
Abstract
Dementia is understood to arise from a mixed etiology, enveloping chronic inflammatory and vascular impacts on the brain, driven by a constellation of modifiable risk factors which are largely mediated by lifestyle-related behaviors. These risk factors manifest over a prolonged preclinical period and account for up to 40% of the population attributable risk for dementia, representing viable targets for early interventions aimed at abating disease onset and progression. Here we outline the protocol for a 12-week randomized control trial (RCT) of a multimodal Lifestyle Intervention Study for Dementia Risk Reduction (LEISURE), with longitudinal follow-up at 6-months and 24-months post-intervention. This trial integrates exercise, diet, sleep, and mindfulness to simultaneously target multiple different etiopathogenetic mechanisms and their interplay in a healthy older adult population (aged 50–85 years), and assesses dementia risk reduction as the primary endpoint. The LEISURE study is located in the Sunshine Coast region of Australia, which has one of the nation’s highest proportions of adults aged over 50 years (36.4%), and corresponding dementia prevalence. This trial is novel in its inclusion of mindfulness and sleep as multidomain lifestyle targets, and in its comprehensive suite of secondary outcomes (based on psychological, physical health, sleep activity, and cognitive data) as well as exploratory neuroimaging (magnetic resonance imaging and electroencephalography) and molecular biology measures. These measures will provide greater insights into the brain-behavioral underpinnings of dementia prevention, as well as the predictors and impacts of the proposed lifestyle intervention. The LEISURE study was prospectively registered (ACTRN12620000054910) on 19 January 2020.
INTRODUCTION
Dementia is a syndrome, most commonly caused by neurodegenerative disease, characterized by complex symptomatology including impaired cognition, behavioral changes, and progressive functional decline, beyond the typical expectations of biological aging [1]. The number of people currently living with dementia is estimated at 50 million worldwide, with this number expected to triple within the next 30 years [2] in the wake of demographic aging and the absence of effective preventative interventions. The evidence to date indicates that dementias, such as that caused by Alzheimer’s disease (AD), are multifactorial in nature and may be classified as age-related neurodegenerative diseases resulting from chronic disease processes initiated in mid-life [3]. Research suggests that dementia is likely preceded by a prolonged preclinical stage whereby interventions may be applied to slow future progression toward disease [4]. Accordingly, the World Health Organization states that research efforts should prioritize the development of interventions aimed at delaying, slowing and even preventing cognitive decline and dementia by targeting a range of modifiable risk factors [5].
A number of key pathogenic mechanisms have been implicated in the development of dementia, including, but not limited to, chronic neuroinflammation [6–8], oxidative stress [9–12], lowered brain metabolism (particularly insulin resistance [13–17], reduced expression of neurotrophic factors (particularly brain-derived neurotrophic factor (BDNF) [18–24]) as well as extracellular accumulations of amyloid-β (Aβ) plaques, which exacerbate pathology [25, 26]. These systemic and neurological mechanisms represent promising targets for non-pharmacological approaches toward dementia risk reduction, as they simultaneously address the heterogeneity of the disease [25].
A number of lifestyle factors have now been shown to impact these brain processes, as well as demonstrate positive health and cognitive outcomes during aging. Four such behaviors are exercise, diet, sleep, and mindfulness practice. Regular exercise has been shown to mitigate oxidative burden [12, 27] and is inversely related to insulin resistance [28–31]. Exercise induced irisin release also appears to be associated with anti-inflammatory processes [32] as well as increased expression of hippocampal BDNF [33]. Furthermore, healthy diets, such as the Mediterranean diet, have been found to inversely relate to inflammatory biomarkers [34] as well as increase the efficiency of the mitochondrion electron transport chain, effectively reducing oxidative stress [25]. Furthermore, adopting a healthy diet strongly reduces biomarkers of insulin resistance while enhancing the peptide’s function [35–38]. Moreover, insufficient sleep duration, inadequate sleep quality, and circadian misalignment detrimentally influence markers of insulin sensitivity [39] and lower glymphatic-vascular-lymphatic clearance of Aβ and tau proteins from neural tissue [40, 41], with better sleep quality also found to mediate the impact of stress on peripheral BDNF levels [42]. Lastly, mindfulness has been shown to downregulate redox transcription factor Kappa B [43], implicated in sustaining chronic inflammatory response cycles [44]. Moreover, there is accumulating evidence that suggests that mindfulness practice is capable of relieving stress which subsequently reduces oxidative burden [25] and augments peripheral BDNF levels [45], altogether reducing Aβ induced neuroinflammation [46]. Importantly, simultaneously targeting these lifestyle factors would likely produce additive or even synergistic effects [47, 48]. These positive impacts are then coupled with the well-documented affective benefits of lifestyle modifications on depression [49–52], a known risk factor for dementia through its influence on neurobiological systems [53]. It is therefore hypothesized that multi-modal lifestyle strategies may collectively leverage factors which positively influence neurogenesis, neural transmission, metabolic health, and Aβ clearance whilst mitigating cellular stress and apoptosis.
In recent years, large-scale RCTs targeting multiple lifestyle domains have gained momentum. One of the first and most influential large-scale European RCTs to investigate a multimodal strategy was the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability trial (FINGER), which utilized a combination of diet, exercise, cognitive training and vascular risk monitoring in an older population at risk for dementia (n = 1,190, Mage 69.3±4.7 years) [54]. The authors reported a significant beneficial effect of the intervention on neuropsychological test battery scores over 24 months, with an estimated mean improvement of 0.20 SD for the intervention group compared with 0.16 SD for active controls (regular health advice). Furthermore, significant mean differences between groups per year for changes in executive functioning and processing speed were seen [55]. Furthermore, exploratory subgroup analysis (n = 112) revealed that a reduction in dementia risk (estimated using the Cardiovascular Risk Factors, Aging and Dementia (CAIDE) risk score [56]) was associated with less pronounced decline in hippocampal volume for those in the intervention arm, but not the control group [57]. While this trial utilized neurocognitive measures as the primary study endpoint, post-hoc analysis demonstrated that multimodal lifestyle interventions reduced dementia risk factors and brain atrophy in a population at risk of dementia. As part of the world-wide FINGERS initiative, several replication trials have since commenced, including an Australian study (AU-ARROW [58]) which largely follows the FINGER protocol and aligns with the US arm of the collaboration (US-POINTER [59]).
