
Abstract
Background:
Alzheimer’s disease (AD) plagues 6.5 million Americans 65+, yet treatments are lacking. The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet has been developed to address the expansive impact of dementias on the general public. This systematic review evaluated the impact of the MIND diet on cognition in those with pathologies across the dementia spectrum.
Objective:
To evaluate the application of the MIND diet for prevention and/or treatment of dementia.
Methods:
PubMed was used to conduct a search using the MIND diet and terms related to cognition. Articles were excluded if they were published prior to 2018, studied a population without dementia or significant risk factors, or did not include those 65 + . The overall quality of each source was analyzed based on the cognitive test(s) used, the selection of subjects, and the sample size.
Results:
The search generated 33 papers, which yielded 11 articles after screening. Of these studies, one was conducted on those with mild cognitive impairment, one with AD, two with general dementia, and seven with at-risk individuals. All the studies found a positive correlation between adherence and some form of cognitive functioning, but results were mixed for specific cognitive domains.
Conclusions:
These findings suggest that the MIND diet may be a useful long-term treatment option for those with various dementia pathologies. However, more research is needed on subjects with onset dementias. Additionally, there is a need for more research into the mechanisms behind the common comorbidities.
Keywords
INTRODUCTION
As of 2022, roughly 6.5 million Americans aged 65 + have been diagnosed with Alzheimer’s disease (AD), and it is the 5th leading cause of death in this population. Although incidence has remained stable for the past decade, prevalence continues to climb as lifetime expectancy increases. AD results in decreased quality of life, inability to perform Activities of Daily Living (ADLs), and eventually death, yet we lack treatments aimed at prevention or slowing its progression [1]. Decreased functioning causes many patients suffering from AD to require nursing or in-home care, placing a burden on caregivers, families, and the general tax-paying population [2]. In fact, the average cost of care for someone with AD or a related dementia is $41,757 annually, roughly triple that for someone without AD [1]. However, AD does not exist in a microcosm. Approximately 12–18% of Americans 60 + have been diagnosed with MCI, a form of dementia that is a predictor for AD and other neurodegenerative diseases [3]. Dementia is a condition characterized by cognitive decline and AD represents only one form of dementia [1]. AD is characterized by the neuroanatomical changes that often cause dementia which is why Jack et al. proposes a “research framework” to address the complexity of dementia in today’s era. This modern “research framework” provides a new perspective in which AD, mild cognitive impairment (MCI), and other forms of dementia are all recognized under an umbrella of degenerative cognitive conditions. This holistic approach has become a widely accepted tool for better-informed treatment, yet the literary field is slow to adapt to the new perspective [4].
Although we know that nerve damage plays a role in the onset of AD, we know very little about the underlying causes of these changes, which dramatically limits treatment options. As of date, seven pharmaceutical drugs have been approved for treatment, but many aim to treat the symptoms rather than the etiology [5]. Due to the interactions between neurocognition and the nervous system, AD often co-occurs with many metabolic comorbidities including hypertension, stroke, high cholesterol, obesity, coronary heart disease, and type II diabetes [6–9]. Environmental factors such as social interaction have also been shown to reduce cognitive decline in older adults with and without AD [10]. Lifestyle factors such as physical exercise [11], dietary patterns [12], and dietary biomarkers [13] also play a role in AD, but the pathways by which these treatments improve functioning is unclear. Additionally, Apolipoprotein E (APOE) ɛ4 is a gene on the 19th chromosome that increases the risk of developing AD by roughly 35%, but its interaction with other risk factors is unclear [14]. In terms of nutrition, there is a correlation between the consumption of essential fatty acids and preserved cognitive functioning [15] which is why the Mediterranean diet has become a proposed intervention for AD.
