
Abstract
Background:
Higher allostatic load (AL), a multi-system measure of physiological dysregulation considered a proxy for chronic stress exposure, is associated with poorer global cognition (GC) in older non-Hispanic white adults. However, evidence of these associations in middle-aged and older US-based Hispanic/Latino adults is limited.
Objective:
To examine associations of AL with level of cognition, performance in cognition 7 years later, and change in cognition over 7 years among middle-aged and older US-based Hispanic/Latino adults.
Methods:
We used data (n = 5,799, 45–74 years at baseline) from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) and SOL-Investigation of Neurocognitive Aging (SOL-INCA). The AL score comprised 16 biomarkers representing cardiometabolic, glucose, cardiopulmonary, parasympathetic, and inflammatory systems (higher scores = greater dysregulation). Cognitive outcomes included GC and individual tests of verbal learning and memory, world fluency (WF), Digit Symbol Substitution (DSS), and Trail Making (Parts A & B). Survey-linear regressions assessed associations of AL with performance in cognition at baseline, 7 years later, and via 7-year cognitive change scores adjusting for sociodemographic characteristics, lifestyle factors, and depressive symptoms.
Results:
Higher AL was associated with lower baseline performance in GC and WF; and lower 7-year follow-up performance in these same measures plus DSS and Trail Making Parts A & B. Higher AL was associated with more pronounced 7-year change (reduction) in GC and on WF and DSS tests.
Conclusions:
Findings extend previous evidence in predominantly older non-Hispanic white cohorts to show that AL is related to level of and change in GC (as well as WF and DSS) among middle-aged and older US-based Hispanic/Latino adults.
INTRODUCTION
Allostatic load, generally known as a biological index of “wear and tear,” is a multi-system measure of physiological dysregulation considered a proxy for chronic stress exposure [1, 2]. This “load” is generally operationalized as a total score comprised of multiple biological systems, including indicators related to lipid and glucose metabolism, inflammation, and cardiopulmonary, neuroendocrine, and parasympathetic functioning. Allostatic load has been shown to be a stronger predictor of health outcomes compared to its individual biomarkers [3] and other related composite scores such as the metabolic syndrome across populations, including non-Hispanic white [3] and Hispanic/Latino populations [4]. Therefore, in the minority health and health disparities literature [5, 6], the allostatic load construct is generally used to examine the biological pathways through which stressful life experiences may impact health, well-being, and aging. Despite its hypothesized central role in stress responses, allostatic load is understudied in the context of cognitive function in minoritized populations, especially Hispanic/Latino adults [7–14].
To date, most studies on allostatic load and cognitive function have employed a cross-sectional design [8, 10–13], solely included older adults aged 65 and older [8, 14], and focused almost exclusively on non-Hispanic white samples [7–9, 14], with a few exceptions that had a small representation of Hispanic/Latino adults (ranging from 6% [12] to 21% [10] of the total sample). These studies have reported that higher allostatic load is associated with worse global cognition [8, 13] and greater risk for decline in global cognition [9, 14]. Further, higher allostatic load has been shown to be cross-sectionally associated with lower performance across measures of executive function and processing speed [7, 11] and a semantic knowledge-based composite score [8]. In contrast, findings on the association of allostatic load with memory have been mixed with some studies showing an association [11, 12] but others reporting null findings [7, 8]. Furthermore, the generalizability of the current evidence on the associations between allostatic load and cognitive function to middle-aged and older US-based Hispanic/Latino adults of diverse backgrounds has not been established. Given the high burden of chronic stressors reported by Hispanic/Latino adults living in the US [15–22], in part, due to effects of structural racism contributing to social disadvantage [23, 24], the generalizability of previous studies on the relationship between allostatic load and cognition among older non-Hispanic white adults to middle-aged and older Hispanic/Latino adults remains unclear. Moreover, the higher education and income levels among non-Hispanic white adults compared to Hispanic/Latino adults may also limit the generalizability of previous studies on older non-Hispanic white adults to middle-aged and older Hispanic/Latino adults.
To address the aforementioned gaps in the literature, we used data from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) [25, 26] and its Study of Latinos-Investigation of Neurocognitive Aging (SOL-INCA) ancillary study [27] to examine the associations of baseline allostatic load with level of cognition, performance in cognition 7 years later, and change in cognition over 7 years among middle-aged and older Hispanic/Latino adults living in the US. In addition to the outcome of global cognition, we evaluated individual tests of verbal learning and memory, word fluency, executive function, and processing speed. We also explored whether sex modified the associations of interest given previously documented sex differences in the subjective and objective experience of stress [28, 29], previous HCHS/SOL findings showing sex differences in cognition [30] and allostatic load [31], and more pronounced associations between higher cardiovascular risk and worse cognition in women (compared to men) [32]. The HCHS/SOL, one of the largest epidemiological studies of the health of US-based Hispanic/Latino adults, and its SOL-INCA ancillary study, present an opportunity to address previous calls [5, 6] for prospective research on the applicability of the allostatic load framework to examine health outcomes in racial and ethnic populations that have been historically minoritized in the US.
MATERIALS AND METHODS
Study design and analytic sample
The HCHS/SOL is a multi-center, prospective cohort study of community-dwelling Hispanic/Latino adults (ages 18–74 years at recruitment). During the baseline examination (2008–2011), 16,415 participants were recruited from field centers located in four major US metropolitan areas (Bronx, NY; Chicago, IL; Miami, FL; and San Diego, CA). The cohort includes participants who self-identified as having Cuban, Central American, Dominican, Mexican, Puerto Rican, South American, or more than one or other Hispanic/Latino background. The overall HCHS/SOL objective is to identify risk and protective factors associated with chronic conditions in US-based Hispanic/Latino adults of diverse backgrounds. Sociodemographic characteristics, lifestyle factors, depressive symptoms, and allostatic load biomarkers were obtained at baseline. Cognitive function measures were also administered at this time among participants aged 45–74 years.
Details of the baseline study design and sampling strategy have been previously published [25, 26]. Briefly, the HCHS/SOL target population is defined as non-institutionalized Hispanic/Latino adults, aged 18–74 years, residing in specific geographical areas (i.e., Census block groups) across the four field centers. The selection of Census block groups was designed to provide diversity among participants in terms of socioeconomic status and national origin. Participants were selected using a probability sampling design to obtain a representative sample of the target population. A stratified two-stage area probability sample of household addresses was selected in each field center. The first sampling stage randomly selected Census block groups with stratification based on proportion of high/low socioeconomic status, while the second stage randomly selected households with stratification from US Postal Service registries that covered the selected Census block groups. Both stages oversampled certain strata to increase the likelihood of selecting a Hispanic/Latino household. After households were sampled, in-person or telephone contacts were made to screen eligible households and to roster its members. The study also oversampled the 45–74 age group to facilitate examination of target outcomes. Consequently, participants included in the HCHS/SOL cohort were selected with unequal probabilities of selection, and these probabilities are taken into account during data analysis to appropriately represent the target population.
