
Abstract
Background:
Western studies indicate potential associations between hippocampal volume and memory in the trajectory of Alzheimer’s disease (AD). However, limited availability of neuroimaging technology and neuropsychological tests appropriate for sub-Saharan African (SSA) countries makes it difficult to establish neuroanatomical associations of hippocampus and memory in this locale.
Objective:
This study examined hippocampal volumes and memory in healthy control (HC) and probable AD groups in the Democratic Republic of Congo (DRC).
Methods:
Forty-six subjects with probable AD and 29 HC subjects were screened using the Community Instrument for Dementia and the Alzheimer Questionnaire. Participants underwent neuroimaging in Kinshasa, DRC, and memory was evaluated using the African Neuropsychology Battery (ANB). Multiple linear regression was used to determine associations between hippocampal volumes and memory.
Results:
Patients with probable AD performed significantly worse than HCs on ANB memory measures, and exhibited greater cerebral atrophy, which was significantly pronounced in the medial temporal lobe region (hippocampus, entorhinal cortex). Both AD and HC subjects exhibited high rates of white matter hyperintensities compared to international base rate prevalence, which was significantly worse for probable AD. Both also exhibited elevated rates of microhemorrhages. Regression analysis demonstrated a significant association between hippocampal volume and ANB memory tests. Hippocampal atrophy discriminated probable AD from the HC group.
Conclusions:
This study establishes the feasibility of conducting neuroimaging research in the SSA, demonstrates many known neuroimaging findings in probable AD patients hold up using culturally appropriate memory tasks, and suggest cardiovascular problems are a greater issue in SSA than in Western countries.
Keywords
INTRODUCTION
There are an estimated 2.1 million individuals with dementia in countries in sub-Saharan Africa (SSA), and it is projected that this number will triple by the year 2040 [1]. Despite these projections, persons from SSA are rarely included in studies of Alzheimer’s disease (AD), researchers and clinicians lack neuropsychological tests appropriate for SSA populations, and diagnostic protocols and neuropathological correlative studies in African populations are virtually nonexistent. In the current study, we sought to establish the feasibility of conducting such research in SSA, and to determine if test results of the recently developed African Neuropsychological Battery (ANB) [2] would conform or differ from typical results observed in the non-African world in relation to neuroimaging findings.
Most medical guidelines recommend that all subjects with cognitive decline undergo structural magnetic resonance imaging (MRI) as part of the proposed diagnostic criteria for AD and for other dementias [3]. MRI measures of cerebral atrophy have been shown to have strong correlation with cognitive decline when compared with other imaging biomarkers [4]. Major findings of structural MRI in AD patients have included gray matter atrophy beginning in the entorhinal cortex, followed by medial temporal lobe (TL) regions (hippocampus, amygdala, parahippocampus, and posterior cingulate), and progressing to the temporal neocortex, parietal cortex, and frontal cortex [5, 6]. Medial temporal lobe atrophy (MTLA) on structural MRI is considered to be an important biomarker and predictor of disease progression with sensitivity and specificity of ∼50–70% for distinguishing prodromal AD at pre-dementia stage and non-AD degenerative diseases (e.g., dementia with Lewy bodies, vascular dementia, frontotemporal dementia) [6].
These findings have had little impact on clinical care or research in the less economically developed countries of SSA [7]. Decades of research on AD from overwhelmingly Western countries have established hippocampal atrophy as a characteristic finding in the condition [8], with the degree of atrophy correlating with the severity of the dementia, as well as neuropathology at autopsy [9]. Hippocampal volume positively correlates with learning and memory performance on visuospatial and verbal memory tasks in individuals with amnestic mild cognitive impairment (MCI) and different stages of AD [10–13]. Further, longitudinal studies have implicated hippocampal atrophy, MTLA, and entorhinal atrophy as factors that predict the progression from MCI to AD [14–16]. Together, these studies support the role of the hippocampus as a possible biomarker that can improve the diagnostic precision with respect to the presence of AD although there are some studies that suggest that hippocampal atrophy lacks specificity in distinguishing AD from other neurodegenerative conditions, particularly in early stages [17].
It is important to note that these studies were conducted primarily in individuals from Western and developed nations, which limits the generalizability of these findings. We are starting to appreciate that cognitive aging, risk factors, clinical course, and neuropathological features of AD can differ as a function of race, and ethnicity, and genetic composition [18]. Moreover, it is possible that different geographic regions will vary with regards to environmental (e.g., inadequate food resources) and social risk factors (e.g., limited educational opportunities, smoking, obesity), and the prevalence and type of comorbid conditions (e.g., vascular conditions, malnutrition) [19–22]. Therefore, it is important to extend this research to more diverse populations, including in SSA. Although most guidelines recommend that all subjects with cognitive decline undergo structural MRI as part of diagnostic workup for AD and for other dementias [23], the limited availability of neuroimaging technologies and scanners in developing countries has made it difficult to establish the neuroanatomical profile of AD in SSA.
