
Abstract
After over 50 years of use, lithium-salts remain the first-line therapy for the management of bipolar disorder. Throughout this period, the potential for lithium salts has been extensively studied and numerous data favor its use in the treatment of neurodegenerative disorders such as Alzheimer’s disease (AD). We reviewed existing evidence gathered from clinical case reports and studies on the effect of lithium on neuropsychological symptoms of AD and as a disease-modifying treatment acting on cognitive symptoms. The review summarizes the molecular pathways, involving GSK-3β inhibition and neuroprotection, through which lithium is proposed to exert its effect. Limitations to its current use in AD are discussed and future perspectives as a potential treatment option for AD are considered in regard to ongoing clinical trials using different forms of lithium.
Keywords
Lithium salts (carbonate, citrate, or sulphate) for medicinal purposes began in the 1850 s with their use in the treatment of gout. Later in the 1950 s, P.C. Baastrup and M. Schou [1], supported by studies by J.F. Cade [2], first demonstrated lithium as an effective treatment for manic depressive illness, showing improvements in both manic and depressive symptoms in 70 to 80% of patients, making it the first medication specifically developed to treat bipolar disorder. Today considered as the “classic” mood stabilizer, lithium was the first to be approved by the US FDA, and remains the mainstay treatment of bipolar disorder, especially for acute mania and in maintenance treatment [3, 4]. In addition, as lithium appears to reduce the risk of suicide in patients with bipolar disorder [5], off-label use in patients with other mental disorders is not uncommon. Studies concerning the use of lithium revealed inhibition of glycogen synthase kinase 3 beta (GSK3β), an enzyme also involved in Alzheimer’s disease (AD) pathogenesis, as one of the underlying mechanisms. In this regard, numerous in vitro and in vivo experiments studied lithium in AD and its potential neuroprotective effect [6].
AD is characterized as a severe, chronic, and progressive neurodegenerative and incurable disorder, associated with memory loss and cognitive decline, accompanied by abnormal emergence of multiple neuropsychiatric symptoms (NPS), such as agitation and psychotic symptoms. Both cognitive impairment and NPS represent a major challenge in the medical management of patients, drastically impact the quality of life of both patient and caregiver and are a major cause of institutionalization. Lithium seems to offer dual benefits in AD, with a symptomatic effect on NPS and a disease-modifying effect on neurodegeneration.
LITHIUM USE IN ALZHEIMER’S DISEASE: TREATMENT OF NEUROPSYCHIATRIC SYMPTOMS
Literature on the use of lithium to treat NPS in AD is quite scarce. In 2017, Devanand et al. published a case series on the effect of lithium treatment on three AD patients with agitation and/or aggression [7]. Patients showing no response or a partial response to antipsychotics improved on lithium, as determined by clinical judgement and/or objective rating scales (Clinical Global Impression-Severity and -Change, and the Neuropsychiatric Inventory, NPI). Adverse effects were absent to tolerable at low oral doses (300–600 mg) with low serum levels at the final visit (0.30–0.32 mmol/L). These outcomes led to a Phase II placebo-controlled 12 week trial to further explore the efficacy and side effects of the same low dose lithium in the treatment of agitation/aggression with or without psychosis in 80 patients with AD [8].
Although lithium was not significantly superior to placebo in improving symptoms of agitation/aggression, with 31.6% of responders on lithium compared to 17.9% on placebo (χ2 = 1.26, p = 0.26), it did permit moderate or marked improvement in global Clinical Global Impression-Change in 10/38 = 36.8% of patients taking lithium compared to none of those taking placebo (0/39 = 0%, Fisher’s exact test p < 0.001). In addition, exploratory analyses showed greater improvements with lithium than with placebo in NPI scores for delusions and irritability/lability (ps < 0.05) [9]. It remains unclear whether narrowing to one NPS (agitation/aggression) could have impeded the observation of a more global positive effect of lithium. One interesting question warranting further investigation is whether a specific patient profile combining a particular set of NPS may benefit most from lithium.
LITHIUM USE IN ALZHEIMER’S DISEASE: DISEASE-MODIFYING TREATMENT
Hallmarks of neurodegenerative diseases, such as AD, include a decrease in neurogenesis and an increase in neurotoxicity. Several studies have been conducted both in vitro and in vivo to investigate a putative positive effect of lithium on neurogenesis and a neuroprotective effect that could be translated into it being considered as a therapeutic option for dementia.