The SOL-INCA study, an ancillary study to the HCHS/SOL, was designed to examine cognitive functioning among a subset of participants [27] and conducted in parallel to the second HCHS/SOL visit (2015–2018). Briefly, participants who completed baseline cognitive testing during HCHS/SOL and returned for HCHS/SOL Visit 2, were aged 50 years and older at Visit 2, and consented to participate were eligible to participate in SOL-INCA [27]. All participants provided informed consent, and study protocols were approved by Institutional Review Boards at each study site and institution. Study procedures involving human subjects were conducted in accordance with the 1975 Helsinki Declaration. The HCHS/SOL Coordinating Center generated INCA-specific probability weights to allow for the generalization of estimates to the SOL-INCA target population (individuals age 50+ years at the second visit) in the HCHS/SOL target area and to account for any bias due to non-response (e.g., mortality). All statistical analyses were conducted using the complex survey design elements (i.e., probability weights, clustering, and stratification) of SOL-INCA.
The current study focused on SOL-INCA participants (N= 6,377), including 5,945 individuals who had at most 2 missing allostatic load component biomarkers (in accordance with the HCHS/SOL previous definition of allostatic load [31]). From those, we excluded 133 individuals who had any missing covariates and 15 individuals whose fasting time before the examination was less than 8 hours. The final analytic sample of this study was 5,797 participants.
Study measures
Cognitive function. Trained interviewers administered the cognitive battery in the preferred language of the participant (i.e., English or Spanish). Neurocognitive tests administered at baseline (and the scores of interest) included the Brief- Spanish English Verbal Learning Test (B-SEVLT-Sum and B-SEVLT-Recall); Word Fluency (WF); and Digit Symbol Substitution (DSS). Briefly, as previously described in detail [30], the B-SEVLT was used to assess verbal episodic learning and memory starting with a 15-item list (i.e., list A) which was read in 3 consecutive learning trials, followed by a distractor list, then immediately by a memory trial to assess free-recall post-interference [33, 34]. B-SEVLT-Sum (range: 0–45) is the sum of the number of items correctly recalled from list A in the 3 learning trials. B-SEVLT-Recall (range: 0–15) is the sum of the number of items correctly recalled post-interference (in a maximum of 60 seconds per trial). The B-SEVLT was originally developed for use in English and Spanish. To assess WF [35, 36], interviewers asked participants to generate as many words as possible starting with the letter F in the first trial and the letter A in the second trial (in a maximum of 60 seconds per trial); the WF score (range: 0–50) is the sum of correctly generated words in both trials. DSS [37] assessed mental processing speed; participants had the option of recalling words in English and Spanish. The DSS score (range: 0–83) is the sum of correctly identified and transcribed symbols based on the key provided to participants (in a maximum of 90 seconds).
To evaluate cognitive change, the above cognitive battery was repeated at SOL-INCA approximately 7 years later, along with two additional tests measuring executive functioning (i.e., Trails Making Test Parts A and B [38]). All tests were z-score transformed ([X-Mean]/SD) relative to each visit’s target population to facilitate the interpretation of results across a common metric. Trails Making Test Parts A and B were reverse coded to allow higher values to represent better performance across all cognitive tests. A global cognitive function composite score was generated by averaging the z-scores of the above tests (excluding Trails Making Test parts A and B) for baseline and SOL-INCA, respectively. For the repeated cognitive measures and the global measure of cognition, a cognitive change score indicator was generated using regression-based techniques. Specifically, weighted linear regressions were used to predict cognitive performance at SOL-INCA (raw scores for the repeated individual tests and the z-scored average for the global cognition) as a function of cognitive performance at baseline, adjusting for lapsed time between cognitive assessments. Test-specific measures of change and global cognitive change were calculated using (T2 - T2pred)/RMSE, where T2 represents a participant’s score on a cognitive test at SOL-INCA, T2pred is the predicted score from the regression model specified above, and RMSE is Root Mean Squared Error of the fitted model. Detailed rationales for this regression-based technique have been published previously [39].
Allostatic load. In accordance with a previous HCHS/SOL descriptive study on allostatic load in our cohort [31], we operationalized allostatic load based on the count-based method (one of the most commonly used methods in the literature [6]) which counts the number of biomarkers in the high risk quartile. Briefly, the baseline allostatic load score (range: 0–16) was constructed using values of the following 16 different biomarkers (summarized in Table 1), representing 5 subsystems: 1) cardiometabolic/lipid metabolism: body mass index (BMI), waist-to-hip ratio (WHR), serum triglycerides, and fasting levels of high- and low-density lipoprotein cholesterol (HDL-c and LDL-c); 2) glucose metabolism: fasting plasma glucose (FPG), blood glycosylated hemoglobin (HbA1c), and homeostatic model assessment of insulin resistance (HOMA-IR); 3) cardiopulmonary measures: systolic blood pressure (SBP), resting pulse pressure, resting heart rate, and lung function (% FEV1/FVC); 4) parasympathetic measures: two ultra-short time domain measures of heart rate variability (HRV), including the square root of the mean squared difference of successive NN intervals and the standard deviation of NN intervals; and 5) inflammation: high-sensitivity C-reactive protein (hs-CRP) and total white blood cell count (WBC). Allostatic load biomarkers were collected using standardized protocols during the HCHS/SOL baseline examination; details of laboratory methods are described on the study website (www2.cscc.unc.edu/hchs/).
The allostatic load construct: Distribution of the allostatic load biomarkers, Hispanic Community Health Study/Study of Latinos (HCHS/SOL; n = 5,797)
The allostatic load construct: Distribution of the allostatic load biomarkers, Hispanic Community Health Study/Study of Latinos (HCHS/SOL; n = 5,797)
High risk cut-points were derived from the bottom 25th percentile for high-density lipoprotein cholesterol, lung function, and heart rate variability measures; the top 75th percentile was used for all other biomarkers. *Biomarker was defined as high risk if the participant was taking medication to lower these biomarkers.
Based on the count-based method, each allostatic load biomarker was assigned a score of one if its value reached the high risk quartile; the high risk quartile was defined as the lowest quartile for HDL, FEV1/FVC, and HRV, and as the highest quartile for all other biomarkers. Participants taking medications designed to lower the value of a specific biomarker were categorized as high risk regardless of the biomarker value. Specifically, these medications and its biomarkers were: a) anti-diabetes medications for FPG and HbA1c, b) anti-hypertension medications for SBP, c) β-blockers for heart rate, d) fibrates for serum triglycerides, and e) statins, cholesterol absorption inhibitors, niacin, and/or bile acid sequestrants for LDL-c. The allostatic load score (range 0–16) and its five subsystem scores outlined above were then calculated by summing across values of the corresponding biomarkers (continuous variable); higher scores represent greater dysregulation (greater health risk). Given that the count-based scoring method depends on the distribution of the study sample, in sensitivity analyses, we applied two alternative definitions of allostatic load. The first alternative definition incorporated clinically defined thresholds when available to define high risk, while the second one excluded medication use from the primary count-based definition.
