
Abstract
Background:
Hyperuricemia in patients with gout is associated with a low risk of neurodegenerative diseases, including dementia. However, the prevalence of dementia in patients with gout has not yet been reported.
Objective:
To analyze the prevalence of dementia among patients diagnosed with gout by utilizing the Health Insurance and Review Assessment database, a nationwide registry of the South Korean population.
Methods:
Data from the Health Insurance and Review Assessment database of patients diagnosed with gout between 2011 and 2018 were extracted. The annual prevalence of dementia according to age and sex was analyzed. We investigated whether there was an association between comorbidities and gout medication in patients with both gout and dementia and in patients with only gout.
Results:
Between 2011 and 2018, the age-adjusted prevalence of dementia per 100,000 persons ranged from 54.0 (95% confidence interval: 47.7–60.2) to 69.9 (95% confidence interval: 65.3–74.5). Compared to previous studies, the prevalence of dementia was lower in patients with gout than in the general population. Patients with both gout and dementia were more likely to be women, have a wide range of comorbidities, and be prescribed gout-related drugs, including allopurinol, febuxostat, nonsteroidal anti-inflammatory drugs, and steroids than patients with gout without dementia.
Conclusions:
This study demonstrated a relatively low prevalence of dementia in patients with gout. Gout, characterized by hyperuricemia, might be associated with a reduced risk of dementia.
INTRODUCTION
Dementia is an irreversible deterioration in multiple cognitive domains, resulting in social or occupational activity impairment [1]. Extended life expectancy due to decreased mortality rates among people aged over 60 years and low fertility rates have led to population aging, resulting in an increased number of patients with dementia [2]. As a result, approximately 57.4 million people worldwide were reported to have dementia in 2019, and the number of patients with dementia is expected to double every 20 years, increasing to 152 million people in 2050 [3]. The estimated age-standardized prevalence of dementia in the population aged over 60 years, classified by regions, varies from 4.65% to 8.67% [2]. Meanwhile, between 2011 and 2015, the standardized prevalence of dementia in a South Korean population-based cohort of older adults (aged > 60 years) reportedly increased from 2,492.09 per 100,000 persons to 5,319.01 per 100,000 persons [4]. When estimating the prevalence of dementia in the general population using the diagnostic code within the Health Insurance and Review Assessment (HIRA) database, the standardized prevalence of dementia among patients aged≥65 years increased from 3.13% to 6.20% from 2008 to 2016 [5].
Gout is a chronic disease characterized by the deposition of monosodium urate crystals in articular and non-articular structures [6]. Elevated serum urate concentration (hyperuricemia) is a major risk factor for crystal formation [6]. Uric acid can function as both an antioxidant and pro-oxidant [7, 8]. The antioxidant effects of uric acid increase the lifespan and decrease the risk of cancer, whereas its pro-oxidant effects increase the risk of cardiovascular diseases [9]. With respect to neurodegenerative diseases, higher plasma uric acid levels are correlated with milder progression in diseases such as Parkinson’s disease (PD), amyotrophic lateral sclerosis, Huntington’s disease, and multiple system atrophy [10–13]. Lower uric acid levels are also associated with a greater risk of developing PD and Alzheimer’s disease [14–16]. However, whether the prevalence of neurodegenerative diseases demonstrates an inverse association in individuals with gout remains unclear. In a previous study, we examined the association between gout and the prevalence of amyotrophic lateral sclerosis and found a lower prevalence of amyotrophic lateral sclerosis in the gout group than in the general population [17].
In the present study, we aimed to investigate the prevalence of dementia in patients with gout. We used data from the HIRA database of the South Korean population to analyze the demographics of patients with gout with and without dementia. Furthermore, we determined the age-adjusted prevalence of dementia in patients with gout and compared this with previous reports on the prevalence of dementia in the general population.