Recently, the MIND diet has been developed from the Mediterranean and Dietary Approaches to Stop Hypertension (DASH) diets to address the dementia crisis [16]. The characteristic foods of the MIND diet are 10 food groups that have been linked to neurocognitive health: green leafy vegetables, other vegetables, nuts, berries, beans, whole grains, seafood, poultry, olive oil, and wine. An additional five foods (butter/margarine, cheese, red meat, fast fried foods, pastries/sweets) are not recommended based on research surrounding their consumption and dementia. Adherence to the MIND diet is measured through a MIND score, which uses dietary information from Food Frequency Questionnaires (FFQ) to quantify adherence. The MIND score uses individuals’ responses of their consumption of the preceding 15 food groups (recommended and not advised) to approximate the number of servings of each MIND food that an individual consumes over the course of a set timespan. The frequencies are then assigned numerical values and compiled into an overall score from 0-15, with 0 being low adherence and 15 being high [16]. Although the use of the MIND diet as a treatment has not been directly studied, the MIND diet has been associated with reduced incidence of AD [16] and improved global cognition scores in the general population [12]. The forthcoming MIND study analyzes the impact of the MIND diet on cognition in older individuals with a family history of AD [17]. This study will provide vital information about the potential of the MIND diet for treatment and prevention.
Cognition is a complex term encompassing six main neurological processes and countless subdomains: memory, processing speed, language, attention, visual-spatial perception, and executive functioning. Due to this, cognition is often measured through a battery of tests aimed at examining each cognitive domain [18]. For example, the Global Cognition Score (GCS) is a standard metric of cognitive function comprised of multiple tests, commonly the Clock Drawing Test, Mini-Cog test, General Practitioner Assessment of Cognition, Mini-Mental State Examination (MMSE), and the Montreal Cognitive Assessment [19]. The validity of each of these tests is measured through sensitivity and specificity, which are collectively termed normative data in the literature.
There is a fair amount of research on the relationship between the MIND diet and cognition but the population varies across studies, so a systematic review of various dementia populations is required to gain a full perspective on the scope of the MIND diet. The proposed study will fill this gap by compiling and critically analyzing the existing research surrounding the impact of the MIND diet on cognitive function in those with dementia, with the intent of possibly using the MIND diet as a future treatment option.
METHODS
Study design
The protocol for this specific systematic review was derived from the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) with the exception that this was a solo review [20]. The guidelines were tailored to this subject using existing evidence from the field [21], while this protocol was not registered a priori. The search was restricted to papers written since 2018, to account for the recent application of the research framework in this field [4] and to update the most recent meta-analysis [22]. All articles had to be written in English and study designs had to include the MIND diet as an intervention that preceded data collection. PubMed was used to conduct the search required for the analysis. Although PubMed provides a US-centric perspective and may neglect some international research sources, it was the most accessible and comprehensive source for medicine-specific data, including various study designs [23]. All articles used in this study were accessed on February 24, 2023. No supplemental search strategies were implemented, to avoid identifying excess duplicates.
Search terms relating to cognition (including global cognition, cognitive performance, cognitive health, and cognitive functioning), and MIND diet were used [12] in the following search: ((MIND diet[Title]) OR (Mediterranean-DASH Intervention for Neurodegenerative Delay))AND ((cognition[Title]) OR (cognitive[Title])). Although restricting to titles with the key terms may have excluded some relevant sources, this method also efficiently removed most of the extraneous sources, making this solo review possible.
The screening process occurred over two stages: title and abstract screening and full-text screening. The backgrounds of the resulting articles were screened in accordance with the following criteria: MIND diet was the independent variable, cognition was a dependent variable, population was humans including those 65 and older, population included those diagnosed with AD, dementia, MCI, or were flagged for having an increased risk of developing dementia [4]. For the purpose of this study, “increased risk” was defined as possessing risk factors other than old age, such as related comorbidities and APOE genotyping.
Articles that studied memory exclusively as a dependent variable were excluded, because memory is just one facet of cognition. Papers that included those with any form of dementia within the general aging population were also included to account for undiagnosed dementia in the general population and evidence suggesting that cognitive decline may begin as early as age 45 [24]. Due to the correlations between dementia and a host of comorbidities, the study population could include subpopulations (i.e., stroke victims) [6]. Articles that studied the impact of the MIND diet along with other Mediterranean-derived dietary patterns were included [16].
