
Abstract
GRN mutations, causing frontotemporal dementia, can be associated with atypical white matter hyperintensities (WMH). We hypothesized that the presence of WMH may impact neurofilament light chain (NfL) levels, markers of neuroaxonal damage. We analyzed plasma NfL in 20 GRN patients and studied their association to visually-scored WMH burden. The 12 patients displaying atypical WMH had significantly higher NfL levels (98.4±34.9 pg/mL) than those without WMH (47.2±29.4 pg/mL, p = 0.003), independently from age, disease duration and Fazekas-Schmidt grade. NfL correlated with WMH burden (rho = 0.55, p = 0.01). This study prompts considering WMH burden as a variability factor when evaluating NfL levels in GRN patients.
Keywords
INTRODUCTION
Frontotemporal dementias (FTD) are rare neurodegenerative dementias, with a strong genetic component. GRN mutations are responsible for 20% of familial FTD [1]. The main phenotypes associated with GRN mutations are the behavioral variant of FTD (bvFTD), followed by primary progressive aphasia and corticobasal syndrome [2]. In addition to lobar atrophy, GRN mutation carriers were found to present an unusually high burden of white matter hyperintensities (WMH), extending from subcortical to paraventricular white matter, particularly in the frontal and occipital lobes [3–5]. Notably, these WMH can be found in the absence of any cardiovascular risk factors [6]. In addition, WMH often display atypical distribution, along some of the main white matter bundles, such as the tracts linking the dorsal striatum with the prefrontal cortex, the genu of the corpus callosum, and the posterior parts of the superior longitudinal fasciculus and inferior fronto-occipital fasciculus [5]. For these reasons, these WMH have been hypothesized to be probably due to “atypical”, presumably degenerative leukopathy, with distinct imaging features than those of vascular leukopathy [7]. The underlying pathophysiology of WMH in GRN mutation carriers is not yet determined, although prior evidence suggests that they may result from regional microglial dysfunction and axonal degeneration [6, 9].
Neurofilament light chain (NfL) are plasma-based biomarkers sensitive to neuroaxonal damage, whose levels are increased in many neurological disorders with proven usefulness for both prognostic assessment and monitoring of treatment responses [10, 11]. Among FTD patients, NfL are higher in GRN compared to C9orf72 and MAPT carriers or sporadic cases [12–15], which could be possibly explained by severe neuroaxonal degeneration occurring in GRN disease [5]. In this study, we aimed to analyze plasma NfL levels in GRN patients according to the features and extension of their WMH burden. We hypothesized that patients displaying more severe and widely distributed leukopathy would display higher NfL levels. This is an important question because international efforts are currently underway to identify the factors impacting NfL levels and the thresholds to be considered for clinical practice and therapeutic trials in genetic FTD.
MATERIALS AND METHODS
Participants
Patients included in this study all carried loss-of-function mutations in GRN gene (Supplementary Table 1). They were recruited through a French research network on FTD/ALS (Inserm RBM 02-59) and Predict-PGRN study (NCT04014673) [16, 17]. They had a clinical diagnosis of bvFTD, formulated according to current diagnostic criteria [18–20], based on behavioral and cognitive evaluation. Disease severity was rated using the CDR+NACC FTLD (Clinical Dementia Rating plus National Alzheimer’s Coordinating Center FTLD) scale. All patients had at least one brain MRI scan with a blood sampling for NfL measurement performed within 6 months. Individuals who had concurrent neurological conditions, outside FTD spectrum, were excluded. Patients were assessed for common cardiovascular risk factors (hypertension, diabetes, dyslipidemia, smoking, and hyperhomocysteinemia) or coronary artery disease (see Supplementary Table 2). Moreover, known factors impacting NfL levels (traumatic brain injury, seizures, kidney disease) were ruled out prior to their dosage. All patients signed informed consent for clinic-genetic study. Those protocols were approved by the Paris Necker Hospital/AP-HP Ile-de-France VI ethics committees (CPP 68– 15, ID RCB 2015-A00856-43). For more details on patient selection, see the Supplementary Material.