Additional multimodal RCTs have published mixed findings. The Prevention of Dementia by Intensive Vascular Care (preDIVA) trial (n = 3,454, Mage 74.5±2.5 years) targeted various cardiovascular risk factors at the individual level, in an unselected population of community dwelling, non-demented older adults [60], and did not identify significant effects on incident dementia at 72 months for the intervention or care-as-usual control group (adjusted mean difference –0.02, 95% CI –0.38 to 0.42, p = 0.93) [61]. The Multidomain Alzheimer Preventive Trial (MAPT) (n = 1,525, Mage 75.3±4.4 years) [62], which provided nutrition counseling, physical activity, and cognitive stimulation with/without omega-3 supplementation in frail older adults with memory complaints, did not find significant changes in cognition at 36 months [63]. A possible reason for these non-significant primary outcomes is that either very large sample sizes, or very long follow up periods, tend to be required to detect the effects of lifestyle interventions on incident dementia and cognitive function in healthy older adults [64, 65]. Because of this, standardized, validated dementia risk scores (a weighted composite of risk factors that reflects the likelihood of developing dementia), have been suggested as an alternative primary endpoint for dementia risk reduction trials [66].
Several tools have been developed to provide a reliable means of assessing dementia risk. These dementia risk scores are developed to be prognostic, incorporating risk factors that have been identified as predictive of subsequent dementia diagnosis based on epidemiological data from cohort studies. The CAIDE score was developed as one of the first and is now a highly validated and cited tool, permitting 20-year dementia risk estimates based on mid-life risk factors [67, 68]. Moreover, The Australian National University Alzheimer’s Disease Risk Index (ANU-ADRI) was developed for public health settings and predicting AD [69], involving an integrated assessment of 15 risk/protective factors [66]. Most recently, the Assessment for Cognitive Health and Dementia Risk Reduction (CogDrisk) was developed as a comprehensive means of estimating risk for any form of dementia, in both high and low resource settings, through the utility of an algorithm encompassing 17 risk/protective factors [70]. The CogDrisk is currently being validated in five external cohorts from the United States and Sweden [70].
Several RCTs have since published results using dementia risk scores as primary endpoints. The Brain Body Life (BBL) RCT (n = 176, Mage 55.5±3 years), which provided a web-based intervention (involving risk factor education, dementia literacy, engagement in physical, social and cognitive lifestyles as well as nutrition and health monitoring) in adults at risk of AD, showed a significant reduction in dementia risk (measured using ANU-ADRI scores) at 12 weeks for the intervention group [71]. Following this, two similar multidomain RCTs also reported significant reductions in dementia risk (measured using ANU-ADRI score) in two different populations: a) community dwelling older adults presenting with several risk factors for dementia (n = 32, Mage 76.8±4.7 years) [72]; and b) middle-aged adults in primary care with BMI of >25 kg/m2 or a chronic health condition (n = 125, Mage 50.8±13.3 years) [73]. Recently the PRODEMOS study joined as one of the few RCTs to investigate dementia risk reduction as a primary endpoint (i.e., CAIDE score) following an app-based, coach-supported multimodal intervention, targeting seven risk factors (overweight, unhealthy diet, insufficient physical activity, smoking, hypertension, dyslipidemia, and diabetes) at the individual level, in older adults (55–75 years) at risk for dementia [74]. To date, no RCT has investigated the effectiveness of a multimodal dementia risk reduction intervention using the CogDrisk as the primary endpoint.
Here we outline our protocol for a multimodal Lifestyle Intervention Study for Dementia Risk Reduction (LEISURE), which integrates exercise, diet, sleep, and mindfulness to reduce dementia risk, measured using CogDrisk. Secondary outcomes include a comprehensive suite of psychological, physical health, sleep activity, and cognitive assessments, as well as neuroimaging [magnetic resonance imaging (MRI) and electroencephalography (EEG)] and molecular biological measures, which will provide greater insights into the neurobiological and cognitive predictors, as well as effects, of the lifestyle intervention on dementia risk in healthy older adults (50–85 years).
METHODS
Study design
LEISURE is a 24-month longitudinal, parallel-group RCT being conducted at the Thompson Institute, Australia (UniSC), enrolling 120 independent community-dwelling older adults aged 50–85 years (Australian New Zealand Clinical Trials Registry registration record ACTRN12620000054910) who satisfy inclusion criteria and are deemed generally healthy. All participants complete baseline assessment and an individual Dementia Risk Report (DRR) is generated detailing their personal dementia risk profile across a range of lifestyle, cognitive, and biometric domains.
Following the baseline assessments, whereby assessor and participant are blind, the program Team Lead randomly assigns participants to either a 12-week multimodal lifestyle intervention (LIFE), designed to target the modifiable dementia risk factors identified in the DRR, or a 12-week control condition. The randomization process is achieved by coin toss, with a 1:1 allocation ratio, absent of any intentional effort to balance the groups.
The primary outcome (i.e., dementia risk) will be assessed for both groups at baseline (T1) and after completion of the 12-week intervention (T2), with secondary outcomes assessed at these timepoints in addition to 6-month (T3) and 24-month (T4) post-intervention. The LEISURE protocol adheres to the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) recommendations (see Supplementary Material 1). The study design for LEISURE is presented in Fig. 1.
