <0.01.
The increase of complete disability in each BI item with the decrease of the total BI score was evaluated in AD patients (Table 2). At BI scores of 45-60, BI items showing complete disability in more than 50% of patients were bathing and grooming in male and female patients. At BI scores of 25-40, additional BI items using the same criteria were stair climbing in male and female patients and ambulation in female patients. At BI scores of 0-20, all BI items showed complete disability in more than 50% of patients.
Increase of complete disability of ADL in each BI item with the decrease of the total BI score
Patient numbers (%) showing complete disability of ADL were summarized for each BI item with respect to the total BI score. Underlined patient number (%) indicates complete disability of ADL in more than 50% of patients. ADL, activities of daily living; BI, Barthel index.
Because the age distribution and BI at diagnosis and comorbidities differed between male and female patients, risk factors for decreased ADL were determined separately by sex. In the separate analysis of decreased ADL for male and female patients, a total of 3,111 male patients and 3,719 female patients with BI≥65 at baseline were divided into two groups based on the lowest BI during the observation period of up to 3 years: the ADL-preserved group and the ADL-decreased group (Table 3). Because patients in the ADL-decreased group were older and showed lower BI than the ADL-preserved group, propensity score matching by age and BI was conducted separately for male and female patients. SMD values of less than 0.1 in age and BI clearly indicated adequate variable balance after matching in male and female patients. The average age of the ADL-preserved group and the ADL-decreased group was 81.3 years and 81.0 years in male patients and 82.6 years and 83.0 years in female patients, respectively.
Propensity score matching by age and BI between the ADL-preserved group and the ADL-decreased group
Patients with BI≥65 at baseline were divided into the ADL-preserved group and the ADL-decreased group, based on the lowest BI during the observation period of up to 3 years. Age and BI are shown as average (Ave) and standard deviation (SD) values before and after propensity score matching. SMD values less than 0.1 for age and BI clearly indicate adequate variable balance after matching in male and female patients, respectively. ADL, activities of daily living; BI, Barthel index; SMD, standardized mean difference.
The risk factors associated with decreased ADL were identified by comparing the ADL-decreased group and the ADL-preserved group by multivariable logistic regression analysis, separately for male and female patients (Table 4). In male patients, decreased ADL was significantly associated with BMI < 21.5 kg/m2, stroke, and hip fracture, and inversely associated with hyperlipidemia. In female patients, decreased ADL was significantly associated with BMI < 21.5 kg/m2, vertebral fracture, and hip fracture, and inversely associated with lower back pain (Fig. 2).
Multivariable analysis of risk factors associated with decreased ADL during long-term care in AD patients
The incidences of low BMI and the comorbidities are summarized as patient numbers (N) and rates (%). A logistic regression model was used to perform multivariable analysis, and the results are shown as odds ratios. AD, Alzheimer’s disease; ADL, activities of daily living; BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease.
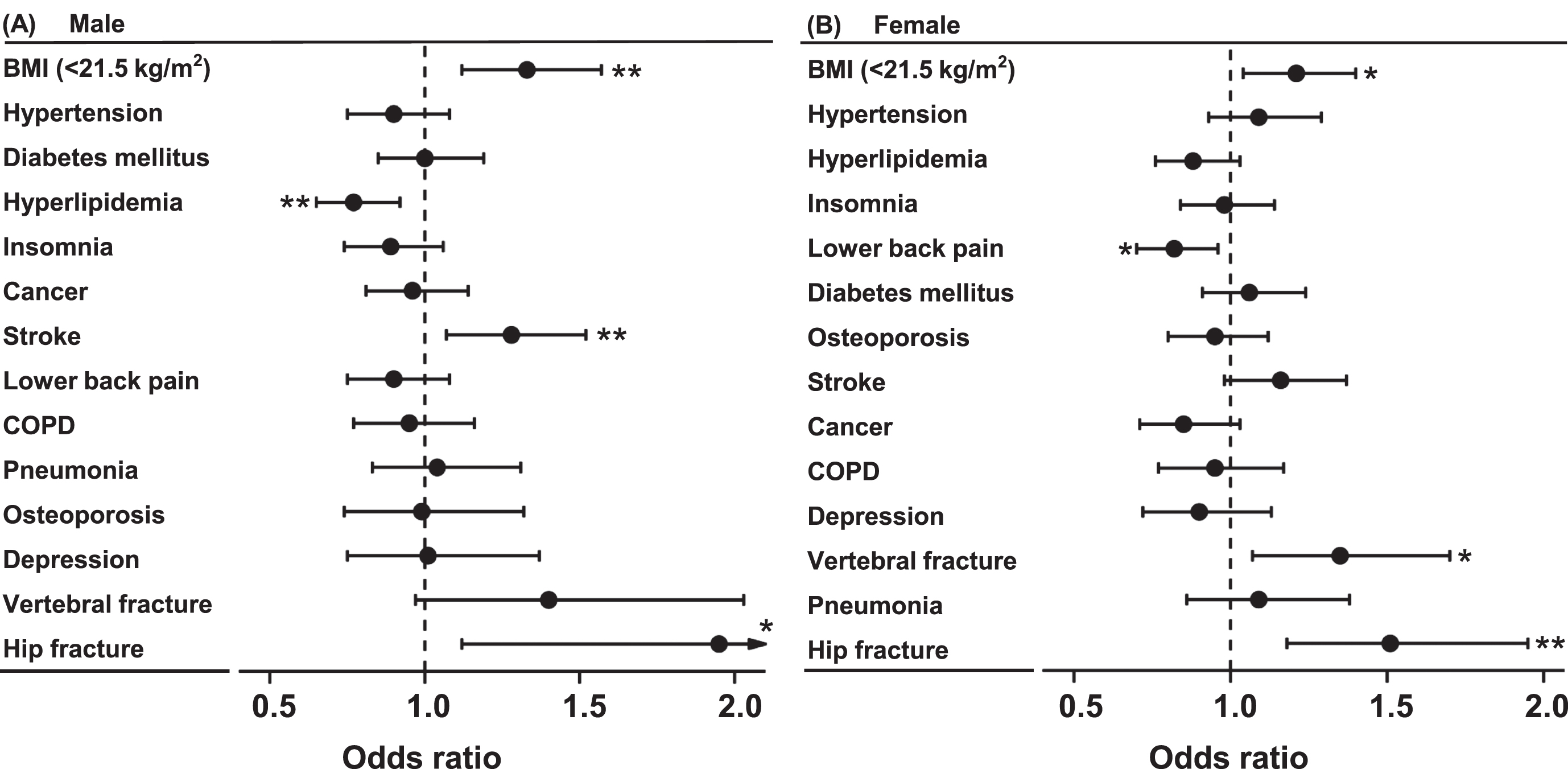
