
Abstract
Background:
Apolipoprotein E (APOE) is the most recognized risk gene for cognitive decline and clinical progression of late-onset Alzheimer’s disease (AD); nonetheless, its association with neuropsychiatric symptoms (NPSs) remains inconclusive.
Objective:
To investigate the association of APOE ɛ4 with NPSs and explore nutritional status and cognition as joint mediators of this association.
Methods:
Between June 2021 and October 2022, patients with amnestic mild cognitive impairment (aMCI) or AD were recruited from the Chinese Imaging, Biomarkers, and Lifestyle Study. NPSs were assessed using the Neuropsychiatric Inventory, while global cognition and nutritional status were evaluated using the Mini-Mental State Examination (MMSE) and Mini-Nutritional Assessment (MNA), respectively. Simple mediation and multiple chain mediation models were developed to examine the mediating effects of the MNA and MMSE scores on the relationship between APOE ɛ4 and specific neuropsychiatric symptom.
Results:
Among 310 patients, 229 (73.87%) had NPSs, and 110 (35.48%) carried APOE ɛ4. Patients with APOE ɛ4 were more likely to have hallucinations (p = 0.014), apathy (p = 0.008), and aberrant motor activity (p = 0.018). MNA and MMSE scores mediated the association between APOE ɛ4 and hallucinations (17.97% and 37.13%, respectively), APOE ɛ4 and apathy (30.73% and 57.72%, respectively), and APOE ɛ4 and aberrant motor activity (17.82% and 34.24%), respectively. Chain-mediating effects of MNA and MMSE scores on the association of APOE ɛ4 with hallucinations, apathy, and aberrant motor activity after adjusting for confounding factors were 6.84%, 11.54%, and 6.19%, respectively.
Conclusion:
Nutritional status and cognition jointly mediate the association between APOE ɛ4 and neuropsychiatric symptoms in patients with aMCI or AD.
Keywords
INTRODUCTION
Apolipoprotein E allele 4 (APOE ɛ4) remains the strongest and most established genetic risk factor for sporadic Alzheimer’s disease (AD), which has been linked to amyloid-β peptide aggregation, tau neurofibrillary degeneration, microglia and astrocyte responses, and blood-brain barrier disruption [1, 2]. These pathological processes may contribute to cognitive impairment; however, the association of APOE ɛ4 with neuropsychiatric symptoms (NPSs) remains inconclusive and unclear [3]. A prospective study that followed up with 332 older patients with mild cognitive impairment (MCI) found additive interactions between APOE ɛ4 and depression and between APOE ɛ4 and apathy [4]. Further, a 1-year follow-up study found that APOE ɛ4 was associated with psychosis in patients with AD [5]. However, a previous longitudinal study failed to show any association between APOE alleles and NPSs in patients with AD [6]. A retrospective cohort of 463 patients with NPSs and AD demonstrated that the total and subscale Neuropsychiatric Inventory (NPI) scores were similar between patients with different APOE haplotypes [7]. The variable findings in the existing studies can be explained by differences in patient populations, lack of statistical power to detect potential mediation, interaction, regulatory effects of the associations in the studies with negative results, and small sample sizes generating false positives that cannot be consistently replicated [8].
Accumulating evidence suggests that nutritional status can affect AD-related pathological changes, cognition, and progression [9, 10]. ApoE protein, the major lipid and cholesterol carrier in the central nervous system, has been shown to affect lipid and glucose metabolism or related pathways in the pathogenesis of AD [11]. A previous animal study found that APOE-knock-out mice failed to show growth catch-up after refeeding and presented a high risk of malnutrition [12]. With increasing attention being paid to the effect of nutrition on AD, several recent studies have focused on investigating the association between NPSs and nutritional status. A longitudinal study demonstrated that poor nutritional status increased the severity of NPSs, especially aggression and disinhibition, in women with MCI and early-stage AD during a 2.5-year follow-up period [13]. Another observational study found that malnutrition was associated with individual NPSs among older adults with MCI [14].
Additionally, existing evidence has made it clear that APOE ɛ4 is related to the risk of AD, conversion from MCI to dementia, and the age of onset of cognitive impairment [15]; a recent study also demonstrated that APOE ɛ4 carriers contributed to faster Mini-Mental State Examination (MMSE) score decline than APOE ɛ3/ɛ3 carriers [16]. Cognitive decline as a risk factor for the development of NPSs requires further investigation. For instance, a longitudinal cohort study revealed that abnormal motor behavior was significantly correlated with cognitive deterioration (p = 0.03) [17]. Moreover, a cross-sectional analysis found that patients with AD and apathy had worse cognitive performance than those without apathy [18]. In line with the abovementioned evidence, nutritional status and cognition may be related to the association between APOE ɛ4 and NPS. However, limited evidence exists regarding the mediating effects of nutrition and cognition on the association between APOE ɛ4 and NPSs, especially in studies with negative findings. Thus, this study aimed to investigate the association between APOE ɛ4 and NPSs and examine the extent to which the effect of APOE ɛ4 on specific NPS is mediated by nutritional status and cognition in patients with amnestic MCI (aMCI) or AD.