A Danish epidemiological study in an observational cohort explored the effect of continuous use of lithium on the incidence of dementia. They identified a sample of 16,238 individuals who purchased lithium at least once and a further 1,487,177 from the general population who did not purchase lithium, acting as control. They observed that lithium administration lowered the risk of dementia [10]. They also investigated a possible association between lithium treatment in patients with mania or bipolar disorder and subsequent dementia. They reported that continued treatment with lithium was associated with a reduced rate of dementia in contrast to continued treatment with anticonvulsants, antidepressants, or antipsychotics [11].
Macdonald et al. [12] conducted a pilot study assessing the feasibility and tolerability of lithium carbonate at therapeutic levels (targeted serum levels between 0.3 and 0.8 mM) in mild to moderate AD over an extended period (up to one year). This open label observational study enrolled 22 patients, of which 8 completed the full year of therapy. 21% withdrew treatment due to adverse events, 21% due to investigator’s decision. High rate of discontinuation, outside of the ones due to adverse events, seems to be influenced by change in concomitant treatment leading to contraindication and/or loss of compliance to study procedure or study drug. Interestingly, no serious adverse event nor irreversible events related to treatment were encountered during the trial. Side effect appeared to be mild and those estimated to be due to lithium were not the cause of withdrawing in most of the cases.
Hampel et al. [13] conducted a placebo controlled trial on the effect of 10 weeks lithium treatment in 71 mild AD patients (Mini-Mental State Examination (MMSE) score > or = 21 and < or = 26). The 10-week treatment included a 6-week titration phase to reach the target serum level of lithium (0.5–0.8 mmol/L). The treatment showed no effect on GSK3β activity in lymphocytes or cerebrospinal fluid-based biomarker concentrations (p-tau, total tau, and Aβ1 - 42; p > 0.05), on global cognitive performance as measured by the Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog) (p = 0.11) or on depressive symptoms (NPI score). However, in a second analysis of this trial, Thomas et al. observed a significant increase in BDNF serum levels and a significant decrease in ADAS-Cog scores among patients in the lithium treated group in comparison to placebo-treated patients and found a correlation between outcome and serum lithium concentration. Noteworthy is the cognitive improvement (ADAS-Cog increase >4 points) that was observed in 28.6% of lithium-treated patients versus 14.3% of the placebo group, although this difference did not reach statistical significance [14].
Forlenza et al. [15] evaluated the effect of long-term lithium treatment on cognitive and biological outcomes in patients with amnestic mild cognitive impairment (MCI) in a 2-year double blinded, randomized, controlled trial followed by a single blinded extension phase for an additional 24 months. In an interim analysis at 12 months of treatment for 45 patients (24 received lithium (0.25–0.5 mmol/L)), study group reported that lithium treatment was associated with a reduced cognitive decline and significant decrease in p-tau (p = 0.02) compared to placebo. In the final analysis [16], 61 patients were randomized to receive either lithium (50.8%) or placebo (49.2%), of these 52 completed the double blinded phase and 40 completed extension phase. Over 24 months, patients treated with lithium were cognitively and functionally stable, whereas patients treated with placebo had statistically significant cognitive and functional decline on ADAS-Cog and CDR-SoB scores. There was a trend toward a lower conversion rate from MCI to dementia in patients treated with lithium compared to placebo. Overall tolerability and adherence were good. The same team re-assessed the global cognitive and functional state of the patients enrolled in the initial trial 11 to 15 years later [15]. Of the 36/61 participants the team was able to reach, 22 had received lithium and 14 placebo. They found statistically significant differences in MMSE score and a better performance in the phonemic verbal fluency test for patients having previously received lithium [17].
Nunes et al. [18] evaluated over a 15-month period the effect of daily administration of micro-dose of lithium (300μg) on patients with AD. The lithium-treated group showed no decreased performance on the MMSE test in contrast to lower scores observed for the control group, with differences becoming significant from three months of treatment and increasing progressively.
In 2014, Mauer et al. [19] conducted a systematic review on twenty-four clinical, epidemiological, and biological reports assessing lithium at standard or low doses for dementia or other behavioral or medical purposes. They reported that most studies on lithium at standard doses showed notable cognitive benefits or effectiveness in preventing dementia.
