
Abstract
Background:
Hypertension and skeletal muscle decline are common findings in patients with Alzheimer’s disease (AD). Angiotensin-converting enzyme (ACE) inhibitors preserve skeletal muscle and physical capacity; however, the driving mechanisms are poorly understood.
Objective:
We investigated the effects of ACE inhibitors on the neuromuscular junction (NMJ) with relevance to skeletal muscle and physical capacity in AD patients and age-matched controls.
Methods:
We evaluated controls (n = 59) and three groups of AD patients, including normotensive (n = 51) and patients with hypertension taking ACE inhibitors (n = 53) or other anti-hypertensive medications (n = 49) at baseline and one year later. We measure plasma c-terminal agrin fragment-22 (CAF22) as a marker of NMJ degradation, handgrip strength (HGS), and Short Physical Performance Battery (SPPB) as markers of physical capacity.
Results:
At baseline AD patients demonstrated lower HGS and SPPB scores and higher CAF22 levels than controls, irrespective of the hypertension status (all p < 0.05). The use of ACE inhibitors was associated with higher HGS and relative maintenance of SPPB scores, gait speed, and plasma CAF22 levels. Conversely, other anti-hypertensive medications were associated with an unaltered HGS, reduced SPPB scores and elevated plasma CAF22 levels (both p < 0.05). We also found dynamic associations of CAF22 with HGS, gait speed, and SPPB in AD patients taking ACE inhibitors (all p < 0.05). These changes were associated with reduced oxidative stress in AD patients taking ACE inhibitors (p < 0.05).
Conclusion:
Altogether, ACE inhibitors are associated with higher HGS, preserved physical capacity, and the prevention of NMJ degradation in hypertensive AD patients.
Keywords
INTRODUCTION
Hypertension is a common finding in patients with advanced old age and an independent risk factor for developing Alzheimer’s disease (AD) [1]. Patients with AD are also more likely to develop an early and severe form of age-related muscle decline, termed sarcopenia [2]. Specifically, these patients exhibit muscle weakness, atrophy, and reduced gait speed, which can contribute to compromised physical capacity [2]. Sarcopenic patients are also more likely to have a functionally dependent lifestyle and risk of fall than the age-matched controls [3].
Sarcopenia has a multifactorial etiology, and it is possible that progressive denervation of skeletal muscle in AD patients contributes to sarcopenia [4]. We have recently shown that the disintegration of the neuromuscular junction (NMJ) contributes to sarcopenia phenotype and physical compromise in mouse models [5] and older adults [6]. We have also established the biomarker potential of plasma c-terminal agrin fragment-22 (CAF22), a breakdown product of neuronal agrin at the NMJ, in diagnosing sarcopenia and physical capacity [2]. Specifically, the patients with reduced handgrip strength (HGS) and functional dependency exhibit higher plasma levels of CAF22 than age-matched controls [6].
Many patients with AD also present with systemic hypertension, an independent risk factor for dementia [1]. Furthermore, long-term systemic hypertension may negatively affect skeletal muscle independent of cognitive decline [7]. Thus, treating hypertension in AD patients may be imperative in protecting skeletal muscle and restoring physical capacity. Among various anti-hypertensive medications, angiotensin-converting enzyme (ACE) inhibitors are protective against dementia and skeletal muscle decline [8, 9]. Several potential mechanisms may account for the protective effects of ACE inhibitors on skeletal muscle. For example, ACE inhibitors reduce skeletal muscle fibrosis and exhibit antioxidant and anti-inflammatory properties [10, 11]. In addition, ACE inhibitors also prevent motor neuron toxicity in cell culture models [12]. Together, these findings show that the ACE inhibitors may have protective effects at the interface between motor neurons and skeletal muscle at the NMJs.
It is well recognized that an increased oxidative stress and inflammation can trigger NMJs degradation [13, 14]. For example, an increase in the production of reactive oxygen species can disrupt NMJ structure and function. Similarly, chronic inflammation is associated with degradation of NMJs in patients with dystrophies [14]. In this context, plasma 8-isoprostanes and c-reactive proteins (CRP), the markers of oxidative stress and inflammation, respectively, may be relevant to investigating NMJs [2]. Patients with NMJ disruption also present with muscle damage, which results in the leakage of muscle-specific creatine kinase in blood [2]. Thus, the measurement of creatine kinase levels can provide a useful estimate of muscle atrophy in such patients [15].