METHODS
Standard protocol approvals, registrations, and patient consents
The data used in this study were acquired from the Chinese Imaging, Biomarkers, and Lifestyle (CIBL) Study (chictr.org.cn, identifier: ChiCTR2100049131). The CIBL study is an ongoing large-scale prospective cohort study that aims to evaluate the risk factors, biomarkers, and neuroimaging findings of individuals with AD in the Chinese population. The CIBL study was approved by the Institutional Ethical Review Board of Capital Medical University, Beijing Tiantan Hospital (number: KY-2021-028-01). All participants or their caregivers (if necessary) provided written informed consent.
Design and subjects
This study recruited patients with aMCI or AD at baseline from the CIBL study between June 1, 2021, and October 31, 2022. The inclusion criteria were 1) patients aged 50–90 years; 2) patients with AD, who had its onset after 60 years and met the 2011 or 2018 National Institute on Aging Alzheimer’s Association workgroup diagnostic criteria for probable AD or confirmed AD [19, 20]; and 3) patients with aMCI who were diagnosed based on Petersen’s diagnostic criteria for aMCI including a memory complaint verified by an informant, preserved performance in activities of daily living, and absence of dementia [21]. Patients were excluded if they 1) had core features of other central neurodegenerative diseases, such as dementia with Lewy bodies, frontotemporal dementia, or Parkinson’s disease; 2) had concomitant central nervous system diseases that could cause cognitive impairment, such as cerebrovascular disease, tumor, encephalitis, and epilepsy; 3) had a history of a mental disorder, including bipolar disorder and schizophrenia, in accordance with the Diagnostic and Statistical Manual of Mental Disorders-5 [22]; 4) presented with cognitive impairment due to traumatic brain injury; 5) had a history of alcohol or drug abuse or exposure to toxic environments within the past 2 years; or 6) had systemic diseases, such as syphilis or human immunodeficiency virus infection. Figure 1 presents a detailed flowchart of the inclusion and exclusion processes.
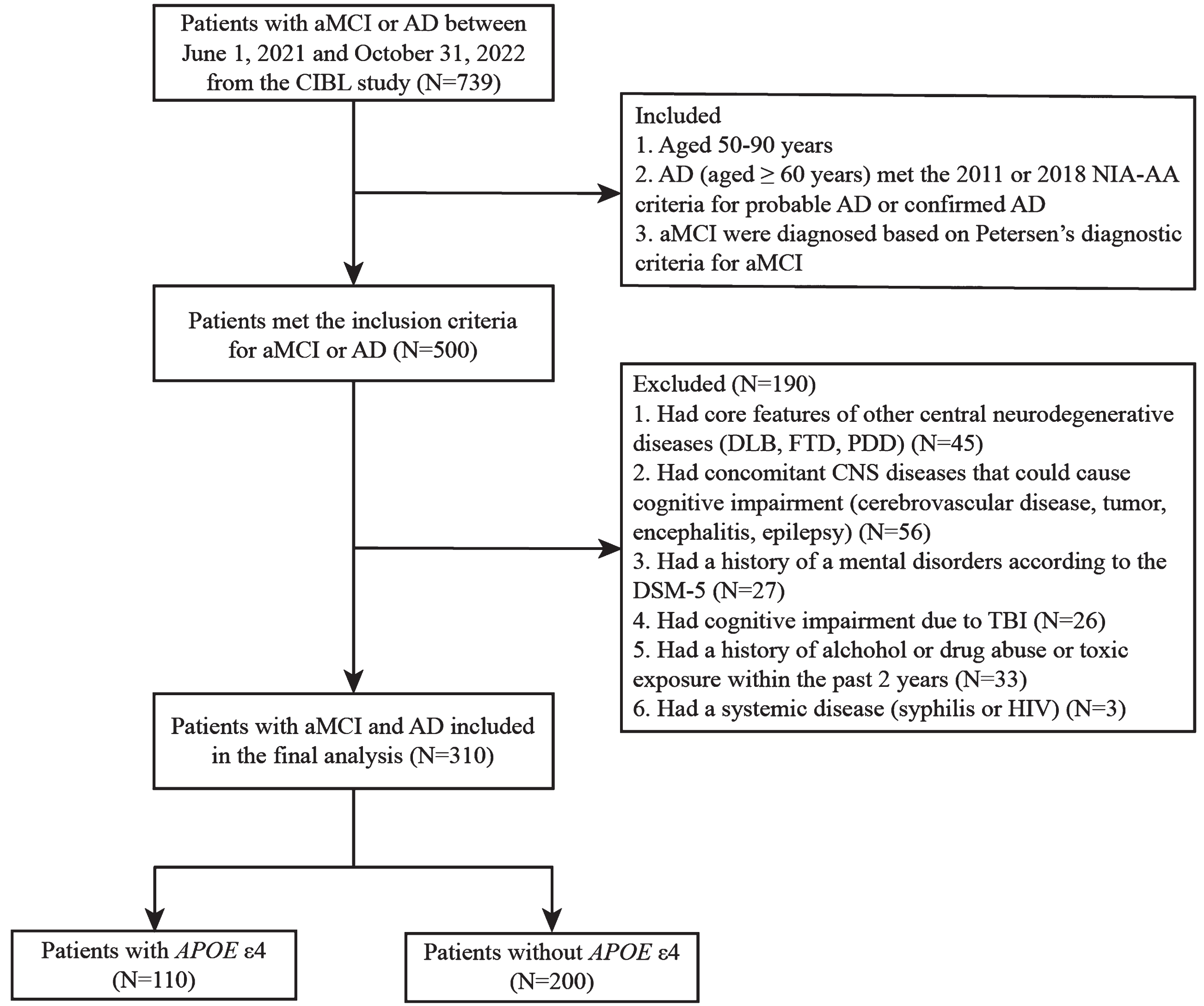
A detailed flowchart of the inclusion and exclusion processes. aMCI, amnestic mild cognitive impairment; AD, Alzheimer’s disease; CIBL, Chinese Imaging, Biomarkers, and Lifestyle; NIA-AA, National Institute on Aging Alzheimer’s Association; MMSE, Mini-Mental State Examination; DLB, dementia with Lewy bodies; FTD, frontotemporal dementia; PD, Parkinson’s disease; CNS, central nervous system; DSM-5, Diagnostic and Statistical Manual of Mental Disorders-vision 5; TBI, traumatic brain injury; HIV, human immunodeficiency virus; APOE ɛ4, apolipoprotein E type epsilon.
Data collection
Clinical data