Included epidemiological studies were numerous, large, and replicated and the randomized controlled trials also showed clear biological and/or clinical benefits. Aligned with these outcomes, Matsunaga et al. [20] conducted a meta-analysis of randomized placebo-controlled trials testing lithium as a treatment for patients with AD and/or individuals with MCI (3 clinical trials, 232 participants). They reported that lithium treatment appeared to be associated with significant decrease in cognitive decline as compared to placebo (standardized mean difference = –0.41, 95% confidence interval = –0.81 to –0.02, p = 0.04, I2 = 47%).
MECHANISM OF ACTION OF LITHIUM IN AD
Lithium is the smallest and lightest solid element and yet it has a wide diversity of effects. Proposed pathways involved in the pleiotropic pharmacological effects of lithium in neurodegenerative disorders such as AD illustrates the different mechanisms underlying the observed efficacy of lithium (Fig. 1).
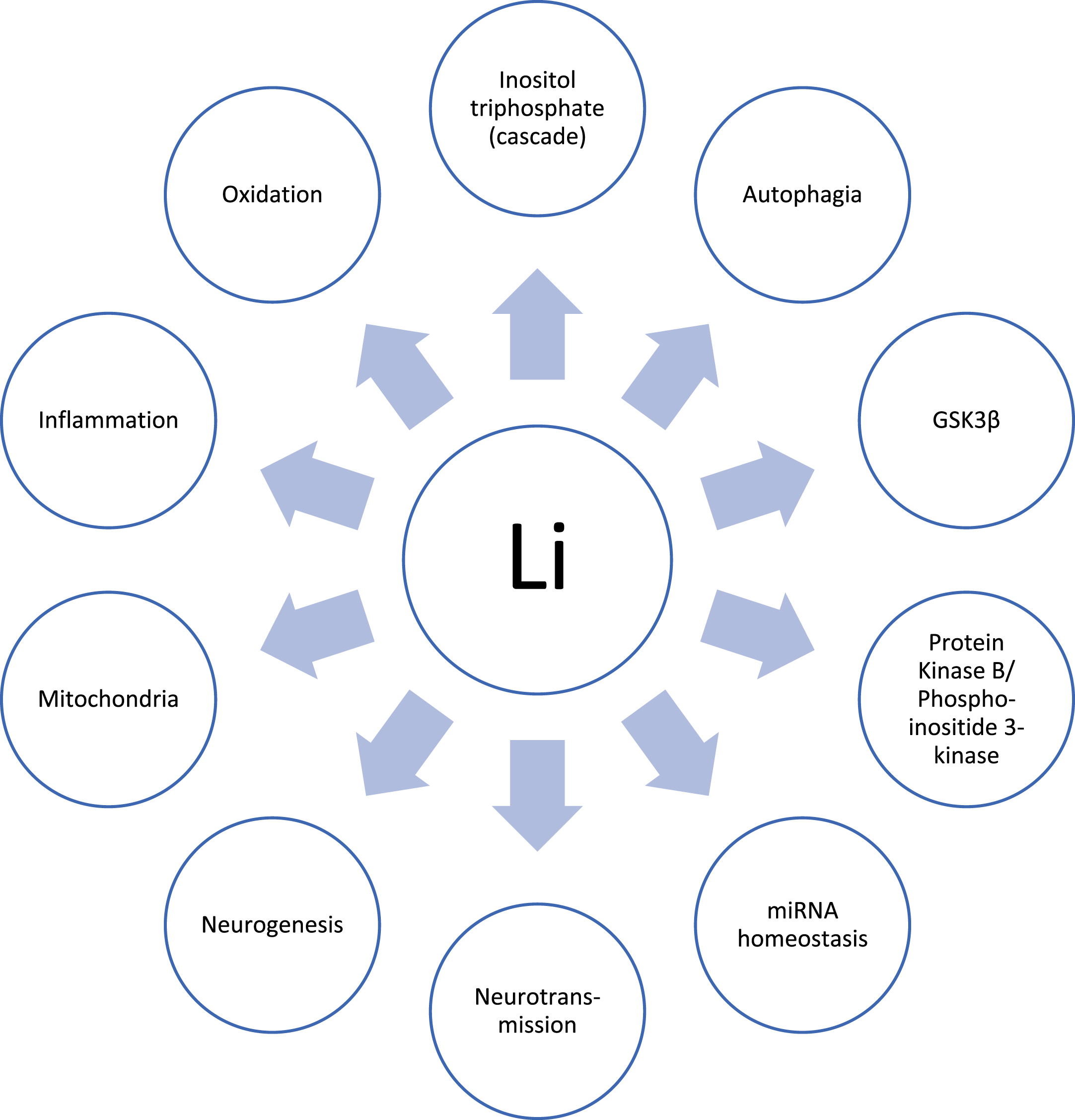
In vitro and in vivo studies have identified several pathways through which lithium exerts its effects.