Another barrier in the investigation of neuroanatomical correlates of AD in SSA has been the lack of culturally appropriate neuropsychological tests for SSA [24]. Prior attempts at assessment in SSA have primarily used translated Western tests with little attention to cultural appropriateness, which led to anomalous situations where test items were employed that are unknown in Africa (e.g., fruits, vegetables, and animals not commonly found on the continent). To address these confounds, the ANB provides a linguistically appropriate neuropsychological test battery to assess cognitive function across the adult lifespan in SSA. The ANB assesses attention, perceptual and motor abilities, language, memory, and executive function using tasks and stimuli familiar to persons in SSA countries, with versions of the battery available in both colonial (English and French) and traditional (Lingala, Kikongo, Tshiluba, and Swahili) languages [25].
We sought to explore the relationship between memory performance assessed with the ANB and MRI volumetric analysis. We hypothesized that hippocampal volumes would be lower in patients with presumed AD compared to healthy age-, education-, and gender-matched controls. We also hypothesized that the volume of the hippocampus would correlate positively with performance on memory tests of the ANB, and that the presence of white matter lesions and microhemorrhages would be higher in patients with AD than control subjects, and also independently contribute to restrictions in memory performance. Establishing some of these core neuroimaging and neuropsychological findings in a cohort of subjects with probable AD from the Democratic Republic of Congo (DRC) will represent an important first step towards establishing the use of these neurodiagnostic tools in a country where they have been critically lacking.
MATERIALS AND METHODS
Participants
Participants were healthy matched elderly subjects and subjects with probable dementia recruited from churches, clinics, hospitals, older adult associations and gatherings, and door-to-door. Subjects were screened with Community Screening Instrument for Dementia (CSID) and Alzheimer’s Questionnaire (AQ). Subjects were classified as having possible AD dementia or normal cognitive aging based on test criteria (defined below under test descriptions). Those who were screened and diagnosed with major neurocognitive disorder underwent cognitive evaluation (List Memory Test), completed a clinical interview and questionnaires (Geriatric Depression Scale for depression, hypertension, weight, and height), and other psychiatric and neurological evaluations to determine the etiology of their cognitive deficits. Evaluations were completed by trained psychologists of our team at our memory clinic. An expert panel [neurologist (EP), psychiatrist (GG), and neuropsychologist (JI)] utilized all clinical data to classify the participants as having possible AD dementia or other cognitive status.
Participants needed 1) to be age 50 or older 2) have a family member or close friend to serve as a collateral informant or care partner, 3) to have no current or past history of neurodevelopmental, mental disability, or other neurodegenerative diagnosis other than AD, 4) no current diagnosis of significant psychiatric pathology (e.g., schizophrenia), 5) no contraindications for MRI scan (metal in the body, claustrophobia, pregnancy); 6) adequate sensory perceptual skills to be able to see and draw, and 7) able to give informed consent. All procedures were done in accord with the Declaration of Helsinki. The study was approved by the Ethics Committee of the University of Kinshasa and Institutional Review Board of Emory University.
Screening measures for probable dementia
Community Screening Instrument for Dementia (CSID) [3]: Participants were screened using the CSID. The CSID has been extensively used in many international dementia studies and has been shown to be a sensitive instrument for screening dementia [4, 26]. The CSID consists of cognitive assessment interviews with the subject and with the informant or caregiver. The cognitive assessment is based on the following domains: orientation (place and time), attention and calculation, language (naming and fluency), constructional apraxia, learning and memory (3 trials of 10 words each and a delayed recall trial). The CSID has been used in two central African capitals for prevalence of dementia and the score of 18.6 was the cutoff for probable dementia and of 28.4 for normal cognitive aging [4].
Alzheimer’s Questionnaire (AQ): Caregivers evaluated cognitive and functional abilities of care recipients using the AQ, which is an informant or caregiver-based screening instrument [26–28]. AQ evaluates five domains which includes memory, orientation, functional ability, visuospatial skills, and language functions of the participants. Based on previous literature [3, 26], participants were assigned to the probable dementia group with an AQ score of 13 or higher and normal cognition with a score of less than 13. The AQ has sensitivity of 98.55 and specificity of 96 for AD [28] and has not yet been tested in this cohort.
Neuropsychiatric measure
Geriatric Depression Scale (GDS): Participants were evaluated with the 15-item GDS for symptoms of depression. GDS is a self-report questionnaire used to evaluate depression in older adults. Total scores range from 0 to 15, with higher scores indicating greater levels of depressive symptoms. A cutoff score >5 suggests the presence of depression [29]. The GDS has an α coefficient of 0.745 [30] and has not yet been tested in this cohort.