Analysis
The following characteristics were arranged into a table for each data source: reference, study design, follow-up duration, mean age of sample population, sex distribution of sample population, comorbidities of the sample population, method of cognitive assessment, pathology of population (general dementia, risk, MCI, AD), average MIND score, and source population. Quality analysis protocol was tailored to the study design and cognitive test used by each source. Nonrandomized study designs were analyzed using criteria from the Newcastle-Ottawa Scale [25] (the selection of subjects, the comparability of study groups, and the assignment of the exposure and control) as precedent, but the numerical scale was not used [26]. Based on each article’s adherence to the preceding criteria and its sample size, an overall risk of bias rating was assigned: a “low” rating will correlate with a 3, an “unclear” rating will correlate with a 2, and a “high” rating will correlate with a 1. The quality of each of the cognitive tests used was analyzed based on the specificity and sensitivity for dementia detection reported in a meta-analysis performed by [27]. The specificity and sensitivity of each test was averaged to provide an overall measure of the test or battery’s strength. The risk of bias number and test strength number was combined to yield a composite quality score [21]. Consequently, the findings of the articles with greater quality ratings were more heavily considered than those with lesser ratings in the overall synthesis process.
To maintain the research framework perspective, the first step was to stratify the data sources based on the population of interest. There were four broad categories of dementia based on the presence and severity of symptoms: at risk, MCI, general dementia, and AD [4]. Since the study design had a huge impact on how the relationship between the MIND diet and cognitive functioning was discussed, this was the next level of stratification [21]. Finally, a thematic analysis was conducted based on the relationship (or lack thereof) discovered between the MIND diet and cognitive functioning. Broader implications for treatment and prevention were discussed to determine the scope of these findings for dementia at large.
RESULTS
Study selection