In AD-specific pathways [6 , 21–23]:
Lithium acts as an inhibitor of the enzyme GSK3β implicated in AD pathogenesis via its role in tau hyperphosphorylation, neuroinflammation, oxidative stress, apoptosis, and modulation of gamma-secretase and beta-secretase both required for the production of Aβ protein. It reduces beta-secretase-1 (BACE1) hyperactivity which in turn diminishes the production of Aβ protein. The unexpected negative clinical effect obtained from inhibiting BACE1 in patients could be explained by the need to fine-tune the inhibition of this enzyme rather than completely block it. It also prevents tau phosphorylation though inhibition of kinases, including GSK3β, although it appears that it is not able to act on tau already aggregated within neuro fibrillary tangles.
Lithium also acts on disease nonspecific pathways: Inhibition of oxidative stress and the inflammatory cascade following lithium treatment can be observed with an increase in antioxidants and a decrease in lipid peroxidation, free radicals, inflammatory cytokines and microglia activation [21
, 24]. By stimulating the synthesis and release of neurotrophic factors (BDNF, neurotrophin-3, vascular endothelial growth factor [21
, 24]), lithium activates neurotrophic responses and has neuroprotective effects. Lithium reduces excitatory (dopamine and glutamate) but increases inhibitory (γ-aminobutyric acid) neurotransmission; however, these broad effects are undermined by complex neurotransmitter systems striving to achieve homeostasis by way of compensatory changes [21, 24]. It improves mitochondrial function by increasing mitochondrial biogenesis, activating the mitochondrial respiratory chain, and increasing the regulation of mitochondrial DNA [23, 24]. By lowering the levels of inositol 1,4,5- trisphosphate, lithium induces autophagia [21
, 25]. It also has an anti-apoptotic effect through inositol 1,4,5-trisphosphate/protein kinase B, B-cell lymphoma 2, and mitogen-activated protein kinase pathways [21
, 26–28].
This broad spectrum of lithium actions could explain the positive results observed in animal models with regards to AD biomarkers and cognitive improvement.
LIMITATIONS TO CURRENT USE OF LITHIUM IN AD
Lithium is a monovalent cation that shares certain properties with sodium, potassium, and calcium. The active agent in lithium salts is the lithium-ion Li+, which having a smaller diameter, can easily displace K+ and Na+ and even Ca2 + from important enzyme or neurotransmitter receptor sites [29]. The safety profile of lithium and its well-known narrow therapeutic index are directly correlated to its circulating concentration and cell penetration mechanisms.
In the treatment of bipolar disorder, the administered daily dose varies between 500 mg and 1,250 mg of lithium carbonate (10–20 mEq/day). To cross cell membranes, lithium uses mainly the sodium pump, sodium leak channel, and sodium-lithium counter transporter.
All these systems involve other cations and require a certain circulating concentration (>0.5 mEq/L varying between subject) in order to shift the transport towards getting lithium inside the cells in accordance with the pharmacokinetics plateau principal [29 –32].
Signs of lithium toxicity are tremor, ataxia, dehydration, nystagmus, renal impairment, confusion, and convulsion. They are mostly observed at blood concentrations >1.5 mEq/L [30 –32].
The narrow therapeutic index of lithium, between 0.6 and 1.2 mEq/L, imposes the routine monitoring of its serum concentrations: serious toxicity can be observed at concentrations exceeding 1.5 mEq/L. The maintenance level is between 0.4 and 0.8 mEq/L [30, 32].