Cognitive measures
Learning And Memory: Participants were also tested with the ANB for learning and memory. For the current study, two memory tests (one verbal and one visuospatial) of the ANB were included. These learning and memory measures included the African List Memory Test (ALMT) and the African Visuospatial Memory Test (AVMT). Each memory measure consists of 3 learning trials, an interference trial, a short delay recall, a 20-min long-delay recall trial, and a recognition trial. The ALMT scores range from 0–12 in each trial. AVMT score ranges between 0 to 20 points in each trial. Psychometrically, the ALMT and AVMT have good test-retest reliability. Intraclass correlation stability coefficients have been found to be 0.80 and 0.53 [25].
Neuroimaging
All subjects were imaged on a 1.5 Tesla MRI unit (Siemens, Magneton Sonata) scanner at HJ Hospitals in Kinshasa using the same standardized imaging acquisition protocol based on the Alzheimer’s Disease Research Center (ADRC) protocol of Emory University. This consisted of sagittal volumetric T1-weighted, (MPRAGE), coronal T2-weighted, and axial diffusion-weighted, T2-weighted, and T2-FLAIR sequences. Typical acquisition parameters for the MPRAGE sequence were TR = 2200 ms, minimum full TE, TI = 1000 ms, flip angle = 8°, FOV = 25 cm, with a 192×184 acquisition matrix, yielding a voxel size of approximately 1.25×1.25×1.2 mm.
Images were reviewed by a subspecialty certified neuroradiologist (AMS) with 14 years of experience. White matter hyperintensity was graded according to the age-related white matter changes (ARWMC) scale [31]. Number of chronic brain parenchymal microhemorrhages were recorded. Lobar volume loss pattern of the brain was assessed. MPRAGE images were reoriented into the oblique coronal plane orthogonal to the principal axis of the hippocampal formation, and MTLA [32] and entorhinal cortex atrophy (EriCa) [33] scores were assessed. Finally, the presence or absence of any additional abnormalities was noted, and patients were excluded if neuroimaging evidence indicated an etiology other than probable AD (e.g., presence of a braintumor).
Quantitative volumetric analysis using Freesurfer
The 3D T1w images were segmented using Freesurfer (v.6, MGH, MA), which includes a full processing stream for MR imaging data that involves skull-stripping, bias field correction, registration, and anatomical segmentation as well as cortical surface reconstruction, registration, and parcellation. Regional brain volume for both cortical and subcortical brain regions were calculated. The left and right hippocampal volume were averaged. Interindividual variation in head size were accounted for in further statistical analysis by controlling for the effects of the total intracranial volume. Brain segmentation was performed by experts at Emory University who routinely perform this methodology for related studies, including a large FDA clinical trial involving epilepsy surgery (Stereotactic Laser Amygdalophippocampotomy in Temporal Lobe Epilepsy: SLATE trial, Medtronic, Inc.). Quality checks were performed on each case to ensure that automated processes were resulting in reasonable data.
Procedure
Participants were administered the dementia screening measures to assign them to the group of those with probable dementia as based on their CSID score. Patients with scores in the range of mild cognitive impairment [MCI] (i.e., CSID score ranged from >18 to <28 and AQ <13) were excluded from the current study. The exclusion of this cohort was based our desire to start with findings related to AD, cognition, and neuroimaging that are well-established in the Western world. Availability of funding did not make it possible to consider three subgroups and given the novelty of both the test battery and the use of neuroimaging in SSA, we felt the most productive approach would be to ensure that known findings can be replicated under these conditions. The possible HCs had to produce a normal score on all screening measures. Informed consent was obtained from participants meeting study participation criteria. Participants were administered questionnaires and the ANB and underwent clinical interview to gather demographic and disease-related variables during a single session lasting 2.5–3 h. After completing neuropsychological tests, participants underwent the MRI scan at HJ Hospitals the following day. While performance on the CSID and the AQ were used to classify participants as normal cognitive aging or probable dementia, the ANB scores were used to test the association between cognitive performance and neuroimaging. Participants were provided with a stipend for completing the psychometric measures and MRI scan to offset the time they invested in the study.
Statistical analysis and power analysis
Data were analyzed at Emory University using SAS statistical software. Statistical analyses included: 1) calculation of descriptive statistics (mean, median, standard deviation, range) for each group. Scores on the delayed recall trials of the AVMT and ALMT were used as measures of visuospatial memory and verbal memory, respectively. Total memory scores were also calculated by combining verbal and visuospatial memory performance of free delayed recall trial scores.