MATERIALS AND METHODS
Data acquisition
The views expressed are those of the authors and do not necessarily those of HIRA or the Ministry of Health and Welfare. Data were based on the study dataset retrieved from the HIRA database, which contains de-identified health claims data for the entire Korean population. HIRA reviews the medical claims data transferred by medical institutions. Therefore, the HIRA database provides patient baseline information, International Classification of Diseases, 10th revision (ICD-10) diagnostic codes, and all medical data, including diagnostic tests and therapeutic approaches, such as drug prescriptions or surgery. We utilized the data collected between January 1, 2011 and December 31, 2018, from the HIRA database (M20200217325) to assess the demographics and comorbidities (as indicated by the Charlson comorbidity index [CCI] scores) of patients with gout and the medications administered to them.
Study population
Using the HIRA database, we identified 1,919,489 patients diagnosed with gout between 2011 and 2018 according to the Korean Classification of Disease 6th and 7th editions (M10.0 and M10.9). Of these, patients who visited a clinic on a single occasion were excluded from the study. All patients who fulfilled the abovementioned criterion were prescribed medications for gout. The index date for the patients with gout was defined as the first prescription date of a gout-related medication after visiting the clinic for gout on two occasions [18]. Medication for gout included allopurinol, febuxostat, colchicine, probenecid, selective and non-selective nonsteroidal anti-inflammatory drugs, and systemic and intra-articular steroids.
Dementia was defined as a claim with the ICD-10 diagnostic codes for Alzheimer’s disease (F00, G30), vascular dementia (F01), dementia in PD (F02.3), unspecified dementia (F03), frontotemporal dementia (G31.00–04), or dementia with Lewy bodies (G31.82) for the first or second diagnosis registered in the HIRA database between 2011 and2018 [5].
Ethical approval
This study was approved by the institutional review board of Guri Hospital, Hanyang University (2020-01-025). The study was registered with the Clinical Research Information Service (KCT0006241). The requirement for informed patient consent was waived owing to the use of publicly available and de-identified patient data.
CCI
The ICD-10 diagnostic codes for CCI, which include 17 diseases (acute myocardial infarction, congestive heart failure, peripheral vascular disease, cerebral vascular accident, dementia, pulmonary disease, connective tissue disorder, peptic ulcer, liver disease, diabetes, diabetes complications, paraplegia, renal disease, cancer, metastatic cancer, severe liver disease, and human immunodeficiency virus infection), were utilized in this study [19]. However, because all participants had dementia, the CCI score was determined by weighting the remaining 16 diagnostic categories. Supplementary Table 1 lists the weighted values and the related ICD-10 diagnostic codes.
Statistical analyses
Descriptive analyses were performed to determine the demographic characteristics of the participants. All individuals were classified and compared according to sex, age (seven groups: <60, 60–64, 65–69, 70–74, 75–79, 80–84, and > 85 years), and CCI (three groups: 0, 1–2, and 3 years). The annual crude prevalence of dementia between 2011 and 2018 was calculated by dividing the number of patients diagnosed with gout and dementia annually by the total number of patients diagnosed with gout in the same year. Its prevalence is indicated per 100,000 persons. The adjusted prevalence of dementia was also estimated and assessed over time. The mid-year population for 2008 in South Korea data were used to determine the age-adjusted prevalence of dementia. Furthermore, 95% confidence intervals (CIs) were calculated. The Annual percentage change (APC) in dementia prevalence was calculated using linear regression to estimate trends and 95% CIs. Statistical analyses were performed using the SAS software (version 9.3; SAS Institute Inc., Cary, NC, USA).
