
Abstract
Maintaining diversity in drug development in research into Alzheimer’s disease (AD) is necessary to avoid over-reliance on targeting AD neuropathology. Treatments that reduce or prevent the generation of oxidative stress, frequently cited for its causal role in the aging process and AD, could be useful in at-risk populations or diagnosed AD patients. However, in this review, it is argued that clinical research into antioxidants in AD could provide more useful feedback as to the therapeutic value of the oxidative stress theory of AD. Improving comparability between randomized controlled trials (RCTs) is vital from a waste-reduction and priority-setting point of view for AD clinical research. For as well as attempting to improve meaningful outcomes for patients, RCTs of antioxidants in AD should strive to maximize the extraction of clinically useful information and actionable feedback from trial outcomes. Solutions to maximize information flow from RCTs of antioxidants in AD are offered here in the form of checklist questions to improve ongoing and future trials centered around the following dimensions: adhesion to reporting guidelines like CONSORT, biomarker enrichment, simple tests of treatment, and innovative trial design.
Keywords
DIVERSITY IN ALZHEIMER’S DISEASE DRUG DEVELOPMENT
The dominant idea in biomedical research into Alzheimer’s disease (AD) is that amyloid-β (Aβ) and tau proteins not only define AD but also cause it. The most vigorously tested therapeutic strategy, amyloid-lowering in AD patients, had generally met with disappointment [1] until recent findings of statistical significance following 12–18 month treatment with the anti-amyloid antibodies lecanemab and donanemab [2]. But the results obtained with these drugs have still not reached established criteria for clinical meaningfulness [3]. Moreover, anti-Aβ antibodies are costly, frequent infusions that increase the risk of brain injuries in the form of bleeding and swelling, which can have fatal consequences [4]. Finally, concerns have also been raised about the possibility of unblinding in the lecanemab treatment group in the CLARITY trial, resulting in reporting bias that cannot currently be ruled out without access to primary data and relevant analyses [5]. Thus, even these most recent results do not entirely counter claims that the AD community has historically been, and may still be, over-reliant on the amyloid-lowering strategy to find a disease-modifying treatment for AD [6].
It is therefore of vital importance that basic and clinical science reflect the values of scientific pluralism and plausibility [7]. In clinical research, the most recently-published analysis of AD drug development suggests that there is indeed significant diversity in the current pipeline. As of January 1, 2023, of 187 phase I, II, or III trials:
“22 (16%) of agents have amyloid, 13 (9%) tau, 24 (17%) inflammation, 18 (13%) synaptic plasticity/neuroprotection, 10 (7%) metabolism and bioenergetics, 7 (5%) oxidative stress, and 4 (3%) proteostasis/proteinopathy as their primary mechanistic targets” [8].
However, this snapshot of the pipeline only concerns the later stages of development of drugs for AD. So that it remains diverse in the future, it is vital that the community avoids over-reliance on the dominant amyloid hypothesis of AD which might result from the imposing reputation and credibility of those who argue in favor of amyloid-lowering as opposed to other strategies [9], as well as significant interest from the industry and patient organizations. For example, Ruth Itzhaki, who has long worked on the role of microbes in AD and has been a vocal critic of over-reliance on the amyloid hypothesis, has described “a series of battles …awful problems getting [research] published” [10]. It is vital that we continue to support the testing of different theories of AD in ways that respect pluralism and plausibility [9].
Despite the historical focus on amyloid, other strategies have indeed been tested over the past decades, and in 2019, Liu et al. [1] subsumed oxidative stress as part of the “Mitochondrial Cascade and Related Hypotheses” and found that 17% of clinical trials had tested such hypotheses over the last thirty years. This review will focus on oxidative stress as a possible therapeutic target in AD, highlighting the rationale behind targeting oxidative stress-related processes, lessons learned from historical and ongoing trials testing the therapeutic value of antioxidants in AD patients, and practical steps to improve future trials.