We standardized the hippocampus volume as follows: standardized hippocampal volume = (hippo-campal volume – means of the full group)/(standard deviation from the whole group). We obtained standard deviation units (SDU) for the hippocampal volume. Standardized hippocampal volumes were obtained for left, right, and total hippocampal volume. Total hippocampal volume was calculated adding left hippocampal and right hippocampal volume. We also used chi square to determine whether or not there were significant difference between the frequency of clinical MRI abnormalities of probable AD and HC subjects.
2) Linear regressions models were used to estimate differences between diagnostic groups in age, gender, year of education, and standardized hippocampal volume. We also conducted linear regression models to examine the association of ANB memory scores with standardized hippocampal volumes controlling for age, education, gender, GDS score, and intracranial volume. Our model was as follows: Y =β0 + β1X1 + β2X2 + β3X3 + β4X4 + β5X5 + β6X6 where Y = memory score, X1 = standardized hippocampal volume, X2 = age, X3 = sex, X4 = education, X5 = GDS score, X6 = intracranial volume (only for brain volume m, and β1 = true slope associated with standardized hippocampal volume, adjusted for X2, X3, X4, X5, X6.
To determine if there was an association between memory and standardized hippocampal volumes, we performed the following analyses: 1) verbal memory with either left, right or total standardized hippocampal volume; 2) visuospatial memory with either left, right or total standardized hippocampal volume; and 3) total memory with either left, right or total standardized hippocampal volume. To determine the diagnostic accuracy, receiver operating characteristic (ROC) analysis were used to calculate areas under curve (AUCs) for the comparisons of probable AD versus HCs. Logistic regression analyses were used to explore the relative contribution of neuroimaging and cognitive variables for identifying dementia after adjusting for age, education, GDS score, and gender. As prior studies have found depression to be correlated independently with both cognitive performance and hippocampal volume [34, 35], we decided to control for depression symptomatology using available GDS scores.
To correct for multiple testing, the Benjamini-Hochberg procedure with a false discovery rate (FDR) of 0.1 was applied. The p values were ordered and the Benjamini-Hochberg critical value for each test was calculated. The test with the largest p-value that is less than its Benjamini-Hochberg critical value and all tests with a smaller p value were considered significant. The tests that were considered significant after FDR adjustment were highlighted.
A power analysis was conducted based on data from previous studies [36]. Assuming a pooled standard deviation of 0.06, our study required a sample size of 23 for each group (i.e., a total sample size of 46, assuming equal group sizes), to achieve a power of 80% and a level of significance of 5% (two sided), for detecting a true difference in means between the test and the reference group of – 0.0499 (i.e., 0.26–0.31).
RESULTS
Descriptive data
We screened 1,432 potential subjects in the DRC between 2019 and 2022, which resulted in 114 individuals who were eligible to serve as either patients with probable AD or HCs. After completing the diagnostic tests used for classification, we ended up with 59 patients with probable AD and 55 HCs. Of these 114 potential subjects, 80 of these individuals agreed to undergo MRI scans. Seventy-seven total participants completed neuroimaging. Two participants were excluded due to abnormal clinical findings (right subdural hematoma with midline shift and a pituitary macroadenoma), resulting in 75 participants in total (probable AD [n = 46] and HCs [n = 29], combined). Our total sample was 52% female (18 were HC and 21 with probable AD), 40% male (11 were HC and 25 with probable AD). The sample averaged 72.5 years of age (SD = 8.4 years) and there was no statistical difference in age between HC and the probable AD groups. The HC group had more years of education (x = 10.7 years, SD = 5.2 years) than the group with probable AD (x = 8.0 years, SD = 5.3 years). From a psychiatric standpoint, the group with probable AD [8.67, SD (3.72)] had significantly higher depression symptom scores than the HC group [4.71, SD (2.410], p < 0.0001]. Cognitively, the HC group performed significantly better than the probable AD group in both verbal and visual modalities of learning and memory (see Table 1). Significant negative correlations of a moderate effects size were observed between GDS score and various memory scores (p < 0.0001). In contrast, there was not a significant correlation between GDS scores and hippocampal volumetric values in our sample.
Demographic data, neuropsychological results, and MRI brain variables presented for the probable AD and healthy control subgroups
AD, Alzheimer’s disease; SD, standard deviation; ALMT, African List Memory Test; AVMT, African Visuospatial Memory Test.
Hippocampal volumes are reported in Table 1. These results showed statistically significant differences in hippocampal volumes between HC and probable AD groups. The probable AD subjects had smaller hippocampal volumes (left, right and total) than HCs (Fig. 1).