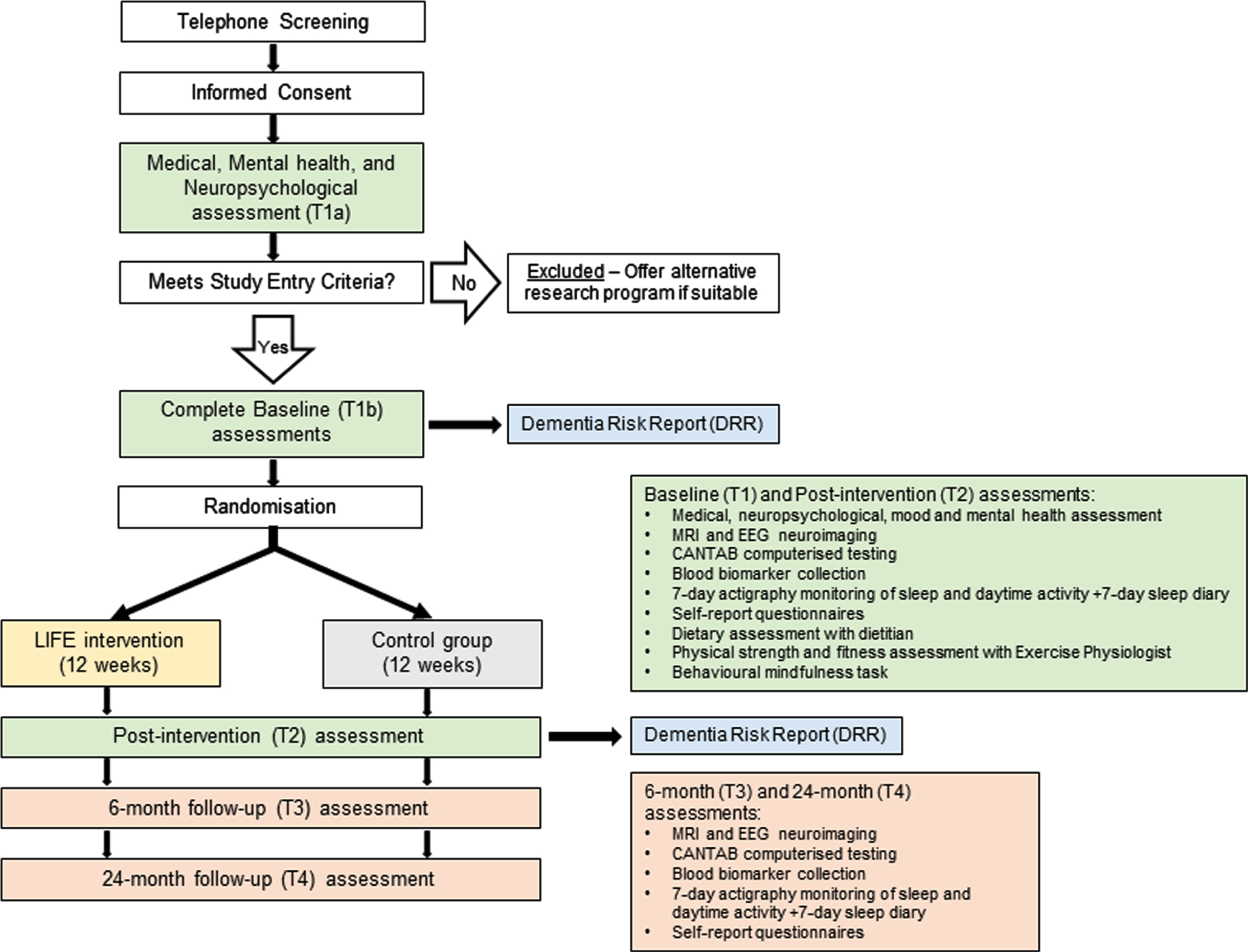
Participant flow chart through the LEISURE study protocol.
Participant selection: Inclusion and exclusion criteria
Participants for LEISURE are recruited from the general community through a study specific webpage, media announcements and local community groups. Eligibility criteria are operationalized both via self-report and clinician assessments. Interested participants first complete a self-report pre-screening survey, which details their medical history/symptoms and identifies potential MRI contraindications. Once pre-screening is satisfied, participants proceed to a telephone interview which confirms an individuals’ preliminary eligibility for the trial following open-ended discussion of study information. Next, those who meet general eligibility criteria have this confirmed via in person assessment. This comprises: a) the Montreal Cognitive Assessment (MoCA) as a screening tool, b) mood assessment and full neuropsychological assessment with a registered psychologist (see Neuropsychological assessment), and c) medical assessment undertaken by a registered nurse (see Medical assessment). Participants are deemed eligible if they are aged between 50–85 years at enrolment, have normal or corrected-to-normal vision, and do not meet criteria for either dementia or mild cognitive impairment (Winblad criteria [75]) on neuropsychological testing. Participants are excluded from enrolment if they meet MRI contraindications (e.g., metal fragments, pacemaker or aneurysm clip); prior head injury with loss of consciousness >60 min; stroke or TIA; symptomatic cardiovascular disease; pulmonary respiratory conditions (e.g., chronic obstructive pulmonary disease); metabolic disorders; currently undergoing chemotherapy; history of schizophrenia or bipolar disorder; major neurological condition (e.g., Parkinson’s disease, multiple sclerosis); epilepsy; current alcohol or other substance misuse; intellectual disability; acute psychosis; insufficient English language skills to complete standardized assessment; current usage of medications known to affect central nervous system (e.g., antidepressant medications); as well as concurrent participation in a conflicting study. Participant recruitment commenced in September 2020 and is ongoing, with a baseline sample size of n = 87 at the time of writing.
Assessments and measures
To determine eligibility, participants complete a medical, mental health, and neuropsychological assessment (T1a). As shown in Fig. 1, only participants who meet eligibility criteria following these assessments are enrolled and progressed to further baseline testing (T1b).