Baseline demographic data, including age, sex, body mass index (BMI), years of education, and marital status, were collected. Medical histories of hypertension, diabetes mellitus, stroke, coronary atherosclerotic heart disease, dyslipidemia, and smoking and alcohol consumption were also collected. Blood was drawn from all participants, and genetic data were assessed at the WeGene Lab (Shenzhen, China) using a customized Illumina WeGene V3 Array containing approximately 700,000 markers (Illumina iScan System; Illumina, Inc., San Diego, CA, USA). The APOE haplotypes (ɛ4/ɛ4, ɛ4/ɛ3, ɛ4/ɛ2, ɛ3/ɛ3, ɛ3/ɛ2, and ɛ2/ɛ2) were determined, as previously described by Forlenza, using two single nucleotide polymorphisms (rs7412 and rs429358) [23].
BMI, commonly used as a predictor of nutritional status and overall adiposity, was calculated by dividing each participant’s weight in kilograms by their height in meters squared [24]. Marital status was defined as being married, and other statuses included widowhood, separation, divorce, and never married. Hypertension was defined as self-reported and caregivers-confirmed physician-diagnosed hypertension (systolic blood pressure≥140 mmHg or diastolic blood pressure≥90 mmHg) or use of antihypertensive medication within the last 2 weeks [25]. Diabetes mellitus was diagnosed based on two of the following abnormal screening test results: fasting plasma glucose level≥7.0 mmol/L, 2-h plasma glucose level≥11.1 mmol/L during a 75-g oral glucose tolerance test, or glycated hemoglobin A1c level≥6.5% [26]. Stroke was defined as self-reported and caregivers-confirmed stroke or brain neuroimaging findings confirming a medical history of ischemic stroke, transient ischemic attack, hemorrhagic stroke, or cerebral small vessel disease [27, 28]. Coronary atherosclerotic heart disease was defined as self-reported and caregivers-confirmed acute or chronic coronary syndromes, and the former also included ST-segment elevated myocardial infarction, non-ST-segment elevated myocardial infarction, and unstable angina [29, 30]. Dyslipidemia was defined as taking lipid-lowering medications or presenting with various lipid abnormalities, including an increased total cholesterol level (≥6.20 mmol/L), increased low-density lipoprotein cholesterol level (>4.13 mmol/L), increased triglyceride level (>2.25 mmol/L), or decreased high-density lipoprotein cholesterol level (<1.03 mmol/L) [31]. Smoking status was assessed by patients’ self-reported and caregivers-confirmed smoking behaviors that included whether they were current, former, or never smokers, and then former and current smokers were combined to create an ever/never smoking group. The age patients started smoking and average amount of cigarettes they smoked daily were also recorded. Alcohol consumption was assessed using patients’ self-reported and caregivers-confirmed information about the patients’ average weekly consumption of beer and long drinks, wine, and spirits.