OXIDATIVE STRESS, AGING, AND ALZHEIMER’S DISEASE: THE RATIONALE FOR CLINICAL TRIALS OF ANTIOXIDANTS
Oxidative stress is caused by an imbalance in the redox state, when the production and accumulation of reactive oxygen species (ROS) in cells and tissues exceeds their detoxification [11]. Oxidative stress is ubiquitous across biological systems, and the oxidative stress theory of aging—in which it is thought to not only cause, but also define age—was dominant for much of the latter part of the 20th century, but is now thought to be untenable [12]. Oxidative stress and ROS are clearly involved in age-related neurodegeneration [13]. However, untangling the nature of this involvement is still under intense empirical and conceptual investigation. One way in which ambiguities about the role of oxidative stress in AD would be to maximize the quality of information flow across translational science into oxidative stress in AD.
Indeed, there is a wealth of data from preclinical and human observational studies implicating oxidative stress in AD [13–16]. In particular, there is very compelling evidence from both human observational data as well as pre-clinical studies that oxidative stress is involved in the etiology of AD based on the study of different areas of research, including oxidative damage to biomacromolecules and mitochondria [17]; metal ion homeostasis [18]; the spatial relationship between amyloid deposition and sites of oxidative stress [19]; and genetic variability in failure to limit ROS levels in AD [15, 20].
But across the spectrum of translation in AD research, there are interpretative hurdles to overcome in order to ascertain the precise role of different processes in disease etiology. Some sources of data lack the precision required to draw precise conclusions. For instance, there is significant epidemiological evidence that the consumption of ultra-processed foods leads to increased oxidative stress [21] and cognitive decline across different types of dementia [22]. It was indeed found that oxidative stress mediated the association between fat intake and cognition in older adults [23]. But there are many confounding factors that complexify our understanding of the mechanism by which certain behaviors or diets may increase or decrease the risk of age-related cognitive decline [24]. In other words, there are major “signal-to-noise” issues.
As such, there is a need to establish the extent to which oxidative stress has specific prognostic and therapeutic value in AD [7]. This debate has focused on the possibility of oxidative stress markers serving as biomarkers for AD [25, 26], and as therapeutic targets in clinical trials [13, 28]. Central to the meaning of the term “Alzheimer’s” is diagnosis of a specific clinical syndrome. Historically, AD was understood as a specific clinico-pathological syndrome, defined by progressive amnesia, aphasia, and emotional dysregulation, as well as the discovery of specific neuropathological hallmarks post-mortem. But since the discovery of in vivo biomarkers, a controversial in vivo biological definition of AD based on Aβ, tau protein, and neurodegeneration has been proposed [29]. Nevertheless, most clinicians continue to argue that the diagnosis of AD requires a specific clinical syndrome to accompany such biomarker changes, defined as progressive hippocampal amnesia, logopenic variant primary progressive aphasia, and/or posterior cortical atrophy [30].
It is increasingly realized that there may be multiple realizability of the AD clinical syndrome through different biological pathways that contribute to neurodegenerative burden in individuals and populations [7]. It is important to note that, as concerns the prognostic and therapeutic value of oxidative stress in AD, biomarkers of oxidative stress are not currently part of the clinically-informed understanding of AD, and there are no treatments available for AD based on targeting oxidative stress. Currently, clinically-validated biomarkers of AD are restricted to cerebrospinal fluid (CSF) and positron emission tomography markers of Aβ, tau, and neurodegeneration [30].
Moreover, when we talk about “biomarkers” of oxidative stress, we must be clear about the uses of such biomarkers and their application to AD [31]. The major use of biomarkers of oxidative stress in AD is likely to be “theranostic” (a neologism of therapeutics and diagnosis), i.e., to improve diagnosis, monitor therapy (e.g., target engagement), predict treatment outcomes, and offer a more personalized medicine approach based on biomarker stratification [32].