RESULTS
After excluding 660,706 patients who visited a medical institution only once for gout, 1,258,783 patients were included in the present study [17]. Medication for gout was prescribed to all patients. Among the 1,258,783 patients with gout, 4,410 were diagnosed with dementia. The demographics of the patients with gout with or without a dementia diagnosis are presented in Table 1. The mean age at the first diagnosis of gout was greater in patients with dementia than in those without dementia and this difference was significant (74.36±9.22 versus 51.94±15.48; p < 0.001). Moreover, patients with gout and dementia were more likely to be women than patients with gout without dementia (31.86% versus 18.87%; p < 0.001). The mean CCI score was higher in patients diagnosed with gout and dementia than in patients with gout without dementia (1.64 versus 0.48; p < 0.001). Except for connective tissue disease, severe liver disease, and human immunodeficiency virus, most CCI comorbidities were prevalent in patients with gout and dementia. While allopurinol, colchicine, and nonsteroidal anti-inflammatory drugs were frequently prescribed to patients with gout, allopurinol, febuxostat, nonsteroidal anti-inflammatory drugs, and steroids were more frequently prescribed to patients with dementia than to patients without dementia.
Demographic features and comorbidities in patients with gout with or without dementia between 2011 and 2018
Data are presented as mean±SD or number (%), if not indicated otherwise. MNDs, motor neuron diseases; CCI, Charlson comorbidity index; HIV, human immunodeficiency virus; NSAIDs, nonsteroidal anti-inflammatory drugs; SD, standard deviation. †Pearson’s chi-square and ‡Fisher’s exact tests were used.