Assessment of NPSs
NPSs were evaluated using the NPI, a fully structured questionnaire investigating 12 different behavioral and neuropsychiatric domains including delusions, hallucinations, agitation, depression, anxiety, euphoria, apathy, disinhibition, irritability, aberrant motor activity, sleep and night-time behavior, and appetite or eating disturbances [32]. The NPI scale provides a severity score (on a 3-point scale) and a frequency score (on a 4-point scale) for each reported symptom. NPI total severity scores were calculated by summing the 12 severity sub-scores (severity score×frequency score).
Global cognitive assessment
Global objective cognition was assessed using the Chinese version of the MMSE [33] and Beijing version of the Montreal Cognitive Assessment (MoCA) [34]. Patients with a total MMSE score of≤24,≤20, and≤17 for > 6, 1–6, and 0 years of education, respectively, or a total MoCA score of≤24,≤20, and≤14 for > 6, 1–6, and 0 years of education, respectively, were considered to have cognitive impairment.
Nutritional assessment
The nutritional status of all patients was assessed using the Mini-Nutritional Assessment (MNA) [35]. The MNA scale is used as a single, rapid assessment of the nutritional status of older patients in outpatient clinics, hospitals, and nursing homes. It comprises simple measurements and brief questions, including anthropometric measurements, a global assessment, dietary questionnaire, and subjective assessment. The sum of the MNA scores distinguishes between well-nourished patients (≥24), patients at risk of malnutrition (17–23.5), and malnourished patients (<17). The higher the MNA score, the better the nutritional status.
Statistical analyses
All statistical analyses were performed using SPSS version 26.0 software (SPSS Inc., Chicago, IL, USA). Chi-square or Fisher’s exact tests were used to assess statistical differences in categorical variables; continuous variables with a normal distribution were compared using independent t-tests; and skewed data were compared using the Mann–Whitney U test. A bootstrap with 5,000 iterations was used to perform the mediation analyses. A simple mediation model was developed through the establishment of three pathways to explain the mediation effects of nutritional status (MNA scores) or cognition (MMSE scores) on the association of APOE ɛ4 with specific NPS (hallucinations, apathy, or aberrant motor activity) (Fig. 2A). The chain multiple mediator model was developed through the establishment of four pathways to explain the chain-mediating effects of nutritional status (MNA scores) and cognition (MMSE scores) on the association of APOE ɛ4 with specific NPS (hallucinations, apathy, and aberrant motor activity) (Fig. 2B). Under these frameworks, the total effect (TE) can be divided into two components: natural direct effects (NDEs) and natural indirect effects (NIEs). The NDEs represented the effect of APOE ɛ4 on hallucinations/apathy/aberrant motor activity independent of MNA or MMSE scores (X⟶Y). NIEs represented the effect of APOE ɛ4 on hallucinations/apathy/aberrant motor activity, which could be explained by changes in MNA (X⟶MNA⟶Y) and MMSE scores (X⟶MMSE⟶Y). For the chain multiple mediator model, NIE also represents the chain effect of the MNA and MMSE scores (X⟶MNA⟶MMSE⟶Y) on the association of APOE ɛ4 and hallucinations/apathy/aberrant motor activity. The mediation effect was measured by percentage mediated, computed as NIE/TE×100% on a log-transformed odds ratio scale, which is the percentage of the TE mediated by the mediator [36].