Forest plots of multivariable analysis identifying risk factors associated with decreased ADL. A logistic regression model was used to perform multivariable analysis in male (A) and female (B) patients, and odds ratios and 95% confidence intervals (CIs) are shown. AD, Alzheimer’s disease; ADL, activities of daily living; BMI, body mass index; COPD, chronic obstructive pulmonary disease, *p <0.05, **p <0.01.
The increase of BI items showing complete loss of ADL during the observation period of up to 3 years was evaluated in patients in the ADL-preserved group and the ADL-decreased group (Table 5). The major BI items showing complete loss of ADL in more than 90% of patients were bathing and grooming in male and female patients in the ADL-decreased group. No relevant changes were seen in patients in the ADL-preserved group during the observation period.
Increase of complete disability of ADL in AD patients during long-term care
Patient numbers (%) showing complete disability of ADL are summarized in the ADL-preserved group and the ADL-decreased group. Underlined patient numbers (%) indicate complete disability of ADL in more than 90% of patients. AD, Alzheimer’s disease; ADL, activities of daily living; BI, Barthel index.
DISCUSSION
The results of this study provide nationwide, real-world evidence in Japan for the age distribution of AD patients and decreased ADL with age. The diagnosis of AD peaked at age 83 years in male and 86 years in female patients. The total number of AD patients was higher in female than in male patients. In addition, the percentage of AD patients with disability increased at age≥80 years in male and female patients and was higher in female than in male patients. The appropriate timing of medical checkups to evaluate cognitive function and the ADL level and optimal management may differ between male and female AD patients.
The present study demonstrated that low BMI at diagnosis was the independent risk factor for decreased ADL during the observation period for up to 3 years in both male and female patients. Decreased ADL in low BMI individuals has been reported in other studies. The cohort study with 12,376 Japanese individuals with dementia aged > 65 years showed that BMI < 23 kg/m2 was a risk factor for disability due to dementia [22]. The nationwide database study in Japan found that underweight BMI (<18.5 kg/m2) was significantly associated with low BI of ADL and a higher overall complication rate in 13,348 elderly patients with femoral fractures [23]. The significant association of low BMI with decreased ADL was also reported in studies of nursing home residents [24, 25]. Importantly, poor nutritional status was significantly correlated with low BMI, low muscle power, and low BI of ADL in elderly individuals [26, 27], and a randomized, controlled trial showed significant improvement of ADL by nutritional supplements [28]. In Japan, the optimal BMI range of 21.5 to 24.9 kg/m2 was recommended for the population aged≥65 years in the 2020 version of Dietary Reference Intakes for Japanese [18]. Appropriate education and management of nutritional status and BMI may preserve ADL in AD patients.
In the present study, decreased ADL was associated with stroke in male but not in female patients. Stroke has been reported to increase the risks of decreases in both cognitive function and ADL. Fifty-seven percent of stroke patients without pre-existing cognitive impairment developed cognitive decline one year after stroke [29]. The coincidence of stroke with cognitive impairment increased the severity of ADL decline, compared with either alone [30, 31]. A systematic review of time course studies showed that patients with impaired motor function of the leg were at higher risk of decreased ADL after their first stroke [32]. The small impact of stroke on decreased ADL in female patients may be due to their lower rate of comorbid stroke than male patients.