MR study and image analysis
MRI studies were performed in clinical practice, including a mandatory FLAIR sequence with standard parameters. WMH burden was calculated through visual rating by two independent experts (neuroradiologist, neurologist), separately. In case of discordance, the scoring of the neuroradiologist prevailed (a concordance index of k = 0.9 was obtained). WMH were considered due to atypical leukopathy in presence of: 1) extensive, confluent lesions (“plaques”), 2) including deep/periventricular and subcortical WMH (with U-fiber involvement), and 3) associated with cortical atrophy in the same regions. Eight different regions were assessed for the presence of those WMH (F = frontal right/left, P = parietal right/left, O = occipital right/left, T = temporal right/left). An ad hoc score of WMH burden severity, derived from a previous work on WMH in GRN disease [4], and adapted to take into account the number of all affected regions, in analogy to visual rating used in small vessel disease [21], was then calculated. Outside these criteria, other WMH were estimated to be due to vascular risk factors and were visually rated using the Fazekas-Schmidt scale [22]. Participants displaying high concurrent vascular burden (Fazekas-Schmidt grade = 3) were systematically excluded. Examples of two paradigmatic cases, with and without atypical WMH are provided in SupplementaryFigure 1.
NfL dosage in plasma
Plasma NfL levels were analyzed using Single Molecule Array (SiMoA) in accordance with the manufacturer’s instructions (Quanterix, USA) as previously described [14]. All measurements were performed in the same facility, in duplicate. Samples with a coefficient of variation (CV) of > 5% were excluded. The median intra-assay CV was 2.5% (range: 0.4%–5%). As previously described, internal control plasmas of different NfL concentrations were analyzed in each run, demonstrating satisfactory run-to-run variability [14].
Statistical analyses
Demographic and clinical variables were compared between the groups using Fisher’s exact test for categorical variables, and Student’s test and Kruskal-Wallis’ test for continuous variables. Shapiro-Wilk’s test was used to test data normality and Bartlett’s test to assess homoscedasticity across groups. Correlation analyses were performed with Pearson’s or Spearman’s test according to data distribution. General linear model was used to adjust all confounding variables such as age, gender, disease duration, and CDR+NACC FTLD score. A two-sided p-value of < 0.05 was considered statistically significant. Statistical analyses were performed with the RStudio software version 4.2.2.
RESULTS
Population
Among the 20 patients included in the study, 12 presented WMH (GRN-WMH+ group) and 8 did not present WMH lesions on MRI (GRN-WMH- group). All types of loss-of-function mutations were found, and there were no specific recurrent mutations or prevailing mutation types in any group. Their demographic and clinical characteristics are described in Table 1. The mean age at onset was 58.2±10.0 years (range: 33-73), and the mean disease duration at visit was 3.4±1.7 years.
Demographic and clinical characterization of the sample cohort. Asterisks indicate the significance of comparisons between the groups: **p<0.01, CDR+NACC FTLD, Clinical Dementia Rating plus National Alzheimer’s Coordinating Center FTLD; F, female; FAB, Frontal battery assessment; M, male; MMSE, Mini-Mental State Examination; NfL, neurofilament light chain; WMH, white matter hyperintensities. p-values in the table refer to Fisher’s test (for sex), and Student’s t-test (for age at onset, age at evaluation, disease duration, NfL levels, MMSE, FAB, CDR+NACC FTLD scores)
In GRN-WMH- group, the mean age at visit was 59.4±12.1 years and mean duration of disease was 2.9±1.1 years. Median Mini-Mental State Examination (MMSE) and Frontal Battery Assessment (FAB) were, respectively 25 (Q1 22; Q3 26.5) and 9 (Q1 4.5; Q3 13). Mean CDR+NACC FTLD global score was 1.6±0.7 (range: 1-3). Three patients had known cardiovascular risk factors (Supplementary Table 2) and 5 presented vascular leukopathy (Fazekas-Schmidt grade 1 in four patients and grade 2 in one).