The absence of oxidative stress in our clinical understanding of AD is suggestive of the lack of precision of our current understanding of the role of oxidative stress in producing the precise AD phenotype, i.e., a constellation of specific cognitive (progressive hippocampal amnesia, logopenic variant primary progressive aphasia), cerebral (posterior cortical atrophy), and biomarker abnormalities [7, 30]. But there could be other therapeutic rationale for targeting oxidative stress in AD beyond specificity for cognitive decline. For instance, oxidative stress is also well correlated with muscle loss and frailty [33]. The International Working Group on AD recognizes frailty, the accumulation of non-specific health deficits resulting in a clinical syndrome, as a risk factor for progression from mild cognitive impairment (MCI) to full-blown AD [30]. As such, there could be therapeutic benefits to targeting frailty in AD as an indirect “proxy” therapeutic target acting on non-specific aspects of the aging process [34].
Moreover, it has been argued that “it is still unclear whether oxidative stress is a cause or a consequence of the process that occurs in AD patients’ brains” [13]. Thus, there is also solid rationale for targeting oxidative stress for the purpose of symptomatic relief in AD. For instance, the antibodies lecanemab and donanemab slowed relative cognitive decline in AD patients by approximately 30% over the 18-month trial period [2]. However, 12-to-18 month trials represent a small part of the disease spectrum, and there is community-wide disagreement about the effect of the small benefit beyond the trial window. Planche and Villain [35] argue that there are three anti-Aβ scenarios in AD: a symptomatic effect (no slowing), an enduring effect (early slowing), and an increasing effect (sustained slowing across disease stages). They consider that current trials cannot be used to determine which of these scenarios is correct, and that anti-Aβ antibodies may act via a symptomatic mechanism.
Moreover, just as there are lessons for antioxidants in AD from putative disease modifying anti-Aβ drugs, so too are there lessons from approved cholinesterase inhibitors, generally understood to be symptomatic treatments. These drugs improve certain symptoms linked to a defect in cholinergic transmission within the central nervous system, highly vulnerable to the pathophysiological process of AD. Though understood as “symptomatic” agents as regards the theories of what is thought to cause AD [1], there is evidence suggesting that their long-term use leads to reduced functional decline [36] and mortality in AD patients [37]. More will be said on the question of trial design with antioxidants in AD in the final section of this review.
Finally, when considering the “rationale for clinical trials,” it is not just based on the solid scientific claim that oxidative stress is an early or central event in AD that may have prognostic and/or therapeutic value to patients. It is also based on the need for a tool to provide patient-centered feedback on the therapeutic value of the oxidative stress theory of AD. It is not a “guillotine” hanging over the oxidative stress theory of AD, in that one failed trial would lead to the rejection of an entire theory supported by different lines of evidence [38]. Nevertheless, it is important that the therapeutic value of the oxidative stress theory be tested with patients in need of better treatments.
Implementing such tests has meant giving antioxidants to patients with MCI or AD. Antioxidants are compounds that inhibit oxidation or reactions that result from unstable free radicals. They counteract the effects of free radicals by neutralizing them or converting them to a less-toxic molecule. The most ubiquitous process by which oxidation occurs—“autoxidation”—results from hydrocarbons reacting with oxygen at normal temperatures. As such, antioxidants have a variety of industrial and alimentary uses to extend the lifetime of different hydrocarbon-based products. Such hydrocarbon-based entities include biological membranes. As such, within bodily cells, different antioxidants act to reduce damage from oxidative stress that occurs during normal bodily homeostasis.
Pisoschi and Pop define antioxidants according to the following criteria: “enzymatic and non-enzymatic, preventative or repair-systems, endogenous and exogenous, primary and secondary, hydrosoluble and liposoluble, natural or synthetic” [39]. Most discussions concerning different classes of antioxidants and their possible role as putative therapies in AD have tended to focus on the most specific dimension to human biology, endogenous [40] and exogenous [41] antioxidants—those that are produced in the body, versus those that are found in the environment (i.e., diet). Pritam et al. [13] consider seven classes of antioxidants “documented for having the potential to counter AD”: vitamins, carotenoids, polyphenols, alkaloids, hormones, coenzymes, and what they term “other compounds” (“MitoQ, selegiline”).
There is one final informational hurdle that may affect the signal-to-noise ratio at the level of the population. Based on early, influential studies of antioxidants in AD with published conclusions such as “High dietary intake of vitamin C and vitamin E may lower the risk of Alzheimer disease” [42], health-conscious members of society may already be implementing such dietary recommendations to lower their risk of developing AD.