Lithium has no clinically important protein binding properties and no metabolites. It is excreted almost entirely by the kidneys, although small amounts are also lost in sweat and feces. A substantial amount of filtered lithium is reabsorbed (primarily in the proximal tubules), explaining an observed five-fold higher renal clearance rate of creatinine compared to lithium [32]. The elimination half-life of lithium is about 18 to 24 h, although it is considerably longer in the elderly because of the age-related decrease in glomerular filtration rate (and correspondingly shorter in young patients). Lithium is not liver metabolized [30].
As a direct consequence of lithium’s pharmacokinetic profile, any conditions affecting circulating concentration (sodium depletion, dehydration) can trigger its toxicity. All adverse events are positively correlated with dose and duration of exposure and are usually reversible with a dose decrease or by discontinuing treatment. Long-term adverse effects on the thyroid, parathyroid gland and kidney are observed with continuous high-dose treatment. Tolerance may be low in some patients due to the moderate side effects, including gastrointestinal symptoms such as dyspepsia, nausea, vomiting, and diarrhea, as well as weight gain, hair loss, acne, tremor [29, 32].
Lithium as a therapeutic agent in neurodegenerative diseases other than AD has also been widely studied, particularly in Huntington’s disease, dementia other than AD, Parkinson’s disease, Alexander’s disease, Down syndrome, Kleine-Levin syndrome, fragile×syndrome, amyotrophic lateral sclerosis, Machado-Joseph disease, and prion disease [6]. In most of these clinical investigations, lithium was administered at a dose ranging from 150 to 1200 mg per day which can lead to serious side effects, including renal toxicity. Results have increased toxicity awareness and a desire to develop low dose lithium formulations to provide therapeutic efficacy without side effects. A certain number of research groups [9 , 19] have studied the effect of micro doses of lithium in the treatment of neurodegenerative disease and observed very good long-term tolerance. Clinical trials aiming to demonstrate the efficacy of low dose lithium in the treatment of AD, used doses between 150 and 600 mg/day targeting a circulating concentration of 0.25–0.8 mEq/L.
The narrow therapeutic index being difficult to manage in clinical practice led to a general decrease in lithium use, particularly in frail patient populations such as the elderly, often more subject to renal disorders, polypharmacy, and dehydration and therefore more sensitive to lithium toxicity [33]. On the other hand, the narrow therapeutic index could also explain some inconsistency in the positive outcomes observed with lithium in neurodegenerative diseases, as the use of a micro dose that fell just below the plateau would preclude the pharmacological benefit.
ONGOING STUDIES ON THE USE OF LITHIUM IN ALZHEIMER’S DISEASE
Lithium still holds great promise in the treatment of neurodegenerative diseases and its potential benefits for AD continue to motivate researchers and pharmaceutical companies in their investigations:
NanoLi-AD [34]: Clinical safety and efficacy evaluation of NanoLithium® NP03 in patients with mild-to-severe Alzheimer’s disease
Nanolithium is a new investigational product based upon the Aonys® technology developed by Medesis Pharma [35 –38]. Encapsulating lithium within Aonys® confers a different absorption and distribution profile to lithium. Using the buccal route, Nanolithium passes through the oral mucosa and is transported in the systemic circulation in its protected form in high density lipoproteins (HDL). Lithium is then released as an ion (Li+) inside cells via the lipoprotein receptor (s.a. SR-B1) expressed ubiquitously and notably on the blood-brain barrier [39].
Use of this cell penetration mechanism bypasses voltage-dependent ion channels and enables pharmacological activity at doses largely inferior to those needed with classical lithium solution. The lower circulating dose permitted with Nanolithium in turn results in much reduced toxicity rates. The benefit of Nanolithium has been demonstrated in animal models of AD [40 –42]. Globally, it appeared that Nanolithium administration at a concentration of 0.04 mg Li/kg (0.0058 mmol/kg) reduced key aspects of early and late AD amyloid pathology. Effect on neuroprotection observed with classical lithium were at a dose of 0.24 to 121.44 mmol/kg, so 40 to 20,000 times the dose used with Nanolithium. Initiated both during the early and late amyloid pathological stages, study evidenced that Nanolithium reduces overall brain amyloid burden, early and late neuroinflammation, oxidative damage, inhibits GSK3β and provides preservation of cognition by enhancing multiple aspects of neuroplasticity and neuroprotection. The cognitive benefits were observed with Nanolithium treatment during the early and late amyloid pathological stages.