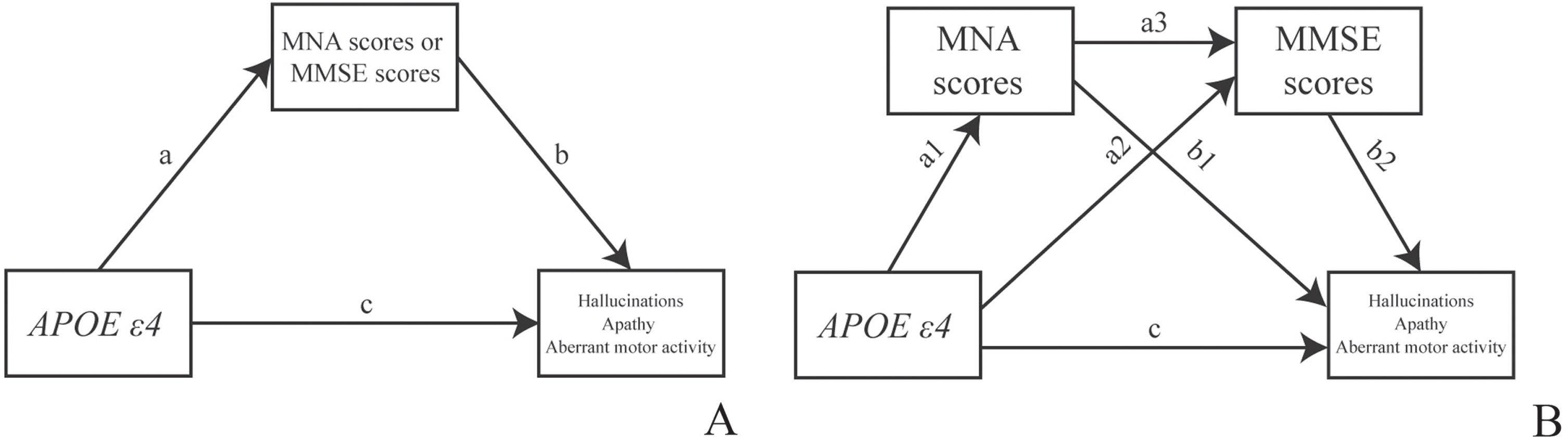
The simple and chain mediation models to explain the mediation effects of MNA and MMSE scores on the association of APOE ɛ4 with three specific NPSs. MNA, Mini-Nutritional Assessment; MMSE, Mini-Mental State Examination; APOE ɛ4, apolipoprotein E allele 4.
The mediating effect was considered significant if the 95% confidence interval (CI) was not zero. Factors known to be associated with NPSs in the univariate analysis were included in the subsequent mediating analyses as confounders, including age, sex, and years of education.
Univariate and multivariate linear regression analyses were performed for MNA scores, APOE ɛ4 status (exposure), and all confounders. Univariate and multivariate linear regression analyses were performed for MMSE scores, APOE ɛ4 status (exposure). and all confounders. A multivariate logistic regression model was fitted for hallucinations/apathy/aberrant motor activity (outcome), APOE ɛ4 status, MNA scores, MMSE scores, and all confounders. Statistical significance was set at a two-tailed p-value<0.05 in all analyses.
RESULTS
Baseline clinical characteristics
This study analyzed 310 patients with aMCI (185) or AD (125). The age of patients with aMCI was 64.33±7.23 (range, 53–84) years, whereas the age of patients with AD was 71.42±7.64 (range, 60–88) years. Of them, 229 (73.87%) presented with NPSs. The most common specific NPS was anxiety (n = 117, 51.09%), followed by apathy (n = 116, 50.66%), depression (n = 115, 50.22%), irritability (n = 95, 41.48%), sleep and night-time behavior (n = 85, 37.12%), agitation (n = 74, 32.31%), delusion (n = 55, 24.02%), disinhibition (n = 43, 18.77%), appetite or eating disturbances (n = 41, 17.90%), hallucination (n = 35, 15.28%), aberrant motor activity (n = 31, 13.54%), and euphoria (n = 24, 10.58%). Among the 310 patients with aMCI or AD, 110 (35.48%) carried APOE ɛ4. Table 1 shows the characteristics of general and specific NPSs in patients with aMCI or AD, with or without APOE ɛ4. Patients with APOE ɛ4 had higher total NPI scores than those without APOE ɛ4 (median [interquartile range, IQR]: 6.00 [1.75, 16.00] versus 4.00 [0.00, 11.75], Z = –2.187, p = 0.029). Patients with APOE ɛ4 were more likely to present with hallucinations (17.27% versus 8.00%, χ2 = 6.093, p = 0.014), apathy (47.27% versus 32.00%, χ2 = 7.060, p = 0.008), and aberrant motor activity (15.45% versus 7.00%, χ2 = 5.636, p = 0.018) than those without. No significant differences were observed in the general NPSs and other specific NPSs, including delusions, agitation, anxiety, depression, euphoria, irritability, disinhibition, sleep, and night-time behavior between the two groups.