Covariates. Covariates were identified a priori based on a review of relevant literature and all were assessed at baseline. Covariates included sociodemographic factors: self-reported age, sex (female, male), education (less than high school, high school or equivalent, greater than high school), Hispanic/Latino background (Dominican, Central or South American, Cuban, Mexican, Puerto-Rican, or more than one or other heritage), annual household income (< $20,000, $20,000–$50,000, > $50,000, or not reported), language preference for baseline examination (Spanish or English), field center (Bronx, Chicago, Miami, or San Diego), and years living in the US; lifestyle factors: diet quality, cigarette usage, meeting physical activity guidelines, and alcohol usage, and mental health: depressive symptoms. Participants who declined to report their household income were included as a category to avoid deleting those observations. Dietary intake was assessed via two 24-hour dietary recalls administered by trained interviewers [40]. The 2010-Alternate Healthy Eating Index (AHEI), as an indicator of diet quality, was computed based on servings/day of vegetables (not including potatoes), whole fruit, whole grains, sugar-sweetened beverages and fruit juices, nuts and legumes, red/processed meats, trans fats, long-chain (n-3) fats, polyunsaturated fatty acids, alcohol, and sodium [41]. Self-reported cigarette use was classified as never, former, or current [42]. Physical activity in a typical week was assessed using the Global Physical Activity Questionnaire (GPAQ) [43] and categorized according to adherence to the 2008 US Guidelines for meeting high or medium activity levels [44]. Adherence included high activity (i.e., >300 min/week of moderate-intensity physical activity, or > 150 min/week of vigorous activity, or a combination of both) and medium activity (i.e., 150–300 min/week of moderate-intensity activity, or 75–150 min/week of vigorous-intensity physical activity, or combination of both). Lack of adherence included low activity (i.e., activity beyond baseline but < 150 min/week of moderate-intensity physical activity, or < 75 min/week of vigorous-intensity activity, or a combination of both) and inactivity (i.e., no activity beyond baseline activities of daily living). Participants were classified according to self-reported alcohol consumption (current, former, or never) [45]. Depressive symptoms were assessed with a 10-item version of the Center for Epidemiologic Studies Depression scale [46].
Analytic approach
Four major steps were followed to conduct the statistical analysis of this study, including descriptive statistics, and main, secondary, and sensitivity analyses— as described in detail below. First, we estimated the survey-weighted mean values for each allostatic load biomarkers for the overall analytic population and by sex (Table 1). We also estimated descriptive statistics for the overall analytic population and according to sex; the group differences by sex were tested using survey-adjusted Wald-tests and chi-square tests for continuous and categorical variables, respectively (Table 2). Second, in our main analysis, to examine the hypothesized associations of allostatic load with cognition at baseline, 7 years later, and based on 7-year cognitive change, we fit a series of multivariable survey linear regressions adjusting for: 1) age, sex, education, Hispanic/Latino background, annual household income, language preference, years living in the US, and field center (i.e., Model 1: Sociodemographic factors); and 2) additionally, diet quality, cigarette usage, physical activity, alcohol usage, and depressive symptoms (i.e., Model 2: Sociodemographic factors + lifestyle factors + depressive symptoms). Of note, time between study visits was not included as a covariate since it was included in the calculations of the change in cognition variables, as previously described. While the estimated coefficients and their standard errors for our minimally adjusted Model 1 are presented in Tables 3 to 4, we focus on the fully adjusted Model 2 given that there were only small changes in the estimated coefficients (and statistical significance tended to persist) with sequential adjustment. In post-hoc analyses, we calculated average marginal estimates and plotted these with their 95% confidence intervals to facilitate interpretation of results (Figs. 1–3). We then tested for modifications by sex in the associations of allostatic load with cognitive outcomes using the same sequence of model adjustments specified above, but with the addition of the sex by allostatic load interaction term (Table 5). For the significant interactions, we estimated and graphed marginal means and their 95% confidence intervals to facilitate the interpretation of results (Supplementary Figures 1 and 2).
Baseline characteristics, Hispanic Community Health Study/Study of Latinos (HCHS/SOL; n = 5,797)
Sample size is unweighted; all other reported values are weighted to represent the target population. Diet quality was assessed based on the 2010 Alternative Healthy Eating Index (AHEI-2010; range: 0 to 110). Physical activity was assessed based on the Global Physical Activity Questionnaire (GPAQ); participants were classified according to adherence to the 2008 US Guidelines for meeting high or medium activity levels. Meeting physical activity guidelines included high activity (i.e., >300 min/week of moderate-intensity physical activity, or > 150 min/week of vigorous activity, or a combination of both) and medium activity (i.e., 150–300 min/week of moderate-intensity activity, or 75–150 min/week of vigorous-intensity physical activity, or combination of both). Depressive symptoms were assessed using the 10-item Center for Epidemiologic Study of Depression (CESD-10) scale (range: 0 to 30). The allostatic load score range is 0 to 16, and range of its sub-systems is the following = cardiometabolic risk: 0 to 5; glucose metabolism: 0 to 3; cardiopulmonary functioning: 0 to 4; parasympathetic functioning: 0 to 2; inflammation score: 0 to 2.
Associations of allostatic load with cognitive function (z-scores) at HCHS/SOL baseline and 7-year cognitive change (z-scores) from HCHS/SOL Baseline to SOL-INCA (n = 5,797)
Bolded values denote statistical significance. *p < 0.05, **p < 0.01, ***p < 0.001. Model 1: Age, sex, education, Hispanic/Latino background, household annual income, language preference, years living in the US, and field center. Model 2: Model 1 + diet quality, cigarette usage, physical activity, alcohol use, and depressive symptoms. B-SEVLT, Brief Spanish English Verbal Learning Test; WF, Word Fluency; DSS, Digit Symbol Substitution; Δ, change.
Associations of allostatic load with 7-year cognitive performance (z-scores) at SOL-INCA (n = 5,797)
Bolded values denote statistical significance. *p < 0.05, **p < 0.01, ***p < 0.001. Model 1: Age, sex, education, Hispanic/Latino background, household annual income, language preference, years living in the US, and field center. Model 2: Model 1 + diet quality, cigarette usage, physical activity, alcohol use, and depressive symptoms. B-SEVLT, Brief Spanish English Verbal Learning Test; WF, Word Fluency; DSS, Digit Symbol Substitution. Trails A and Trails B were reverse-coded; higher value indicates better performance.