Figure 1 summarizes the screening process. The initial search yielded 33 sources. During the initial stage of title and abstract screening five duplicates, one non-English, one non-empirical, and one unavailable article were excluded. Tertiary sources that included primary or secondary sources that were also identified in the search were categorized as duplicates. During the second stage of title and abstract screening, four irrelevant and one title with the wrong independent variable were excluded. Titles were excluded if they did not include the MIND diet and a term relating to cognition. The remaining 20 articles proceeded to full-text screening when three articles were excluded for having a different independent variable, two articles for a different dependent variable, and four articles due to population characteristics. The screening process yielded 11 articles [22, 28–37] to be included in synthesis.
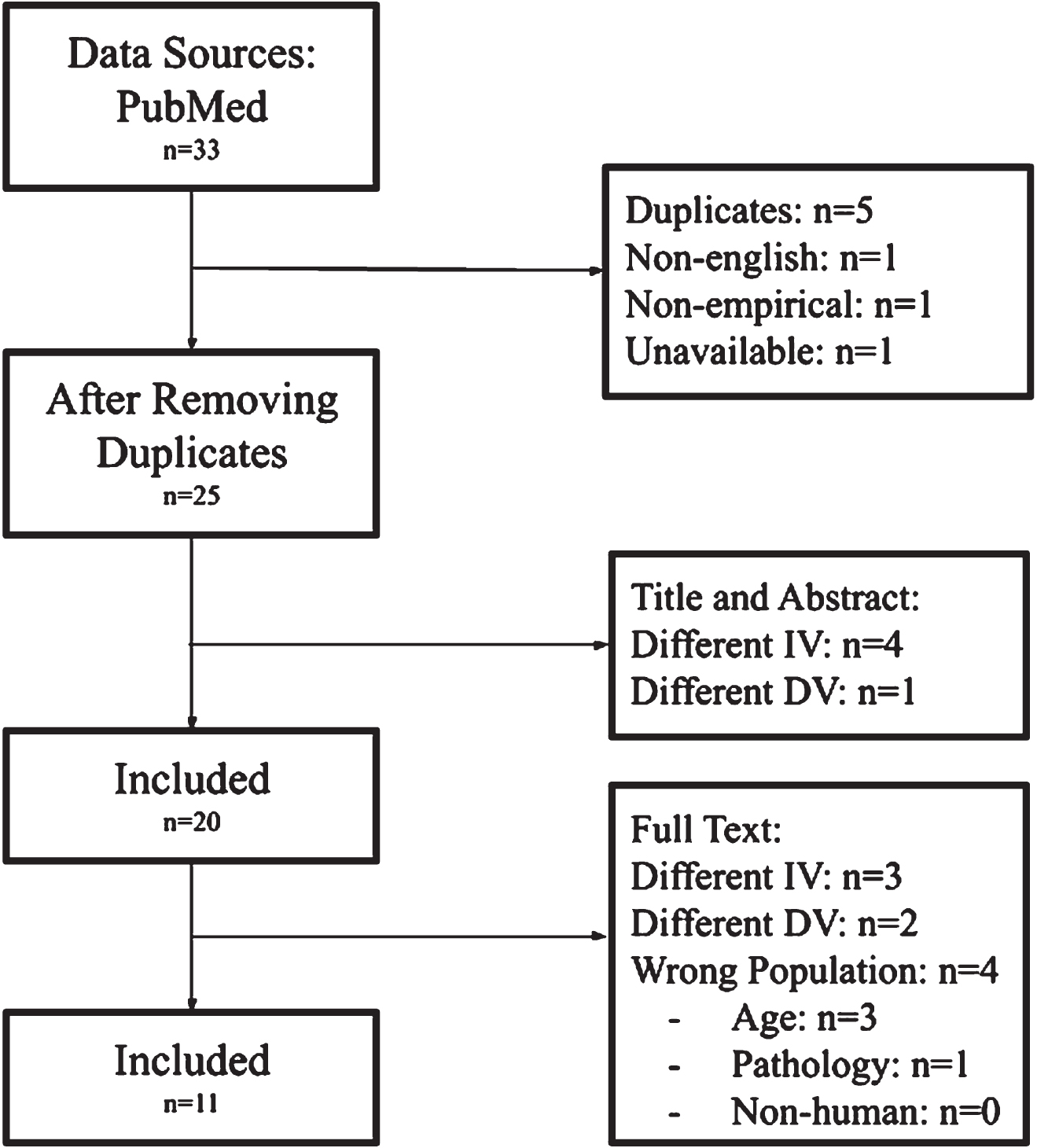
PRISMA diagram.
Study characteristics
The characteristics of each study are described in Table 1. In addition to the charting characteristics previously mentioned, the source population was also included to account for the high volume of secondary analyses. Three of the studies used the Memory and Aging Project for secondary analysis, thus yielding similar findings and covariates. All the studies used the MIND score developed by Morris et al. to measure adherence based on FFQ [16] except for Huang et al. which used the cMIND score which is a score (out of 12) that is tailored to modern Chinese dietary norms [32]. The average MIND diet score for each reference is reported in Table 1. For studies that only reported the median MIND diet score for each quartile, the median scores for each were averaged. Five studies were cohort studies, four studies were longitudinal, one study was cross-sectional, and one study was a systematic review. Follow-up duration ranged from two to 20 years. The sample size ranged from 106 to 16,058. Most of the studies included a majority of women and the mean age varied from 51.8 to 90.8. Two studies [32, 36] used the MMSE exclusively and nine studies used a battery of tests to measure cognitive function. Eight studies included APOE genotyping with various levels of dominance in each study population. A few of the studies also included subjects with comorbidities such as stroke [28], cardiovascular disease [37], and type II diabetes [35]. Common covariates included body mass index, age, sex, APOE status, smoking status, alcohol status, hypertension, diabetes, total energy intake, social interaction, physical activity, and education level. The population in seven studies was characterized as “at risk” [22, 35–37], one study as MCI [32], two studies as general dementia [22, 34], and one as AD [29]. Studies on individuals with various levels of cognitive functioning at baseline were categorized as “general dementia” since many of these subjects likely fit the diagnosis criteria for some form of dementia despite lacking a concrete diagnosis.
