
Abstract
Alzheimer’s disease (AD) is a progressive neurological disorder characterized by memory loss, cognitive decline, and behavioral changes. Immunotherapy aims to harness the immune system to target the underlying pathology of AD and has shown promise as a disease-modifying treatment for AD. By focusing on the underlying disease pathogenesis and encouraging the removal of abnormal protein aggregates in the brain, immunotherapy shows promise as a potential treatment for AD. The development of immunotherapy for AD began with early attempts to use antibodies to target beta-amyloid. The amyloid hypothesis which suggests that the accumulation of beta-amyloid in the brain triggers the pathological cascade that leads to AD has been a driving force behind the development of immunotherapy for AD. However, recent clinical trials of monoclonal antibodies targeting amyloid-β have shown mixed results, highlighting the need for further research into alternative immunotherapy approaches. Additionally, the safety and efficacy of immunotherapy for AD remain an area of active investigation. Some immunotherapeutic approaches have shown promise, while others have been associated with significant side effects, including inflammation of the brain. Sleep has a significant impact on various physiological processes, including the immune system, and has been linked to the pathogenesis of AD. Thus, improving sleep quality and duration may benefit the immune system and potentially enhance the effectiveness of immunotherapeutic approaches for AD. In this review, we discussed the promises of immunotherapy as a disease-modifying treatment for AD as well as possible methods to improve the efficacy and safety of immunotherapy to achieve better therapeutic outcomes.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a major public health concern that affects millions of people globally and is characterized by a gradual loss of memory and cognitive decline [1]. Furthermore, accumulating evidence suggests that sleep disturbances may contribute to AD pathology through various mechanisms, such as the accumulation of amyloid-beta (Aβ) and tau proteins, neuroinflammation, oxidative stress, and impaired glymphatic clearance [2, 3]. Presently, treatment options for AD are limited to symptomatic management, highlighting the urgent need for innovative, disease-modifying therapies [4]. Given the complex interplay between sleep and the immune system, researchers have also explored the potential of immunotherapy in AD, particularly in the context of sleep-immune interactions [5, 6]. Immunotherapy approaches involve targeting the pathological processes underlying AD, such as the accumulation of Aβ and tau proteins, with antibodies or other immune-based interventions [7]. Recent clinical trials have shown promising results in reducing Aβ burden and improving cognitive function in patients with early-stage AD [8, 9]. However, challenges remain in optimizing the efficacy and safety of these therapies, particularly in more advanced stages of the disease.
Immunotherapy has emerged as a promising approach in AD research, with several studies demonstrating its potential to modify the disease course [10]. Different molecules such as Sirtuin 1 (Sirt1) have been identified to play an important role in attenuation of pathological hallmarks of AD [11]. Hence, they are being considered for combinatorial therapy with AD immunotherapy. Among physiological processes, sleep is a complex and dynamic process that plays an essential role in the maintenance of various physiological functions, including memory consolidation, synaptic plasticity, and neuronal repair [12, 13]. Sleep is a critical physiological function that is increasingly recognized for its association with neurodegenerative disorders, such as AD, and its role in maintaining cognitive health [14]. Studies have shown that disrupted sleep patterns, particularly in the form of sleep fragmentation or deprivation, can accelerate cognitive decline and increase the risk of developing AD [15]. This review aims to provide a thorough analysis of the historical context and potential applications of immunotherapy in AD, covering early attempts to treat AD with immunotherapy, the advent of the amyloid hypothesis, the state of immunotherapy in AD at the moment, safety concerns, immunotherapy side effects, and novel immunotherapeutic methods. Furthermore, the impact of sleep on immunotherapeutic methods will be explored, as devices that improve sleep quality may have the potential to enhance the effectiveness of these treatments [16]. By shedding light on the interplay between sleep, immunotherapy, and AD, this review seeks to discuss the prospective future research and contribute to the development of more effective therapeutic strategies for this debilitating disease.
HISTORICAL PERSPECTIVE OF IMMUNOTHERAPY IN AD
Since the 1990s, when researchers first tried to utilize active vaccination to remove Aβ from the brains of transgenic mouse models of AD, immunotherapy has been used to treat AD [17]. Aβ peptides are administered during active vaccination to elicit an immunological response and the formation of Aβ-specific antibodies. Transgenic mice showed increases in cognition and Aβ plaque reductions in the early outcomes of this strategy [17, 18]. Hock and colleagues published the findings of a clinical experiment in which they gave Aβ vaccine to the patients representing mild to moderate AD. The research revealed that the vaccination was secure and well-tolerated, and that the brain levels of Aβ protein in those who received it had significantly decreased [19]. Based on these discoveries, scientists started to create passive immunotherapy methods that used monoclonal antibodies (mAbs) that target Aβ. In 2000, Aβ mAbs 10D5 was first successfully used by Schenk and colleagues to lessen Aβ deposition in the brain of a transgenic mice model of AD [20]. Researchers started looking into the use of mAbs as an alternative kind of immunotherapy for AD after the failure of Aβ vaccines. To remove amyloid plaques from the brain, the first-generation antibodies, such as bapineuzumab and solanezumab were developed to target Aβ protein [21]. Aβ vaccine clinical studies failed because some patients experienced negative side effects such as meningoencephalitis and brain inflammation [22, 23]. The limited efficacy and potential safety issues with the use of first-generation mAbs had subdued the initial excitement surrounding these techniques. For instance, the AN1792 active immunization study is an example where the study was suspended because several participants developed meningoencephalitis [23].