Because of the combined informational complexity, both of AD as a clinico-biological entity with a complex etiology and an uneven distribution of its risk factors across the aging population, and the evolved, ubiquitous and informationally complex nature of oxidative stress as a cellular process that lacks a specific receptor or a single major metabolic pathway [14, 43], the testing of the therapeutic value of antioxidants to at-risk or AD patients is essential from an informational point of view. Moreover, as alluded to above, the extensive classification of antioxidants is such that there are many putative therapeutic mechanisms by which these compounds may be useful in AD. Given this informational complexity, it is vital that there be some method available to test the direct therapeutic value of modulation of oxidative stress in AD patients or at-risk populations.
This is what makes the randomized clinical trial (RCT) of antioxidants in AD such a useful tool to both patients and researchers alike. There is no denying that there is a paradox between recent models of AD etiology in which complexity is the dominant theme [44], versus the relative simplicity of RCTs that measure the therapeutic effects of changes in one variable. However, the RCT is useful not just because of claims made about knowledge, but also for ethical reasons: care practices and recommendations based on rigorous outcomes of RCTs allow for more ethical medical practice and avoid the propagation of non-validated treatments [45], which is a pre-existing problem in AD research and care [46].
Indeed, one obstacle on the way to such standardization is a widespread idea within the AD research community that informs trial designs: the premature combination of putative treatments [47]. While researchers are increasingly realizing that AD has a multifactor etiology [44], there are extreme instances of combination treatments in the AD research community in the form of popularized “metabolic enhancement protocols” that have several ethical consequences for research, including the frustration of information flow [46]. But there are other less problematic examples formulated within the AD literature that fundamentally rely on the same idea. Well-known “multi-domain” RCTs in at-risk populations, the Finnish Geriatric (FINGER, see below), pre-DIVA, and MAPT, all relied on a combination of different aspects of physical, cognitive, and social stimulation. It is intuitive to design such trials: if we seek to maximize the putative therapeutic impact of the intervention for a condition with multifactorial etiology, it makes sense to include as many therapeutic variables as possible. If the trial reaches its primary outcomes, as in the small therapeutic effect of the FINGER trial [48], then recommendations can be made based on such outcomes. The problem is when RCT methodology is not used as in the case of metabolic enhancement protocols [46], or, in the case of RCTs, the trial fails to reach its primary outcomes (see below).
Aspects of historical and ongoing trials of antioxidants will now be studied so as to inform practical steps that could lead to their improvement in the future.
HISTORICAL AND ONGOING CLINICAL TRIALS OF ANTIOXIDANTS IN ALZHEIMER’S DISEASE
It is important that the model used to understand translation in AD research, characterized by high attrition rates of clinical trials across different therapeutic targets, be as adequate as possible. Here, the translation from theories of AD to clinical research and practice is understood as a “web of information” [49] rather than a linear pipeline, as is often construed [8]. According to the web of information, the product of translation is information “about the coordinated set of materials, practices, and constraints needed to safely unlock the therapeutic or preventive activities of drugs, biologics, and diagnostics” [49].
Thus, the pipeline is a useful first image to understand the process of drug development and the differences between pre-clinical and later-stage clinical research. But it does not reflect the reality of data and information flow in the process of translation, and is slightly misleading insofar as it reinforces the idea that the arrow of progress moves in only one direction from preclinical studies to later clinical trials, with an emphasis on treatment hardware as the end product (e.g., a drug) [49]. In other words, there is only movement “from bench to bedside.” However, RCTs treating patients via randomization into two groups at the “end” of the drug pipeline serve not only the role of potentially improving outcomes in the treatment arm, but also providing actionable feedback for future trials and priority setting [49]. In this sense, even a “failed” trial can represent progress if useful information can be extracted from it. Thus, information flow would be more adequately described by the expression “from bench to bedside and back again” [50, 51].