Nanolithium is currently being studied in phase II prospective, multicenter, randomized (1:1), placebo-controlled, parallel-group trial, with a double-blind period followed by an open-label trial period. The objectives are to demonstrate the efficacy of Nanolithium on NPS associated with AD (primary endpoint) over a 12-week period and to explore the disease-modifying potential over a year (48 weeks) with regards to biomarkers, neuroimaging, and cognitive outcomes. A daily dose of 1.8 mg of Li+ is being used, 68 patients have been enrolled so far and a first set of results are anticipated in the second half of 2023. This study will provide additional insight into the efficacy of lithium in AD patients and could highlight Nanolithium as a new therapeutic option for symptomatic AD and potentially as a disease-modifying treatment [43].
AL001 (aka LISPRO® [44])
AL001 is a crystal-engineered combination of lithium-salicylate-proline being studied for the therapeutic delivery of lithium in AD, frontotemporal dementia, and bipolar disorder. Pharmacokinetic studies have indicated that AL001 treatment provides significantly higher brain levels and more stable plasma levels of lithium in both normal and transgenic Alzheimer’s- like mice when compared to lithium carbonate. In another study, AL001 treatment was shown to prevent cognitive deficits, depression, and irritability in a mouse model of AD (APPSWE/PS1dE9 transgenic mice).
Treatment with AL001 was superior in preventing associative memory decline, as determined by contextual fear conditioning, and in reducing irritability, as determined by a touch escape test, in comparison with classical lithium salt. All salts were effective in preventing spatial cognitive decline and depression-like behavior [45].
The ongoing Phase I/IIa, multi-center, placebo-controlled, double-blind, randomized, multiple ascending dose clinical trial aims to determine the safety and maximum tolerated dose of AL001.
A maximum of approximately 72 participants will be enrolled. Participants are being randomly assigned to receive the studied drug (active AL001) or placebo in a ratio of 6:2, respectively, with 8 patients in each dose cohort made up of a mix of healthy non-elderly and elderly subjects, and AD subjects. The study includes a 14-day treatment period and a 42-day follow-up period.
The first part of the study was completed in 2022 and results indicate the bioequivalence of AL001 at 150 mg dose and the marketed 300 mg dose of lithium carbonate, as well as the similarity in the shapes of the lithium plasma concentration versus time curves. Also encouragingly, AL001 plasma concentrations were observed to be well-tolerated and consistently within safe limits. So far, the safety profiles of both AL001 and the marketed lithium carbonate capsule have been benign. Outcomes from the next phase of the study are expected in the second half of 2023 [46].
LATTICE Study [47]: Lithium as a treatment to prevent impairment of cognition in elders
This is a phase IV pilot-feasibility study initiated in 2017, examining the potential disease-modifying properties of lithium in individuals with MCI expressed as a delay in conversion to dementia. The study was to enroll and randomly assign 80 individuals 60 years and older with MCI to take lithium, titrated to a maximally tolerated blood level (0.5 to 0.8 mEq/L), or placebo for two years, in order to assess the effect of lithium on preserving cognition and delaying conversion to dementia.
Participants were to receive annual neurocognitive assessments, blood- and cerebrospinal fluid-based biomarker measurements, and 7T MRI of structural brain volumes (e.g., hippocampal, total cortical gray). Coprimary endpoints assessed over 2 years are change from baseline in cognitive testing measurements, biomarker levels (GSK-3β activity, BDNF) and brain volume values measured by structural imaging (7T MRI) including total volume, grey and white matter volume, and regional volumes. Inclusion criteria are patients 60 years or older diagnosed with MCI. Baseline measurements include positron emission tomography imaging for Aβ in all able subjects. No outcomes from this study have yet been reported.