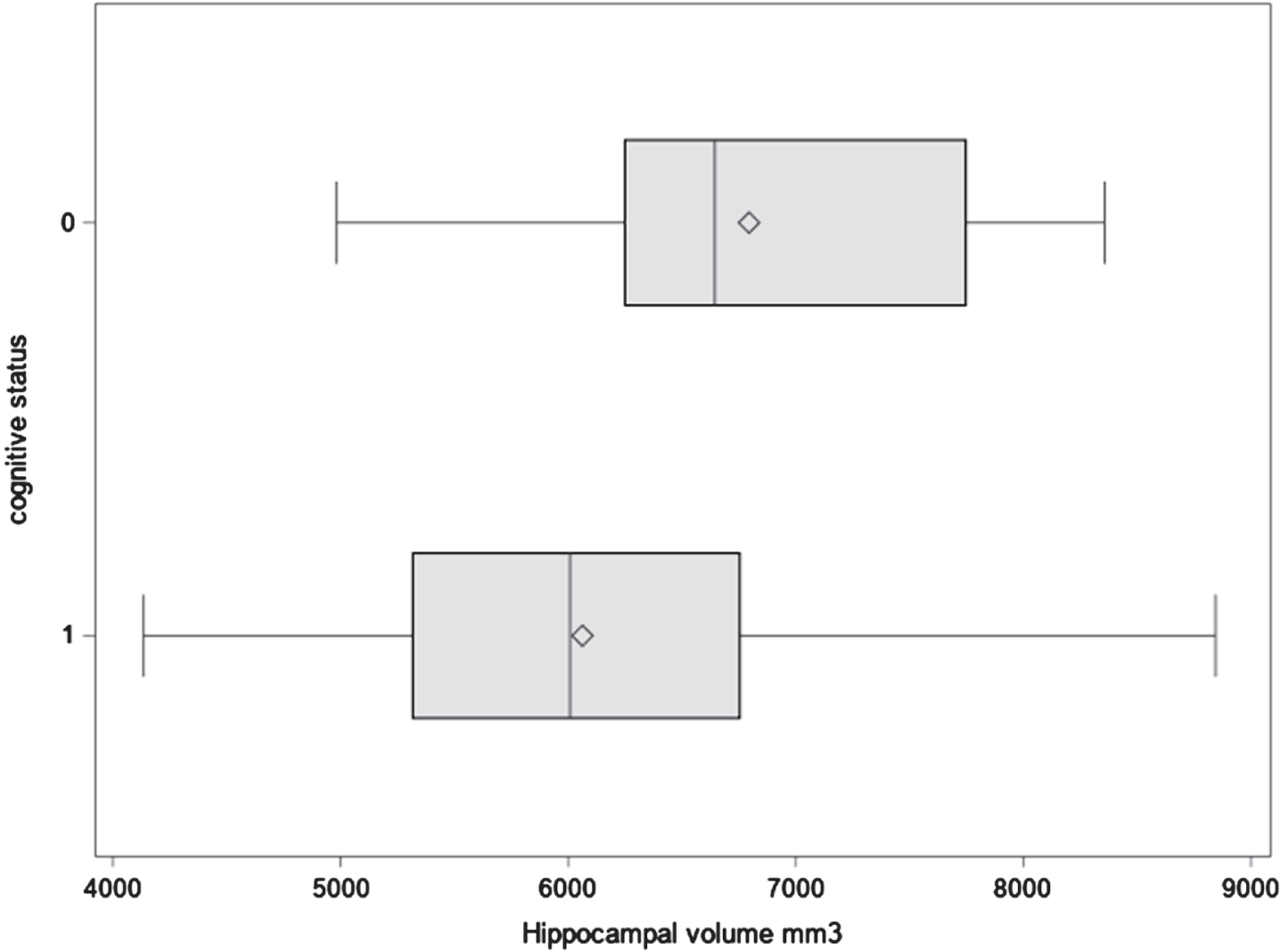
Scatter plot showing difference in mean between control (0) and probable AD (1) groups.
The clinical assessments of subjects’ MRI scans are presented in Table 2, and MRI scans demonstrating various neuropathological findings are presented in Fig. 2. Comparing the two groups with respect to evidence of atrophy, the probable AD subgroup exhibited a much greater prevalence of generalized volume loss, EriCa, and MTLA than the HCs. These significant differences were particularly notable for the medial TL regions (i.e., EriCa and MTLA). While white matter hyperintensities were much worse for probable AD subgroup, the HCs had an extremely high rate of these abnormalities as well. There was no significant difference in prevalence of microhemorrhages between the subgroups, with each group (particularly the HCs) exhibiting rather elevated rates of such findings compared to international base rates (e.g., 3–6% of healthy older adults typically have evidence of microhemorrhages; approximately 23% of AD patients) [37–39].