Between 2011 and 2018, the total crude prevalence of dementia ranged from 121.3 to 198.5 per 100,000 persons (Table 2). The crude prevalence of dementia was highest in the groups aged > 85 years, whereas it was lowest in the group aged < 60 years (Fig. 1A). The overall crude and age-adjusted prevalence rates tended to increase over time (crude prevalence rate APC: 1.42%, 95% CI: 1.38%–1.46%; age-adjusted prevalence rate APC: 1.28%, 95% CI: 1.24%–1.32%; Table 2; Figs. 1A, B). The crude and age-adjusted prevalence rates of dementia were higher in women than in men (Fig. 1B, C). The prevalence of dementia, adjusted for age, ranged from 54.0 to 69.9 per 100,000 persons (Table 2 and Fig. 1C). Among the patients aged≥65 years, the age-adjusted prevalence increased from 380.2 per 100,000 persons in 2011 to 590.2 per 100,000 persons in 2018 (Table 2).
Annual prevalence of dementia in patients with gout
Age-adjusted prevalence using the mid-year population for 2008 in South Korea data. ‡CI for age-adjusted prevalence. CI, confidence interval.
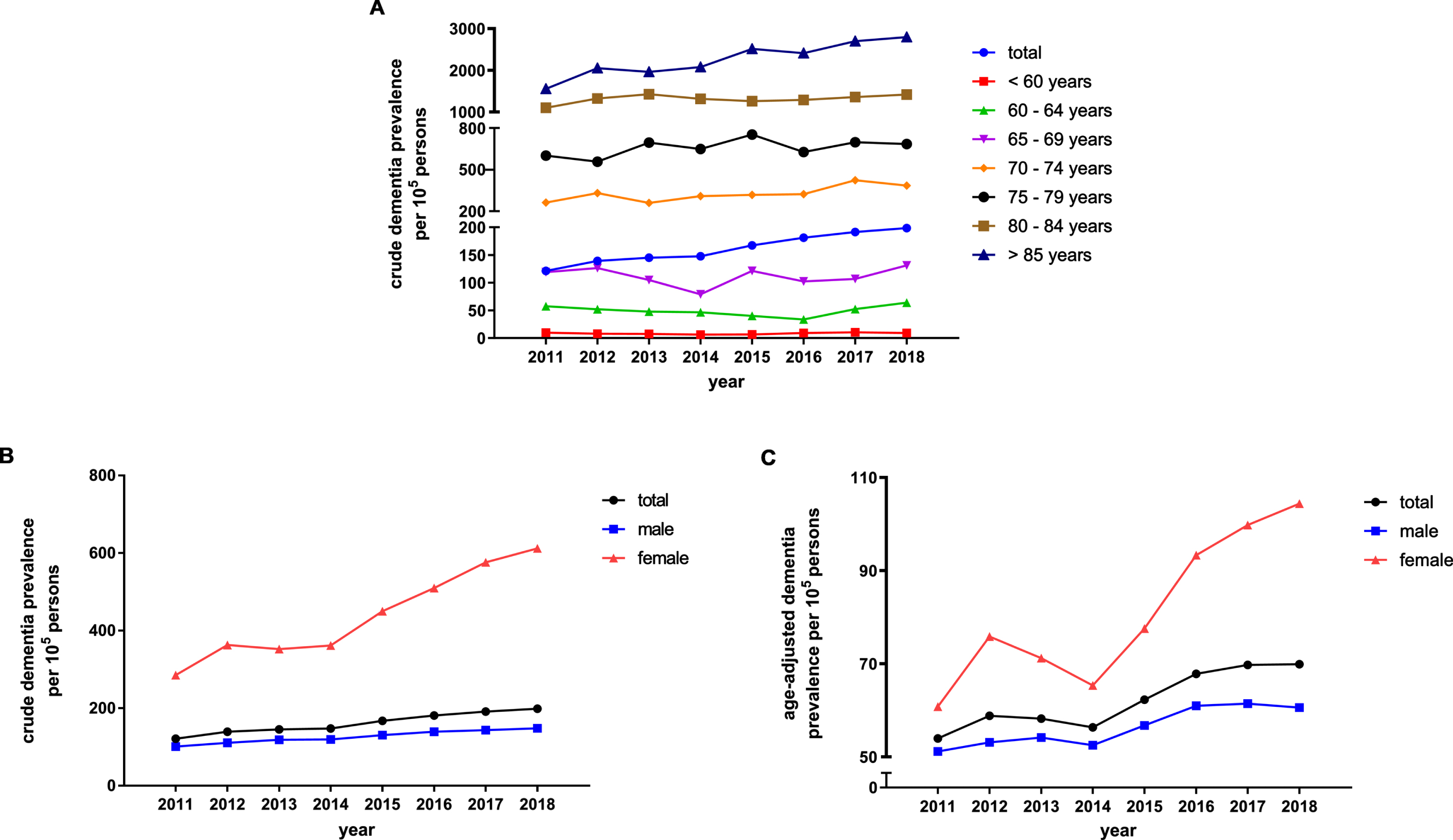
Annual prevalence of dementia in patients with gout. A) Crude prevalence of dementia stratified by age. B) Crude prevalence of dementia stratified by sex. C) Age-adjusted prevalence of dementia stratified by sex.
DISCUSSION
This study investigated the prevalence of dementia in patients with gout using data from the HIRA database, a nationwide population-based database of the entire Korean population. Between 2011 and 2018, the prevalence of dementia in patients with gout ranged from 121.3 to 198.5 per 100,000 persons. Among the patients aged≥65 years, the prevalence of dementia in gout patients ranged from 380.2 per 100,000 persons to 590.2 per 100,000 persons, revealing an upward trend. This prevalence was considerably lower than the prevalence of dementia in the general population aged≥65 years reported by a previous study using the same diagnostic codes and database (dementia prevalence ranging 5,046 to 7,218 per 100,000 persons between 2011 and 2016) [5]. Patients with gout with dementia were more likely to be women, had an older mean age at the first diagnosis of gout, and had a greater number of comorbidities than patients with gout alone.