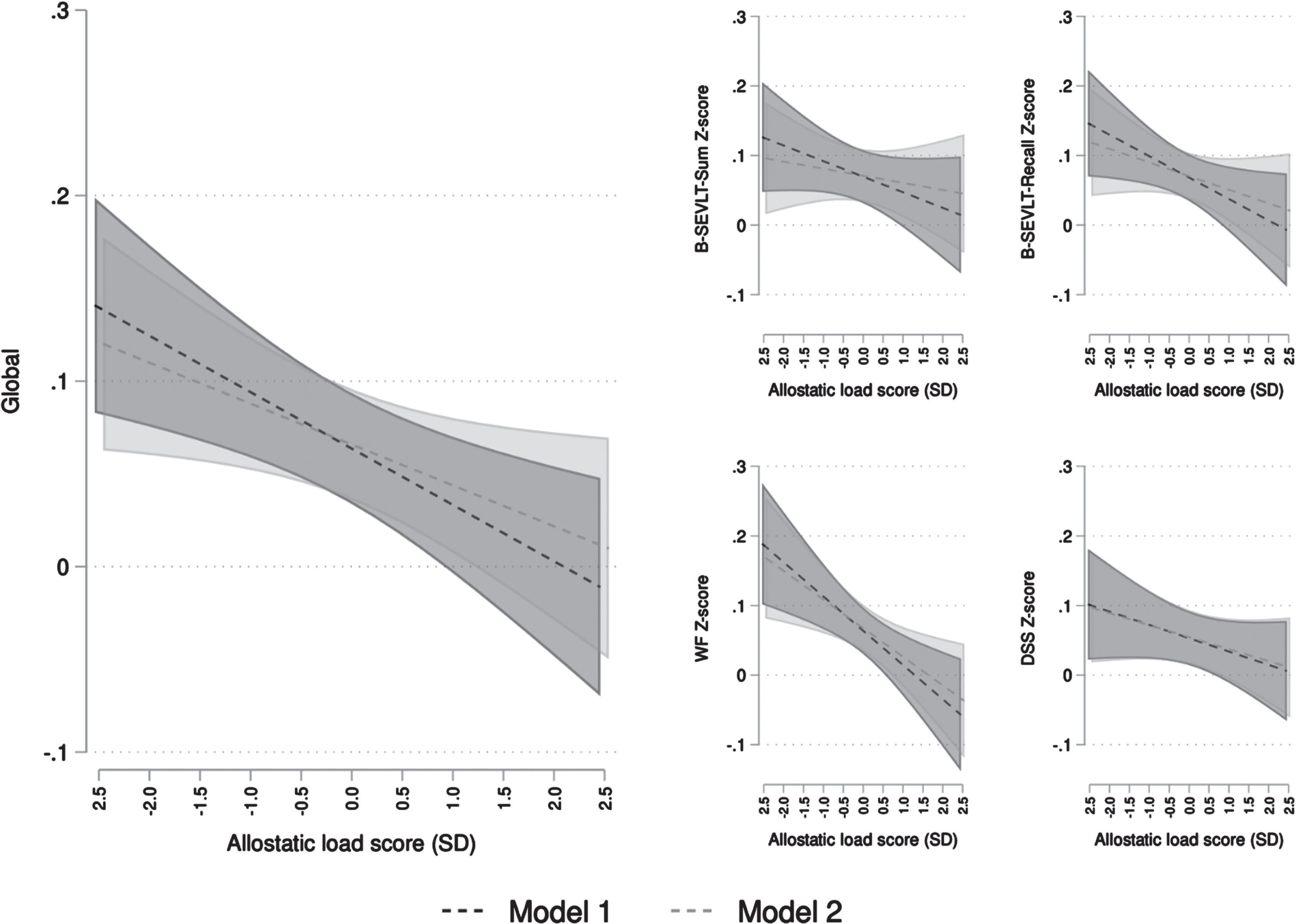
Estimated marginal means (Average Marginal Effects; AMEs) and 95% confidence intervals for the associations between allostatic load and cognitive function (z-scores) at HCHS/SOL Visit 1 (n = 5,797). Results are derived from survey generalized linear models. Model 1 adjusted for age, sex, education, ethnicity, income, language preference, years in the US, field center. Model 2 additionally adjusted for diet quality, cigarette usage, physical activity, alcohol use, and depressive symptoms. B-SEVLT, Brief Spanish English Verbal Learning Test; WF, Word Fluency; DSS, Digit Symbol Substitution; SD, Standard Deviation.
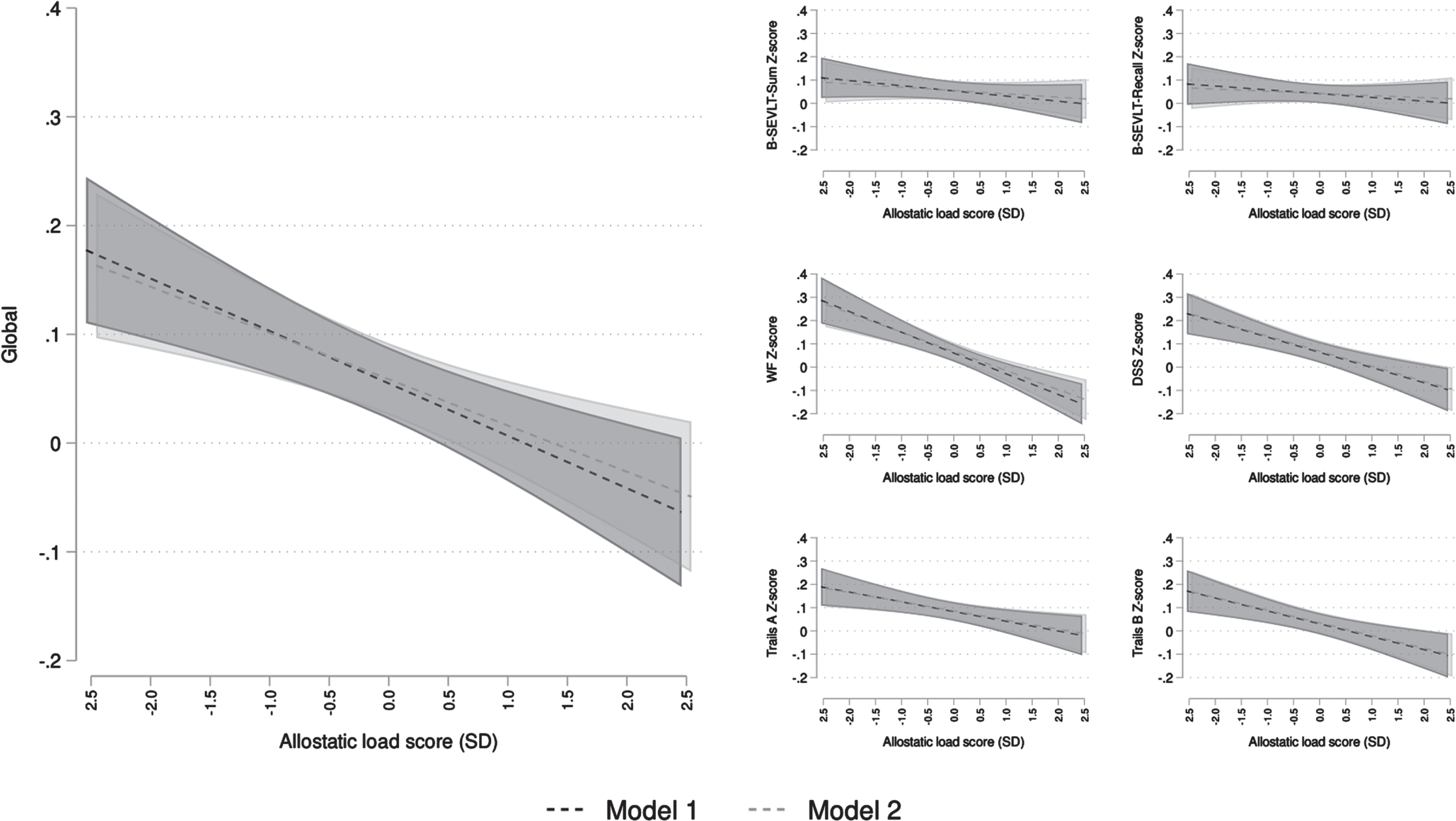
Estimated marginal means (Average Marginal Effects; AMEs) and 95% confidence intervals for the associations between allostatic load and cognitive performance (z-scores) at SOL-INCA (n = 5,797). Results are derived from survey generalized linear models. Model 1 adjusted for age, sex, education, ethnicity, income, language preference, years in the US, field center. Model 2 additionally adjusted for diet quality, cigarette usage, physical activity, alcohol use, and depressive symptoms. B-SEVLT, Brief Spanish English Verbal Learning Test; WF, Word Fluency; DSS, Digit Symbol Substitution; SD, Standard Deviation.