General and specific NPS characteristics of patients with aMCI or AD carrying or not carrying APOE ɛ4
Data were evaluated using the χ2 or Mann–Whitney U test. Data are shown as n (%) or median (interquartile range). p value refers to the statistical findings of NPS characteristics between APOE ɛ4 carriers and APOE ɛ4 non-carriers in patients with aMCI and AD. aMCI, amnestic mild cognitive impairment; AD, Alzheimer’s disease; APOE ɛ4, apolipoprotein E type epsilon 4; NPI, Neuropsychiatric Inventory; NPS, neuropsychiatric symptoms; IQR, interquartile range.
Clinical characteristics of patients with three specific NPSs
Table 2 shows the clinical characteristics of the three specific NPSs: hallucinations, apathy, and aberrant motor activity. Patients with hallucinations were older (mean±SD: 72.06±7.18 years versus 66.57±8.09 years, t = –3.825, p < 0.001), had fewer years of education (median [IQR]: 9.00 years [6.00, 12.00] versus 12.00 years [9.00, 13.00], Z = –2.812, p = 0.005), had a higher frequency of being APOE ɛ4 carriers (54.29% versus 33.09%, χ2 = 6.093, p = 0.014), and had lower MMSE scores (median [IQR]: 16.00 [9.00, 21.00] versus 25.00 [19.00, 28.00], Z = –5.761, p < 0.001), MoCA scores (median [IQR]: 10.00 [3.00, 16.00] versus 20.00 [14.00, 24.00], Z = –5.425, p < 0.001) and MNA scores (median [IQR]: 22.00 [19.00, 24.50] versus 24.50 [22.00, 26.50], Z = –3.206, p = 0.001) than those without. Compared to those without apathy, patients with apathy were older (mean±SD: 68.68±8.91 years versus 66.30±7.57 years, t = –2.507, p = 0.013), had a lower frequency of being female (52.59% versus 64.95%, χ2 = 4.635, p = 0.031), a higher frequency of being APOE ɛ4 carriers (44.83% versus 29.90%, χ2 = 7.069, p = 0.008), and lower MMSE scores (median [IQR]: 19.00 [11.00, 24.00] versus 26.00 [22.00, 28.00], Z = –7.605, p < 0.001), MoCA scores (median [IQR]: 14.00 [7.00, 19.00] versus 16.00 [21.00, 24.00], Z = –7.516, p < 0.001) and MNA scores (median [IQR]: 22.50 [20.13, 24.88] versus 25.00 [22.88, 27.00], Z = –5.896, p < 0.001). Patients with aberrant motor activity were older (mean±SD: 71.00±8.23 years versus 66.77±8.06 years, t = –2.767, p = 0.006), had a higher frequency of being APOE ɛ4 carriers (54.84% versus 33.30%, χ2 = 5.636, p = 0.018) and had lower MMSE scores (median [IQR]: 17.00 [6.00, 24.00] versus 25.00 [19.00, 28.00], Z = –4.094, p < 0.001), MoCA scores (median [IQR]: 12.00 [2.00, 20.00] versus 19.00 [13.00, 23.00], Z = –3.892, p < 0.001) and MNA scores (median [IQR]: 21.50 [19.50, 24.00] versus 24.50 [22.00, 26.50], Z = –3.279 p = 0.001) than those without.
Clinical characteristics of patients with three specific NPSs
Data were analyzed using the χ2 test, independent samples t-test, and the Mann–Whitney U test. Data are shown as the mean±standard deviation, median (interquartile range), or n (%). BMI, body mass index; APOE ɛ4, apolipoprotein E type epsilon 4; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment MNA, Mini-Nutritional Assessment; IQR, interquartile range.
Simple Mediating Effect of MNA or MMSE scores on the association of APOE ɛ4 with three specific NPSs
Figure 3 presents the findings of the crude regression analysis and simple mediating effect of MNA or MMSE scores on the association of APOE ɛ4 with three specific NPSs without adjustment. Both the MNA and MMSE scores showed a strong mediating effect on the association between APOE ɛ4 carriers and three specific NPSs. Regarding hallucination, the proportion of the association between APOE ɛ4 carriers and hallucination mediated by MNA scores was 17.97% (95% CI: 0.0216–0.3501), while that mediated by MMSE scores was 37.13% (95% CI: 0.1487–0.6597) (Fig. 3A, B). MNA scores mediated 30.73% (95% CI: 0.0600–0. 4272) of the association between APOE ɛ4 carriers and apathy, whereas MMSE scores mediated 57.72% (95% CI: 0.1934–0.7388) of the association between APOE ɛ4 carriers and apathy (Fig. 3 C, D). For aberrant motor activity, the proportion of association between APOE ɛ4 carriers and aberrant motor activity mediated by MNA scores was 17.82% (95% CI: 0.0190–0.3606), whereas the proportion of association between APOE ɛ4 carriers and aberrant motor activity mediated by MMSE scores was 34.24% (95% CI: 0.1211–0.6359) (Fig. 3E, F).