To our knowledge, no study has investigated the potential effects of ACE inhibitors on NMJs and plasma CAF22 levels in AD patients. In addition, it is not known if the protective effects of ACE inhibitors on skeletal muscle and physical capacity are at least partly mediated by NMJ preservation. Lastly, the relevant antioxidant and anti-inflammatory roles of ACE inhibitors remain elusive.
We aimed to bridge these gaps in the literature by investigating the associations of plasma CAF22 with HGS and physical capacity in hypertensive AD patients taking ACE inhibitors. We hypothesized that the ACE inhibitors reduce and/or maintain plasma CAF22 levels, which result in a higher HGS and maintained physical capacity in AD patients. These effects are at least partly associated with mitigation of oxidative stress and inflammation in AD patients.
MATERIALS AND METHODS
Study design and participants
The study includes controls (age = 67 – 80 years; n = 59) and patients with AD (age = 69–84 years; n = 153) recruited at the Department of Neurology and Stroke Medicine, Rehman Medical Institute, Peshawar, Pakistan. All participants provided written informed consent. The diagnosis of AD was based on the Mini-Mental State Examination (MMSE) scores, as described previously by us [16]. The AD patients were further subdivided into normotensive (n = 51) patients and two subgroups of hypertensive patients receiving ACE inhibitors (n = 53) or other anti-hypertensive medications (n = 49). The ACE inhibitors used in the study were centrally-acting captopril and lisinopril [17]. The baseline data about physical capacity, body composition, and plasma biochemistry for AD patients were retrospectively collected from hospital records. The data from controls were collected at one time point only. The inclusion and exclusion criteria are described by us in detail elsewhere [2]. Briefly, patients with musculoskeletal disorders, joint diseases, recent major surgeries, and acute or chronic impairment of major organs were excluded. Control participants were matched for age and gender and were recruited from a large cohort described elsewhere [18]. Sarcopenia was diagnosed according to the revised criteria by the European Working Group on Sarcopenia in Older People, as reduced handgrip strength (HGS≤27 kg), reduced appendicular skeletal mass index (ASMI≤7 kg/m2), and reduced gait speed≤0.8 m/s [19, 20]. Ethics approval to conduct the study was obtained from the hospital ethics committee. This study was conducted under the declaration of Helsinki [21].
HGS and body composition
We used a digital handgrip dynamometer (CAMRY, South El Monte, CA, USA) to measure HGS, as described previously [18]. A bioelectrical impedance analysis scale (RENPHO, Dubai, UAE) was used to measure the body composition, including fat content, phase angle, appendicular skeletal muscle mass (ASM), and appendicular skeletal muscle mass index (ASMI), as described previously [18].
Measurement of physical capacity
The Short Physical Performance Battery (SPPB), including a 4-m walking test (4MWT), balance, and five times chair-stand (5-STS) tests, was used to measure the physical capacity. Each SPPB component had a score ranging from zero (worst performers) to four (best performers), and a cumulative score of three components was used to evaluate the generalized physical capacity [22]. Daily step count was measured with a smartwatch pedometer, and the mean values from the daily counts of the past four weeks were reported, as described elsewhere [23].
Measurement of circulating biomarkers
Blood samples were collected from the cubital veins between 0900 to 1000 hours with the participants on an overnight fast. We used appropriate anticoagulant tubes to collect blood, which was immediately centrifuged at 3000 rpm for 15-20 min to separate plasma, as previously described by us [24]. The plasma samples were transferred to a fresh tube and stored at -80°C for further use. We measured plasma CAF22 levels with an ELISA kit (NTCAF, ELISA, Neurotune, Schlieren-Zurich, Switzerland), as described previously [25]. We used ELISA kits to measure plasma CRP (R&D Systems, Minneapolis, MN, USA), 8-isoprostanes (Cayman Chemical, Ann Arbor, MI, USA), and creatine kinase, as described previously [23, 26].