The effectiveness of these antibodies in clinical trials has been inconsistent, with some studies showing a decline in Aβ levels but no improvement in cognitive performance and others demonstrating no appreciable effects on either Aβ levels or cognitive outcomes [21, 25]. The blood-brain barrier, a barrier that prevents dangerous compounds from entering the brain, proved to be a hindrance for these first-generation antibodies [26, 27]. Because of this, to have any impact on brain Aβ levels, these antibodies were given in high dosages or straight into the cerebrospinal fluid (CSF) [28]. Another drawback of these antibodies was their limited therapeutic window, as high doses could have adverse effects, such as vasogenic edema and micro-hemorrhages, while there is no therapeutic effect at low doses [29]. The selectivity of first-generation antibodies for particular Aβ isoforms is another of their main drawbacks. For instance, whereas bapineuzumab and gantenerumab target both the soluble and insoluble forms of Aβ, solanezumab preferentially targets the soluble form [30, 31]. Recent research, however, indicates that different Aβ isoforms may play unique roles in the pathogenesis of AD, with insoluble Aβ being more closely related to neurodegeneration and cognitive decline [32–34].
The potential for immunogenicity or the emergence of immunological reactions to the therapeutic antibody, is thought to be another limitation of immunotherapy. This may result in diminished effectiveness or possibly unfavorable consequences like infusion reactions or serum sickness [35, 36]. Moreover, the effectiveness of immunotherapy may be hampered in certain people by pre-existing Aβ antibodies [37, 38]. The high expense of producing and administering antibodies would have restricted their accessibility and availability to patients. These difficulties highlighted the requirement for the creation of more efficient and reasonably priced immunotherapies for AD. Despite these limitations, first-generation antibodies provided important insights into the potential of immunotherapy for AD and paved the way for the development of next-generation antibodies that can overcome these challenges.
Early immunotherapy clinical studies for AD had many difficulties and failures, including several promising strategies. For instance, the failures demonstrated by the phase III clinical trials [39] of two of the most researched mAbs, bapineuzumab and solanezumab, showed the complexity of AD pathophysiology and the requirement for more efficient therapeutic strategies where they failed to achieve their main objectives of enhancing cognitive function in AD patients [25, 40]. Similar to clinical studies with bapineuzumab, the first mAb, to target Aβ, which failed to demonstrate any discernible efficacy, phase III clinical trials were conducted for solanezumab, another Aβ targeting mAb, and that also failed to achieve its primary endpoints [41]. One possible explanation for the lack of effectiveness in these trials is that the mAbs were unable to eradicate the brain’s aggregated and insoluble forms of Aβ, which are known to be more closely related to neurodegeneration and cognitive decline as stated before [35]. Due to the possibility of immunogenicity, i.e., the emergence of an immune response to the therapeutic mAb, adverse effects such as infusion responses or serum sickness were another problem encountered in early clinical studies [36]. The lack of efficacy seen in some trials may have also been a result of these side effects.
The administration and dose of immunotherapeutic agents were one of the main difficulties. As mentioned before, high doses of the vaccine were employed in the early clinical trials of AN1792 to induce a strong immunological response which had some severe side effects. These side effects prevented the vaccine from being further developed [23, 42]. The process of choosing and enrolling patients presented another difficulty. Early clinical studies frequently included individuals with moderate to severe AD, which may have reduced the capacity of immunotherapeutic drugs to influence the course of the illness. Also, among patients with AD, there was variation in the amount and distribution of amyloid pathology, which could have affected how well immunotherapy worked [21]. All things considered, these difficulties and setbacks emphasize the necessity of thoughtful dose and administration, patient selection and stratification, and the creation of efficient immunotherapy drugs for the treatment of AD. Despite these difficulties, research into immunotherapy for the disease has continued to be driven by the amyloid hypothesis, which holds that the build-up of Aβ in the brain is a primary driver of AD pathology [43]. This idea has had a big impact on the development of immunotherapy for AD because many of the existing immunotherapeutic methods concentrate on reducing Aβ levels in the brain. However, the amyloid hypothesis has received criticism, and other researchers have offered replacement theories that emphasize the role that inflammation, tau protein, and other factors play in AD pathology [44, 45].
The setbacks faced in early therapeutic methods that were developed following the formulation of the amyloid hypothesis led to a re-evaluation of the immunotherapeutic approach, with researchers developing new strategies and next-generation antibodies aimed at improving efficacy and reducing side effects. The amyloid hypothesis has also had an impact on the design of clinical trials for immunotherapies. Clinical studies now routinely evaluate Aβ levels in the brain using biomarkers like positron emission tomography (PET) imaging, which enables researchers to find patients with high levels of Aβ who will likely benefit from treatment [46]. Recent clinical trials of immunotherapy for AD have yielded more encouraging outcomes despite some setbacks. In early-stage AD, aducanumab, a mAb that targets Aβ, has been demonstrated to lessen Aβ plaques in the brain and halt cognitive deterioration [24]. Such findings illustrate the value of continued research in this field and have rekindled interest in the potential of immunotherapy in AD management.