The crude regression analysis and mediating effect of MNA or MMSE scores on the association of APOE ɛ4 with three specific NPSs without adjustment. MNA, Mini-Nutritional Assessment; MMSE, Mini-Mental State Examination; APOE ɛ4, apolipoprotein E allele 4.
Chain-mediating effect of MNA and MMSE scores on the association of APOE ɛ4 with three specific NPSs
The results of the regression analysis demonstrated that in the chain-mediated effect model constructed in this study, APOE ɛ4 and MNA scores (β= –0.8483, p = 0.0355), APOE ɛ4 and MMSE scores (β= –1.6578, p = 0.0307), MNA scores and MMSE scores (β= 0.6681, p<0.0001), MMSE scores and hallucinations (β= –0.0903, p = 0.0007), MNA scores and apathy (β= –0.1163, p = 0.0063), MMSE scores and apathy (β= –0.1342, p<0.0001), and MMSE scores and aberrant motor activity (β= –0.0893, p = 0.0010) were all statistically significant after adjusting for confounding factors (Supplementary Table 1).
Table 3 shows the chain-mediating effect of MNA and MMSE scores on the association of APOE ɛ4 with the three specific NPSs after adjusting for confounding factors. For hallucinations, the chain-mediating effect of MNA and MMSE scores on the association of APOE ɛ4 with hallucinations was 6.84% (95% CI: 0.0026–0.1274). The proportion of the effect of APOE ɛ4 carriers on hallucinations mediated by MMSE scores alone was 19.99% (95% CI: 0.0080–0.3737), while no significant mediating effect of the MNA scores on the association between APOE ɛ4 and hallucinations were found after controlling for age, sex, and educational years. For apathy, the chain-mediating effect of MNA and MMSE scores on the association of APOE ɛ4 with apathy was 11.54% (95% CI: 0.0014–0.1784), and the proportion of the effect of APOE ɛ4 carriers on apathy mediated by MMSE scores alone was 33.77% (95% CI: 0.0097–0.4843). In contrast, no significant mediating effects of the MNA scores on the association between APOE ɛ4 and apathy were found. For aberrant motor activity, the chain-mediating effect of MNA and MMSE scores on the association of APOE ɛ4 with apathy was 6.19% (95% CI: 0.0007–0.1367), while the proportion of the effect of APOE ɛ4 carriers on aberrant motor activity mediated by MMSE scores alone was 18.61% (95% CI: 0.0077–0.3871). However, no significant mediating effect was found on the MNA scores.
Chain-mediating effect of MNA and MMSE scores on the association of APOE ɛ4 with three specific NPSs
NPS, neuropsychiatric symptoms; APOE ɛ4, apolipoprotein E type epsilon 4; MMSE, Mini-Mental State Examination; MNA, Mini-Nutritional Assessment; CI, confidence interval.
DISCUSSION
In this study, the chain mediation analysis demonstrated that MNA and MMSE scores completely mediated the relationship between APOE ɛ4 and three specific NPSs, including hallucinations, apathy, or aberrant motor activity. This study is the first to investigate the mediation of nutrition and cognition on the association between APOE ɛ4 and NPSs, which adds evidence to the previous diverse findings on the association of APOE ɛ4 with NPSs. Approximately 6% to 60% of the variance in hallucinations, apathy, or aberrant motor activity, as captured by APOE ɛ4 carriers, could be attributed to a difference in MNA and MMSE scores, suggesting that targeting nutritional intervention and cognitive improvement should be considered as important strategies for preventing NPSs in patients with aMCI or AD.
Previous reports have yielded inconsistent results regarding whether APOE ɛ4 is associated with general or specific NPSs. Our findings are consistent with those of previous cross-sectional studies that failed to identify a direct association between APOE ɛ4 and NPSs. For instance, a case-control study found that the presentation of delusions and disinhibition in patients with AD was not associated with APOE ɛ4 status [37]. Another study that investigated the possible associations of synergistic genotypes (APOE ɛ4 status and circadian variants) with NPSs (depression, sleep disorder, delusions, hallucinations, and anxiety) in patients with AD progression did not find any association [38]. In contrast, some longitudinal studies have revealed that patients with AD carrying APOE ɛ4 had an increased incidence of delusions during a 9.3-year follow-up period [39], while another longitudinal study demonstrated that the presence of APOE ɛ4 carries a 19.0-fold risk for developing hallucinations and a 3.4-fold risk for delusions [40]. Additionally, an observational study showed that moderately impaired patients with AD carrying APOE ɛ4 demonstrated worse delusions and aberrant motor behavior but had a lower level of apathy compared with those not carrying APOE ɛ4. The mixed results of previous studies may be due to substantial methodological heterogeneity and the selection of NPSs among the studies.