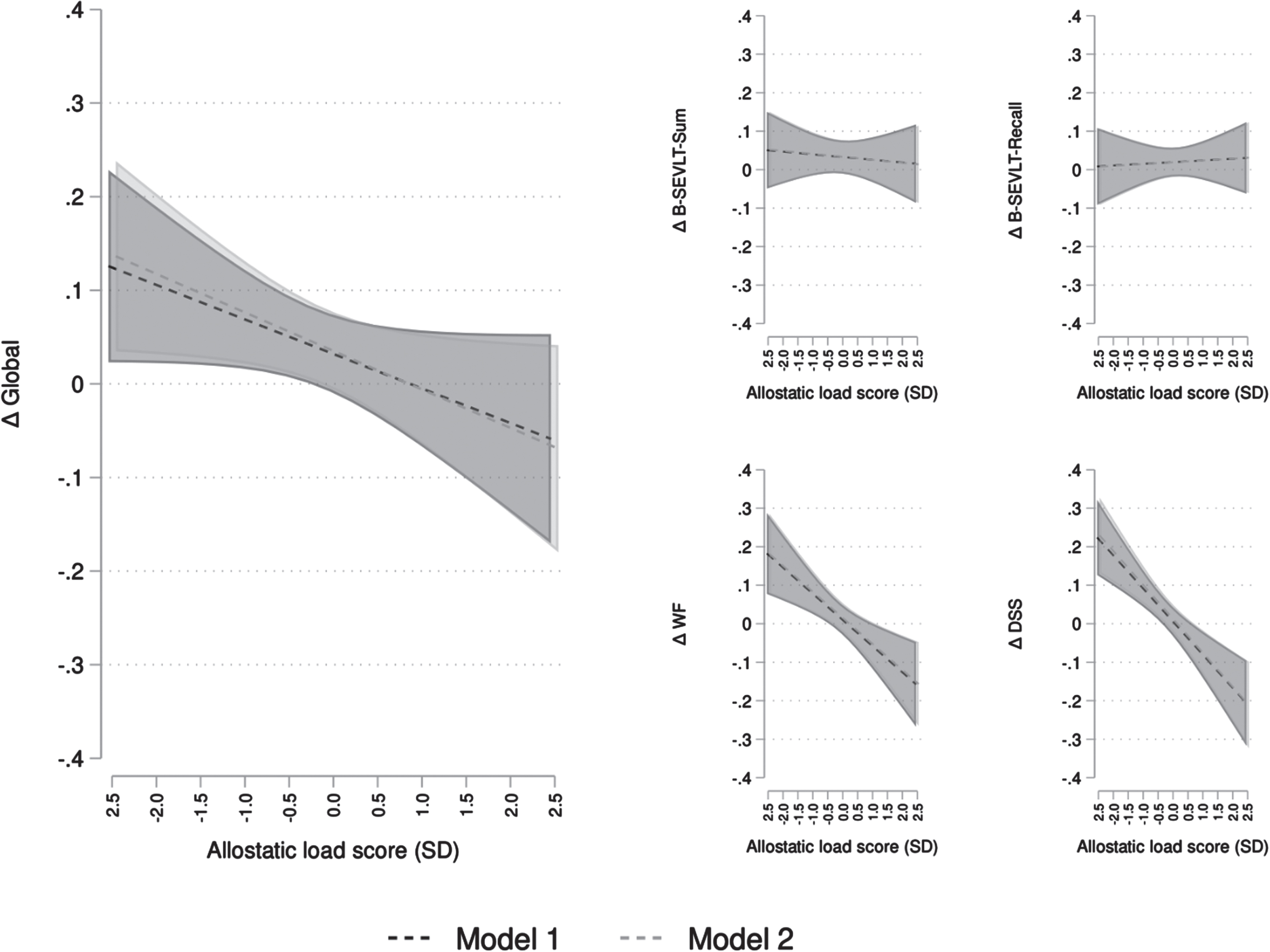
Estimated marginal means (Average Marginal Effects; AMEs) and 95% confidence intervals for the associations between allostatic load and 7-year cognitive change from HCHS/SOL Visit 1 to SOL-INCA (n = 5,797). Results are derived from survey generalized linear models. Model 1 adjusted for age, sex, education, ethnicity, income, language preference, years in the US, field center. Model 2 additionally adjusted for diet quality, cigarette usage, physical activity, alcohol use, and depressive symptoms. B-SEVLT, Brief Spanish English Verbal Learning Test; WF, Word Fluency; DSS, Digit Symbol Substitution; SD, Standard Deviation; Δ, change.
Sex modifications in the associations of allostatic load with cognitive outcomes at Baseline, 7-years later at SOL-INCA, and 7-year cognitive change from HCHS/SOL Baseline to SOL-INCA (n = 5,797)
Bolded values denote statistical significance. B-SEVLT, Brief Spanish English Verbal Learning Test; WF, Word Fluency; DSS, Digit Symbol Substitution; Δ, change. The results presented are from the models including sex by allostatic load score interaction and adjusting for sociodemographic factors (i.e., age, education, ethnicity, income, language preference, years in the US, field center), lifestyle factors (i.e., diet quality, cigarette usage, physical activity, alcohol use), and depressive symptoms.