The emergence of the amyloid hypothesis has significantly influenced the course of research into immunotherapies for AD, giving the reason for the creation of immunotherapeutic strategies meant to lower Aβ levels in the brain. Recent developments in the field, including the aforementioned development of next-generation antibodies and the use of biomarkers to identify appropriate patients, have renewed interest in the potential of immunotherapy as a treatment approach for AD in spite of the setbacks received in early clinical trials.
CURRENT STATUS OF IMMUNOTHERAPY IN AD
Immunotherapy is a promising therapeutic strategy for AD. There are numerous immunotherapeutic strategies, including passive and aggressive strategies that are currently being employed in clinical settings (Fig. 1). The delivery of premade antibodies that bind to particular targets is a component of passive immunotherapy. Aβ, the main component of the amyloid plaques observed in the brains of AD patients, is the target of the most well-known passive immunotherapy strategy for the treatment of AD. The first Aβ-targeting monoclonal antibody created for AD was bapineuzumab and that due to multiple reasons including but not limited to, a lack of efficacy and safety issues, its clinical trials did not succeed [47]. Recently, use of graphene quantum dots and nanoparticles have shown promising results [48, 49]. In collaboration with immunotherapeutic paradigms, it can prove to be a successful therapy procedure.
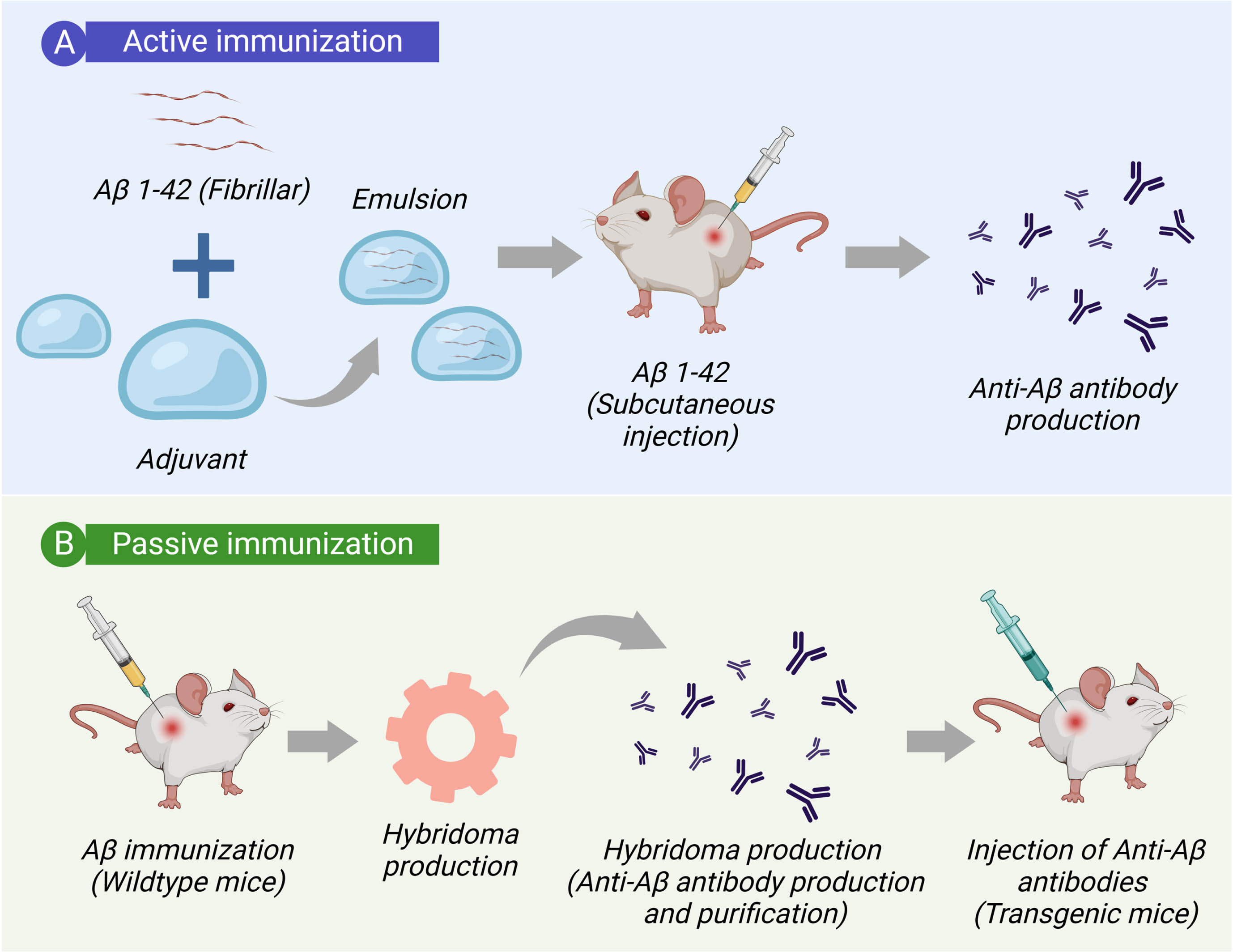
Molecular basis and active and passive immunization. A) Active immunization (Vaccination) stimulates the immune system to produce antigen-specific antibodies. B) Passive immunization initiate an immune response to produce antigen-specific antibodies bypassing the need of immune system activation. In both immunization process, anti-Aβ antibodies bind Aβ, targeting the Aβ peptide for clearance.