Statistical analysis
All data are presented as mean and standard deviation after confirming the normal distribution using the D’Agostino-Pearson test. The analysis of variance with Tukey’s post-hoc test was used to compare groups. A regression analysis was used to measure the relationships of percent changes in plasma CAF22 with percent changes in HGS, SPPB, and plasma biochemical markers. A paired t-test was used to compare the changes in physical and biochemical parameters between the two time points. A p-value<0.05 was taken as statistically significant. Data were analyzed using GraphPad Prism 8 (Graphstats technologies private limited, Bangalore 560035, India).
RESULTS
Baseline characteristics of the participants
The basic characteristics of the study population are described in Table 1. At baseline, there were no differences in age, body mass index, ASM, and percentage fats among the groups. Conversely, all patients with AD had lower phase angles and higher plasma CAF22, CRP, 8-isoprostanes, and creatine kinase levels than controls (all p < 0.05). In addition, the proportion of sarcopenic patients was higher among AD patients than controls (Table 1).
Baseline characteristics of control and AD patients with different hypertensive and medication status. *p<0.05 versus controls using one-way analysis of variance, #p <0.05 versus baseline for the same group using paired t-test. Values are expressed as mean±SD (n = 49-59 per group). AD, Alzheimer’s disease; BMI, body mass index; ASM, appendicular skeletal mass; CAF22, c-terminal agrin fragment-22; CRP, c-reactive protein; ACE, angiotensin-converting enzymes
Anti-hypertensive medications and NMJ
At one year time-point, we found no alterations in plasma CAF22 levels in normotensive and hypertensive AD patients taking ACE inhibitors (Table 1). Conversely, hypertensive AD patients taking other anti-hypertensive medications exhibited a significant increase in CAF22 after one year (p < 0.05) (Table 1). We next investigated the plasma biomarkers relevant to NMJ damage in the study participants. There was a reduction in plasma CRP levels in normotensive and hypertensive AD patients taking other anti-hypertensive medications (both p < 0.05) (Table 1). However, such an effect was not found in AD patients taking ACE inhibitors. We also found a reduction in 8-isoprostanes in AD patients taking ACE inhibitors for one year (p < 0.05), which was not observed in the other two groups of AD patients (Table 1).
We next investigated the dynamic associations of plasma CAF22 with creatine kinase (Fig. 1A–C), CRP (Fig. 1D–F), and 8-isoprostanes (Fig. 1G–I) levels in AD patients (Fig. 1). Plasma CAF22 exhibited significant correlations with CK in patients on ACE inhibitors (r2 = 0.094, p = 0.032) (Fig. 1B) but not in normotensive patients (Fig. 1A) and patients taking other anti-hypertensive medications (Fig. 1C). Similarly, a significant correlation was found between plasma CAF22 and CRP in patients on ACE inhibitors (r2 = 0.139, p = 0.008) (Fig. 1E), but not in the other two groups of AD patients (Fig. 1D, F). We found a similar trend for the association between plasma CAF22 and 8-isoprostanes, which was significant in the patients taking ACE inhibitors (r2 = 0.262, p = 0.002) (Fig. 1H), but not in the normotensive (Fig. 1G) and hypertensive patients on other anti-hypertensive medications (Fig. 1I).

Linear regression analysis showing the associations of alterations in plasma CAF22 levels with alterations in plasma CK (A-C), CRP (B-F), and 8-isoprostane (G-H) levels in normotensive (A, D, and G) and hypertensive AD patients on ACE inhibitors (B, E, and G) and other anti-hypertensive (C, F, and I) medications during one year of the study period (n = 49 – 59 per group). CK, creatine kinase; CRP, c-reactive proteins; CAF22, c-terminal agrin fragment-22; ACE, angiotensin-converting enzymes; AD, Alzheimer’s disease.
Anti-hypertensive medications and physical capacity
We next investigated the associations of anti-hypertensive medications with physical capacity in AD patients. The use of ACE inhibitors was associated with higher HGS in hypertensive AD patients (p = 0.024) (Fig. 2A). However, there was no significant alteration in HGS in AD patients on other anti-hypertensive medications and normotensive AD patients (Fig. 2A). Normotensive AD patients exhibited a reduction in gait speed after one year, when compared to baseline (p = 0.0005) (Fig. 2B). Conversely, there was no change in gait speed in all hypertensive patients despite a trend toward a reduction in patients taking other anti-hypertensive medications (p = 0.098) (Fig. 2B). We found a reduction in SPPB in normotensive (p = 0.031) and hypertensive patients on other anti-hypertensive medications (p = 0.009) after one year, when compared to baseline (Fig. 2C). However, such a reduction was not observed in AD patients taking ACE inhibitors (p = 0.495) (Fig. 2C). Lastly, we did not observe a change in ASMI in any of the three groups of AD patients (Fig. 2D).