Third, as part of our secondary analyses, we examined the associations of each allostatic load subsystem (i.e., cardiometabolic/lipid metabolism, glucose metabolism, and cardiopulmonary, parasympathetic, and inflammation measures) with cognitive performance at baseline and 7-years later, as well as via 7-year cognitive change. We included all covariates (age, sex, education, Hispanic/Latino background, annual household income, language preference, years living in the US, field center, diet quality, cigarette usage, physical activity, alcohol usage, and depressive symptoms) for adjustments. The estimated coefficients and their standard errors are presented in Supplementary Tables 1–3. Finally, we conducted sensitivity analyses to examine whether our results are robust to different definitions of allostatic load. In our first sensitivity analyses (Sensitivity 1), we operationalized allostatic load while employing clinically relevant cut-off points (if available) instead of quartiles to define high risk as with the former count-based definition, participants taking medications designed to lower values of specific markers were categorized as high risk regardless of biomarker value. Clinical high risk cut-points were not available for HOMA-IR, resting pulse pressure, heart rate variability, and white blood cell count; thus, we used the previously defined high-risk quartiles. Additionally, in our second sensitivity analyses (Sensitivity 2), we operationalized allostatic load solely based on the high-risk quartiles values of the biomarkers, excluding medication use. The survey-weighted summary statistics for the allostatic load score and subsystem scores with alternative definitions are shown in Supplementary Tables 4 and 5. Using the alternative definitions of allostatic load, we examined the associations of allostatic load with cognitive performance at baseline, 7-years later, and using cognitive change scores (Sensitivity 1: Supplementary Tables 6–8, Sensitivity 2: Supplementary Tables 9–11).
All statistical analyses were performed using Stata Statistical Software (Stata Corp LP, College Station, TX). A statistical significance level of p < 0.05 was used. To allow readers to navigate the results generated from all the models and facilitate visualization of the effect sizes across the considered exposures and cognitive outcomes, we developed a Shiny dashboard that is accessible at this address: https://solincalab.shinyapps.io/Allostatic_load/.
RESULTS
Descriptive statistics
Table 1 depicts the continuous distribution of each allostatic load biomarker (overall and stratified by sex). Females had higher mean levels of BMI, HDL-c, LDL-c, resting heart rate, lung function, square root of the mean squared difference of successive NN intervals, hs-CRP, and WBC than males, whereas males had higher mean levels of waist-to-hip circumference ratio, triglycerides, fasting plasma glucose, and systolic blood pressure than females. At baseline, the mean age was 56 years, more than 60% had a high school diploma or above, and approximately 46% had an annual household income of less than $20,000 (Table 2). The average years living in the US was 25 years and 87% preferred Spanish for testing. Nearly 20% were current smokers, 47% reported current alcohol consumption, and 60% met the 2008 US physical activity level guidelines at baseline. Except for the number of reported years living in the US, sociodemographic characteristics were significantly different by sex. For instance, more females (than males) reported an education of less than a high school diploma and an annual household income of less than $20,000. The average allostatic load score (range: 0–16) for the overall analytic population was 4.5. There was a significant group difference by sex in the allostatic load score and cardiometabolic/lipid metabolism, parasympathetic measures, and inflammation subsystem scores. The inflammation score was higher among females, while all other scores were higher among males.
Main analysis
The derived regression estimates for the models linking allostatic load to cognitive outcomes are presented in Tables 3 and 4. In fully adjusted models, higher (i.e., worse) allostatic load was significantly associated with lower performance in GC at baseline (βGC = –0.008, SE = 0.004, p < 0.05) and at 7-year follow-up (βGC = –0.015, SE = 0.004, p < 0.001), and with more pronounced 7-year change (i.e., reduction) in GC (βΔGC = –0.014, SE = 0.007, p < 0.05). Higher allostatic load was significantly associated with lower performance in WF at baseline (βWF = –0.014, SE = 0.005, p < 0.01) and 7-year follow-up (βWF = –0.028, SE = 0.006, p < 0.001), as well as a more pronounced 7-year change (i.e., reduction) in WF (βΔWF = –0.023, SE = 0.007, p < 0.001), regardless of adjustments.
Higher allostatic load was also significantly associated with poorer performance in processing speed and executive functioning via DSS and Trail Making Parts A and B at 7-year follow-up (βDSS = –0.022, SE = 0.006, p < 0.001; βTrailsA = –0.014, SE = 0.005, p < 0.01; βTrailsB = –0.019, SE = 0.006, p < 0.001), and more pronounced 7-year change (i.e., reduction) in DSS (βΔDSS = –0.030, SE = 0.007, p < 0.001); however, allostatic load was not related to baseline DSS scores. No association of allostatic load was detected with either B-SEVLT measure at baseline, 7-year follow-up assessment, or with 7-year change; the only exception was the negative relation between allostatic load and B-SEVLT-Recall at baseline (βB - SEVLT - Recall = –0.011, SE = 0.005, p < 0.05). The marginal means from the main models are presented in Figs. 1–3.
The test statistics from the interaction models investigating sex as an effect modifier of the relations of allostatic load and cognition are presented in Table 5. We found evidence of significant modification by sex only in the associations of allostatic load with baseline GC and WF. Compared to males, female had significantly more pronounced slopes for negative associations between these variables in the final, fully adjusted model (Supplementary Figures 1 and 2).
The derived regression estimates for the models on the relations of each allostatic load subsystem with cognitive outcomes are presented in Supplementary Tables 1–3. Higher (i.e., worse) cardiometabolic/lipid metabolism score was significantly associated with lower WF scores at both baseline (βWF = –0.023, SE = 0.011, p < 0.05) and 7-year follow-up (βWF = –0.043, SE = 0.016, p < 0.01), but not with 7-year change in WF. Higher glucose metabolism score was significantly associated with lower GC at 7-year follow-up (βGC = –0.042, SE = 0.011, p < 0.001) and more pronounced 7-year change (i.e., reduction) in GC (βΔGC = –0.050, SE = 0.020, p < 0.05). It was also significantly associated with lower WF scores at baseline (βWF = –0.028, SE = 0.013, p < 0.05) and 7-year follow-up (βWF = –0.058, SE = 0.015, p < 0.001), and more pronounced 7-year change (i.e., reduction) in WF (βΔWF = –0.047, SE = 0.019, p < 0.05). A significant association of higher glucose metabolism score was additionally found with processing speed and executive functioning measures at the 7-year follow-up (βDSS = –0.053, SE = 0.015, p < 0.001; βTrailsA = –0.035, SE = 0.015, p < 0.05; βTrailsB = –0.050, SE = 0.015, p < 0.001) as well as 7-year change in DSS (βΔDSS = –0.077, SE = 0.020, p < 0.001).
Higher cardiopulmonary functioning score was significantly associated to lower GC at baseline (βGC = –0.023, SE = 0.009, p < 0.05), 7-year follow-up (βGC = –0.039, SE = 0.011, p < 0.001), and 7-year change in GC (βΔGC = –0.036, SE = 0.018, p < 0.05). We also found significant associations of higher cardiopulmonary functioning score with WF (βWF = –0.053, SE = 0.016, p < 0.01), processing speed (βDSS = –0.055, SE = 0.015, p < 0.001; βTrailsA = –0.038, SE = 0.015, p < 0.01) and executive functioning (βTrailsB = –0.030, SE = 0.014, p < 0.05) at the 7-year follow-up, as well as with 7-year change in WF and DSS (βΔWF = –0.046, SE = 0.018, p < 0.01; βΔDSS = –0.070, SE = 0.019, p < 0.001). Higher inflammation score was significantly associated with lower WF (βWF = –0.064, SE = 0.024, p < 0.01) and Trails Part B (βTrailsB = –0.043, SE = 0.022, p < 0.05) at the 7-year follow-up only.