Several monoclonal antibodies, like solanezumab, aducanumab, and gantenerumab, are presently undergoing clinical testing for AD (Table 1). Gantenerumab targets both soluble and insoluble forms of Aβ, whereas solanezumab and aducanumab only target soluble forms of Aβ. Previous clinical trials using these antibodies have had mixed results, with some exhibiting efficacy that is encouraging and others failing to achieve their main endpoints [25, 50]. In active immunotherapy, the immune system of the patient is prompted to create antibodies against particular targets. Vaccines against Aβ are one form of active immunotherapy for AD. These vaccines work by stimulating the immune system to create antibodies against Aβ. AN1792 was shelved owing to security issues. CAD106 and UB-311 are two other Aβ vaccines that are currently being developed in clinical trials [51–53]. Further active immunotherapy strategies for AD, such as the use of DNA and RNA vaccines, which can stimulate long-term antibody generation, are being investigated in addition to mAbs and Aβ vaccines [24]. Immunotherapy may be more effective when used in combination with other treatments for AD, such as cholinesterase inhibitors or memantine. However, more research is needed to determine the optimal combination of therapies [54, 55].
Current immunotherapy treatment paradigms and their mechanism of action available for AD
The number of clinical trials examining the effectiveness of immunotherapy in the treatment of AD has increased dramatically during the past ten years. The majority of these studies have concentrated on Aβ plaques, which are regarded as the disease’s defining characteristic. Recent clinical trial findings have had significant implications in this field. The knowledge gathered from the AN1792 experiment resulted in the creation of new generation antibodies that are directed against Aβ plaques. As stated before, clinical trials for the first generation of antibodies, such as bapineuzumab and solanezumab, were not entirely successful [75]. However, the encouraging outcomes with aducanumab and gantenerumab (second-generation antibodies) hold great promise. In the phase III trial, aducanumab significantly reduced Aβ plaques and slowed cognitive deterioration in individuals with early-stage AD [76]. But the phase III trial of gantenerumab, a different mAb that targets aggregated Aβ, did not achieve its main objective of delaying cognitive aging [59].
Due to problems associated with the designs and variable outcomes of trials between dosage groups, the US Food and Drug Administration’s (FDA) decision to approve aducanumab in light of its positive results has sparked controversy [77]. It received accelerated approval from the FDA in June 2021; however, further confirmatory trial for the medication is required [78]. In preclinical and early clinical trials, immunotherapeutic strategies other than those that target Aβ, such as those using anti-tau antibodies, have also shown promise [79]. To ascertain the efficacy and safety of these methods, further research is necessary as they are still in the early stages of development. The use of immunotherapy for AD has showed promise in recent clinical trial outcomes, particularly when Aβ plaques are the target. Recently, the use of immunotherapy in combination with gene therapy has been given a focus. Gene therapy is a promising new approach to treating AD. Immunotherapy could be used to enhance the effects of gene therapy or to deliver genes that encode protective proteins in the brain [80, 81]. To determine the long-term effectiveness and safety of these strategies, more research is required. The controversy surrounding the aducanumab approval underlines the requirement for more exacting clinical trial design and outcome interpretation.
In the realm of clinical aspects, the implementation of immunotherapy for AD faces several challenges [82]. One crucial aspect is patient selection and stratification. The heterogeneity of AD pathology and the varying response to immunotherapy necessitate the identification of suitable biomarkers and diagnostic tools to accurately predict treatment outcomes and monitor disease progression [82]. Biomarkers such as Aβ and tau levels in the CSF, neuroimaging techniques including PET scans, and genetic markers associated with AD risk are being explored for their potential utility in patient selection and monitoring treatment response [83, 84]. Additionally, the timing of intervention is critical. Initiating immunotherapy during the early stages of the disease, when the pathological burden is relatively lower, may offer better chances of success compared to late-stage interventions [85, 86]. Nevertheless, the optimal duration and frequency of immunotherapy, as well as the long-term effects and sustainability of the treatment response, require careful evaluation through longitudinal studies [86]. To ensure the successful translation of immunotherapy into clinical practice, the development of standardized protocols, dosing regimens, and treatment guidelines is imperative. Collaboration between academia, pharmaceutical companies, regulatory authorities, and healthcare providers is crucial to establish rigorous clinical trial designs, harmonize outcome measures, and navigate regulatory pathways for expedited drug approval. Furthermore, the cost-effectiveness of immunotherapy and its accessibility to a broader population are important considerations in the development and implementation of these therapies [87]. Addressing these clinical aspects will be vital for the successful integration of immunotherapy into the existing treatment landscape for AD and ultimately improving patient outcomes. Further, development and testing immunotherapy approaches for Alzheimer’s disease has been depicted in Fig. 2.