CONCLUSIONS AND CLINICAL PERSPECTIVES [6 , 48–50]
An estimated minimum of 55 million people worldwide currently suffer from dementia and this number is set to rise to 139 million by 2050. AD is the most commonly diagnosed form of dementia, accounting for an estimated 60% to 80% of cases. NPS, even at early stages of the disease, are the most disruptive aspect for patients, caregivers, and healthcare systems, for which there remains no safe and efficacious drug treatment. This represents an urgent unmet need, particularly when research suggests that interventions to reduce or eliminate AD could significantly reduce the prevalence of dementia in coming decades, and that even a modest delay in disease onset could generate billions in savings to society. The pathophysiology of AD initially involves the misprocessing of amyloid precursor protein leading to the creation of toxic peptides that assemble into oligomers themselves forming deposits or plaques over time, ultimately leading to synaptic degeneration and the emergence of tau phosphorylation inside neurons. Eventually sufficient loss of neurons leads to dysconnectivity in key cognitive networks and the emergence of symptoms. Targeting amyloid protein has been the field of focus and yet despite over two decades of extensive research and investment in AD therapeutic development, only two therapeutics have come to market.
The two anti-amyloid therapies recently approved in the United States offered a maximum 25% slowing of decline, enough to give study participants a few extra months of independent living. Both must be infused and require close monitoring due to the potentially life-threatening amyloid-related imaging abnormalities. These successful developments represent a pivotal milestone for AD treatment research. Results so far suggest that these anti-amyloid therapies appear most likely to impact a certain subset of patients if delivered early enough, thereby highlighting the need for earlier diagnosis and proper patient identification. Considering the involvement of numerous intertwined pathways beyond and independent of amyloid accumulation in AD pathophysiology, it seems likely that anti-amyloid therapies will be used in combination with other drugs developed in the future to tackle different stages of the disease. While it is still too early to assess the impact of the monoclonal amyloid antibodies on daily clinical practice in early AD, it is now possible to design clinical trials where patients are first treated with a monoclonal amyloid antibody, then randomized to an anti-tau agent. This type of combination therapy in sequence is being tested in the DIAN (Dominantly Inherited Alzheimer Network) cohort, using an anti-tau antibody [51]. Other putative anti tau agents such as lithium salts could be considered in future clinical trials.
Administration of lithium-salts for the treatment of psychiatric disorders has now exceeded nine decades in the history of medicine. Its safety profile, although complex, has been well studied and optimized. The multimodal action of lithium in AD detailed above allows it to impact a variety of pathophysiological mechanisms (prevention of Aβ accumulation, prevention of Tau phosphorylation, anti-inflammatory effect, etc.) ultimately achieving a certain homeostasis and finely-tuned dysregulation of the AD disease cascade.
In this literature review, we have outlined the potential of lithium as a therapeutic option in AD, for the treatment of neuropsychological symptoms and as a potential disease-modifying treatment. However, the clinical translation of this potential has yet to be achieved. The challenges and limitations imposed by the narrow therapeutic index, especially in the elderly population with dementia, have greatly impacted its broader development in neurodegenerative disorders. However, the interesting new approaches discussed in this paper could overcome these obstacles. It appears that in order to clearly demonstrate a disease-modifying potential of lithium, a year-long treatment initiated early in the disease course and using micro doses to avoid long term toxicity would be needed. The lack of evidence of a clear benefit on NPS, could be explained by a need to properly identify the set of NPS that might most benefit from lithium treatment.
Precision medicine, also known as personalized medicine, is concerned with finding the right treatment for the right patient at the right time. Recent developments in profiling patients based on their NPS with mild behavioral impairment criteria suggests [48] that it might represent a good novel marker of preclinical disease. Perhaps a subset of patients with early disease and NPS would benefit most from lithium treatment. Lithium would also represent a good candidate for combination therapy, as it targets different mechanisms to those targeted by the anti-amyloids; especially with the optimized formulations developed, bypassing the metabolism pathways source of to drug-drug interaction.
Lithium clearly has a future in AD therapeutics but in order to develop to its full potential it will be necessary to overcome long-standing misbelief surrounding its safety profile and rigorously exemplify the benefits.
Footnotes
ACKNOWLEDGMENTS
We would like to acknowledge Philippine Marce, employee of Medesis Pharma for the editorial support.
FUNDING
English language editing service has been provided by Medesis Pharma.
CONFLICT OF INTEREST
S. Guilliot is an employee of Medesis Pharma.
S. Gauthier is a paid member of the scientific advisory board of Medesis Pharma.
J. Touchon participates in paid Scientific Advisory Board for Medesis Pharma, Ariana Pharma, Regenlife; has stock options in Regenlife; and receives fees from Regenlife.
M. E. Soto receives consulting fees and participates in paid advisory boards for Medesis Pharma, Acadia, Eisai, Biogen.