Among the 12 GRN-WMH+ individuals, the mean age at visit was 62.9±8.8 years and mean disease duration was 3.7±1.9 years. Median MMSE and FAB were, respectively, 19 (Q1 16; Q3 24) and 6 (Q1 5; Q3 12). Mean CDR+NACC FTLD was 2.2±0.6 (range: 1-3). All of them (n = 12) had WMH in frontal regions, three in parietal, two in occipital, and one in temporal areas (Table 2). In case of asymmetric distribution, WMH prevailed on the more atrophied hemisphere. Moreover, eleven of them presented concomitant signs whose distribution and features were typical of vascular leukopathy. Their Fazekas-Schmidt grade was 1 in nine and 2 in the remaining two patients. Four of them had at least one identified, well-controlled cardiovascular risk factor (Supplementary Table 2).
Characterization of imaging findings in the GRN-WMH+ subgroup. WMH: white matter hyperintensities. a) Vascular leukopathy was present in 16 out of 20 (total sample), and present in 5 out of 8 patients in GRN-WMH-
NfL levels in both groups of GRN patients
There were no statistically significant differences between GRN-WMH+and GRN-WMH- patients for gender, age of onset, age at sampling, disease duration, MMSE, FAB, CDR+NACC FTLD scores (Table 1). Plasma NfL were significantly higher in GRN-WMH+ (Fig. 1A and Table 1) (p = 0.003). Mean NfL levels were 47.2±29.4 pg/mL (range 4.9-89.2) in GRN-WMH- patients and 98.4±34.9 pg/mL (range 47.3-168.5) in the GRN-WMH+ group. This difference survived after correction for age at sampling, gender, disease duration, and CDR+NACC FTLD (p = 0.006).
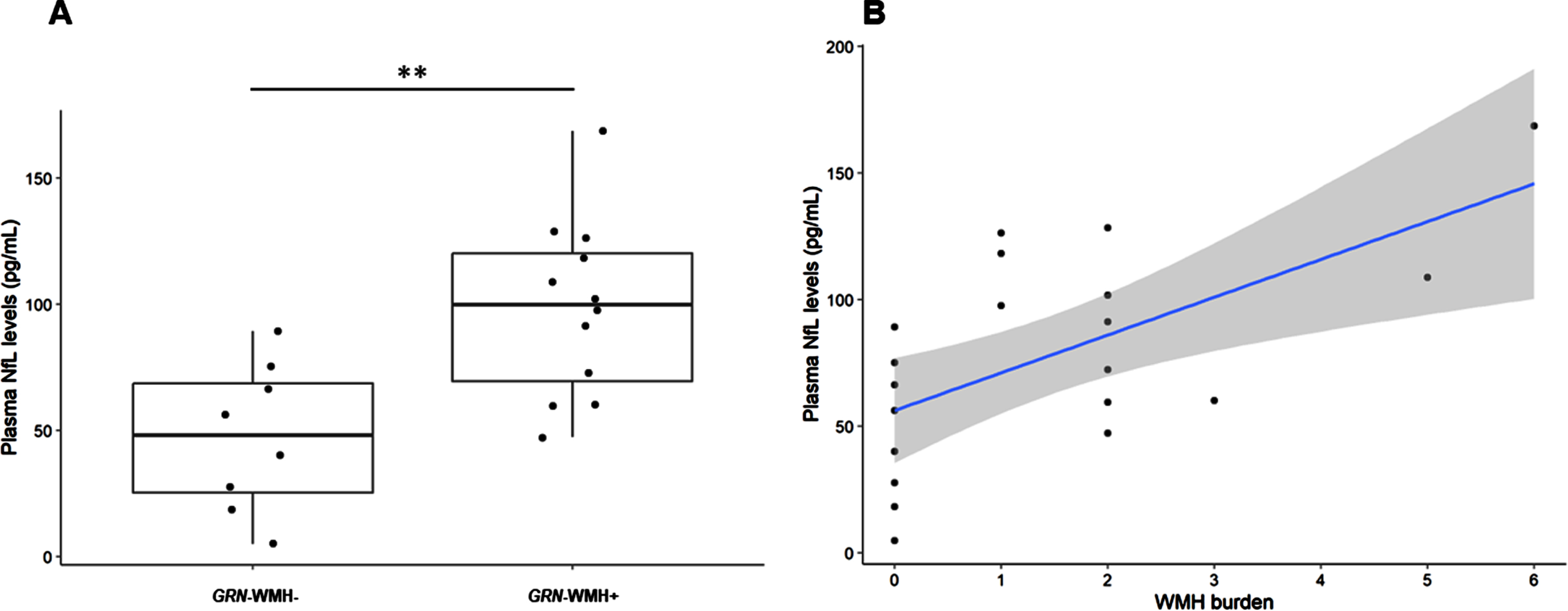
NfL levels according to WMH status (A) and WMH burden (B). Asterisks refer to p-value, with ** meaning p < 0.01. NfL, neurofilament light chain; WMH, white matter hyperintensities.
Correlation between plasma NfL and WMH burden