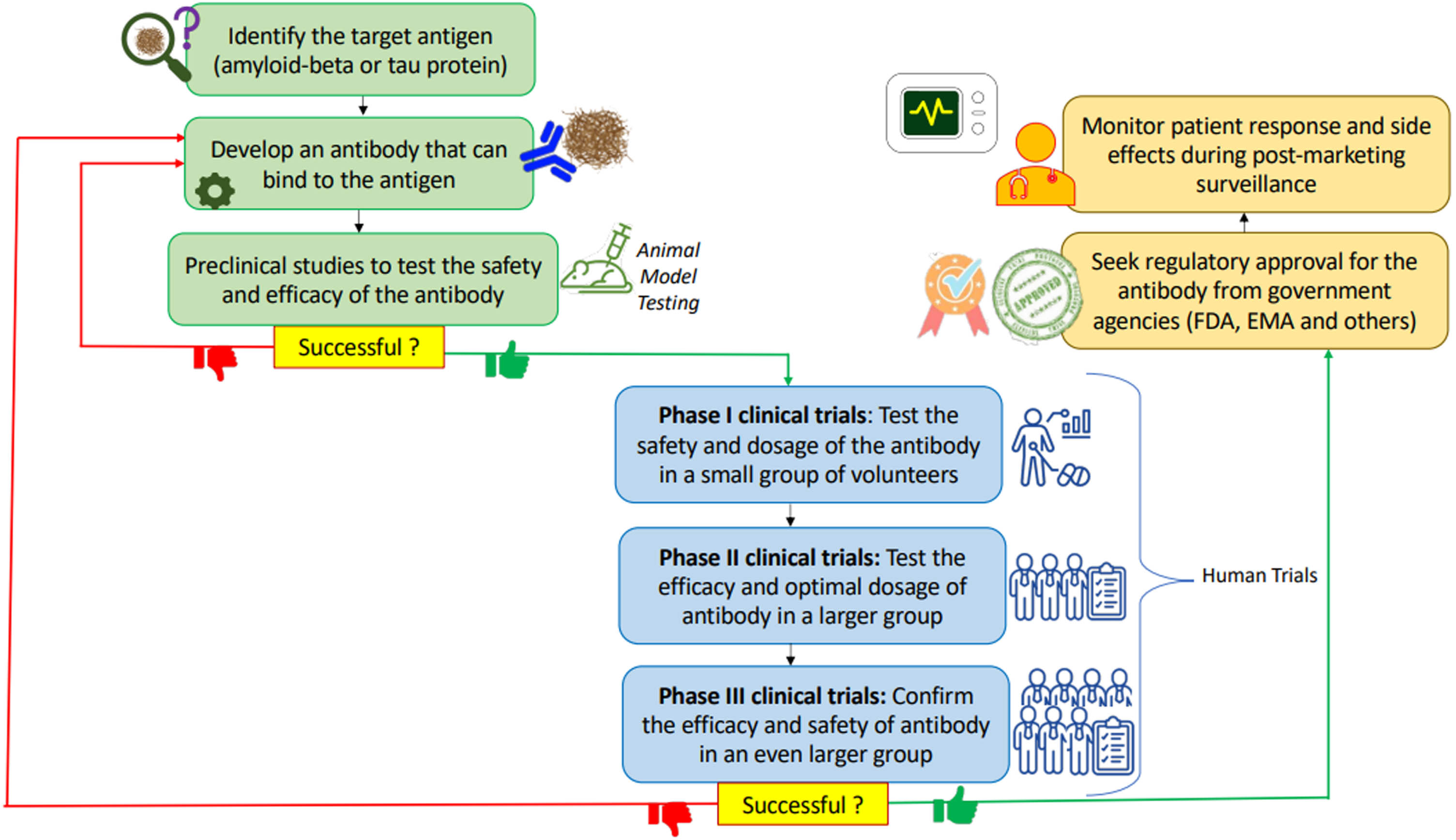
Development and testing immunotherapy approaches for Alzheimer’s disease. The process begins with identifying the target antigen, such as amyloid-β or tau protein, and developing a therapeutic antibody that can bind to it. Preclinical studies are then conducted to test the safety and efficacy of the therapeutic antibody in animal models of Alzheimer’s disease. If preclinical studies are successful, clinical trials are conducted in humans to test the safety and efficacy of the therapeutic antibody. Phase I clinical trials test the safety and dosage of the therapeutic antibody in a small group of healthy volunteers or patients with Alzheimer’s disease. Phase II clinical trials test the efficacy and optimal dosage of the therapeutic antibody in a larger group of patients with Alzheimer’s disease. Phase III clinical trials confirm the efficacy and safety of the therapeutic antibody in an even larger group of patients with Alzheimer’s disease. If clinical trials are successful, regulatory approval is sought from government agencies such as the FDA or EMA. Finally, post-marketing surveillance is conducted to monitor patient response and side effects. This flowchart provides a visual representation of the complex process involved in developing immunotherapy approaches for Alzheimer’s disease, highlighting key steps along the way from target identification to regulatory approval.