Study characteristics of articles studying the impact of the MIND diet on cognition
Analysis
All included studies were assigned a composite quality score based on the merit of their study design and the cognitive assessment(s) used (Table 2). Because none of the study designs had multiple groups or assignment of exposure, these criteria were ignored. For studies using a battery of cognitive tests or a composite test score such as the GCS, the test quality score for each individual test was averaged and then combined with the risk of bias score. For cognitive tests not included in the meta-analysis by Tsoi et al., the sensitivity and specificity scores were outsourced [38–48]. However, the reading and number comparison tests used by Cherian et al. [28] and Dhana et al. [29] do not have adequate normative data on the dementia population, so the quality scores for these studies are incomplete. For the systematic analysis by Gardener & Smith [22], design quality was evaluated based on criteria from A MeaSurement Tool to Assess systematic Reviews (AMSTAR) 2: predetermined protocol, adequacy of the search, and the justification of exclusion criteria [26], none of which were detailed in the Methods section.
Study Quality of Articles Studying the Impact of the MIND Diet on Cognition
ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognition subset; CLHLS, Chinese Longitudinal Healthy Longevity Study; EBMT, East Boston Memory Test; FFQs, Food Frequency Questionnaires; FHS, Framingham Heart Study; GCS, Global Cognition Score; ICDS, Israel Diabetes and Cognitive Decline Study; MAP, Memory Aging Project; MMSE, Mini-Mental State Examination; MRI, magnetic resonance imaging; NHS, Nurses’ Health Study; SNAC-K, Swedish National Study on Aging and Care in Kungsholmen; STICS-m, Spanish version of the TICS-adaptation of MMSE; SUN; Seguimiento Universidad de Navarra; TICS, Telephone Interview for Cognitive Status; TMT, Trail Making Test; WAIS, Weschler Adult Intelligence Scale; CERAD-WL, Consortium to Establish a Registry for Alzheimer’s Disease Word List; WMS, Weschler Memory Scale
Synthesis
The overall findings were heterogeneous with seven studies finding a correlation between adherence to the MIND diet and improved cognitive performance and four studies finding mixed results depending on the cognitive domain. A positive correlation was found between adherence and overall cognitive function in five studies. Results were mixed within the six cognitive domains. In particular, two studies found a positive correlation between adherence and executive function, but Fererra et al. [31] found a negative correlation within the low-income subpopulation of the study. Results were also mixed for GCS, with five studies finding a positive correlation (including the high-income subpopulation of the Fererra et al. [31] study), Berendesen et al. [34] finding no association, and Fererra et al. finding a negative correlation within the low-income subpopulation. There was no trend between overall findings and study design or population pathology.
DISCUSSION
Implications
Nearly everyone is affected by dementia in some way, yet we lack any concrete treatments or prevention methods. Understanding the impact of the MIND diet on cognition in those with dementia may help to create a nutrition-based treatment for dementia. Although the results of this study varied by the cognitive domain, all the studies found a positive correlation between adherence to the MIND diet and some measure of cognition, which suggests that the MIND diet may be protective of cognition. The mixed results with respect to the individual cognitive domains is likely due to the fact that the cognitive tests are designed to be conducted in combination, so analyzing each test in this way may be inappropriate. These findings are consistent with the existing literature, yet it extends the relationship to pathologies across the dementia spectrum.
Since the studies were longitudinal, many of the studies looked at the relationship between the degree of adherence and the degree of cognitive decline. All these studies found a positive correlation. This means that following the MIND diet more strictly, may be more cognitively protective. Moreover, a 2023 study by Agarwal et al. found a correlation between MIND scores and lower global AD pathology, specifically amyloid-β load (a key marker of AD) in those with postmortem AD diagnosis. Additionally, this study found that green leafy vegetables had the largest impact on global AD pathology, suggesting that green leafy vegetables may be a key aspect of the MIND diet in terms of potentially preventing or treating AD [49].
The longitudinal nature of the sources also suggests that the MIND diet may impact changes in cognition over time. Since the study participants fell into four main pathologic categories (at risk, MCI, general dementia, and AD), the scope of these findings is applicable to a broad array of dementias. Although the studies characterized as “at risk” [28, 35–37] excluded those with dementia at onset, many of these participants likely developed some form of dementia over the course of the study. Among these studies, those with higher adherence had better cognitive functioning, suggesting that the MIND diet may be able to preserve cognition in “at risk” individuals. Similarly, Huang et al. [32] found a positive correlation in individuals with the Chinese equivalent of MCI, suggesting that the MIND diet may be able to prevent or slow cognition loss in this population. Two studies [22, 34] in this review included subjects with various levels of cognitive function at baseline, meaning that many of these individuals likely fit the criteria for some form of dementia. These studies also found a positive correlation, suggesting that the MIND diet may be able to slow disease progression. Lastly, one paper by Dhana et al. [29] found a positive correlation in those with postmortem AD diagnosis, suggesting that the MIND diet may be able to preserve cognition in those with AD, thus prolonging quality of life.