When comparing the prevalence of dementia with that reported in a previous study using the same diagnostic criteria and database, the age-adjusted prevalence of dementia in patients with gout aged≥65 years was considerably lower than that of the general population aged≥65 years between 2011 and 2016 (380 versus 4,738 per 100,000 persons in 2011 and 574 versus 6,198 per 100,000 persons in 2016; Supplementary Table 2) [5]. Furthermore, the adjusted prevalence of dementia in participants > 60 years from a nationwide research database of the older population in Korea also presented higher rates than the age-adjusted prevalence in this study (339 versus 2,492 per 100,000 persons in 2011 and 333 versus 5,319 per 100,000 persons in 2015) [4]. Our finding is also consistent with that of a previous study that was based on the National Health Insurance Service-sample cohort database, demonstrating that gout reduced the incidence of dementia during follow-up (mean: 4.38 years) [20]. The prevalence of dementia in patients with gout in the present study was also lower that that calculated in a population-based epidemiologic study among participants aged≥65 years (prevalence of all-cause dementia: 12.3% in 2008 and 9.8% in 2017) [21]. However, a direct comparison of the results with those of the present study is difficult because of the different approaches used in analyzing dementia prevalence. Regarding the lower prevalence of motor neuron disease in patients with gout demonstrated in the previous study, hyperuricemia might have a reduced risk of neurodegenerative disease [17]. The present study also demonstrated an increasing trend in both crude and age-adjusted standardized prevalence rates of dementia in patients with gout, with rates of 1.42% and 1.28%, respectively. The same trend was observed in a previous study that determined the prevalence of dementia in Korea using the National Health Insurance System data [5]. The universal use of Long-Term Care Insurance programs for older people since 2008, the development of an accurate diagnostic process, and the increased sensitivity of dementia diagnosis could contribute to the rise in the prevalence of dementia [4, 22–24].
Uric acid, the end product of purine metabolism, is a natural water-soluble antioxidant that scavenges reactive oxygen species and secondary free radical intermediates such as peroxynitrite [7, 25]. Although the exact mechanism underlying the neuroprotective effect of uric acid related to its antioxidant properties is unclear, decreased serum uric acid levels are a risk factor for developing neurodegenerative disease [26]. In the context of dementia, studies investigating the association between various types of dementia and uric acid levels have presented contradictory results [27–29]. However, recent research suggests that increased uric acid levels may mitigate the risk of dementia, particularly the risk of Alzheimer’s disease and PD [30, 31]. The present study may contribute to elucidating the neuroprotective effect of hyperuricemia in patients diagnosed with dementia.
The onset age of gout in patients with dementia was 20 years more than the age at first diagnosis of all patients with gout. This could have resulted in higher CCI scores and a higher prevalence of comorbidities in patients with dementia and gout than in those with gout without dementia. Patients with gout and dementia are more likely to be women than the overall gout patient population, which may be due to the higher incidence of dementia in women [32, 33].
The present study had some limitations. First, dementia and gout diagnoses were determined on the basis of the claims database, which contains only diagnostic codes and medication history. Therefore, the prevalence described in this study may be an overestimate and should not be regarded as the real-world prevalence of dementia because of the exclusion of patients who did not visit the clinic. In addition, the higher prevalence of gout in men may have lowered the prevalence of dementia. Application of the appropriate diagnostic processes could not be validated in claims data analysis, which may result in sensitivity variation [34]. Second, in the present study, cases of mixed dementia, which constitute a sizable proportion of dementia cases, could not be investigated. Unfortunately, this is a common drawback of studies that rely on large databases that present only currently available diagnostic codes. Owing to these limitations, resulting in the uncertainty of the dementia subtype proportion, additional data regarding the type of dementia were not disclosed. Because demographic characteristics, prevalence, and comorbidities vary depending on the type of dementia, analyzing these data would have contributed to recognizing the distinctive relationship between each type of dementia and hyperuricemia [35].
Despite these limitations, analysis of the data from the HIRA database allowed the investigation of the epidemiological link between dementia and gout. The HIRA database provides a large sample of 1,258,783 people with gout between 2011 and 2018 and is representative of the entire South Korean population. The low prevalence of dementia in patients with gout highlights the protective effects of hyperuricemia against the risk of dementia.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.