WMH burden ranged between 1 and 6 in WMH-GRN+patients (median: 2; Q1 : 1.75, Q3 : 2.25). Plasma NfL levels were higher in individuals displaying a more severe WMH burden (Fig. 1B) (rho = 0.55, p = 0.01). Taking into account the presence of 3 patients (one GRN-WMH- and two GRN-WMH+) with Fazekas-Schmidt grade of 2, we repeated the analyses including only the 17 individuals with Fazekas-Schmidt grade≤1. Plasma NfL were still higher in GRN-WMH+ (104.8±34.8 versus 51.4±29.1; p = 0.005), with a significant correlation with their WMH burden (rho = 0.63, p = 0.007).
Correlation of NfL and WMH burden with other variables
No correlation between plasma NfL and age of onset (r = 0.155, p = 0.513), disease duration (r = 0.173, p = 0.465), or number of cardiovascular risk factors was found in this study (rho=-0.073, p = 0.761). NfL levels did not vary according to Fazekas-Schmidt score (r=-0.143, p = 0.549).
No correlation was found between WMH burden and age of onset (rho = 0.077, p = 0.748), disease duration (rho = 0.319, p = 0.171), MMSE (rho=-0.441, p = 0.275), FAB (rho = 0, p = 1), or Fazekas scale (rho = 0.217, p = 0.358).
DISCUSSION
A relevant proportion of GRN patients present WMH with specific characteristics and localization that allow distinction from more typical leukopathy of vascular origin. These WMH are thought to be due to neuroaxonal degeneration and likely reflect a more aggressive disease course [3–5]. This study analyzed the levels of plasma NfL in patients with GRN mutations and compared the burden between patients with and without WMH.
GRN-WMH+ patients presented significantly higher values of plasma NfL in comparison to GRN-WMH– individuals. Increase in NfL in GRN-WMH+ group was not impacted by patients’ age, which is a well-known factor conditioning NfL levels due to physiological axonal turnover [23]. Additionally, disease duration, disease severity, and clinical features were highly comparable between GRN-WMH+ and GRN-WMH-, suggesting that WMH burden is not simply due to disease aggravation, rather probably translating a more severe degenerative process at the biological level. These results are in line with previous studies evidencing a strong association between WMH burden and plasma NfL concentration in GRN mutation carriers [5]. Previous results and ours suggest that factors conditioning WMH burden are still quite elusive.