Medical assessment
To determine medical-related dementia risk factors, participants undergo a medical and medication history with a registered nurse. Anthropometric data including handedness, height, weight, body mass index (BMI), waist and neck circumference are acquired. Blood pressure and resting pulse are also recorded, along with a resting electrocardiogram to determine safety to participate in exercise. Smoking, alcohol, and other drug history is recorded. Eyesight is assessed using a Snellen eye chart and hearing is assessed using Weber and Rinne tests. Sleep is assessed using the Insomnia Severity Index (ISI) [76], Obstructive Sleep Apnea (OSA)-50 [77], the Epworth Sleepiness Scale [78], the STOP-Bang questionnaire [79], the International Restless Legs Study Group rating scale (IRLS) [80], and the Satisfaction, Alertness, Timing, Efficiency and Duration questionnaire [81]. Participant data from the medical assessment is used to calculate a CAIDE score [67].
Mental health assessment
A mental health and mood assessment to identify psychological risk factors is conducted by an experienced registered psychologist using the Structured Clinical Interview for DSM-5, SCID-5 [82] along with administration of the British Columbia Cognitive Complaints Inventory [83], State-Trait Anxiety Inventory [84], and the Depression Anxiety Stress Scales (DASS-42) [85].
Neuropsychological assessment
A neuropsychological assessment, conducted by an experienced registered psychologist, will be used to ensure participants meet cognitive eligibility criteria. The neuropsychological assessment battery includes the MoCA [86], Test of Premorbid Function [87], Trail making test A and B [88], Digit Span subtest [89], Logical Memory I and II subtests [89], Rey Complex Figure Test copy, 3’ recall and recognition [90], Rey Auditory Verbal Learning Test immediate and delayed recall [91], 30-item Boston Naming Test [92], D-KEFS Color– Word Interference and Verbal Fluency tests [93]. Occurrence of at least two scores <1.5 SDs below premorbid estimate on two different tests was used for the exclusion of mild cognitive impairment.
The Cambridge Neuropsychological Test Automated Battery (CANTAB)
The CANTAB (Cambridge Cognition, 2019) is a validated, culturally neutral, computerized battery which exploits touchscreen technologies and graphical interface to capture instantaneous, non-verbal responses from participants. Computerized test delivery demonstrates minimized floor and ceiling effects, standardized administration, and high sensitivity to both the speed and accuracy of responses [94] and can be used in conjunction with the aforementioned “traditional” neuropsychological tests. The CANTAB will be presented on an iPad and will include the motor screening task (MOT), paired associates learning (PAL), delayed match to sample (DMS), reaction time task (RTI), spatial working memory (SWM), and rapid visual information processing (RVP).
Blood sample collection
Peripheral venous blood samples will be collected to assess fasting glucose, insulin, total cholesterol (including HDL, LDL, and non-HDL cholesterol), and triglycerides using a commercial diagnostic pathology testing laboratory. Additional samples are collected to (i) evaluate inflammatory process including tumor necrosis factor alpha, interleukins (IL)-1β, IL-6, IL-8, IL-10, inducible nitric oxide synthase (iNOS), nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB) and mammalian target of rapamycin; (ii) cell metabolism including peroxisome proliferator-activated receptor-gamma coactivator (PGC-1α); (iii) vascular status including vascular cell adhesion protein 1, vascular endothelial growth factor, and Endothelin-1; (iv) synaptic plasticity including BDNF, irisin, and APOE. The described markers will be performed by enzyme linked immunosorbent assay (ELISA)/multiplex bead-based assay or gene expression or genotyping, as presented in Fig. 2.

Blood-based biomarker assays to be performed under the LEISURE protocol. (*) gene expressions in PBMCs. (**) ELISA/multiplex bead-based assays in serum/plasma. (***) genotyping in whole blood.
Magnetic resonance imaging
Participants will undertake a non-invasive MRI brain scan at each timepoint to assess baseline and longitudinal impact of the study interventions on structure, function, and perivascular space. In addition, brain-behavior relationships with respect to secondary outcome measures will also be investigated. All brain scans will be acquired at Thompson Institute, Australia (UniSC) utilizing a Siemens Skyra 3 tesla MR scanner (Siemens Medical Solutions, Erlangen Germany) and a 64-channel head-coil. In brief, the scan protocol includes T1-weighted (MP-RAGE) structural scan, T2-weighted structural scan, fluid attenuation inversion recovery (FLAIR) structural scan, diffusion-weighted imaging, and blood oxygenation level dependent (BOLD) contrast imaging. While the scan parameters have been omitted for brevity, list of imaging modalities and subsequent data analysis are shown in Fig. 3.