However, actually obtaining actionable feedback from trials is a major problem for neurodegenerative research in general, including therapeutic research into the dominant amyloid-lowering strategy in AD patients [38]. Despite decades of trial failures, the AD research community continued to pursue the amyloid-lowering strategy [3]. Whether or not recent and forthcoming results from anti-amyloid antibodies ultimately justify this persistence, it is suggestive that we as a community do not significantly adjust priority setting based on the negative results of clinical trials.
In AD research, there is a generalized mismatch between promising associations in AD research, and the putative interventions they inspire in the form of RCTs [7]. Thus, like with most other targets in this treatment-resistant population, RCTs testing the therapeutic value of antioxidants in AD have shown negative results over the last two decades [52]. In particular, such RCTs have suffered from “extremely poor comparability” because of their “lack of homogeneity and numerousness of tested groups as well [as] differences in study design, type and dose of supplement, endpoint” [28].
In Pritam et al.’s review of trials of oxidative stress from 2022, it is noteworthy that many of the 21 completed trials did not measure changes in biomarkers of AD neuropathology. One early trial with AD patients showed how antioxidant treatment may impact markers of oxidative stress without affecting markers of AD neuropathology [43]. Given the high attrition rates of clinical trials in AD [53], inclusion of biomarkers of AD neuropathology would provide standardization for patient inclusion as well as the measuring of dose-response effects [54]. Conversely, the absence of biomarkers across the treatment and control group makes it impossible to rule out background assumptions as to why a treatment did or did not work [38].
Moreover, there have been examples of clinical studies of antioxidants in AD research being extremely underpowered. For instance, one pilot study exposed 22 AD patients to a 12-week treatment [55]. From an informational point of view, due to the combination of the small patient sample and the short exposure window, it is very hard to draw conclusions about our understanding of oxidative stress in AD from its finding that “little difference between treatment and baseline periods in the rate of decline of efficacy measures.” Other studies testing antioxidants did not actually report their data (for example, NCT01811381 with curcumin, NCT02033941 using grape seed extract). It is therefore vital that all human studies with antioxidants are appropriately funded, monitored, and reported.
According to the recently published 2023 AD drug development pipeline, there are seven ongoing trials with treatments targeting oxidative stress as its principal mechanism [8]. The actual number may be higher than reported, because there are other putative treatments being tested in AD patients that may act through antioxidant mechanisms amongst other mechanisms. For example, the ongoing trial NCT04044131 is testing the value of combined metabolic activators given as one treatment, which according to the investigators “promotes mitochondrial fatty acid uptake from the cytosol, facilitates fatty acid oxidation in the mitochondria, and alleviates oxidative stress” [56]. Though the treatment is itself complex (i.e. combined), the test of its therapeutic value is simple (one-variable), making interpretation of its mechanism of action more likely [47].
Specifically on the subject of trials testing the therapeutic value of the oxidative stress theory of AD, the “extremely poor comparability” [28] of RCTs of antioxidants in AD is perhaps the biggest obstacle blocking the flow of clinically useful information. Because if we cannot compare trials, how should we prioritize the testing of different therapeutic leads? If an antioxidant-based treatment fails to improve AD outcomes, is it due to a theoretical or practical failure involving trial design and implementation? It is vital that clinical trials become more standardized so as to be more comparable between them.
More specifically on the subject of the role of oxidative stress in AD, Pritam et al. argue that “the integrated system of antioxidants with multiple drugs may provide higher effectiveness” [13]. Veurink and colleagues consider that treating AD may require “simultaneous supplementation of a combination of antioxidants at sufficiently high personalized doses and a nutrient-rich, low-carbohydrate diet” [57]. It is becoming increasingly likely according to different researchers, including those who work on the amyloid-lowering strategy [44], that treating AD may require combination cocktails. However, it should not be the job of the RCT to test those numerous putative contributions all in one go. The problem with combining unvalidated treatments is identifying active and inactive ingredients in a treatment recipe [47]. As a thought experiment, imagine you have a favorite dish at a restaurant, and the chef changes one ingredient (i1) in a taste experiment. You detect the change, do not like it, and tell them to change the recipe back. But if they had changed two ingredients (i2, i3) at the same time, and you still did not like it, you would not know if i2 or i3 might have actually improved the dish individually, but you just did not like the combination [47]. Furthermore, you would also have to take into account doses of each ingredient: maybe more of i2 would have been better, and less of i3, or vice versa. This culinary example holds a lesson here for RCTs in AD: minimize the change in variables in an RCT because, what if one treatment component alone might improve outcomes, for example, with a higher dose, but you cannot detect it because of the combination effect?