Prevalence and types of clinical abnormalities observed on MRI
WMH, white matter hyperintensity; ERICA, entorhinal cortex atrophy score; MTA, Mesial temporal lobe atrophy. Chi-square was conducted to determine the difference the control and probable AD group.
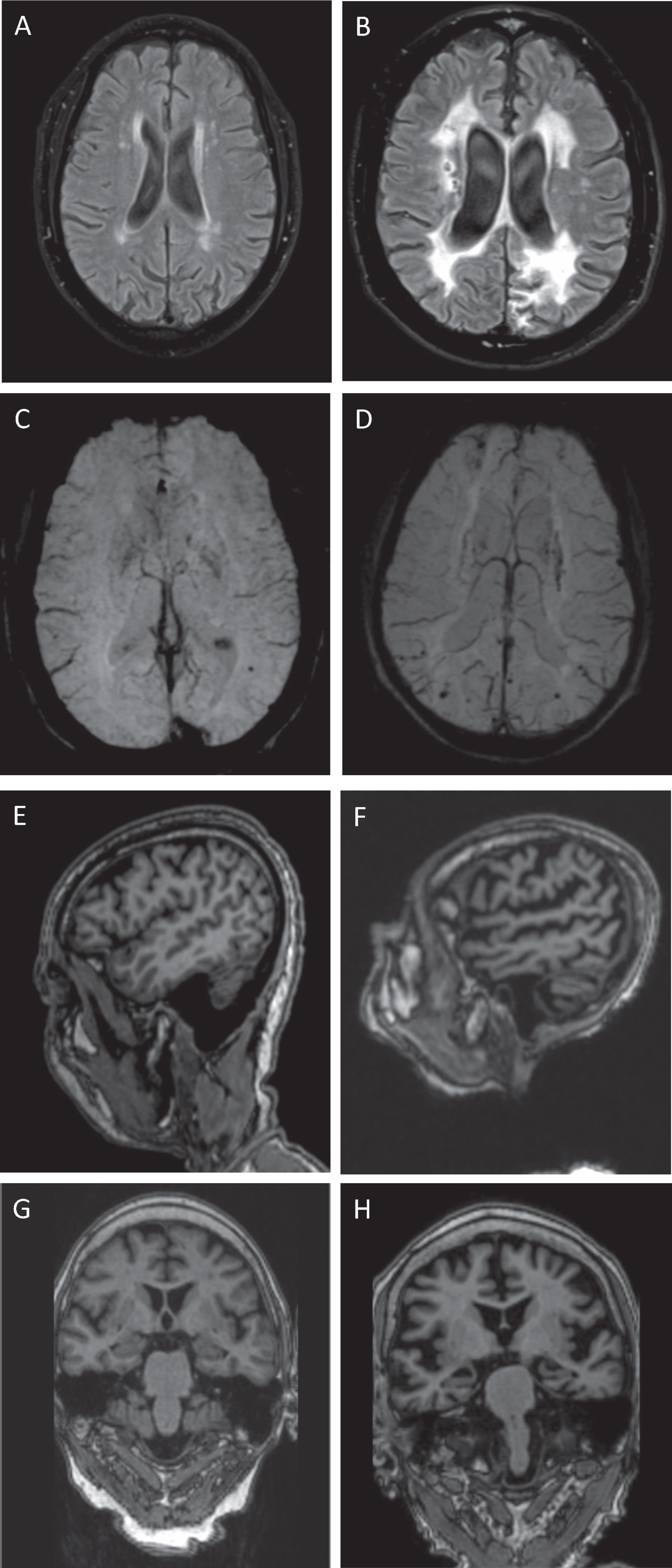
MRI scans demonstrating various neuropathological findings. We present sample MRI scans demonstrating various neuropathological findings as described: A) axial T2-FLAIR of a control participant with age-related white matter changes (mild white matter hyperintensity); B) axial T2-FLAIR of a participant with probable AD with confluent periventricular and deep white matter hyperintensity (severe); C) axial SWI of a control with a single left parietal lobe chronic microhemorrhage; D) axial SWI of a participant with probable AD with multiple punctate chronic microhemorrhages within the bilateral parietal lobes; E) sagittal T1 MPRAGE of a control participant with normal appearance of brain volume; F) sagittal T1 MPRAGE of a participant with probable AD with atrophy involving the temporal and parietal lobes; G) oblique coronal T1 reformat from T1 MPRAGE from a control with normal appearance of mesial temporal lobe structures (MTA 0 and ERICA 0); H) oblique coronal T1 reformat from T1 MPRAGE from a participant with probable AD with atrophy of mesial temporal lobe structures (MTA 3 and ERICA 3).