When assessing the possibility of this therapeutic method, the safety issues and side effects connected to immunotherapy for AD are crucial factors to take into account. The emergence of amyloid-related imaging abnormalities (ARIA), which has been seen in clinical studies for a number of immunotherapeutic drugs including aducanumab, solanezumab, and gantenerumab, is a significant safety risk [88]. Careful monitoring and changing the dose of the immunotherapeutic agents as necessary can reduce the incidence of ARIA. Infusion reactions and the danger of infection are two additional possible side effects of immunotherapy for AD in addition to ARIA [89, 90]. Pre-medication or a slower infusion rate can be used to treat infusion responses like fever, chills, and headache. Although the danger of infection is modest, clinical studies need to be constantly watched [90]. While assessing the possibility of immunotherapy for AD, it is crucial to take these safety issues and adverse effects into account. Despite these worries, immunotherapy has demonstrated promise in clinical trials and is a viable therapeutic strategy for this life-threatening illness. To develop techniques to reduce the risk of adverse events and to better understand the safety profile of immunotherapy, more research is required.
FUTURE DIRECTIONS FOR IMMUNOTHERAPY IN AD
The goal of new immunotherapeutic approaches for AD is to create antibodies of enhanced specificity, effectiveness, and safety. These antibodies are made to target not only Aβ but also tau and alpha-synuclein, two pathogenic proteins involved in AD pathogenesis. Creating antibodies that specifically target certain forms of Aβ, such as oligomeric or fibrillar Aβ, which are thought to be more toxic than soluble forms of Aβ, is one strategy [91]. Another method is to produce antibodies that target Aβ protofibrils, which are believed to be an early pathogenic form of Aβ that predates the formation of fibrillar Aβ plaques [92]. Moreover, longer half-lives and better pharmacokinetics are being worked on in next-generation antibodies, which may allow for less frequent dosing and higher patient compliance. Lecanemab, also known as BAN2401, is one such antibody that has a longer half-life than other antibodies and has demonstrated good outcomes in clinical trials [93]. Another potential approach is to use bispecific antibodies that simultaneously target two distinct proteins. For instance, preclinical investigations have demonstrated that bispecific antibodies that target Aβ and tau diminish both Aβ and tau pathology, respectively [94, 95]. Moreover, next-generation antibodies have the potential to enhance the safety profile of immunotherapy by lowering the frequency of untoward effects including brain swelling [96, 97] which has been noted in certain patients receiving immunotherapy techniques [21]. In a mouse model of AD, for instance, a recent study found that using an antibody fragment rather than a complete antibody could lower the risk of brain swelling while still successfully lowering Aβ pathology [98].
Furthermore, given the intricate interactions between Aβ, tau, and other pathogenic proteins throughout the onset and course of the disease, the development of immunotherapeutic strategies that target different harmful proteins may be especially successful in treating AD [35]. Targeting different pathogenic proteins at once may, in fact, be more beneficial than doing so for a single protein in lowering pathology and enhancing cognitive function, according to recent preclinical research [99, 100]. Bispecific antibodies and next-generation antibodies are just two examples of the innovative immunotherapeutic strategies being researched for the treatment of AD. The UB-311 vaccine which targets simultaneously both Aβ and tau and the CAD106 vaccine which is intended to stimulate an immune response against only Aβ are examples of innovative immunotherapeutic strategies against AD [51, 53]. Nevertheless, non-antibody-based strategies are also being researched, including the use of gene therapy to improve the immune response to Aβ [101]. This approach involves the transfer of the brain-derived neurotrophic factor (BDNF) gene to the brain and lower levels of Aβ, which is a significant pathogenic aspect of AD. In the transgenic mouse model, the researchers also showed that the nanoparticle-based delivery of the BDNF gene could endorse cognitive performance. This path shows the possibility of functionalized nanoparticles as a cutting-edge gene therapy strategy for the treatment of AD.
Last but not least, brand-new immunotherapy approaches that do not rely on antibodies are being created, like using tiny compounds to prevent the aggregation of Aβ or tau. TRx0237 is one such drug that has demonstrated promise in lowering tau pathology in preclinical investigations [102]. Therefore, the development of new immunotherapeutic techniques and next-generation antibodies holds great promise for the treatment of AD. In comparison to current immunotherapy techniques, these strategies may provide better efficacy and safety profiles, which could ultimately result in the creation of potent therapies for AD (Table 2).
Immunotherapeutic approaches for AD. Each of the three approaches has different mechanism of action, advantages, and disadvantages
There are still significant issues that need to be resolved despite the optimistic outcomes of recent clinical trials employing immunotherapy in AD. The ineffectiveness of current immunotherapeutic techniques, which target Aβ plaques in the brain, is one of the main obstacles. Preclinical studies are still being conducted to find additional targets and boost the efficacy of immunotherapy. Targeting tau protein, another defining feature of AD pathogenesis, is one strategy. Neurofibrillary tangles, which are intimately related to neuronal death and cognitive impairment, are formed when tau protein aggregates. Immunotherapy that targets tau protein has been proven in several preclinical studies to reduce tau pathology and enhance cognitive performance in animal models of AD [116, 117]. For example, in a mouse model of tauopathy, Yanamandra and colleagues showed that immunization with a tau peptide vaccine reduced tau pathology and enhanced cognitive performance [90].