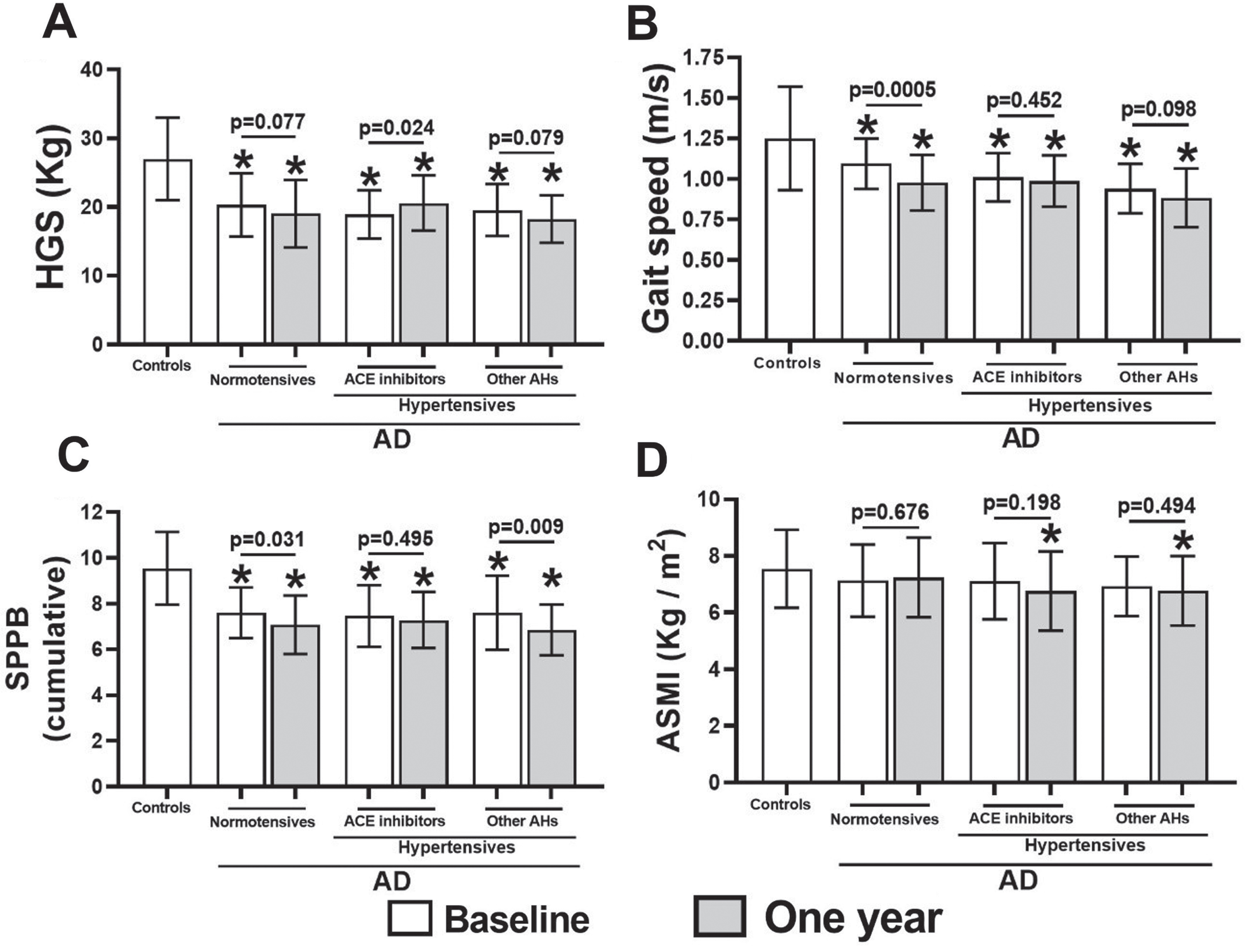
HGS (A), gait speed (B), cumulative SPPB scores (C), and ASMI (D) in control and AD patients with different hypertensive and medication status. *p<0.05 versus controls using one-way analysis of variance. p-values indicate paired t-tests (n = 49–59 per group). HGS, handgrip strength; SPPB, Short Physical Performance Battery; ASMI, appendicular skeletal mass index; AD, Alzheimer’s disease.