The present study also showed that decreased ADL in AD patients was associated with hip fractures in both male and female patients. AD was significantly associated with a 2.5-fold higher risk of hip fracture compared with non-AD controls [33]. In addition, an increased incidence of dementia was reported in patients who developed hip fractures, but not vertebral or non-hip non-vertebral fractures [34]. Because older individuals with dementia have a greater decrease in motor function and impaired neurological reflexes during falls, they may land on the hip and have a higher risk of hip fracture [34]. In contrast, decreased ADL in AD patients was associated with vertebral fractures in female patients, but not in male patients in the present study. Though frailty progression was increased in osteoporosis patients with hip fractures in male and female patients, it was increased with vertebral fractures in female, but not in male patients [35]. Physical frailty and dysfunction were associated with decreased ADL in AD patients and were more noticeable in female than in male patients [36]. Because female AD patients showed higher rates of comorbid osteoporosis, vertebral fractures, and hip fractures than male patients in the present study, female AD patients with fractures and their caregivers may need to pay more attention to decreased ADL and obtain appropriatemanagement.
There was an inverse correlation of decreased ADL with hyperlipidemia in male patients and with lower back pain in female patients. Medication for hyperlipidemia was initiated at average ages in the 60 s and earlier [37, 38]. The prevalence of lower back pain peaked at the age of 45–54 years [39], and patients with lower back pain living with disability peaked at 45-49 years in male and female patients [40]. Treatment, education, and management for these comorbidities at younger ages may reduce the ADL decrease in aged AD patients. Further studies are warranted to determine the relationships of comorbidities and decreased ADL in AD patients.
The present study showed that complete loss of ADL was seen in bathing and grooming the most frequently in patients with disability at diagnosis. Bathing and grooming were also the major BI items showing complete loss in patients in the ADL-decreased group during the observation period of up to 3 years. Decreased ADL in bathing was associated with increased caregiver burden and the risk of acute hospitalization of AD patients [12, 41]. Dementia patients spend time undressing and dressing for bathing and instead refuse bathing due to high levels of anxiety [42], and the aggressive behaviors of dementia patients were most frequently seen during bathing [43]. In addition, decreased ADL in bathing was reported as the optimal indicator for discriminating between participants with MCI and those with dementia and between participants with moderate dementia and those with severe dementia [44]. The decreased ability to perform ADL functions such as bathing may confer a greater risk of total ADL decrease in aged individuals and impose an increased burden on caregivers. Careful observation of aged AD patients is necessary to identify their functional changes for the early detection and management of decreased ADL.
Rehabilitation with exercise can adequately protect against decreased ADL by improving muscle strength, muscle mass, and balance. The recent meta-analysis showed significant improvement of ADL by physical activity in AD patients [45]. In Japan, commuting services of outpatient rehabilitation (OR) are available for older adults living at home, and OR users showed less ADL decrease and less deterioration in care levels, compared with users of outpatient day care services [46]. However, cognitive impairment impacted negatively on rehabilitation outcomes. Patients with severe cognitive impairment received shorter therapy hours and gained less on the BI compared with patients without cognitive impairment [47]. Baseline ADL and cognitive function and the risk factors for decreased ADL are the essential components to determine the optimal management of ADL in AD patients. In the present study, BI was evaluated only once during the observation period in 65.2% of female patients and in 61.8% of male patients. Routine assessments of baseline ADL and their changes in AD patients are required in all medical facilities. The increased allocation of healthcare resources to caregivers may lead to preserving ADL and extending healthy life expectancy of AD patients.
Limitations
There is difficulty in data linkage among medical care facilities in the JMDC database. If a patient receives treatment in another hospital, information from the other hospital cannot be identified. It is also important to recognize that the JMDC database consists of information about patients treated at large acute care hospitals in Japan, and, therefore, the population may not be representative of the general population of AD patients. In addition, large effect estimates may result from special conditions in a database analysis, if the confidence interval of the odds ratio is too wide in a small subpopulation [48]. Despite these limitations, the findings of the present study provide physicians insight based on real-world evidence regarding the appropriate management of AD patients.
Conclusion
In conclusion, male AD patients with low BMI, stroke, and hip fracture and female AD patients with low BMI and vertebral and hip fractures had increased risks of decreased ADL. It is important to make a reliable ADL evaluation in early stages and to optimize rehabilitation to preserve ADL in AD patients with higher risks for decreased ADL.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This work was funded by Eisai Co. Ltd. The funder was involved in the collection, analysis, and interpretation of data, the writing of the report, and the decision to submit the paper for publication.
CONFLICT OF INTEREST
All authors report personal fees from Eisai Co. Ltd. during the conduct of the study and personal fees from Eisai Co. Ltd. outside the submitted work.
DATA AVAILABILITY
All data disclosed in this manuscript were generated from the Japanese health insurance claims database provided by JMDC. All information referred to in the manuscript text is disclosed in the figures and tables provided.