Another strategy is to create new antibodies with enhanced Aβ plaque binding affinity and specificity. For instance, phase Ib and phase II clinical studies of aducanumab, a mAb that targets Aβ, revealed encouraging outcomes [21, 24]. The failure of the aducanumab in phase III trial, however, emphasizes the need for next-generation antibodies that are more efficient. Bispecific antibodies that target both Aβ and tau have been discovered as prospective candidates for next-generation antibodies in preclinical research [107, 108]. Preclinical research is also investigating the use of combination therapy, which entails focusing on numerous pathways connected to the pathophysiology of AD. In a mouse model of AD, for instance, a recent study by Chiang and co-workers [118] demonstrated that combination therapy using an anti-Aβ antibody and a gamma-secretase inhibitor improved cognitive function and decreased Aβ pathology. Combination therapy offers the potential to improve therapeutic effectiveness while lowering the risk of adverse effects. Future clinical trials will be significantly impacted by current preclinical research. First, the discovery of novel immunotherapy targets, such as toxic oligomeric forms of Aβ and tau protein, offers chances for the creation of next-generation antibodies with enhanced efficacy. Second, the use of combination therapy may increase the success of immunotherapy while lowering the risk of negative side effects. Finally, for patient stratification and personalized medicine in immunotherapy research, the identification of biomarkers that can precisely predict treatment response and disease progression will be essential.
For the successful use of immunotherapy, the development of customized treatment in AD is crucial. To optimize therapeutic efficacy and reduce the hazard of side effects, patient stratification, or the determination of those who will benefit from a particular treatment, is essential. Age, genetic background, illness stage, and comorbidities are some of the variables that can affect how well an immunotherapy treatment works. For instance, the apolipoprotein E (APOE) ɛ4 allele is a recognized risk factor for AD, and people who carry this allele may react to immunotherapy differently than people who do not. Also, the illness stage can affect how well immunotherapy works, with early-stage patients having a higher chance of success than late-stage patients.
The categorization and selection of patients for immunotherapy can be aided by the use of biomarkers, such as concentrations of Aβ, tau-beta and tau proteins in the CSF and imaging methods to identify Aβ and tau deposits. For instance, a recent study showed that in early AD patients, the presence of amyloid plaques measured by PET imaging can predict the responsiveness to the anti-amyloid antibody, aducanumab [24]. Next-generation sequencing, which uses individual genetic and molecular traits to identify patients, may help with patient stratification and guide the creation of specialized immunotherapies [119]. Researchers can develop individualized therapeutic strategies that are optimized for individual patient by comprehending the distinct genetic and molecular characteristics of each patient. The development of immunotherapy for AD depends critically on patient classification and tailored medicine. We can maximize the effectiveness and safety of immunotherapy for this terrible disease by identifying individuals who are most likely to benefit from treatment and personalizing medicines to individual genetic and molecular factors.
EFFECT OF SLEEP ON IMMUNOTHERAPY
The field of sleep therapy is gaining momentum in today’s world. There is mounting data that suggests sleep may significantly affect how well immunotherapy for AD works. The innate and adaptive immune systems are both impacted by sleep which is crucial for immune system modulation [6]. Immune malfunction and a reduced response to immunotherapy have been linked to sleep disorders such as insomnia and sleep apnea [120]. There is strong evidence that some lifestyle modifications may modify the prevalence of the disease. The quality of sleep may improve as a result of such a shift. There is growing evidence that insufficient sleep increases the amount of Aβ in the brain, which in turn causes abnormal Aβ levels to disrupt sleep and, consequently, memory consolidation [121, 122]. The effectiveness of immunotherapy for AD may be significantly impacted by the connection between sleep and the immune system (AD). The modulation of the immune response during sleep is influenced by a number of factors and may affect how well immunotherapeutic methods work.
Sleep deprivation and immune response
Lack of sleep has been demonstrated to have a deleterious impact on the immune system, resulting in decreased cytokine production, altered T-cell function, and decreased activation of natural killer cells [123]. Immunotherapy for AD patients may be less successful due to these immunosuppressive effects that can hinder the body’s capacity to establish an efficient defense against amyloid-beta and tau proteins [6].
Sleep and immune cell trafficking
Sleep is known to affect the movement of immune cells, including T-cells and monocytes, which are crucial for the removal of the proteins Aβ and tau [124]. Sleep issues may interfere with these immune cells’ migration to the brain, impeding immunotherapy and lowering treatment effectiveness [125].
Sleep and the glymphatic system
Sleep is when the glymphatic system is most active, which is in charge of removing waste from the brain, including Aβ [14]. Sleep deprivation may hinder the glymphatic system’s ability to operate, causing harmful proteins to accumulate and perhaps lowering the effectiveness of immunotherapy that targets these proteins [126].
Sleep interventions and immunotherapy
Drug therapies and cognitive-behavioral therapy for insomnia have both been demonstrated to improve the quality of sleep in AD patients [127]. The immune system’s response and the glymphatic system’s performance may be strengthened by better sleep, thus enhancing the therapeutic effects of immunotherapy in AD patients [126].