We next asked if the alterations in plasma CAF22 exhibit potential correlations with the alterations in HGS (Fig. 3A–C) and SPPB (Fig. 3D–F) in AD patients over the study duration of one year (Fig. 3). We found that CAF22 exhibited significant correlations with HGS in all three groups of AD patients, including normotensive (r2 = 0.086, p = 0.041) (Fig. 3A) and hypertensive patients receiving ACE inhibitors (r2 = 0.176, p = 0.022) (Fig. 3b) or other anti-hypertensive medications (r2 = 0.107, p = 0.024) (Fig. 3C). Conversely, CAF22 exhibited no significant correlation with SPPB in normotensive patients (Fig. 3D). However, hypertensive AD patients receiving ACE inhibitors (r2 = 0.125, p = 0.011) (Fig. 3E) or other anti-hypertensive medications (r2 = 0.089, p = 0.041) (Fig. 3F) exhibited significant correlations between CAF22 and SPPB.
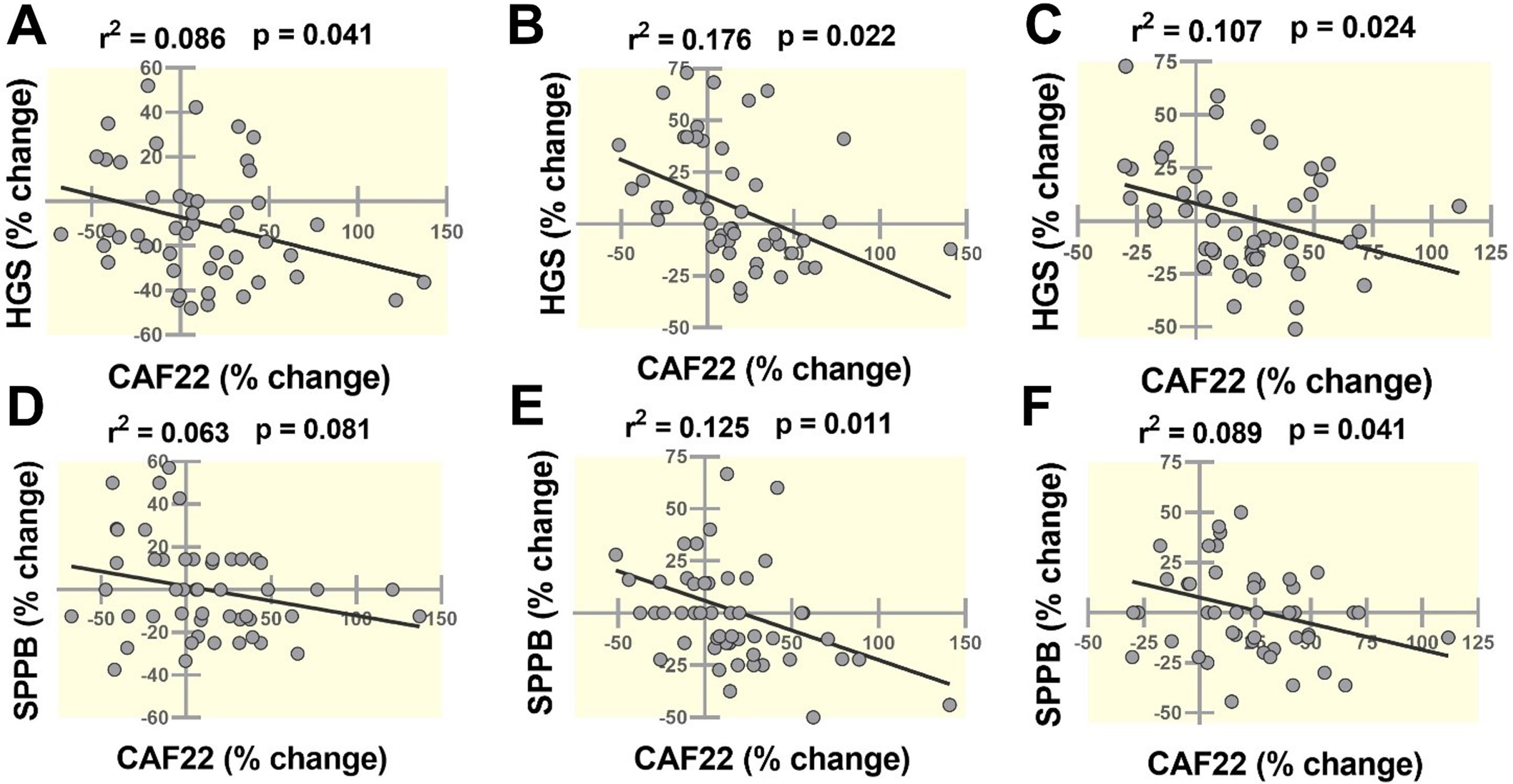
Linear regression analysis showing the associations of alterations in plasma CAF22 levels with alterations in HGS (A-C), and SPPB (D-F) in normotensive (A and D) and hypertensive AD patients on ACE inhibitors (B and E) and other anti-hypertensive (C and F) medications during one year of study period (n = 49–59 per group). HGS, handgrip strength; SPPB, Short Physical Performance Battery; CAF22, c-terminal agrin fragment-22; ACE, angiotensin-converting enzymes; AD, Alzheimer’s disease.
Correlations of plasma CAF22 with physical capacity and plasma biochemistry
Lastly, we investigated the associations of plasma CAF22 with HGS, SPPB, CK, CRP, and 8-isoprostane levels in controls and AD patients at individual time points (Table 2). HGS exhibited varying correlations with CAF22 in different cohorts, which was most robust in the patients receiving ACE inhibitors at baseline (r2 = 0.204, p < 0.05). These patients also exhibited a significant correlation between CAF22 and SPPB at baseline (r2 = 0.148, p < 0.05). Among plasma biomarkers, CK was most significantly associated with CAF22 in normotensive AD patients at baseline (r2 = 0.105, p < 0.05), while CRP was significantly associated with CAF22 in patients receiving ACE inhibitors at baseline (r2 = 0.184, p < 0.05). Lastly, 8-isoprostanes showed significant correlations with CAF22 in hypertensive AD patients, which was most robust in patients receiving ACE inhibitors at baseline (r2 = 0.299, p < 0.05) (Table 2).
Correlation coefficients of plasma CAF22 levels with MMSE, HGS, SPPB, CK, CRP, and 8-isoprostanes in control and AD patients with different hypertensive and medication status at individual time points, *p<0.05, (n = 49 – 59 / group). CAF22, c-terminal agrin fragment-22; HGS, handgrip strength; SPPB, Short Physical Performance Battery; ACE, angiotensin-converting enzymes; CK, creatine kinase; CRP, c-reactive proteins; AD, Alzheimer’s disease
DISCUSSION
We found reduced physical capacity and elevated plasma CAF22 levels in AD patients than in controls. However, the use of ACE inhibitors for one year was associated with no further elevation of plasma CAF22 and a significant improvement of HGS. Conversely, AD patients on other anti-hypertensive medications exhibited an elevation of plasma CAF22 levels with a trend toward reduction of HGS and gait speed. We also found a protective effect of ACE inhibitors against the decline in SPPB compared to other anti-hypertensive medications. These effects were partly mediated reduced systemic oxidative stress in patients taking ACE inhibitors.
Consistent with previous studies, we found reduced HGS, gait speed, and SPPB scores in AD patients than in controls [2]. Elevated plasma CAF22 levels in these patients indicate potential contributions of NMJ degradation to physical compromise. This finding is consistent with our previous reports and published literature [4, 18]. In addition, NMJ degradation is a critical contributor to muscle weakness and atrophy in basic [27] and clinical studies [18]. Thus, the reduced gait speed and SPPB in these patients can partly be due to muscle decline following NMJ degradation.