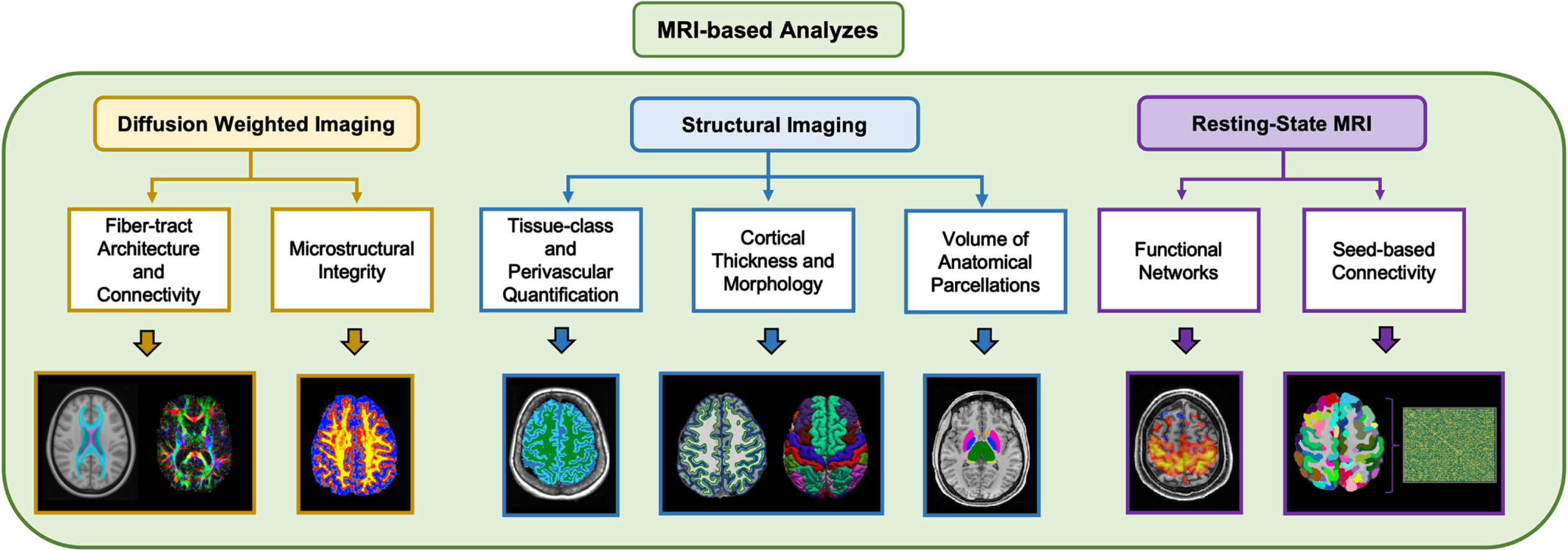
The MRI modalities acquired for the LEISURE protocol, with example data analyses.
Electroencephalography
EEG data will be acquired using a 32-channel Biosemi ActiveTwo system with Ag/AgCl electrodes (Biosemi, Amsterdam, Netherlands). Continuous EEG data will be collected for four minutes in both resting eyes open and resting eyes closed conditions, as well as during a 15-min behavioral mindfulness task. In this task, participants count their in-out breath cycle to 21, reporting each breath with a right-arrow key press and each completed 21-breath cycle with a down-arrow key press (self-caught counting errors are indicated by left-arrow key press). Event-related EEG data will be acquired during two tasks. One, while participants perform a three-tone auditory oddball (presented binaurally over headphone with a 1000 Hz standard tone (70%), a 1500 Hz target tone (15%), and a white noise distractor tone (15%)). Two, the sustained attention to response task, SART [95] assessing both sustained attention and inhibitory control, where participants are required to respond, via button press, to frequent non-target stimuli (numbers 1,2,4,5,6,7,8,9) and to withhold from infrequent target stimulus (number 3).
Activity monitoring
Participants will undertake 24-hour activity monitoring via a non-invasive Actigraph GT3XP-BTLE device (ActiGraph, LLC) worn on the wrist for seven consecutive days to obtain measures of sleep and physical activity levels. The ActiGraph GT3 device contains a tri-axial accelerometer, configured to sample data at 30 Hz. Sleep diary data will be used in conjunction with actigraphy data (extracted using Cole-Kripke scoring algorithm) to calculate various dimensions of sleep, including habitual sleep onset/offset and efficiency, in addition to analyses of acrophase and circadian rhythmicity. Actigraphy data will also be used to measure moderate to vigorous physical activities, in accordance with pre-determined cut-points (extracted using Freedson Adult and Combination (1998) algorithms).
Strength and fitness testing
Functional fitness will be assessed using a modified Senior Fitness Test battery [96] consisting of grip strength, functional chair sit-to-stand test, and tandem, semi-tandem and single leg balance tasks. Participants will also complete a 6-minute walk test (6MWT) to estimate physical fitness, assessed via the distance covered (6MWD). Participants will wear a heart rate monitor during the fitness assessment to determine pre-post intervention changes in heart rate during exercise. This battery of tests is designed for older adults and provides objective assessment of physical function.
Dietary assessment
General diet quality will be assessed in reference to the Australian Guide to Healthy Eating using the Australian Eating Survey (AES) [97]. The AES is a self-administered 120-item semi-quantitative food frequency questionnaire validated in the adult Australian population for comparative validity and reproducibility against gold standard weighed food records. Adherence to a Mediterranean-style dietary pattern will be assessed using the Mediterranean Diet Adherence Screener (MEDAS) [98] and the Mediterranean Diet and Culinary Index (MediCul) [99]. The MEDAS is a 14-item short screening tool validated in English for an elderly Western population and includes 12 questions which assess the main dietary elements of a traditional MedDiet, and two questions related to food intake behaviors consistent with a MedDiet. In contrast, the MediCul is a 50-item survey instrument which assesses adherence to a more traditional Cretan MedDiet and considers aspects of cuisine that are not considered by other dietary indices. Moreover, the MediCul has previously been validated for the assessment of MedDiet adherence in Australian older adults with mild cognitive impairment and those at high risk of dementia [99]. Participants also complete the MedDiet Nutrition Knowledge questionnaire [100] which is a 15-item tool assessing MedDietknowledge.
Self-report questionnaires
An online self-report questionnaire battery will be completed via Qualtrics at each timepoint and will include the Geriatric Depression Scale [101]; the Geriatric Anxiety Inventory (GAI) [102]; the Pittsburgh Sleep Quality Index (PSQI) [103]; the Everyday Memory Questionnaire [104]; the WHO-5 Well-being Index [105]; the UCLA Loneliness Scale [106]; the AUDIT Alcohol Consumption Questionnaire (AUDIT-C) [107]; the Godin Leisure-Time Exercise Questionnaire [108]; the Multifactorial Memory Questionnaire [109]; and demographic information.
Economic evaluation
Psychosocial aspects of quality of life will be assessed utilizing the Assessment of Quality of Life (AQoL-8D) [110]. The AQoL-8D assesses health related wellbeing through 35 items which can be used to calculate quality adjusted life years, a standard outcome measure in economic evaluations. To determine participant’s broader health service resource use, a resource use questionnaire will be completed to value health resources usage in standard Australian unit costs. These tools permit an economic evaluation of the impact of the interventionprogram.