Our study contributes to understand the variability of NfL values among GRN mutation carriers. Previous works showed that GRN mutation patients had higher levels of plasma NfL compared to C9orf72 or MAPT mutation carriers and sporadic cases [12–15]. Notably, increase in NfL levels in GRN carriers occurs at the moment of, or just before the phenoconversion, and their levels tend to stay steadily elevated during the clinical phase, regardless of the stage and with no impact of disease duration [12, 24]. In our cohort, GRN-WMH+ individuals had even higher values than most previously reported NfL levels in GRN patients [5, 15]. This suggests that the presence of WMH in some GRN patients translates into mean higher values of NfL at group level. Therefore, in addition to the responsible genotype, the presence of WMH should be considered as a further factor of variability of NfL levels, among GRN carriers.
Concerning the pathophysiology of WMH, neither the presence of WMH nor their burden presented correlation with vascular risk factors or Fazekas-Schmidt scale. The co-occurrence of atypical leukopathy and cortical atrophy, and the higher values of NfL in GRN-WMH+ group, point out a role of neuronal/axonal loss, as NfL levels have been associated with cortical volume loss [12]. Notably, a previous histopathological study of a brain of a patient with bvFTD associated with a GRN mutation disclosed prominent microglial activation and microglial dystrophy, with only mild axonal loss and minimal vascular pathology [9]. Even if additional factors such as microglial dysfunction may be implicated in WMH pathogenesis, more supporting evidence is needed to confirm this hypothesis with larger pathological series.
This study contributes to better interpret NfL levels in GRN disease. Higher NfL values in GRN-WMH+ patients do not necessarily reflect more severe and/or advanced disease. Based on our results, we propose to consider WMH presence and burden in the interpretation of NfL values and, possibly, to adapt the thresholds accordingly, as done for other known variables (e.g., age, body mass index, renal insufficiency) [25]. Composite scores, including imaging and biochemical data, may prove to be more successful to stratify patients as to their progression, and carriers as to their risk of conversion, as the first proof-of-concept demonstrated [24].
This study has some limitations. The sample studied was not large, although representative due to the rarity of FTD caused by GRN mutations. NfL values were not quantitatively correlated with cerebral atrophy, but that correlation is well established in the literature [12, 25]. Another limit is the use of a semi-quantitative tool for assessing WMH burden, i.e., a visual scoring system, which is undoubtably not as accurate as a quantitative, volumetric method, although it is easy to implement in clinical practice. Finally, longitudinal studies, also including asymptomatic carriers, will be needed to definitely understand whether the presence of atypical leukopathy is a prognostic factor in GRN disease or simply a radiological marker with no practical impact.
In summary, NfL levels are higher in GRN carriers displaying atypical leukopathy, and they correlate with the global WMH burden. This likely results from more severe neurodegenerative process in this subgroup of GRN patients. Altogether, NfL levels in genetic FTD are linked not only to the causative genotype and the clinical phenotype, as already demonstrated, but also to specific neuroimaging profile, which should be taken into account to adapt pathological thresholds.
Footnotes
ACKNOWLEDGMENTS
We thank the DNA and cell bank of the ICM for the technical assistance, notably Sylvie Forlani (DNA and cell bank, ICM). The study was conducted with the support of the Centre d’Investigation Clinique Neuroscience (CIC 1422), Pitié-Salpêtrière Hospital, Paris.
FUNDING
The research leading to these results received funding from the Investissements d’Avenir ANR-11-INBS-0011. This work was partially funded by the Programme Hospitalier de Recherche Clinique (PHRC) Predict-PGRN (to ILB, promotion by Assistance Publique Hôpitaux de Paris).