We also used linear regression models to examine the association of ANB memory scores with standardized hippocampal volumes controlling for age, education, gender, mood, and intracranial volume (see Table 3). Verbal memory scores were not significantly associated with standardized hippocampal volumes when controlling for mood (which accounted for more of the variance in performance than neuroimaging metrics for this variable). In contrast, visuospatial and total memory scores were significantly associated with standardized hippocampal volumes (i.e., left, right, and total hippocampal volumes) with the exception of visuospatial memory score and left hippocampal volume. Total hippocampal volume was the most strongly correlated with total memory by approximatively 2.00 SDU (CI 0.39–3.61), while right hippocampal volume had weakest, non-significant association with verbal memory with a coefficient of 0.57 SDU (CI –0.17–1.31).
Association between memory and standardized hippocampal volume
These results reflect our findings from linear regression analyses, which controlled for age, education, gender, total intracranial volume, and mood (based on the Geriatric Depression Scale). All results with the superscript symbol (‡) remained significant after correction for multiple comparisons (See text for a description of the Benjamini-Hochberg correction procedure).
The HC and probable AD groups were fairly well discriminated by hippocampal volume at 0.88 (Fig. 3). For every standard deviation unit increase in total hippocampal volume, there was a 57% reduction in the odds of dementia (OR = 0. 43).

ROC total hippocampal volume.
DISCUSSION
In the current study, we examined associations between hippocampal volumes and memory performance in a sample of elderly Congolese adults with or without probable AD from Kinshasa, Democratic Republic of the Congo, using newly culturally validated memory measures from the ANB and MRI. Within this context, this study was first a study of feasibility, as a recent report from an expert panel has documented a variety of barriers to neuroimaging access in SSA [40]. We demonstrated that published findings from primarily Western patient populations held up in SSA. More specifically, relationships between structural volumetric changes in the brains of patients with probable AD (e.g., hippocampal volumes) were predictive of worse memory performance scores. Moreover, just as in other parts of the world, these structure-function associations were affected by the presence of depressive symptomatology. We also found an elevated rate of chronic microhemorrhages and white matter hyperintensity in both our patients with probable AD and our HC sample, which seemed surprisingly high for the latter group, and appears consistent with reports that cardiovascular disease represents a significant problem for developing countries in Africa. Finally, we further established the use of the ANB [2], a battery of neuropsychological tests created for Africa, as a potential clinical diagnostic and research tool in the SSA [41, 42].
Establishing neuroimaging diagnostic parameters in a SSA cohort of patients with AD
This first sample of patients with AD and HCs to undergo scanning in the DRC for research purposes demonstrated several expected findings with respect to basic volumetric change in the medial TLs and overall cortex associated with probable AD. This included patients with probable AD exhibiting significantly smaller hippocampi than the HC subjects, including both unilateral and total volumes. Likewise, patients with probable AD were much more likely to exhibit volume loss than HCs (80.4% versus 20.7%), with the most prevalent site of atrophy observed in the medial TL region. The largest difference in terms of atrophy related to the entorhinal cortex scores, with greater atrophy of this region being a prevalent finding in the patients with probable AD and much less frequently observed in the HCs (93.5% versus 31.0%). Of note, finding atrophy in the HCs is consistent with broader research literature as well, and more work is needed to understand the possible relationship between cerebral atrophy and normal aging, conversion to disease, and functional status [43].
We examined evidence of vascular changes on the available neuroimaging, as recent studies continue to demonstrate the important contribution of such factors to the cognitive decline observed in patients with AD [44]. In this regard, both groups were very likely to demonstrate white matter changes in general, and this appeared more extreme than observed in developed countries of the west. The prevalence of white matter changes was higher among probable AD (97.8%) than HCs (89.7%), but both groups showed high prevalence rates. The occurrence of microhemorrhages was elevated in both probable AD and HCs (35.5% versus 25.0%) as well, with the HCs especially showing an elevated prevalence rate compared to international statistics.
Previous studies have reported this profile of white matter changes [45] in temporal, medial TL [5], and entorhinal cortex atrophy [6] in AD patients. These results suggest that white matter abnormalities are also common findings in individuals with probable AD in SSA/DRC. Results also showed that hippocampal atrophy significantly discriminated probable AD from HCs. Finally, the hippocampal volumes of this sample had strong and positive associations with memory measures. Like many Western studies [46], our study supports the use of hippocampal atrophy as a biomarker of AD in thispopulation.
Memory performance in a SSA cohort of patients with probable AD
As hypothesized, the patients with probable AD performed worse than HC subjects on all three memory measures. Many participants showed total forgetting in verbal and visual memory tests. These findings are similar with western memory tests which have demonstrated poor performance among probable AD subjects [47]. These findings also showed the importance of including visual memory tests in the evaluation of AD patients making the AVMT a better test in assessment of cognitive aging. Our results also support the ability to the ANB memory tests (ALT and AVMT) to discriminate probable AD participants from healthy aging.