Dementia risk report
The DRR is provided to all participants at completion of baseline assessment, detailing their personal dementia risk profile. These individualized reports not only encourage sample retention at later timepoints, but also allow assessment of intervention benefit beyond simple dementia risk factor education. To assist participants in understanding the information reported, general information regarding dementia and aging, along with an explanation of dementia risk factors and how lifestyle factors contribute to risk, are included in the DRR. Participants’ personal dementia risk profile is reported as either low, medium, or high based upon population normative data or Australian national health guidelines, and is separated into lifestyle, medical, and cognitive domains (see Supplementary Material 2). Providing this profile within these three domains, allows participants to easily ascertain their personal strengths and weaknesses in relation to dementia risk, thereby enabling them to identify priority areas for modification and risk reduction.
Reported items within the lifestyle domain include physical fitness (6MWD); Mediterranean diet (MEDAS); sleep efficiency (actigraphy); sleep quality (PSQI); sleep disorder (OSA, IRLS, ISI); depression (DASS-42); stress (DASS-42); anxiety symptoms (DASS-42); social connectivity (UCLA); alcohol consumption (AUDIT-C); and smoking status. Reported items within the medical domain encompassed in the DRR include BMI; waist circumference; total cholesterol; total cholesterol:HDL ratio; systolic and diastolic blood pressure; and hearing loss. Reported items within the Cognitive domain includes short-term visual memory (CANTAB DMS picture matching accuracy, and percent correct for 0 s, 4 s, and 12 s delay); visuo-spatial memory and learning task (CANTAB PAL total errors and first attempt score); and attention and control (CANTAB RVP A′ and probability of false alarm).
Study outcomes
Primary outcomes
Dementia risk. Change in CogDrisk dementia risk score from T1 (baseline) to T2 (immediately following the 12-week intervention period). The CogDrisk score comprises an algorithm containing up to seventeen risk/protective risk factors including age, sex, education, mid-life obesity and high cholesterol, diabetes, stroke, traumatic brain injury (TBI), hypertension, atrial fibrillation, insomnia, depression, physical inactivity, cognitive and social engagement, fish intake, and smoking. For each participant, a score for each risk/predictive factor will be provided based on scoring guidelines [70], and will be based on a) self-report measures (age, sex, education, diabetes, stroke, TBI, atrial fibrillation, insomnia, depression, cognitive and social engagement, fish intake and smoking); b) medical assessment (mid-life obesity (for participants aged < =65 years), high cholesterol (<60 years), and late-life hypertension (>65 years)); and actigraphy (physical inactivity). The range of scores are 0 to 46.4 for late-life adults (>65 years), and 0–34.4 for midlife adults, where a higher score indicates higher risk of dementia. The CogDrisk has been recently developed with the most recent evidence for dementia risk [70].
Secondary outcomes
Secondary outcomes include change in a) CogDrisk score from T1 to T3 (6 months post intervention) and T4 (2 years post intervention); b) CAIDE score from T1 to T2, T3, and T4; improvements in c) cognitive functioning (e.g., CANTAB RVP A’, RTIMSMT); d) physical activity and fitness (e.g., actigraphy measured activity intensity, 6-minute walk test); e) diet quality (e.g., MEDAS); f) mood and anxiety (e.g., GAD, GAI); g) cardiovascular health (e.g., waist circumference, Total cholesterol:HDL ratio); h) sleep (e.g., actigraphy measured sleep efficiency); i) MRI (e.g., structural brain changes); j) EEG (e.g., changes in 1/f aperiodic activity); and k) blood biomarkers, including those related to inflammatory profile and oxidative stress (e.g., IL-1β and iNOS, respectively).
Exploratory outcomes
Identification of novel biomarkers of healthy brain aging, including MRI (e.g., functional brain changes), EEG (e.g., event related potentials), blood biomarkers (e.g., synaptic plasticity (e.g., BDNF)), changes in vascular endothelium (e.g., endothelin-1), and enhanced cell metabolism (e.g., PGC-1a, NF-kB, and irisin). Furthermore, changes on additional measures of a) cognitive function (e.g., CANTAB DMS, PAL, MOT, SWM); b) physical activity and fitness (e.g., sit-to-stand test, grip strength test); c) diet (e.g., MediCul, AES); d) cardiovascular health (e.g., BMI); and e) sleep (e.g., dimensions of sleep health such as satisfaction, regularity, and duration).
Dementia risk reduction interventions
All participants complete baseline assessment and receive their individual DRR prior to being notified of their condition allocation. In this way participants are blinded from condition during baseline assessment to prevent confounding influences upon the measures. Concerning participants’ randomized allocation to the LIFE group, a minimum of 66% attendance for each supervised/instructor led component of the intervention arm (including online where necessary) satisfies study adherence criteria. This level of attendance ensures a satisfactory level of engagement with the program while also accommodating unexpected scheduling conflicts, effectively promoting continued involvement and overall high retention rates without jeopardizing the integrity of the intended study outcomes.
LIFE condition
The LIFE arm of the program is a 12-week multimodal lifestyle intervention designed to reduce modifiable risk factors for dementia. The LIFE program integrates exercise, diet, mindfulness, and sleep components into a comprehensive, group-based intervention specifically targeted towards metabolic, inflammatory, and neurogenic biological pathways supportive of healthy brain aging. Additionally, these chosen lifestyle factors can be easily implemented and maintained by individuals in their own lives beyond the intervention period, promoting long-lasting positive impacts on lifestyle.
Exercise component. The exercise component consists of an aerobic, strength, and balance training program delivered by a qualified exercise physiologist. All sessions will be performed in a commercial fitness setting provided by Jetts Fitness Australia with qualified personal trainers for participant supervision and instruction. Participants will complete an introductory session with an exercise physiologist to assess current physical strength and fitness, educate participants on equipment use, safety, and gym etiquette, individualize the program as necessary and complete a supervised run-through of the exercise prescription.