Such is the problem of interpreting the results of multi-domain clinical trials that fail to reach their primary outcomes. And even those trials that do, like the small compound effect of the FINGER trial [48]—actually identifying the active ingredients in the treatment recipe is still near impossible because of the multi-domain nature of the proposed treatment. The FINGER trial consisted of dietary and nutritional guidance; vigorous physical exercise; cognitive training and social activity; and management of metabolic and vascular risk factors, versus regular health advice for controls. It seems reasonable there was at least one treatment component in the FINGER trial that did not contribute to improved outcomes, and also at least one component whose impact could have been increased with a greater relative dose. Moreover, there is also the possibility of combination effects, both synergistic and antagonistic [47]. To not be able to untangle these dimensions leads to a form of interpretative oversight, even for a trial cited as a success.
IMPROVING CLINICAL TRIALS OF ANTIOXIDANTS IN ALZHEIMER’S DISEASE
The suggestions in this section are centered around the following dimensions: proper reporting of trial results through adhesion to reporting guidelines like CONSORT, biomarker enrichment to improve trial precision and interpretation, simple tests of treatment to aid interpretation, and innovative trial design.
As part of the informational need to derive feedback from trials of antioxidants in AD, it is vital that communication from trials respects the criterion of truthful reporting. The first major step in improved communication is actually reporting data from trials, whether they be positive or negative. When data from treatments with AD patients are not reported accurately, it can mislead patients and researchers [46]. Thus, it is vital that results from trials adhere to reporting guidelines such as the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement, including very recent updates to further improve reproducibility with an emphasis on the reporting of outcomes [58]. The purpose of these guidelines is to “enhance trial utility, replicability, and transparency” [58].
Until biomarkers of AD neuropathology came available for use in clinical research within the last decade, it was found that many patients were included in amyloid-lowering trials without confirmation that they were amyloid-positive. By analogy, the unavailability of clinically-validated biomarkers of oxidative stress begs the question about the patient population for which it would be most suitable to test putative antioxidant therapy. Plasma biomarkers of oxidative stress are being developed [59] and increasingly used for clinical research in different conditions [60]. Given the informational complexity of oxidative stress, and the broad meaning of the term “biomarker” with different goals discussed above, there are several questions to ask about which biomarkers would be most appropriate for use in different conditions like AD [61, 62]. Though there are some such biomarkers available in CSF [63], there are many advantages to blood-based biomarkers including reduced invasiveness [64]. Table 1 of Varesi et al. [65] provides a summary of recent progress in research into different putative blood-based oxidative-stress biomarkers that may be suitable for use in AD.