Relationship between neurocognitive performance and neurodiagnostic findings in an SSA cohort of patients with probable AD and HC subjects
In the entire sample, there was a significant positive association between all three memory measures and bilateral hippocampal volumes. After adjusting for the possible effects of depressive symptomatology upon cognitive performance, we found that visual and total memory were significantly associated with independent hippocampal volumes consistent with previous literature [48, 49]. In contrast, we did not find a significant association between verbal memory and various hippocampal volumes and between visual memory and left hippocampal volumes after including depression scores in the statistical model. This highlights the potential confounding effect that mood symptoms can have in these models. Our results with verbal memory and hippocampal volumes remained on the verge of statistical significance even when controlling for mood symptoms and would likely hold up in a larger sample of patients. Total memory demonstrated higher correlation with hippocampal volumes than visual and verbal memory measures. In terms of memory modality, the AVMT showed higher associations with hippocampal volumes than the ALMT scores. In sum, these results confirm the association between memory measures and hippocampal volumes, and the need to control for confounding or interacting variables such as psychiatric status.
While lateralized memory findings are frequently observed in the research literature, our study did not find evidence of laterality with regards to the association between memory specific modality and hippocampal volumes. The strength of association was not dependent on memory modality and hippocampal hemisphere. Bonner-Jackson et al. [10] have reported similar findings in assessing the association between hippocampal volumes and memory tests. These researchers have argued that the use of the heterogenous sample could lead to this lack of lateralization effects.
As noted, this the first study to examine the association between memory tests and hippocampal volumes in SSA/DRC due to lack of culturally appropriate neuropsychological tests and neuroimaging tools. The findings of this study provide evidence of the usefulness of ANB memory measures in this sample to predict probable AD. Our analyses also showed the importance of MRI as a diagnostic tool of AD with specific emphasis on atrophy of the medial TL structures (particularly the hippocampus). Although prevalence of white matter changes was not diagnostic, the elevated rates of such problems across the entire sample suggest that studying cardiovascular factors in the SSA will be critical in any studies of aging and dementia.
Overall, strengths of the current study include use of a culturally validated neuropsychological tests and the ability to collect neuroimaging data in participants who are not familiar with MRI. Our study used a case-control design to obtain cross-sectional results. This study is unique and rare in the SSA because it includes both neuroimaging and cognitive evaluation in the assessment of AD.
Limitations and future directions
For this initial study, we limited our sub-analyses to the medial TL region primarily (i.e., hippocampus, entorhinal cortex), as we wanted to reduce the number of overall correlational analysis in order to minimize risk of Type 1 (i.e., false positive) errors. In part, this resulted from our sample size being modest in this first DRC effort, given both the cost of MRI scans and the novel nature of their introduction in the DRC creating uncertainty about our ability to enroll subjects. Overall, we were pleasantly surprised at the success of the project, and we hope to employ even larger samples in the future, and to examine the association between volumes of other brain regions and memory measures as well as other cognitive tests in patients with probable AD. We also hope that our work will contribute to improved clinical diagnostic accuracy as it relates to the diagnosis of AD and other neurodegenerative dementias in SSA, which will in turn decrease the potential diagnostic heterogeneity that might currently exist. Finally, our focus on probable AD without the inclusion of intermediary cognitive decline (e.g., MCI cohort) could be seen as a limitation as well. As noted in the methods section, the decision to not include MCI was driven by both funding limitations and our desire to explore patterns of AD that are well established in the Western world, as a means of establishing the validity of these techniques in SSA. With this success, we will ultimately want to include other cohorts, and more fully establish the hypothesized utility of our novel African neuropsychological battery. In conclusion, despite some limitations, the current study provides evidence for the association between ANB memory measures and hippocampal volumes in elderly adults in general and in probable dementia in Kinshasa/DRC. Future research should build on the methods and findings provided by this study to the association of ANB and other brain structures in probable AD patients in SSA and in DRC and should include cohorts of patients with intermediary steps of cognitivedecline.
Footnotes
ACKNOWLEDGMENTS
The authors acknowledged the assistance and expertise from the Medical Center of Kinshasa and HJ Hospitals who have assisted our study with magnetic resonance imaging used in the study and other materials.
FUNDING
This study was supported by grants AARG-19-61778701 and P30AG066511-02S1 from the National Institute on Aging. Dr. Alonso was supported by NIH/NHLBI grant K24HL148521 and NIH/NIA grant P30AG06651. Dr. Drane and the neuroimaging analysis efforts were funded by the NIH/NINDS through grant R01 NS088748.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical reasons.