Participants complete three 60-min exercise training sessions each week, including one supervised group training session with an exercise professional and two un-supervised individual sessions. Each session will include a 10-min warm-up, followed by 4–6 individually prescribed whole-body exercises performed at a moderate intensity in a circuit-based format with minimal rest (rating of perceived exertion, Borg Scale 10–15). Resistance weight, sets, and repetitions will be aimed at improving general functional fitness (strength, balance, and function) and will be set at approximately 40–60% repetition maximum, for 1–3 sets of 8–12 repetitions per exercise. Participants will then complete 10 minutes of cardiovascular exercise at a moderate to high intensity (bike, treadmill, rowing, stepping), and a 10-min cool-down.
Intensity will be individually prescribed in the initial session and will be regularly monitored and adjusted as needed by the exercise physiologist during the supervised sessions. Modifications to exercise intensity and program difficulty will be made in a progressive manner and will consider participant feedback, safety concerns, and recovery. The intervention is progressive and periodized to allow for recovery, adaptation, and minimize the risk ofinjury.
Diet component. The diet component is delivered by an accredited practicing dietitian in six face-to-face group counselling sessions (60 min per session) conducted every two weeks over the intervention period. Participants will receive training and guidance to increase adherence to a modified Mediterranean diet (ModiMed) modelled off the MedLey prescription [111], the Mediterranean diet pyramid [112], and concepts from the MIND diet [113]. Educational content covers one food group per session, with additional activities included to assist participants to identify strategies to incorporate dietary change. Participants are to be encouraged to create a Specific, Measurable, Achievable, Relevant, and Time-Bound (SMART) goal relating to the content covered and will also receive printed dietary advice each session.
Mindfulness component. The mindfulness component is delivered by an experienced mindfulness teacher utilizing a standardized mindfulness technique developed for use in longitudinal RCTs [114]. The mindfulness training will begin by using a mindful breathing task and will then slowly be expanded to include all activities of daily living. The instruction material for the mindfulness program is provided in Supplementary Material 3. The program will consist of six instructor-led group training sessions (90 min duration) conducted every two weeks over the intervention period. Sessions will focus upon the delivery of the mindfulness technique, group discussion, and guided practice. Participants will be asked to engage in daily home mindfulness practice beginning at 20 min/day and increasing to 30 min/day following completion of week 2 for the remainder of the program.
Sleep component. The sleep program focuses on optimizing sleep quality, quantity, and daytime functioning and will be delivered by an experienced registered psychologist with expertise in behavioral sleep medicine. The program consists of six face-to-face group sessions (60 min per session) conducted every two weeks over the intervention period. The content of the sessions will be informed by a transdiagnostic sleep intervention, developed to both treat sleep disorders and promote sleep health [115]. The following topics will be covered: education on sleep and circadian rhythms, including normal changes with age and sleep disorders; establishing regular sleep-wake times; improving sleep efficiency through stimulus control and reducing time in bed; and approaches for managing advanced or delayed sleep phases. There will also be content on unhelpful beliefs about sleep and sleep-related worry and vigilance, which will be integrated with learnings from the simultaneously delivered mindfulness sessions. Participants will be encouraged to set individual goals at the outset of the intervention, with barriers to experimenting with intervention strategies to achieve such explored and addressed in group discussions using motivational interviewingtechniques.
Control condition
Participants in the control arm receive a DRR outlining their individual dementia risk profile, thereby constituting a health-information only control group. While participants in the LIFE arm are assisted to reduce their identified modifiable risk factors through engagement with the multi-modal lifestyle intervention, participants in the control condition are not provided with additional intervention information, though they may choose to access their regular health and lifestyle providers to assist them in reducing the modifiable dementia risk factors identified in their DRR. At the completion of T2 assessments, participants in the control condition will be offered online access to resources providing general health advice, however they will not be offered specific material pertaining to the LIFE program, engagement in training sessions or an instructor-guided intervention. Given the considerable time commitment implicated in study involvement, we hope that providing control participants with general information supportive of healthy living will encourage sample retention at later timepoints.
Sample size considerations
A sample size estimate was calculated using G*Power (version 3.1.9.4), based on power estimates from previous multi-modal lifestyle interventions aimed at reducing risk of dementia in midlife and older adults [71]. To detect a small-medium effect (f = 0.22) in a two-group design across two timepoints (four measurements), with a 5% risk of a Type 1 error and 80% power, 104 participants will be required. To account for 10% attrition [71], a baseline sample of 115 participants will be recruited.
Risk management
All procedures and assessments included in the LEISURE study have been approved by the Human Research Ethics Committee of the University of the Sunshine Coast (UniSC), Australia (A191301). All study activities are to be conducted in accordance with the Australian National Statement on Ethical Conduct in Human Research (2007). The UniSC Human Research Ethics Committee reviews all study procedures annually to ensure continued safe operation of study activities. Written informed consent is obtained from all study participants prior to enrolment. Participants will not receive any direct reimbursement or remuneration for their participation in the LEISURE study, although participants may derive benefit from participating, as it enables access to a suite of clinically relevant assessments and lifestyle intervention programs that are often costly or associated with lengthy waiting periods in clinical and public health services. On 19 January 2020, the LEISURE study was also prospectively registered with Australian New Zealand Clinical Trials Registry (ACTRN12620000054910), an online register of clinical trials being undertaken in Australia and New Zealand.
Data management
Participants are informed that all information collected during the study will be treated as confidential and will be de-identified to protect privacy. On acceptance into the study, participants receive a LEISURE ID number, and all participant data collected will be coded with this number and will be de-identified thereafter.