Sensitivity analysis
The summary statistics of allostatic load, operationalized based on the alternative definitions, are presented in Supplementary Tables 4 and 5. The group differences by sex found using the original definitions (i.e., for allostatic load total score and cardiometabolic/lipid metabolism, parasympathetic, and inflammation subsystem scores) remained unchanged. Likewise, results on the associations of the alternative allostatic load scores with cognitive outcomes were consistent in magnitude and direction with the results obtained in the main analyses (Supplementary Tables 6–11).
DISCUSSION
In this study of middle-aged and older US-based Hispanic/Latino adults, we found that higher baseline allostatic load, as defined by a composite score representing biological dysregulation, was associated with lower performance in GC and WF scores at baseline and with more pronounced 7-year change (i.e., reduction) in GC, WF, and DSS, adjusting for sociodemographic characteristics, lifestyle factors, and depressive symptoms. Additionally, higher allostatic load was related to poorer performance in WF, DSS, and Trails Making Parts A & B scores at the 7-year follow-up. Most of the associations documented in this study were consistent across sex, apart from the cross-sectional relations of allostatic load with global cognition and WF, which were stronger in females compared to males. Notably, when examining the allostatic load subsystems, we observed that higher glucose and cardiopulmonary scores were each associated with more pronounced 7-year change (reductions) in GC, WF, and DSS.
Our study contributes to the literature in several ways. First, to our knowledge, this is one of the largest (n = 5,797) and most comprehensive examinations of the associations of allostatic load with level of and change over time in cognitive function (including GC as well as individual tests) among middle-aged and older US-based Hispanic/Latino adults. Second, we confirm previous reports showing that higher baseline allostatic load is associated with level of [8, 13] and change in [9, 14] GC, and extend this work to include middle-aged and older Hispanic/Latino adults— a rapidly growing but understudied segment of the US population. Third, our work adds to the few studies investigating the association between allostatic load and verbal fluency [7, 11], finding novel associations of allostatic load with 7-year change in WF, and pointing towards the need for additional research on the associations of allostatic load with level and change in this and other fluency measures in diverse populations. Fourth, we extend previous cross-sectional research on the associations of allostatic load with aspects of executive function [7, 11] and processing speed [8] to include the associations of allostatic load with performance in these same domains, on average 7-years from baseline, as well as with 7-year change in DSS among middle-aged and older Hispanic/Latino adults. Finally, we highlight that most of these associations are consistent by sex and demonstrate the distinct relations of allostatic load subsystems with cognitive outcomes, including the relatively stronger associations of glucose metabolism and cardiopulmonary functioning scores with 7-year change in GC, WF, and DSS.
The negative associations of allostatic load with level of and change in GC observed in our study are aligned with previous ones conducted in samples of (mostly) non-Hispanic white adults. For instance, higher allostatic load was cross-sectionally associated with poorer GC in primarily non-Hispanic white middle-aged and older adults (ages 44 to 84 years) in the Multi-Ethnic Study of Atherosclerosis (MESA) [10], and older non-Hispanic white adults in the MacArthur Studies of Aging [13] and Lothian Birth Cohort 1936 (LBC1936) [8]. The few studies on the relationships of allostatic load with change in GC have comparably shown that higher allostatic load is associated with faster GC decline in older non-Hispanic white adults in the MacArthur Studies of Successful Aging [14] and LBC1936 [9]. Our study builds on such findings by demonstrating that these relations of allostatic load with level of and change in GC are also present in middle-aged and older Hispanic/Latino adults. Nevertheless, considering the scarcity of longitudinal studies on allostatic load and cognition, future research with additional cognitive outcome time points is needed to reinforce our findings.
Our findings on the relations of allostatic load with specific cognitive test scores agree with some, but not all, previous studies investigating the cognitive domains assessed by our tests. Similar to our findings on the cross-sectional negative relation between allostatic load and WF, higher allostatic load was related to worse performance in an executive function score (comprised of verbal fluency, backward counting, digit span backward, number series, and reaction time tests) among adults, aged 25 to 74 years, in the Midlife in the United States Study (MIDUS) [11] and a semantic knowledge composite score (comprised of reading and verbal fluency tests) in older adults in the LBC1936 [8]. Contrastingly, there was no association of allostatic load with baseline level or change in a test of animal fluency among African American and non-Hispanic white adults, aged 30 to 64 years, in the Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study [7]. Given that some of the previous studies did not include verbal fluency tests [9, 12–14], other solely included verbal fluency tests in composite measures [8, 11], and a lack of studies examining change in verbal fluency, it is difficult to make direct comparisons between our findings and findings from previous studies.
Regarding our null findings on the associations of allostatic load with verbal learning and memory, previous studies have similarly shown that allostatic load is not cross-sectionally related to verbal memory [8] and not prospectively associated with 5-year change in visual memory [7]. In contrast, other studies found a cross-sectional association of higher allostatic load with poorer working memory among adults aged 20 to 59 years in the National Health and Nutrition Examination Survey (NHANES) [12] and poorer verbal episodic memory among adults (ages 49 to 66 years) in the MIDUS study [11]. Although the reasons for dissimilar findings between our study and previous ones are unknown, it is possible that they reflect differences in the samples included across studies. For instance, the NHANES sample [12] was much younger than our HCHS/SOL cohort (median age was 36 years, compared to 56 years in ours) which may limit comparability since allostatic load scores have been shown to increase with age [47]. Another possibility is that differences in findings across studies reflect differences in the operationalization of the allostatic load construct and its biomarkers [48]. For example, the MIDUS study [11] included in their allostatic load variable four measures of neuroendocrine function (i.e., cortisol, norepinephrine, epinephrine, and dehydroepiandrosterone sulfate [DHEA-S]), which are key hormonal agents of the hypothalamic-pituitary adrenal and sympathetic nervous systems previously shown to contribute to hippocampal atrophy and poorer episodic learning and memory performance [49, 50]. These neuroendocrine measures were not available for our HCHS/SOL cohort; thus, future research is needed to examine whether neuroendocrine system measures are related to cognitive level and/or change in Hispanic/Latino adults.
Findings from our secondary analysis on allostatic load subsystems point towards the potential role of glucose and cardiopulmonary functioning subsystems (comprised of FPG, HbA1c, and HOMA-IR; and SBP, resting pulse pressure, resting heart rate, and lung function biomarkers, respectively) on 7-year change in GC, WF, and DSS. Diabetes and hypertension are both related to alterations in whole brain and subcortical structures [51]. Prevalent diabetes was associated with increased mild cognitive impairment prevalence in the SOL-INCA study [52]. Taken together, this supports our findings on the role of worse glucose metabolism on GC decline. Accelerated brain insult, including atrophy and impaired neuronal function, have been proposed as potential mechanisms of the associations of poor glycemic control and type 2 diabetes with worse cognitive function [53, 54]. Further, increased high blood pressure has been related to cerebral hypoperfusion and cortical atrophy [55]. Additionally, worse pulmonary function, assessed based on FEV1/FVC, is associated with lower cognition via reductions in brain volume, gray matter volume, and hippocampal volume [56], possibly due to reduced cerebral blood flow and associated hypoxia and ischemic brain injury [57]. As such, findings from our secondary analysis appear to highlight that improving glycemic control and cardiopulmonary functioning among middle-aged and older Hispanic/Latino adults may be critical public health strategies to reducing the risk of decline in GC and executive function.