As technology developed, several instruments and devices were produced to aid in improving the quality of sleep. These devices could inadvertently contribute to an improvement in the effectiveness and/or efficiency of immunotherapeutic techniques. White noise generators create a steady sound that can be used to conceal distracting noises in the environment and aid in relaxing and sleep. White noise has been found in studies to lengthen and increase the quality of sleep, especially in people who have insomnia [128]. The length, stages, and quality of sleep are just a few of the details tracked by wearable technology and smartphone applications that measure sleep. The accuracy of sleep trackers varies, and even though they might offer insightful data, they should only be used as supplemental tools rather than as diagnostic tools [129].
It has been demonstrated that light therapy, particularly blue light exposure, can improve the quality of sleep and regulate circadian cycles. Yet, nighttime exposure to blue light in excess can interfere with sleep. Thus, it is crucial to use light treatment devices properly and with professional supervision [130]. Sleep-inducing headbands, such as those using electroencephalography technology, monitor brain activity and provide auditory feedback to help users fall asleep faster. These devices have shown promise in improving sleep latency and sleep quality [131]. Modern mattresses and pillows can offer individualized support and comfort, which can enhance the quality of your sleep. There is evidence that certain mattress technologies, such memory foam and adjustable air chambers, might lessen pressure spots and encourage appropriate spinal alignment [132]. Diffusers and sleep masks infused with essential oils are two examples of aromatherapy products that can aid in creating a calm environment that promotes sleep. Some aromas, like lavender, have been demonstrated to enhance sleep quality and lessen anxiety [133]. A combination of immunotherapeutic methods and such devices that can help improve sleep might lead to a better prognosis in AD patients and might to better quality of life and might even hold the potential to be the cure for AD.
DISCUSSION AND CONCLUSION
AD is a well-known fatal neurological condition with few effective treatments. Targeting the disease’s underlying pathophysiology, immunotherapy has become a potential approach of treating AD. The creation of the amyloid hypothesis, which has had a substantial impact on research into immunotherapy, came after early attempts to use immunotherapy as a treatment for AD. Early clinical trials, though, encountered difficulties and failures, underscoring the demand for additional study. Although safety issues and adverse effects must be taken into account, the current situation of immunotherapy for AD is positive, with numerous techniques in clinical development. Next-generation antibodies are one example of an emerging immunotherapy strategy that has the potential to overcome the drawbacks of conventional methods. In addition, dietary modifications [134] along with personalized medicine and patient classification are essential to the success of immunotherapy research for AD.
Sleep might have a significant impact on both the pathogenesis of AD and the effectiveness of immunotherapy on AD. There has been the development and invention of several devices that can improve sleep quality and/or duration. These devices can aid immunotherapeutic methods to perform better and remove of pathogenic amyloid from the brain due to the effect of sleep on the immune system. In conclusion, immunotherapy has a lot of potential as a treatment for AD, and more study is needed in this area to help those who are afflicted by this terrible illness. With research booming in the fields of both sleep study and immunotherapy, there might be significant changes in the way we treat AD in the future. Overall, the growing body of evidence on the role of sleep and the immune system in AD pathogenesis underscores the need for a multifaceted approach to disease management. Future research should aim to elucidate the mechanisms underlying sleep disturbances in AD and explore the potential of immunotherapy in targeting these mechanisms.
Furthermore, the combination of immunotherapy with other therapeutic approaches holds promise for enhancing treatment outcomes in AD. Synergistic effects may be achieved by combining immunotherapy with other disease-modifying strategies, such as anti-inflammatory agents, antioxidants, or drugs targeting tau pathology [135, 136]. Additionally, emerging evidence suggests that lifestyle interventions, including physical exercise, cognitive stimulation, and a healthy diet, can influence the efficacy of immunotherapy and potentially delay disease progression [137, 138]. These multifaceted approaches, targeting various aspects of AD pathophysiology, could offer a comprehensive and personalized treatment approach for individuals with AD. Therefore, future studies should explore the synergistic effects and optimal combinations of immunotherapy with other treatment modalities to maximize therapeutic benefits and improve clinical outcomes. Therefore, immunotherapy represents a promising avenue for the treatment of AD. Despite initial challenges and failures, the field has made significant progress, with the development of next-generation antibodies and exploration of alternative immunotherapy strategies. The interplay between sleep, the immune system, and AD pathogenesis further highlights the importance of considering sleep interventions and optimizing the immune response in immunotherapeutic approaches specially under pathophysiological conditions like obesity [139, 140] which can affect the overall outcome of AD immunotherapy. Ongoing research efforts in both sleep studies and immunotherapy offer hope for transformative advancements in AD treatment [135]. With a multifaceted approach that encompasses personalized medicine, lifestyle interventions, and combination therapies, we have the potential to revolutionize the management of AD and improve the lives of those affected by this devastating disease. Continued research and collaboration among scientists, clinicians, and policymakers are essential to realizing the full potential of immunotherapy in the fight against AD.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank their respective institutes for their support. SG and JKS acknowledge the support from International Brain Research Organisation (IBRO). The authors would like to express their gratitude to the editor and reviewers for their thorough evaluations and constructive criticism, which improved the scientific merit of this manuscript.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.