We found an improvement in HGS in patients taking ACE inhibitors. However, we did not find similar effects of other anti-hypertensive medications on HGS in AD patients. The protective effects of ACE inhibitors on skeletal muscle have previously been reported [10]. For example, ACE inhibitors prevent skeletal muscle atrophy and weakness and reduce age-related physical decline [28, 29]. However, the exact mechanisms driving these functions remain poorly known. Our study indicates that the potential preservation of NMJs may have a mechanistic role in the protective effects of ACE inhibitors on skeletal muscle. Several pieces of indirect evidence support this novel finding. First, ACE inhibitors prevent motor neuron decline in patients with amyotrophic lateral sclerosis [30]. Motor neuron loss is a critical trigger of NMJ degradation; hence, the protective effects of ACE inhibitors against motor neurons may preserve NMJs in AD patients. Second, we found a reduction in plasma 8-isoprostanes levels in patients taking ACE inhibitors. Oxidative stress can initiate and/or exacerbate NMJ degradation in experimental animal models [5]. In addition, clinical studies also indicate a robust association between elevated oxidative stress and NMJ degradation [31]. Thus, it is possible that the higher HGS and preserved NMJs in patients taking ACE inhibitors are partly due to a reduction in oxidative stress. This conclusion is strengthened by our finding of the dynamic association between SPPB and HGS in AD patients taking ACE inhibitors. Third, the cell culture models exhibit that the ACE inhibitors prevent the neurotoxicity of spinal motor neurons [12], which may have protective effects on NMJs. Together, these findings support the relative maintenance of CAF22 and associated preservation of physical capacity in AD patients taking ACE inhibitors.
All AD patients exhibited higher plasma CK, CRP, and 8-isoprostanes levels than controls. However, the patients taking ACE inhibitors had reduced 8-isoprostanes after one year, which was not observed in other AD patients. This finding is consistent with the antioxidant properties of ACE inhibitors [11]. Specifically, ACE inhibitors reduce the production of superoxides associated with the activation of the renin-angiotensin system. The increased oxidative stress has several detrimental effects on skeletal muscle, including muscle weakness and atrophy [32]. In addition, our previous studies indicate that patients with increased oxidative stress exhibit lower physical capacity, including SPPB scores and gait speed [33, 34]. Thus, the antioxidant effects of ACE inhibitors may partly account for increased HGS and preserved physical capacity in AD patients.
The correlation analysis was conducted to investigate the potential contributions of NMJs degradation to physical compromise, systemic inflammation, and oxidative stress. We found significant correlations of plasma CAF22 with HGS and SPPB scores in patients taking ACE inhibitors, indicating the NMJ degradation may have contributed to reduced HGS and physical compromise in these patients. These patients also exhibited modest correlations of plasma CAF22 with CRP and 8-isoprostanes levels, indicating the vulnerability of NMJs to inflammation and oxidative stress.
We did not find additional physical compromise due to hypertension in AD patients. Specifically, the HGS and SPPB scores were similar among normotensive and hypertensive AD patients. However, hypertension was controlled with medications, which may have reduced its detrimental effects on skeletal muscle. Conversely, patients with uncontrolled hypertension and associated sympathetic overdrive exhibit accelerated loss of muscle mass and strength [7].
This study has several major strengths. The single-center design reduces the potential variations due to different clinical and experimental settings. All patients had relatively similar cultural, racial, and ethnic profiles. The measurement of plasma CAF22 levels requires a simple ELISA plate reader and 10-15μl of plasma, which are available in most clinical settings. Plasma samples can be taken from the blood obtained for routine clinical investigations. The measurement of HGS does not require significant expertise and can be performed with a hand-held dynamometer. This study has certain limitations. We did not investigate the non-ambulant patients. However, plasma CAF22 may be a useful assessment tool of physical capacity in these patients since NMJ is susceptible to inactivity-induced degradation. The study only includes men. We did not measure the muscle strengths of the quadriceps, which may be more relevant to the activities of daily living. We did not directly investigate the NMJs morphology since muscle biopsies were not taken in this study. Finally, we did not dissect the potential effects of individual ACE inhibitors on physical capacity and NMJs.
Collectively, we found higher HGS, preserved physical capacity, and a relative maintenance of plasma CAF22 in AD patients taking ACE inhibitors. These findings indicate a potential preservative effect of ACE inhibitors on NMJs, which may contribute to higher HGS and maintained physical capacity. Future studies should take a mechanistic approach in further dissecting the effects of ACE inhibitors on NMJs and skeletal muscle.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This work was supported by the Deanship of Scientific Research at King Khalid University, Abha, Saudi Arabia, through Small Groups Project under grant number (RGP.1/191/43).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.