CONFLICT OF INTEREST
JV, DS, SS, AC, KD, FC, FMH, FP have no conflict of interest to report. ILB served as a member of advisory board for Prevail Therapeutics, Alector, and received research grants from Pfizer ANR, DGOS, PHRC, ARSla Association, Fondation Plan Alzheimer outside of the present work.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
STUDY GROUPS
*The French clinical and genetic research network on FTLD/FTLD-ALS includes: Sophie Auriacombe (Pellerin University Hospital, Bordeaux), Serge Belliard (Rennes University Hospital, Rennes), Frédéric Blanc (Hôpitaux Civils, Strasbourg), Claire Boutoleau-Brétonnière (Laennec University Hospital, Nantes), Alexis Brice (Hôpital Pitié-Salpêtrière, Paris), Mathieu Ceccaldi (La Timone University Hospital, Marseille), Philippe Couratier (Limoges University Hospital, Limoges), Mira Didic (La Timone University Hospital, Marseille), Bruno Dubois (Hôpital Pitié-Salpêtrière, Paris), Frédérique Etcharry-Bouyx (Angers University Hospital, Angers), Maïté Formaglio (Lyon University Hospital, Lyon), Véronique Golfier (Rennes University Hospital, Rennes), Didier Hannequin (Charles Nicolle University Hospital, Rouen), Lucette Lacomblez (Hôpital Pitié-Salpêtrière, Paris), Julien Lagarde (Hôpital Sainte-Anne, Paris), Isabelle Le Ber (Hôpital Pitié-Salpêtrière, Paris), Richard Levy (Hôpital Pitié-Salpêtrière, Paris), Bernard-François Michel (Sainte-Marguerite University Hospital, Marseille), Jérémie Pariente (Toulouse University Hospital, Toulouse), Florence Pasquier (Lille University Hospital, Lille), Daisy Rinaldi (Hôpital Pitié-Salpêtrière, Paris), Carole Roué-Jagot (Hôpital Sainte-Anne, Paris), François Sellal (Colmar Hospital, Colmar), Christel Thauvin-Robinet (Dijon University Hospital, Dijon), Catherine Thomas-Antérion (Hôpital Plein-Ciel, Lyon), and Martine Vercelletto (Laennec University Hospital, Nantes).
**The Predict-PGRN study group includes: Mira Didic (La Timone University Hospital, Marseille), Nadine Girard (La Timone University Hospital, Marseille), Eric Guedj (Marseille University Hospital, Marseille), Michèle Puel (Toulouse University Hospital, Toulouse), Jérémie Pariente (Toulouse University Hospital, Toulouse), Isabelle Berry (Toulouse University Hospital, Toulouse), Pierre Payoux (Toulouse University Hospital, Toulouse), Martine Vercelletto (Laennec University Hospital, Nantes), Claire Boutoleau-Brétonnière (Laennec University Hospital, Nantes), Elisabeth Auffray-Calvier (Laennec University Hospital, Nantes), Amandine Pallardy (Laennec University Hospital, Nantes), Florence Pasquier (Lille University Hospital, Lille), Vincent Deramecourt (Lille University Hospital, Lille), Stéphanie Bombois (Lille University Hospital, Lille), Thibaud Lebouvier (Lille University Hospital, Lille), Adeline Rollin (Lille University Hospital, Lille), Gregory Kuchinski (Lille University Hospital, Lille), Didier Hannequin (Charles Nicolle University Hospital, Rouen), Olivier Martinaud (Charles Nicolle University Hospital, Rouen), David Wallon (Charles Nicolle University Hospital, Rouen), Emmanuel Gerardin (Charles Nicolle University Hospital, Rouen), Pierre Vera (Charles Nicolle University Hospital, Rouen), Daisy Rinaldi (Hôpital Pitié-Salpêtrière, Paris), Agnès Camuzat (ICM, Paris), Alexis Brice (ICM, Paris), Marie Chupin (ICM, Paris), Eric Bardinet (ICM, Paris), Aurélie Kas (Hôpital Pitié-Salpêtrière, Paris), Valérie-Causse Lemercier (Hôpital Pitié-Salpêtrière, Paris), Merry Masmanian (Hôpital Pitié-Salpêtrière, Paris), Hervé Oya (Hôpital Pitié-Salpêtrière, Paris).