The present study has various limitation, including that SOL-INCA is observational in nature, thus, cautious interpretation is warranted. Future research should examine these associations of allostatic load with additional cognitive function follow-up data to determine more conclusively whether allostatic load is an important determinant of cognitive decline in middle-aged and older Hispanic/Latino adults. Another limitation is that we are not able to directly compare the size of the effects observed in our study with previous studies for various reasons, including that our method for calculating cognitive change is not based on simple discrepancy scores and the lack of consensus on the allostatic load score across studies. Overall, our findings are consistent with prior research, as reported in a systematic and meta-analytic review [58], in the relatively modest magnitude and negative direction of the effect sizes. Therefore, they do not necessarily reflect immediate clinical significance at the individual level. However, given the representativeness of this relatively younger cohort and the high burden of mild cognitive impairment and Alzheimer’s disease and related dementias in the rapidly growing US-based Hispanic/Latino population [27], our findings may have important implications related to population-level cognitive decline over time. Related to our findings demonstrating that most of the associations of allostatic load with cognition were not modified by a binary representation of sex, it is important to note that the relations of allostatic load with cognition is complex and may relate to stress-related and sex-related hormones [50]; all of which requires additional investigation in this cohort. Likewise, although beyond the scope of our study, future research is needed to examine whether the associations of interest are modified by Hispanic/Latino background, given previously shown differences in each allostatic load [59] and cognition [30] by Hispanic/Latino background. Finally, while we included the most commonly used allostatic load biomarkers, in the HCHS/SOL cohort neuroendocrine biomarkers (such as cortisol and dopamine) were not available and CRP was the only immune function biomarker available in our study, unlike MIDUS [11] and NHANES III [12] which incorporated Interleukin-6 and Insulin-like growth factor-1; whereas, in terms of the outcomes, additional work is needed to examine language equivalence across the cognitive measures included in our cohort. Strengths of our study include that, to our knowledge, this is one of the first studies on the associations of allostatic load with both level and change in cognition in middle-aged and older US-based Hispanic/Latino adults of diverse backgrounds, and we used a larger sample size (n = 5,797) than most previous studies [7–14] and well-validated instruments to assess cognitive function. Furthermore, we used the traditional allostatic load calculation based on quartile count as originally devised by Seeman et al. (1997) [13]; our sensitivity analysis showed that results remained largely unchanged when two alternative definition of allostatic load were used, highlighting the robustness of our findings.
Conclusions
Our findings extend the evidence base on the associations of baseline allostatic load with poorer GC and faster decline in GC, WF, and processing speed to include US-based middle-aged and older Hispanic/Latino adults. Findings from this study may provide insight into the overall utility of the concept of allostatic load in efforts to better understand health and aging trajectories among middle-aged and older Hispanics/Latinos, a rapidly growing segment of the US population [60] with a disproportionate burden of Alzheimer’s disease and related dementias [27]. Future research is needed to confirm our findings and examine whether lowering allostatic load could be particularly impactful on slowing cognitive decline among middle-aged and older Hispanic/Latino adults [23, 24].
AUTHOR CONTRIBUTIONS
Mayra L. Estrella (Conceptualization; Funding acquisition; Methodology; Writing – original draft; Writing – review & editing); Wassim Tarraf (Data curation; Formal analysis; Methodology; Supervision; Visualization); Sayaka Kuwayama, MS (Formal analysis; Methodology); Linda C. Gallo (Funding acquisition; Methodology; Supervision; Writing – review & editing); Christian R. Salazar (Conceptualization; Writing – review & editing); Ariana M. Stickel (Conceptualization; Writing – review & editing); Josiemer Mattei (Conceptualization; Writing – review & editing); Priscilla M. Vásquez (Conceptualization; Writing – review & editing); Kamal M. Eldeirawi (Writing – review & editing); Krista M. Perreira (Funding acquisition; Writing – review & editing); Frank J. Penedo (Funding acquisition; Writing – review & editing); Carmen R. Isasi (Conceptualization; Funding acquisition; Writing – review & editing); Jianwen Cai (Funding acquisition; Methodology; Writing – review & editing); Donglin Zeng (Methodology; Writing – review & editing); Hector M. González (Conceptualization; Funding acquisition; Methodology; Writing – review & editing); Martha L. Daviglus (Conceptualization; Funding acquisition; Methodology; Writing – review & editing); Melissa Lamar (Conceptualization; Funding acquisition; Methodology; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank all the participants and staff of the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) and the SOL Investigation of Neurocognitive Aging (SOL-INCA) studies for their important contributions and commitment to improving the health of Hispanic/Latino communities.
FUNDING
The Hispanic Community Health Study/Study of Latinos is a collaborative study supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI) to the University of North Carolina (HHSN268201300001I / N01-HC-65233), University of Miami (HHSN268201300004I / N01-HC-65234), Albert Einstein College of Medicine (HHSN268201300002I /N01-HC-65235), University of Illinois at Chicago (HHSN268201300003I / N01- HC-65236 Northwestern Univ), and San Diego State University (HHSN268201300005I/ N01-HC-65237). The following Institutes/Centers/Offices have contributed to the HCHS/SOL through a transfer of funds to the NHLBI: National Institute on Minority Health and Health Disparities, National Institute on Deafness and Other Communication Disorders, National Institute of Dental and Craniofacial Research, National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Neurological Disorders and Stroke, NIH Institution-Office of Dietary Supplements. SOL-INCA received support from the National Institute on Aging (R01AG048642). Melissa Lamar was supported by the National Institute on Aging (R01AG062711). Carmen R. Isasi was supported by the National Institute on Aging (1RF1AG077639). Christian Salazar is supported by the National Institute on Aging (K01 AG076811) and Alzheimer’s Association research fellowship (AARFD-20-682432). Ariana Stickel was supported by the National Institute on Aging (K08AG075351, L30AG074401) and National Cancer Institute (U54CA267789). Mayra L. Estrella was supported by the National Institute on Aging (K01AG075353 and P30AG059305) and National Institute on Minority Health and Health Disparities (L60MD015551).
CONFLICT OF INTEREST
Mayra L. Estrella, Ariana M. Stickel, Hector M. González, and Melissa Lamar are Editorial Board Members of this journal but were not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
All other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are openly available in the BIOLINCC URL (https://biolincc.nhlbi.nih.gov/home/). Researchers can apply for access to the public use data sets for specific research projects by contacting the data curators at NHLBI. The direct link to the Data Request Form for the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) data is: ![]() ; of note, researchers must first register on the BIOLINCC website for access to this form.
; of note, researchers must first register on the BIOLINCC website for access to this form.