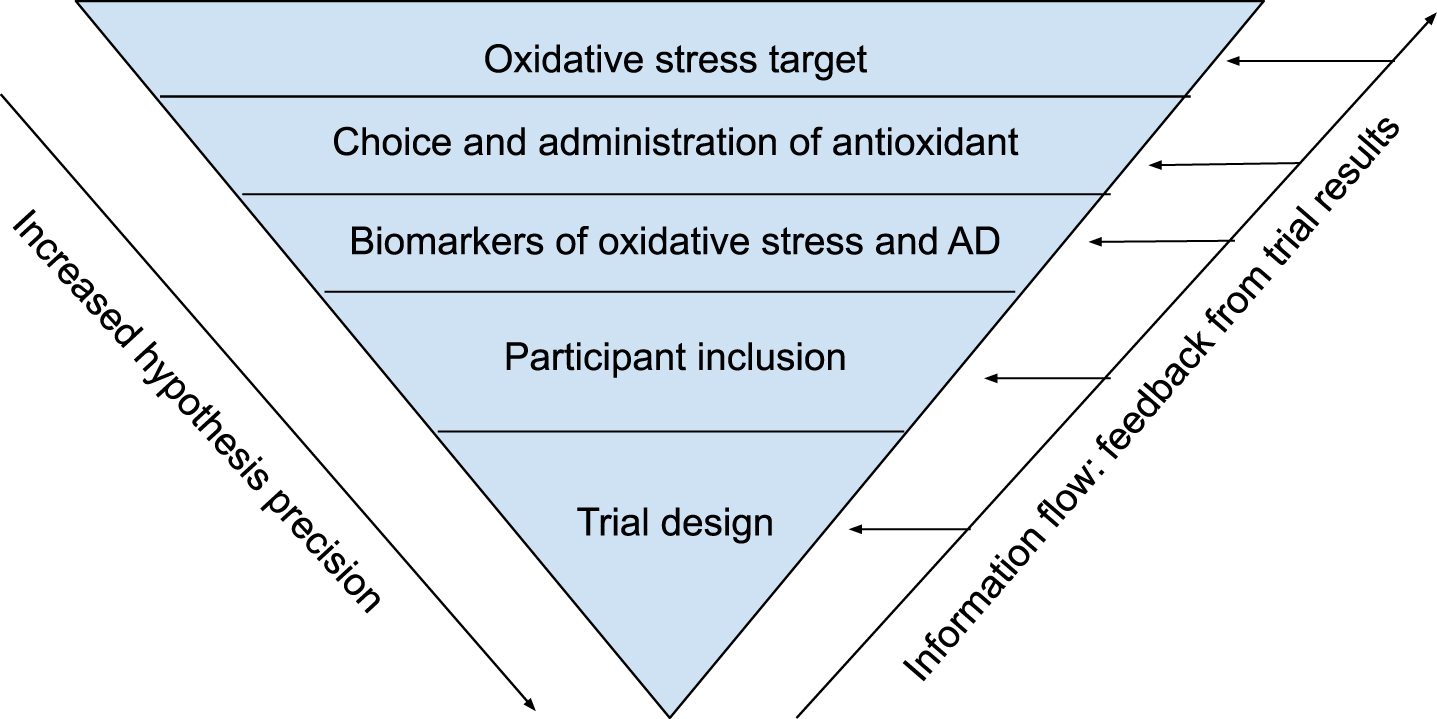
A checklist of questions about target, drug, biomarkers, participants, and trial design to maximize information flow in clinical trials of antioxidants in Alzheimer’s disease (AD). Adapted from Cummings et al. [54]
For example, the first study of blood-based oxidative stress markers and domain-specific cognitive performance in a large general population sample of older adults found that derivatives of reactive oxygen metabolites may have theranostic uses [66]. However, this field of study started around 2015 [66], making it young. In the name of precision [7], researchers should focus on investigating the relationship between plasma biomarkers and the specific clinical AD phenotype. It is therefore significant that glutathione, an endogenous antioxidant produced de novo in the cell cytoplasm, is depleted in the hippocampus of patients with MCI and AD, with the extent of depletion correlational to poorer cognitive test performance [25]. Plasma glutathione may be useful as a predictor of outcomes in stroke [67], but a recent review found that more standardized studies are required to determine the value of both plasma and cerebral markers of glutathione as theranostic biomarkers in AD [68]. One possibility to increase precision in the hippocampus is to use a glutathione–iron tandem biomarker [69]. In any case, it is vital that affordable, specific, and quantifiable biomarkers be developed for clinical research so that patient stratification as well as dose-response relationships (i.e., theranostic goals) can be established, with the goal of improving the design and interpretation of clinical trials. In other words, such biomarkers could be implemented across trials to answer the following questions for RCTs in AD: “Is the trial population oxidative-stress positive in ways relevant to AD?,” and “Did the treatment intervention reduce levels of AD-relevant oxidative stress?”.