Multiple mediation analyses conducted on 12 different NPI domains by adjusting for various confounding factors would produce more reliable evidence revealing the association of APOE ɛ4 with NPSs. Similar to the findings of Qian et al. [42], we also observed that MMSE scores were positively associated with both APOE ɛ4 and hallucinations in patients with aMCI or AD. APOE ɛ4 is a well-known risk factor for cognitive impairment, which is usually evaluated using MMSE scores. A 12-month follow-up longitudinal study found that in patients with AD, cognitive impairment was a significant predictor of changes in NPSs [43]. Additionally, from the perspective of the AD continuum, patients with lower MMSE scores who present with cognitive decline and disease progression are also associated with the presentation or deterioration of NPSs [44]. We found that the MMSE score was a strong mediator that linked APOE ɛ4 and hallucinations, apathy, and aberrant motor activity, which provided important information on the mechanism and development of NPSs and contributed to improving our understanding of the relationship between cognition and NPSs. Considering the limitations on drugs therapy of NPSs in the AD continuum, targeting improvement of cognitive function may be effective strategies for treating NPSs, especially in patients with APOE ɛ4.
A recent review demonstrated that APOE ɛ4 could affect microglia and inflammatory pathways, astrocyte and lipid metabolism, insulin resistance, and glucose metabolism. This provides novel insights into a precision nutrition approach, including a low-glycemic index diet, specific Mediterranean-style food choices, and a panel of seven nutritional supplements, for patients with AD who are APOE ɛ4 carriers [45]. Increasing evidence has revealed the importance of nutrition in the onset and development of AD. Recently, a systematic review highlighted the vicious cycle of malnutrition, cognitive decline, and NPSs development in patients with AD [9]. A longitudinal study including women with aMCI or AD found that poor nutritional status increased NPSs, especially verbal aggressiveness or emotional disinhibition, during a 2.5-year follow-up period [13]. A cross-sectional study reported a significant association between nutritional status, memory impairment, and NPS, including verbal aggressiveness, emotional disinhibition, and apathy [14]. Further, another study enrolled 345 patients with very mild or mild dementia and found a significant correlation between BMI and MNA or MMSE scores [46]. Therefore, we developed a chain mediation analysis to examine the joint mediation effect of MNA and MMSE scores on the link between APOE ɛ4 and specific NPSs, which also emphasized the potential role of targeted nutritional interventions in breaking this chain and preventing the development of NPSs in patients with AD continuum.
Although the current study is the first to reveal the vital role of nutrition and cognition in the association between APOE ɛ4 and NPSs in patients with AD, it has some limitations that need to be addressed in future studies. First, this was a single-center hospital-based cross-sectional study, and the generalizability of the conclusions warrants further validation in large community-based longitudinal studies. Second, this study relied partially on questionnaires as its main research approach. These questionnaires can be influenced by the patients’ cognitive function and caregivers’ attention on the patients.
In conclusion, this study is the first to find that MNA and MMSE scores have a strong chain-mediating effect on the association between APOE ɛ4 and three specific NPSs, including hallucinations, apathy, and aberrant motor activity, in patients with aMCI or AD. This finding adds evidence to the existing literature on the controversial conclusions about APOE ɛ4 and NPSs. Although the underlying mechanisms of NPSs were not completely clear, this study still offers new evidence regarding the synergistic effect between nutrition and cognition in the development of NPSs. Considering the limitations of NPSs therapy in the AD continuum, this study offers novel valuable insights into the role of targeted nutritional interventions in reducing the negative effect of APOE ɛ4 on the onset and development of NPSs. Future research to explore potential neural circuits among nutrition, cognition, and NPSs, and to perform quantitative assessments of mediators, including serum nutrition-related biomarkers and cerebrospinal fluid amyloid-β and tau levels, is needed to thoroughly elucidate the association between APOE ɛ4 and NPSs.
Footnotes
ACKNOWLEDGMENTS
The authors thank all the patients and their caregivers for their participation and the personnel for their contribution to the CIBL study. We also thank all members of the staff of the CIBL study for their role in data collection and analysis.
FUNDING
This research was funded by the National Natural Science Foundation of China (grant numbers 82071187 and 81870821), and the National Key Research and Development Program of China (grant numbers 2021YFC2500100 and 2021YFC2500103).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author (Xu J).