Considering that the MIND diet may be able to preserve cognition in those with many forms of dementia, the MIND diet may also be able to preserve quality of life, thus reducing the burden of older individuals on the public [32]. However, it cannot be ignored that Berendesen et al. [34] found no association between MIND adherence and GCS. This study had strong methodology and it included the largest sample size among the studies. The analysis between adherence and GCS produced a p-value of 0.03, which was deemed insignificant in the study. However, these findings may be attributable to the large age range and MIND score range (2.6-11) among participants. This study also only included women, suggesting that the impact of the MIND diet may be augmented by sex. Lastly, Ferrera et al.’s [31] study found contradicting results based on the income of the participants, suggesting that income may be a possible confounder in this relationship.
Limitations
The largest limitation of the data sources was the sex and race distribution. Since many of the studies included a far greater proportion of female subjects, the generalizability of this data to men is limited. However, women are at greater risk of developing many forms of dementia likely due to their longer lifespan and various biological sex differences [50], so the sex distribution of the studies is somewhat justifiable. Likewise, many of the studies included almost exclusively white participants, so these findings may not be applicable to people of other racial and ethnic backgrounds. Additionally, the reliance on FFQs for intake information undermines the accuracy of the adherence data [21]. This likely explains why there are so few studies on those with a formal dementia diagnosis, since the risk of reporting bias is elevated in this population. Therefore, alternative means of measuring adherence or more direct interventions such as randomized controlled trials are required to study those with cognitive impairment. As previously mentioned, there was only one paper on those with AD, meaning that the findings of this paper may not be representative of the AD population at large.
In terms of this systematic review, the general aging population was excluded, meaning that the findings may not be applicable to those without onset dementia or significant risk factors. However, the prevalence of the major risk factors of dementia is incredibly high. Additionally, the level of cognitive functioning at baseline was unclear in many of the studies, thus making it difficult to accurately categorize sources by pathology. Moreover, the comparability of study groups and the assignment of the exposure and control criteria from the Newcastle-Ottawa Scale were not applicable to the study designs of the sources, thus why the scale was used as a general framework and tailored rather than a strict numerical scale [25]. The normative data is not standardized for each cognitive test, thus limiting this study’s replicability. Lastly, limiting the search to titles that included the desired terms undeniably neglected some relevant sources. However, this issue is somewhat unavoidable, so controlling what types of sources are restricted from the source is vital and this decision ensures that the MIND diet remains at the heart of this study.
Conclusion
One opportunity for future research is to better understand the interaction between dementia and comorbidities, specifically metabolic conditions. The pathways of interaction between metabolic conditions such as hypertension, obesity, and diabetes are well researched, but the mechanisms of their interaction with dementia are unknown. This issue is especially potent since the MIND diet is derived from the DASH diet which strives to address these metabolic pathologies. If these mechanisms were better understood, the role of specific dietary components shared by the MIND and DASH diets could be better utilized. There is also an urgent need for a greater degree of consistency in cognitive testing. Although it is advantageous to use a variety of cognitive tests in order to test all cognitive domains [42], the lack of consistency in the tests used in each battery makes it difficult to compare results. This inconsistency could be minimized if one composite cognition score or battery of tests was universally adopted. Additionally, normative data is lacking for many of these tests on the dementia or general aging population, so the strength of these tests in dementia detection may be lacking.
Footnotes
ACKNOWLEDGMENTS
This was a solo review, but all activity was overseen by Dr. Jessica Holzer through HLTH 3370: Research Design and Writing II at the University of New Haven.
FUNDING
The author has no funding to report.
CONFLICT OF INTEREST
The author has no conflicts of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article and/or its supplementary material.