Participants are free to withdraw at any point during their involvement with the study and are not obliged to provide a reason. Upon withdrawal, participants will be asked to specify if they (a) would like to withdraw consent for further participation, but consent to the continuing use of their de-identifiable data that has already been collected, or (b) would like to withdraw consent for further participation and wish for all their data collected and stored through their involvement in the study to be destroyed.
Participant electronic data is stored on secure UniSC network directories, as well as backed up on password protected hard disk drives stored in secure facilities at the Thompson Institute. Data will be kept for 15 years and then will be destroyed by electronic shredding of computer files and manual shredding of paper files.
Data analysis plan
In the first instance, independent group t tests will be performed to assess for baseline between-group differences in demographics variables (age, education) and dementia risk. Chi-square analysis will be used to assess between group differences in handedness as well as gender balance. To test the effect of the lifestyle program on dementia risk profiles, linear mixed-effect modeling, or mixed-model analysis of variation (ANOVA) of CogDrisk scores will be performed, with group (LIFE, control) as the between-subjects factor and time (T1, T2) as the within-subjects factor. Significant effects pre- to post-intervention will then be investigated using pairwise comparisons. To test the effect of the lifestyle program on secondary/exploratory measures, a repeated measures ANOVA will be performed, with group (LIFE, control) as the between-subjects factors and time (T1, T2, T3, T4) as the within-subjects’ factors. Multiple regression will also be performed to examine relationships between primary, secondary, and exploratory variables. Additionally, Pearson or Spearman correlation will be conducted to measure the degree of relationship between the results obtained from the primary and secondary measures. The robustness of the findings will be assessed using sensitivity analyses, including those investigating the impact of baseline differences between groups, impact of outliers, and impact of missing data. Following complete case analyses for all outcome measures, multiple imputation will be used to account for missing data in a full intention-to-treat analysis, where appropriate.
DISCUSSION
The LEISURE study is designed to assess the efficacy of a targeted multi-modal lifestyle intervention to reduce modifiable risk factors for dementia in healthy older adults. The lifestyle factors targeted in the LEISURE study have been determined in accordance with the 2020 Lancet Commission Report on dementia prevention [116], and in conjunction with an emerging body of research indicating that several types of dementia may result from chronic aberrant metabolic and inflammatory mechanisms, which contribute to neurodegenerative and vascular changes [7]. These signaling pathways may be targeted through a multi-modal lifestyle approach, integrating exercise, diet, mindfulness, and sleep interventions to modify multiple risk factors and mechanisms simultaneously. Based upon the burgeoning research suggesting dementia pathologies such as AD are increasingly considered as metabolic-inflammatory-vascular diseases [3], the approach adopted in the LEISURE study represents a robust approach to dementia riskreduction.
As the evidence of lifestyle contributions to dementia risk grows, there is an increasing need to understand the neurobiological and biomolecular pathways through which lifestyle interventions may support dementia risk reduction [9]. Previous attempts to investigate these multi-factorial processes have been limited due to the small number of outcome measures obtained, most of which have focused on cognitive outcomes via neuropsychological assessment alone, without evaluation of underlying biomarkers or mechanisms [6]. In the absence of comprehensive neuropsychological, neuroimaging, and biomarker measurement, interventions may not have the capacity to elucidate the complex interaction underlying lifestyle-induced neurophysiological changes that reduce risk of neurodegeneration and dementia.
The LEISURE study is one of few RCTs to include an expansive array of outcome measures to the investigation of dementia risk reduction in aging, which expands on currently running multimodal interventions throughout the world. This study is well designed to uncover new insights into healthy brain aging through the utilization of psychometric testing alongside cognitive and behavioral assessment (CANTAB, SART, Trail making test A/B, etc.), measurement of neurophysiological activity (using EEG), structural neuroimaging (to assess anatomical and perivascular changes), BOLD contrast imaging (to assess functional network dynamics and connectivity), diffusion weighted imaging (to assess white matter integrity, tractography and structural connectivity), and a suite of biomolecular markers of inflammation, cellular metabolism, and cardiometabolic health.
Furthermore, the novel combination of exercise, diet, mindfulness, and sleep lifestyle factors separates the LEISURE intervention from previous trials. Typically speaking, previous dementia prevention multimodal lifestyle trials have tended to target various diet and physical activity components, with or without cognitive stimulation. The inclusion of mindfulness and sleep components into this protocol will provide additional insight into the potential protective benefits of stress management and optimized glymphatic clearance, not to mention inflammatory and oxidative relief as well as neurotrophic benefits.
The LEISURE Study has several potential limitations. Firstly, outcome assessors are only partly blinded at follow-up, with some clinicians involved in the delivery of the intervention also assisting with the assessments. Secondly, whether participants dedicate any time and/or effort to address areas of weakness identified in their baseline DRR is not exclusively measured. Thirdly, specific measures of intervention adherence are lacking, with a minimum attendance criterion acting as the studies’ primary measure of fidelity. Fourthly, the potential impact of the COVID-19 pandemic on the ability to implement and maintain any suggested lifestyle changes is not actively captured.
In conclusion, by integrating four specifically chosen lifestyle behaviors capable of targeting the mixed etiology of dementia, the LEISURE study aims to elucidate the molecular and neurobiological mechanisms underlying improvements in cognition and reduced dementia risk in older adults following a multimodal intervention. This understanding will have potential application beyond the field of aging and dementia, as shared mechanisms could be targeted in the treatment of a wide range of attentional and psychological disorders.
Footnotes
ACKNOWLEDGMENTS
We acknowledge the contributions of additional LEISURE study team members: Tyrone Huckstepp, Alicia Campbell, Bernard Clarke, Shae Rendall, Charlie Roberts, Kayla Stefanidis, Ben Isbel, Lauren Den Ouden, Hannah Anderson, Liz van Biljon, Rory Fischer, Sam Manger, Mike Pegg, and Sarah Freeman.
FUNDING
The LEISURE Study is funded by a grant from the Wilson Foundation.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
There is no data to make available at this stage.