Moreover, on the subject of the design of clinical trials, it is important to learn from theoretical and practical issues related to previous trials with other agents. One of the most important features of clinical trials in AD is the difference between two time courses: that of AD itself, which lasts several decades [70], and that of the trial. Even well-funded late-phase trials do not tend to last longer than 18 months, which represents a small portion of the total AD spectrum. Thus, ideally, trials testing antioxidants in AD would last as long as possible to better match the time course of AD [71]. Planche and Villain argue that one way of settling whether a treatment has a symptomatic effect (no slowing), an enduring effect (early slowing), or an increasing effect (sustained slowing across disease stages), is to use a delayed-start trial design with a putative treatment in early AD [35].
Moreover, another lesson from anti-amyloid trials in AD, related to the theoretical disease time-course, is the elaboration of “disease scenarios” [72–74]. In its simplest form, these scenarios are a theoretical schema as to the temporal and pathogenic relationship between a variable and outcomes in AD. Researchers working on the amyloid-lowering strategy elaborated four possible therapeutic hypotheses to be tested in RCTs: driver, trigger, threshold, and speed [38]. The first and most basic is the “driver” scenario in which amyloid exerts a neurodegenerative effect through a linear mechanism; as such, any and all reduction in Aβ in AD would have a therapeutic effect. The next is the “trigger” scenario in which Aβ triggers a neurodegenerative cascade and then essentially becomes a spectator in AD; only early removal of Aβ would be beneficial. The “threshold” scenario would require lowering amyloid below a certain threshold to see an impact. The “speed” scenario would require steep, rapid removal of amyloid below a certain threshold to see an impact [74]. This speed scenario inspired recent interpretations of the possible clinical benefit of lecanemab and donanemab [75]. Researchers testing antioxidants in AD could also attempt to elaborate and test possible therapeutic scenarios. Again, doing so would require the use of biomarkers of oxidative stress for theranostic purposes, underlining the importance of making such biomarkers available for widespread use in AD clinical research.
So as to tie up these different unresolved questions, it is noteworthy that the research community studying oxidative stress in AD has generally not studied familial or autosomal dominant AD, which provides a unique causal cohort that has inspired other research avenues including the amyloid hypothesis as well as recent cases of resistance and resilience to AD through mutations [76]. Some early research into oxidative stress in familial AD could inspire further lines of inquiry [77], including the use of these cohorts to test the long-term value of antioxidant use in these populations through the use of cohort studies.
Finally, Cummings et al. [54] argue that there are five “right questions” to ask for precision drug development in AD: right target, drug, biomarkers, participants, and trial. If any one of these considerations is skipped over, it will increase the likelihood of an informational blockage in the web of information between bench and bedside and back again, because getting feedback from “failures” is made impossible due to the existence of untestable background assumptions. Their important reasoning can be applied to clinical trials of antioxidants in AD. However, unlike the linear vision of translation defended by the authors, such questions can be asked about drug development of antioxidants in ways that reflect the feed-forward-feedback nature of translation (Fig. 1, Table 1).
CONCLUSION
Antioxidants could be used to diversify the treatment arsenal in AD. There is major scope for innovation in trials of antioxidants, including more adequate reporting of results, biomarker enrichment to rule out background assumptions, and innovative trial methodologies for simple tests of antioxidant treatments to improve interpretation. Adopting such measures should lead to improved information flow and better outcomes for people at risk of, or with, AD.
On the other hand, researchers and clinicians can continue to make broad recommendations on possible inclusion of antioxidants as part of healthy dietary advice, as well as action against exogenous sources of ROS through different forms of environmental pollution [81]. But such broad-brush measures, lacking the precision necessary for rigorous trials, should exist alongside other lifestyle measures informed by epidemiological associations, and should not be thought to replace rigorous simple tests of putative interventions [47]. It is vital that researchers make small victories with antioxidants in AD with well-designed, clinically useful trials.
Footnotes
ACKNOWLEDGMENTS
The author thanks three anonymous reviewers for help in improving the manuscript.
FUNDING
The author has no funding to report.
CONFLICT OF INTEREST
Timothy Daly is an Associate Editor of the Journal of Alzheimer’s Disease but was not involved in the peer-review process nor had access to any information regarding its peer-review. The author has no other conflicts of interest to report.